
Abstract
Objectives
There is conflicting data comparing minimally invasive vein harvest (MIVH) using endoscopic technique and open vein harvest (OVH) in terms of bypass patency, wound infection incidence, and patient morbidity. Our institution has performed MIVH since 2003 for peripheral bypass procedures with a consistent team of specialized endoscopic vein harvesters. This study reviewed the major outcomes of MIVH infrainguinal bypass at our institution given a predominant cohort of critical limb ischemia.
Methods
We performed a 10-year, retrospective, single-institution review from January 2005 to December 2014, identifying all patients undergoing MIVH for obstructive infrainguinal disease. Primary outcomes were primary patency, operative time, intraoperative complications, surgical site infection (SSI), and freedom from amputation.
Results
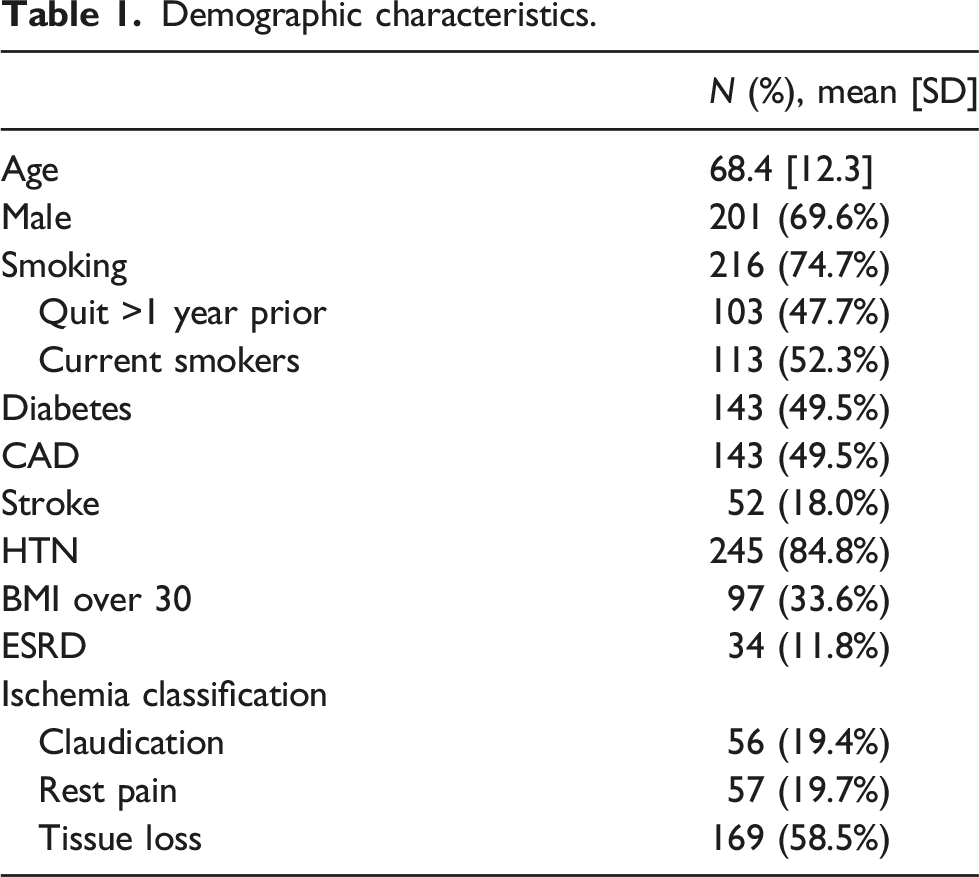
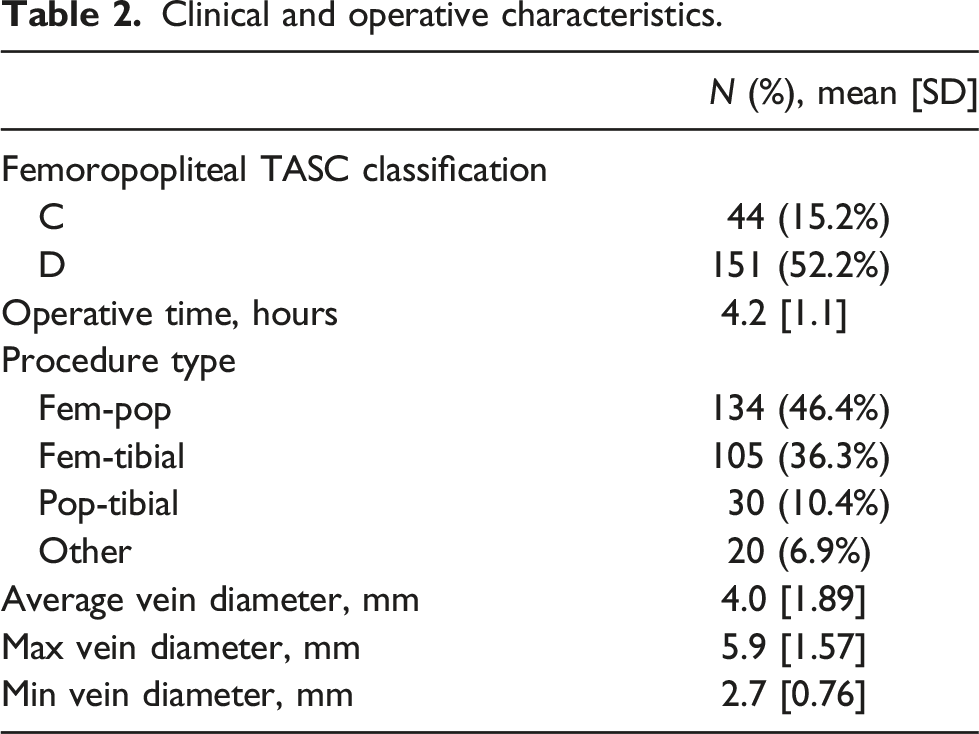
A total of 289 patients (70% male) underwent MIVH infrainguinal bypass at an average age of 68 ± 12 years old, an obesity prevalence of 28%, and with critical limb ischemia in 81% of the patient cohort (20% rest pain, 61% tissue loss/gangrene). Ninety-four percent of patients had no intraoperative complications, 2.5% had adverse cardiac or technical complications, and 4.2% of patients required transfusion. Average operative time was 4.2 h. Femoral-popliteal TASC classification C and D constituted 80% of our patient cohort. At the last follow-up, toe pressures had increased from 30 ± 30 to 62 ± 40 mmHg (p < 0.0001). Primary bypass patency in the first 30 days was 95%. SSI incidence requiring surgical treatment was only 6%. Our median length of stay was 4.0 days, with median intravenous narcotic use of 1 day. In addition, 77% of patients returned to their baseline mobility at first follow-up (median 19 days), and 83% of patients had freedom from amputation at last follow-up (median 820 days).
Conclusions
In a center with experience in MIVH and a consistent group of experienced endoscopic vein harvesters, MIVH bypass has excellent patency, low surgical site infection, short length of stay, and prompt return to baseline mobility.
