
Abstract
Popliteal artery entrapment syndrome (PAES) is a rare vascular disease, and cases of bilateral PAES associated with distinct symptoms in each of the affected legs are very rare. In an effort to improve current understanding regarding the presentation and treatment of this condition, a case of bilateral PAES is herein described with a corresponding review of the associated literature. The overall process of diagnosing and treating one patient affected by bilateral PAES was retrospectively assessed to provide comprehensive insight regarding this disease. This patient was diagnosed via contrast-enhanced computed tomography (CT), and right-sided symptomatic PAES was successfully treated via autogenous saphenous venous graft arterial bypass surgery. In contrast, the asymptomatic left-sided PAES in this patient was subject to close follow-up monitoring. Over a 2-year postoperative follow-up period, this patient did not experience any symptoms or complications. As such, autogenous saphenous venous graft arterial bypass surgery represents a safe and efficacious means of treating PAES, whereas surgery may not be required for cases of asymptomatic PAES even in patients with a bilateral presentation.
Introduction
Popliteal artery entrapment syndrome (PAES) is a rare vascular disease that most frequently develops in younger males.1-3 Most PAES patients exhibit a unilateral presentation, although some bilateral cases have been reported. 4 The most common presenting symptom in PAES is ischemic claudication resulting in disrupted blood flow from the popliteal artery (PA) owing to compression by a fibrous band or by the gastrocnemius or popliteus muscles.5-6 Both computed tomographic angiography (CTA) and magnetic resonance imaging (MRI) can be used to guide the diagnosis of PAES,7-8 and it is most frequently treated through surgical exploration with fasciotomy, myotomy, or the sectioning of established fibrous bands to release the affected PA. In cases where patients experience thrombotic occlusion, it may be necessary to perform thromboendarterectomy with venous patch arterioplasty, or venous graft arterial bypass surgery.9-11 Advances in endovascular techniques have led to the proliferation of these approaches to treating PAES.12-13 However, the use of these techniques remains the subject of controversy, as does the determination regarding whether or not asymptomatic patients should receive treatment. Below, we describe a case of bilateral PAES in which the affected limbs exhibited distinct symptoms, with a corresponding literature review of approaches to treating PAES.
Case report
A 17-year-old male with a 5-months history of intermittent claudication of the right leg and increasing pain over the last month presented for treatment. The patient did not report any history of trauma, nor did he present with risk factors associated with the potential development of thromboangiitis obliterans or atherosclerosis such as infection, smoking, hyperlipidemia, diabetes, or hypercoagulability. Clinical examination revealed that the patient’s right foot and calf were pale and cold, and the pulse in the popliteal, pedal, and posterior tibial arteries could not be detected via palpation. The ABI of the right leg was 0.45. The left leg was angiographically normal, with an ABI of 0.96. The patient was preliminarily diagnosed with right lower limb ischemia following admission, and lower limb CTA imaging revealed the thrombosis of the right PA together with bilateral PAES (Figure 1). The patient exhibited normal results in D-dimer, immune-related antibody, and coagulatory