Introduction
Infrainguinal arterial bypass continues to offer excellent outcomes through standard, well-described operations for limb claudication and ischemia. Open vein harvest techniques have shown excellent results over many decades. Traditionally, lower extremity bypass has been carried out using an open technique that involves a long unilateral incision for vein procurement, bridged incisions for in-situ bypass, or multiple bilateral incisions in the case of contralateral vein harvest.
Endoscopic approaches have widely been used in cardiothoracic surgery1,2 with excellent results regarding patency. With improved endoscopic techniques and technology, there have been decreased wound complications in cardiac surgery patients without compromise of coronary bypass patency.2,3 However, endoscopic vein harvest has not been as widely accepted for lower extremity bypass, with conflicting data comparing minimally invasive vein harvest (MIVH) and open vein harvest (OVH) bypass patency, wound infection rates, and patient morbidity.4–13 A systematic review of 18 cohort studies and case series reported reduced primary patency rates and no advantages with wound complications for MIVH. 8 Of note, the studies reviewed had widely varying protocols and numbers of patients enrolled. Primarily, there is a fear of compromising patency with a minimally invasive approach secondary to endoscopic techniques and handling of the vein during procurement.
Our institution has performed MIVH for vascular surgery procedures since 2003 with a consistent team of experienced physician assistants performing all endoscopic vein harvests for cardiac surgery and vascular surgery services. The purpose of this study is to review major outcomes over a decade’s experience at a high-volume single institution performing lower extremity revascularization with MIVH for obstructive disease. We hypothesize that MIVH leads to favorable primary patency, wound complications, length of stay, and post-operative pain control.
Methods
Patient cohort
We performed a 10-year, single-institution, retrospective cohort study from January 2005 to December 2014, identifying all patients undergoing MIVH for obstructive infrainguinal disease. We excluded patients treated for infrainguinal aneurysmal disease. MIVH was routinely performed for all infrainguinal bypasses. Demographic factors and co-morbid conditions included sex, age, obesity (defined as body mass index > 30), smoking status, hypertension, diabetes, coronary artery disease, stroke, and end stage renal disease. All patients underwent pre-operative vein mapping, and vein diameter measurements (maximum, minimum, and average) were documented. The patient’s operative indication was recorded (claudication, rest pain, or tissue loss). Every patient’s pre-operative angiographic study (diagnostic lower extremity angiogram or computed tomography angiogram of the abdominal aorta with runoff) was independently reviewed by two qualified vascular surgeons to stratify Trans-Atlantic Inter-Society Consensus Document (TASC) runoff classification. The St. Joseph Mercy Ann Arbor Institutional Review Board provided approval for this study (R-15-1709).
Vein harvest technique
A dedicated team of cardiothoracic surgery physician assistants performed all endoscopic vein harvesting for every patient included in the study. This team has significant MIVH experience working with the cardiothoracic team at our institution. In this way, harvesting techniques were standardized and not surgeon dependent. Pre-operative vein mapping was performed to identify the anatomy and suitability of lower extremity veins as conduits.
Several iterations of the current Maquet/Getinge Vasoview Hemopro 2 Endoscopic Vessel Harvesting System have been used at our institution since the late 1990s (Figure 1). The current system provides for a small (2.5–3 cm), single-port incision approach to the greater saphenous vein and other conduits (lesser saphenous veins, cephalic and brachial veins, as well as radial arteries used for coronary bypass). The system uses CO2 insufflation via the port to distend perivascular tissue, creating a tunnel to aid visualization of the conduit, as well as encourage hemostasis. A blunt-tipped dissector attached to a 5 mm endoscope is inserted and passed along the anterior and posterior aspects of the vein. This is the first step to free the vein and branches from surrounding tissues. The endoscope is then inserted into a cannula device containing a retractable “C” ring and a long, retractable endoscopic-styled heat sealer for dividing the branches. The C-ring protects the vein from thermal injury during division of its branches. A “stab-and-grab” technique is typically used at the distal termination of the harvest by making a nick in the skin and inserting a fine-tipped hemostat to grasp the vein under scope visualization and deliver it for extracorporeal ligation and division (Supplementary Figure 1). The vein was then inflated with heparinized saline, if the vein was <3 mm or had multiple areas of stenosis, discarding the vein would have been considered and a second vein harvest on the other leg would have been considered. As an example, the appearance of a superficial femoral to distal posterior tibial bypass with MIVH is shown in Figure 2. Endoscopic greater saphenous vein harvest. Operating room equipment, set up, and approach to endoscopic harvest of right greater saphenous vein via incision just medial and distal to the tibial condyle. Incisions following lower extremity bypass with endoscopic vein harvest. Image shows incisions on post-operative day 1 following mid-superficial femoral artery to posterior tibial bypass with endoscopic harvest of greater saphenous vein. Solid yellow arrows at sites of proximal and distal anastomoses. Dashed red arrow at endoscopic harvest site. Dotted blue arrow at site of “stab-and-grab” extraction site.

Outcomes
Primary outcomes assessed in this study included primary patency and hemodynamic success (assessed using ankle-brachial index (ABI) and toe pressure (TP)), both assessed at first follow-up within 30 days. Primary patency was defined as a patent graft without any endovascular or surgical intervention and was assessed by duplex ultrasound color flow. Other operative outcomes included intraoperative complications (cardiovascular, technical, and transfusions) and operative time. Post-operative outcomes included wound complications including surgical site infection (SSI), length of stay, intravenous narcotic use, return to baseline mobility (at discharge and at first follow-up), and freedom from amputation (at last follow-up). Return to baseline mobility was a patient’s subjective self-assessment of their mobility at the time of assessment compared to their pre-operative mobility.
Statistical analysis
Descriptive statistics including frequency with percent for categorical variables and mean with standard deviation (SD) for continuous variables were reported. ABI and TP measurements were compared pre-operatively and post-operatively using paired samples t-tests. Statistical analysis was performed using Microsoft Excel and iSTAT, with an alpha of 0.05 for statistical significance.
Kaplan–Meier curves were created showing the probability of several outcomes of interest over time, starting with their initial bypass. The outcomes of interest were time to amputation, primary patency (endovascular intervention), and primary-assisted patency (endovascular intervention or revisional bypass). In each case, the time between initial procedure and the outcome of interest is calculated in months (28 days). If a patient did not experience the outcome of interest, the patient was censored at the time of last follow-up.
Results
Demographics and clinical characteristics
Demographic characteristics.
Clinical and operative characteristics.
Primary patency and hemodynamic success
Primary bypass patency as assessed by duplex ultrasound in the first 30 post-operative days was 95%, primary assisted patency rate of 96.5%, and freedom from amputation rate of 98%. Further evaluation at one-year showed a primary patency rate of 81%, primary-assisted patency rate of 87% and freedom from amputation rate of 93%. There was no statistically significant difference between the primary patency rates of ipsilateral and contralateral vein, 5% versus 6%, respectively, (p-value of 0.77). Primary patency over the length of the study is presented in Kaplan–Meier curves (Figure 3). A total of 37 patients (14.3%) required a redo bypass, at median of 6 (1.25–10) months after their initial operation. Freedom from amputation at last follow-up (median 2.25 (0.96–4.14) years) was 82.5%. One-year mortality was 9.9%. Kaplan–Meier curves showing freedom from amputation, primary patency, and primary assisted patency. (a) Time from bypass to amputation. (b) Primary patency. (c) Primary assisted patency.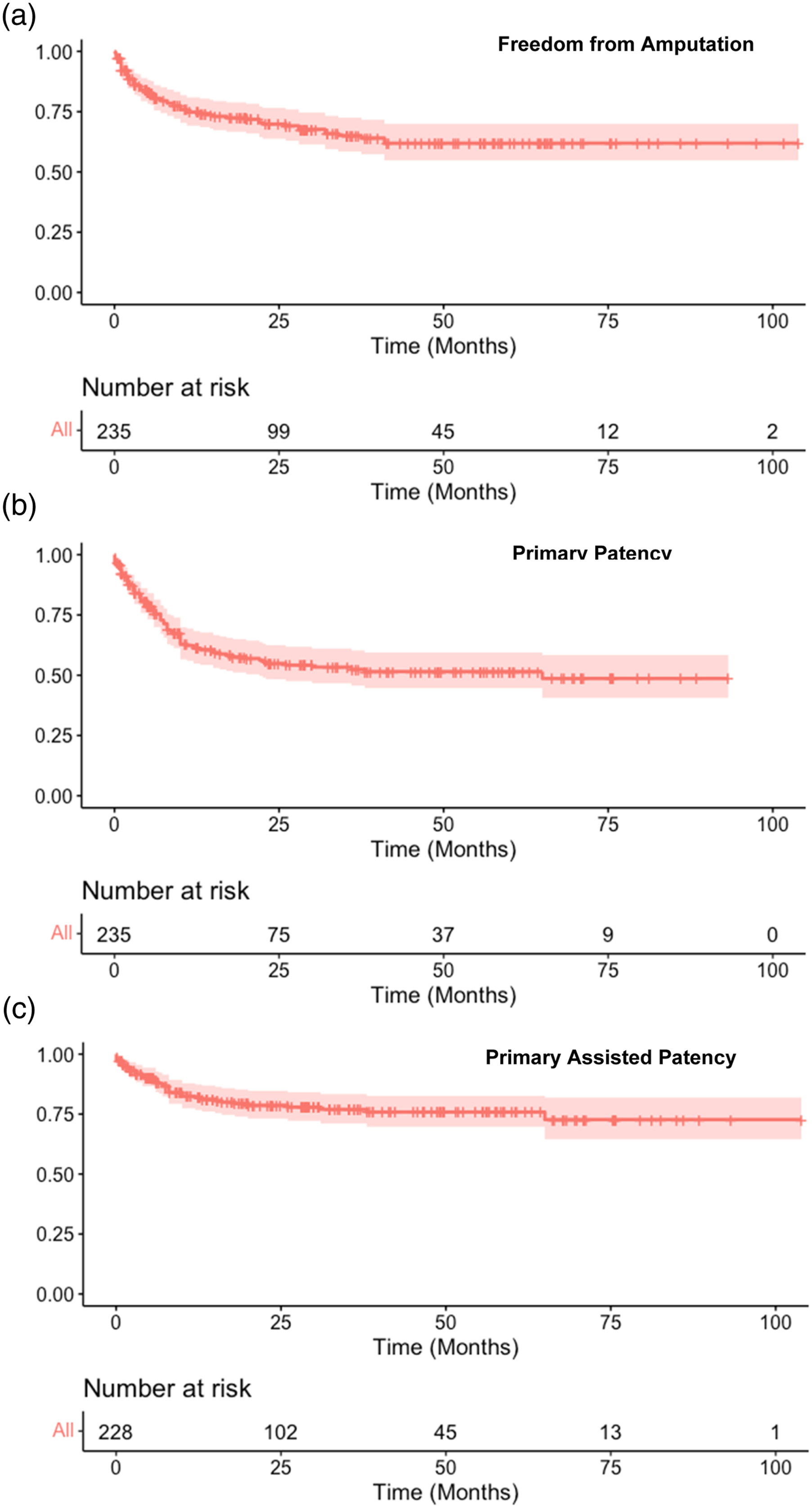
On pre-post analysis of ABI (Figure 4), a significant improvement was noted following surgery, from a pre-operative average of 0.56 (0.34) to 0.86 (0.35) post-operatively (p < 0.001). Given the significant amount of incalculable ABI and CLI in our patient population, toe pressures were also assessed. At last follow-up, toe pressures were found to increase from 30.1 ± 29.6 pre-operatively to 62.0 ± 40 (p < 0.0001). Pre- and post-intervention average ankle-brachial indices and toe pressures. Toe pressure measurements in mmHg.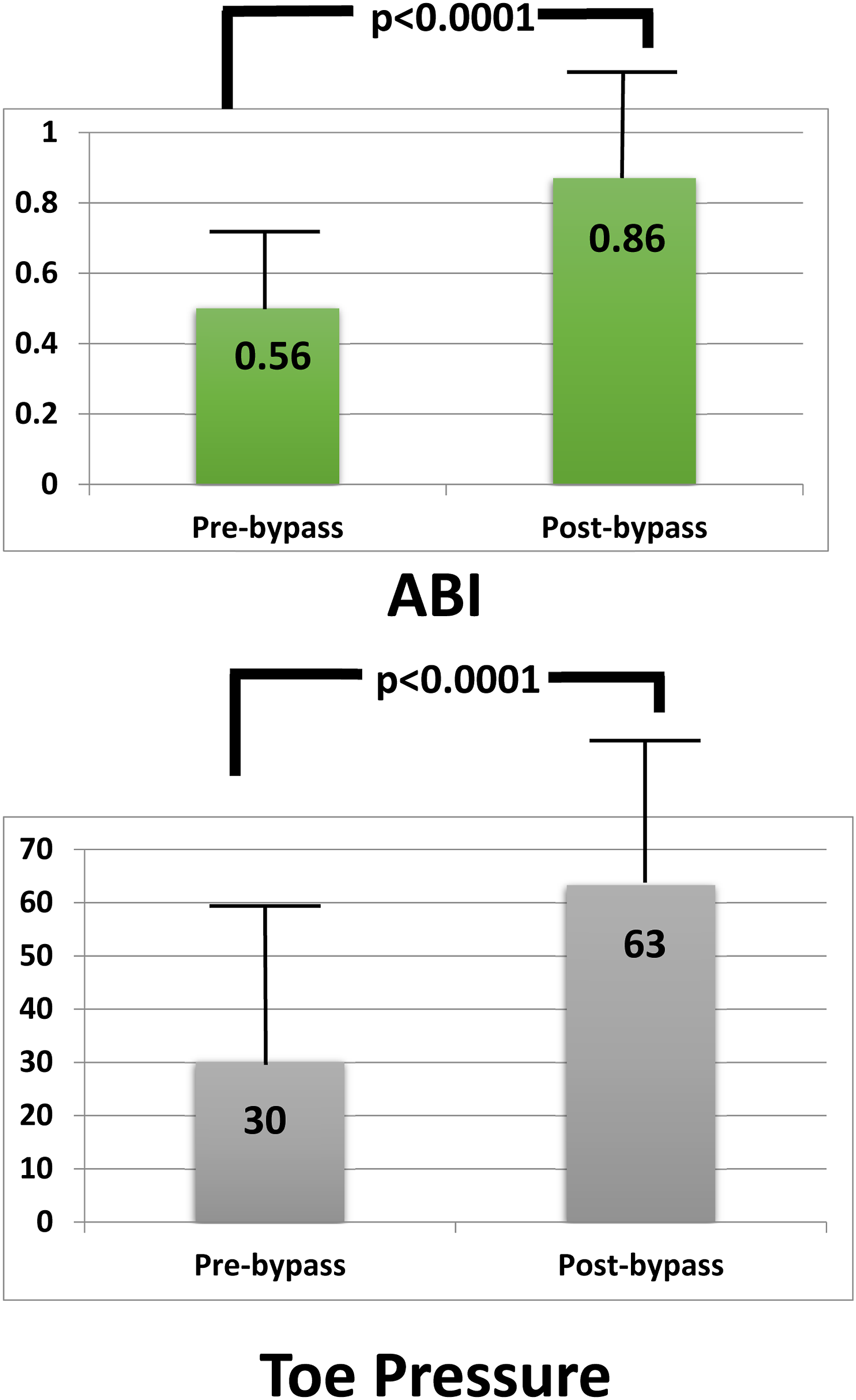
Post-operative clinical outcomes
Post-operative clinical outcomes.
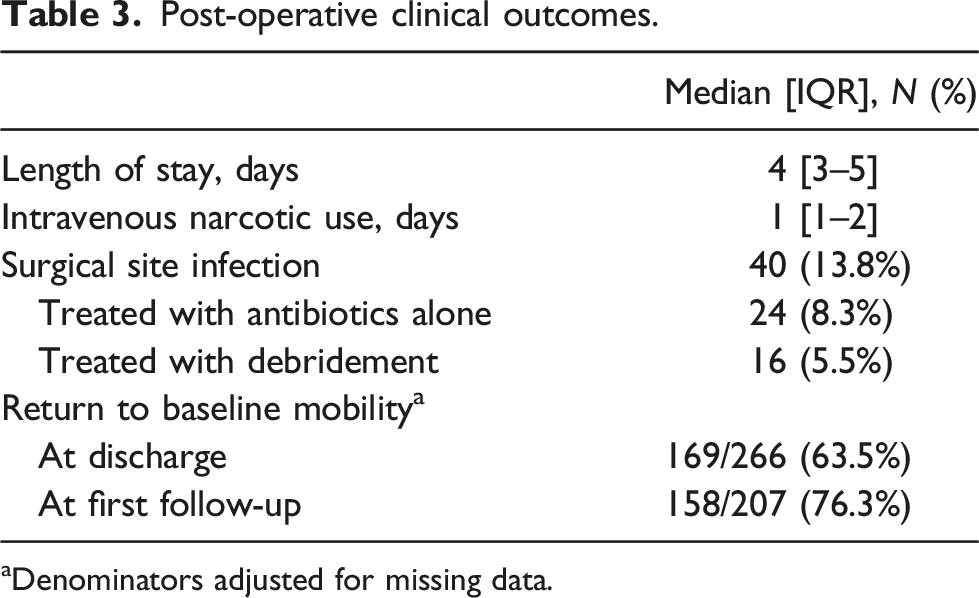
aDenominators adjusted for missing data.
Discussion
The role of endoscopic vein harvest for lower extremity bypass remains controversial. In the absence of prospective trials, there have been conflicting results from retrospective reviews. At our institution, 289 patients undergoing infrainguinal bypass with MIVH demonstrated excellent short-term primary patency with hemodynamic success. This cohort demonstrated very favorable results, with low rates of wound complications, short length of stay, minimal need for IV narcotics, and prompt return to baseline mobility. Previous cohort studies and case series of endoscopic vein harvest for lower extremity bypass are relatively small, with the largest previously published series including 170 patients. 10 Our study represents the largest cohort of lower extremity bypass with MIVH to date, with 289 patients treated over a 10-year period with excellent short-term outcomes and enhanced recovery for this population that underwent surgery primarily for CLI. These procedures were performed by five surgeons over the 10 years of the study, but unlike previous studies, the endoscopic vein harvest was performed by a trained and dedicated team of physician assistants. MIVH was routinely used for all lower extremity bypass procedures, eliminating the potential for patient selection to impact our results. Our cohort shows superb results possible at a high-volume center with a team of dedicated and highly trained operators.
Previous studies have shown reduced primary patency rates following MIVH compared to OVH.4,8,10,12 Notably, a recent retrospective analysis of 194 OVH and 86 MIVH patients demonstrated higher primary patency for OVH (82.8%) compared to MIVH (59.9%) at 1 year. 14 Another retrospective study looking at 164 patients showed excellent short-term patency with a 30-day primary patency rate of 90.5% and higher 1-year primary patency of 68.9%. 9 However, another recent study of 113 patients treated by surgeons with >5 years experience performing MIVH demonstrated similar primary patency and improved secondary patency following MIVH compared to OVH. 15 The authors also found improved patency compared with their previous initial experience using MIVH at their institution. They conclude that with continued use and experience, patency rates have shown a clear improvement. Our results showing primary patency of 95% at 30 days and 81% at 1 year following MIVH support their conclusion that with experience, lower extremity bypass with MIVH results in excellent short-term patency. Longer-term, our freedom from amputation in this series show favorable results without the fear of recurrent need for early secondary interventions or early thrombosis from thermal injury. In part, this may be due to a highly trained group of endoscopic vein harvesters achieving high volumes and shared between cardiac surgeons performing coronary artery bypass grafting in addition to vascular surgeons with a robust lower extremity bypass program.
Decreased wound complications and patient morbidity are relatively well-established benefits of MIVH. This has been demonstrated in multiple previous studies.6,12,14 The rate of any wound complications was 16.2%–20.4% for MIVH compared to 22.9%–46.9% for open vein harvest reported in two institutional studies.4,15 Our study again demonstrates low rate of wound complications following MIVH, with only 14% of patients having any wound complication and of those only 6% had significant enough SSI to require debridement. This notably includes the anastomotic site and not only the harvest site. Our study also found that patients had minimal IV narcotic need and prompt return to baseline mobility. Return to baseline mobility is a critical functional outcome measure following lower extremity intervention, particularly with open surgical bypass. These salutary benefits should not be overlooked when evaluating a patient’s overall recovery and evaluation of surgical bypass value. It serves as an important in-hospital and short-term endpoint, with effects on morbidity, mortality, clinical value, and quality of life. 16 Our study demonstrated 77% of patients promptly returned to baseline mobility, which may be an added benefit of endoscopic techniques over traditional OVH. An additional benefit of MIVH that is not to be overlooked is the financial impact, with one study demonstrating a US$2200 decreased cost per procedure compared with open harvest. 6 In our study, we found relatively short post-operative courses for our patients, the median length of stay was 4 days with 61% of patients being discharged between post-operative days 2 through 4. We feel this approach supplements the armamentarium of a modern-day vascular surgeon and complements alternative, aggressive endovascular revascularization as a means of achieving surgical durability with decreased morbidity.
Our findings should be interpreted with several limitations in mind. This is a single-institution, retrospective review that is susceptible to biases inherent to retrospective studies, namely, selection bias. Most patients came back with routine arterial surveillance studies, but this was underpowered to draw meaningful conclusions regarding primary assisted or secondary patency rates. However, all patients at our institution treated with surgical bypass were treated with MIVH, and therefore there was no selection of patients for MIVH (instead of open vein harvest) by the surgeons. This practice pattern contributes to another possible limitation, which is the lack of a control or comparison group in our study. While we are unable to directly compare patients treated with MIVH and OVH due to the lack of OVH volume, the outcomes of our MIVH cohort remain notable when considering results from historical cohorts and those from other studies.
Conclusions
In this large retrospective review of lower extremity bypass with MIVH, excellent rates of patency and limb salvage were obtained in a predominantly critical limb ischemia population. Patients also had favorable post-operative outcomes including wound infection, IV narcotic use, length of stay, and prompt return to baseline mobility. MIVH is an excellent adjunct to obtain acceptable patency, reduce morbidity of open surgery, and improve the value of surgical bypass as a strong competitor to ever-increasing aggressive endovascular revascularization techniques.
Supplemental Material
Supplemental Material - Ten-year experience of infrainguinal bypass with endoscopic vein harvest
Supplementary Material for Ten-year experience of infrainguinal bypass with endoscopic vein harvest by Rhami Khorfan, Aela Vely, Farwa Batool, Miles W Jackson, M LaWaun Hance, Diane J Jones, Jarred A Napier, Michael J Heidenreich and Abdulhameed Aziz in Vascular
Footnotes
Author’s note
This paper was presented as an oral presentation at the Midwestern Vascular Surgery Society 2017 Annual Meeting in Chicago, IL.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The St. Joseph Mercy Ann Arbor Institutional Review Board provided approval for this study (R-15-1709).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.