function tests. Accordingly, a clinical diagnosis of bilateral PAES was proposed. Following a discussion of this case, it was determined that autogenous saphenous venous graft arterial bypass surgery was the most appropriate treatment for the right-sides PAES, whereas the left-sided PAES would be subject to close monitoring and follow-up. CT three-dimensional reconstruction showed PAES of both limbs and thrombosis of right popliteal artery (L for left, R for right, A for artery, M for muscle and T for thrombosis).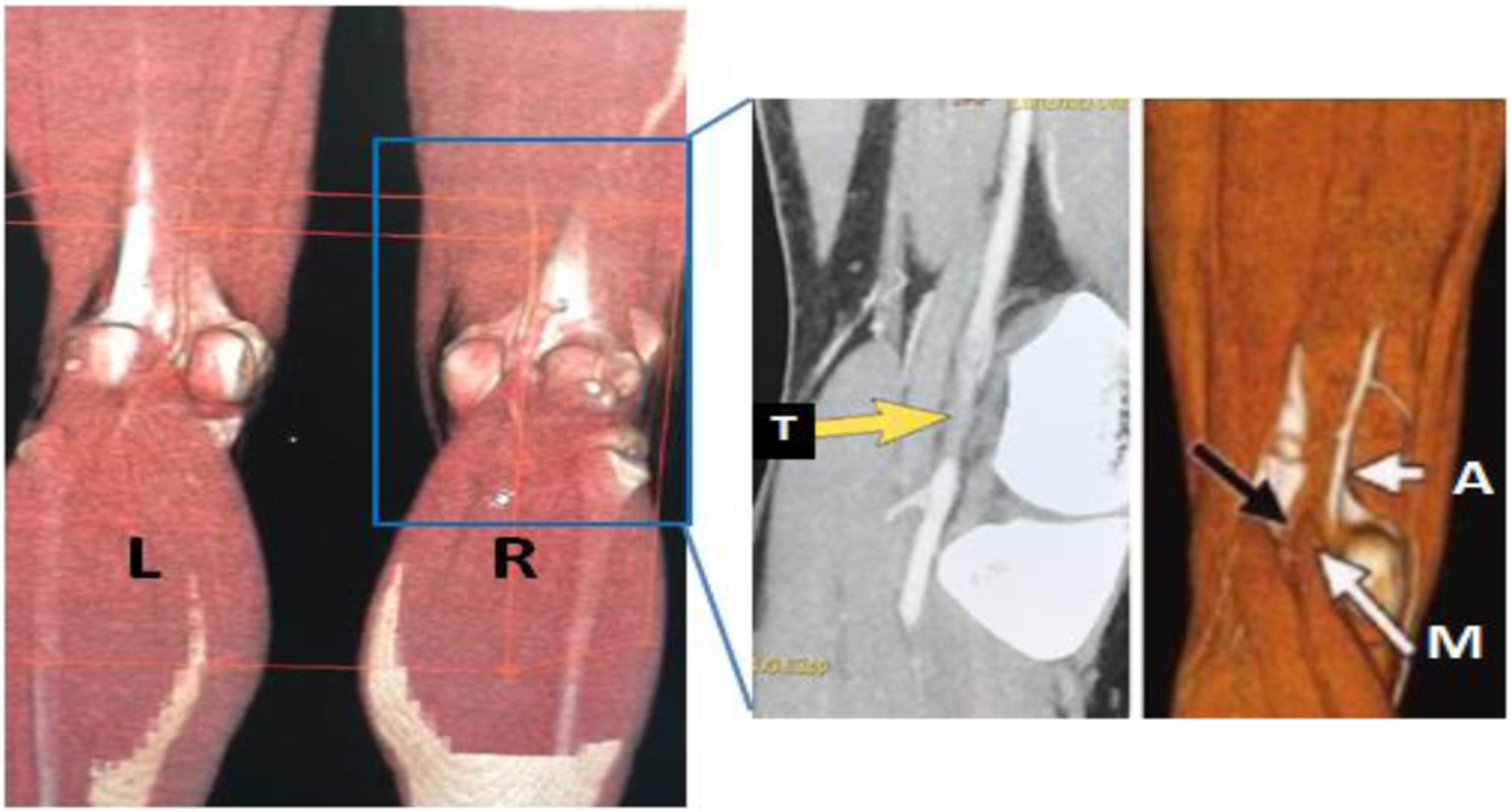
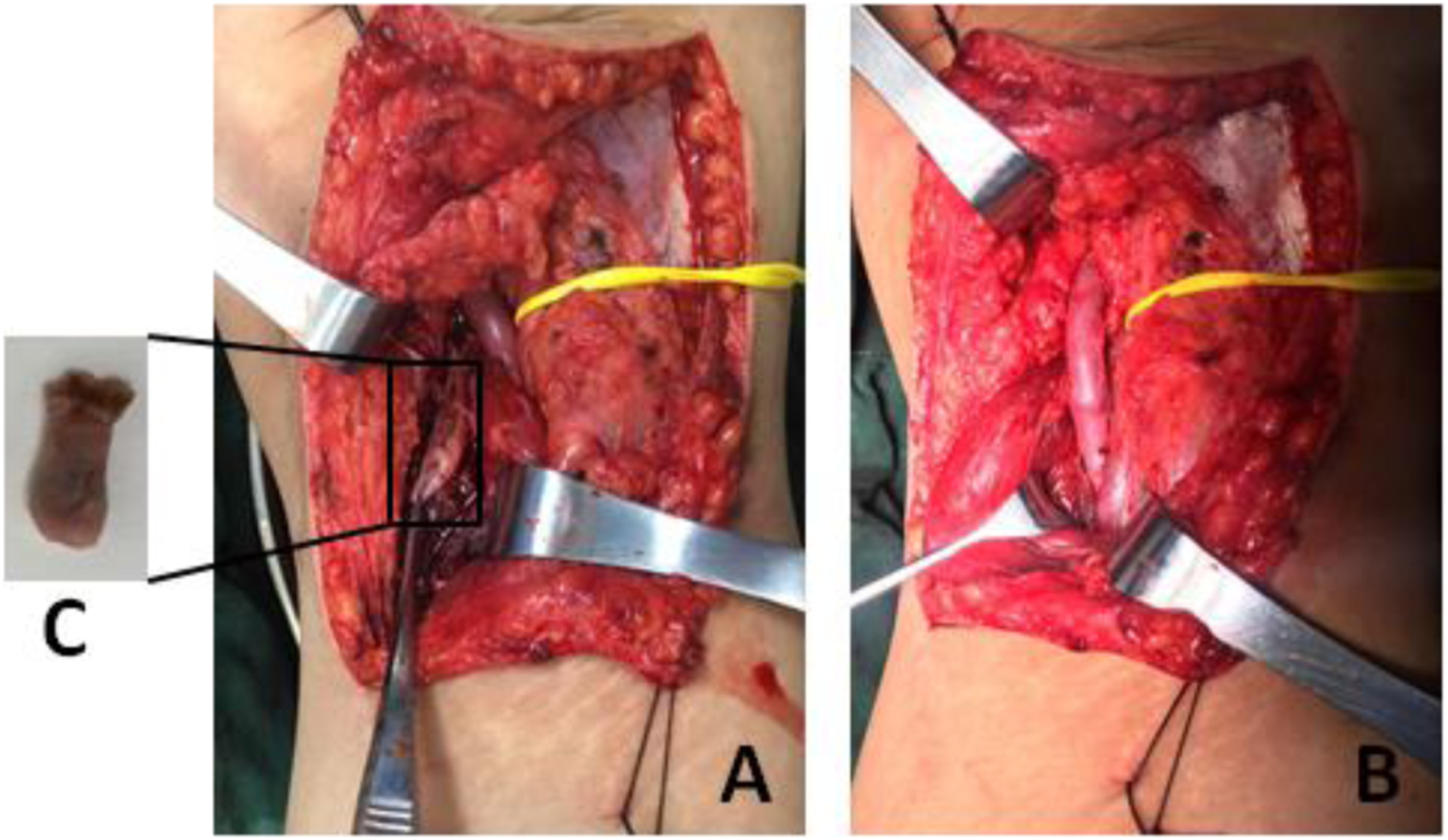
After the initiation of total intravenous anesthesia, the patient was administered a bolus of heparin (2500 U). The left femoral great saphenous vein (GAV) was then sufficiently exposed, and an 8 cm segment of the GAV was excised for grafting (Figure 2). The entirety of the right PA was then dissected and assessed, revealing type II PAES in which the PA had been compressed by the dislocation of the medial gastrocnemius head toward the lateral aspect (Figure 3(a)). When a longitudinal venotomy of the compressed right PA was performed, an old thrombus was found therein (Figure 3(c)). The GAV graft was then used to bypass the compressed region of the PA to the middle of the medial and lateral heads of the gastrocnemius (Figure 3(b)). End-to-end arteriovenous anastomosis was performed with continuous 6-0 polypropylene sutures, and the patient was administered postoperative low molecular weight heparin (LMWH) for 1 week without any complications, after which he was discharged. Great saphenous vein for graft. Autogenous saphenous venous graft arterial bypass surgery (A showed Type II PEAS in this patient, B showed blood flowing in grafted vessels, C showed thrombosis in popliteal artery).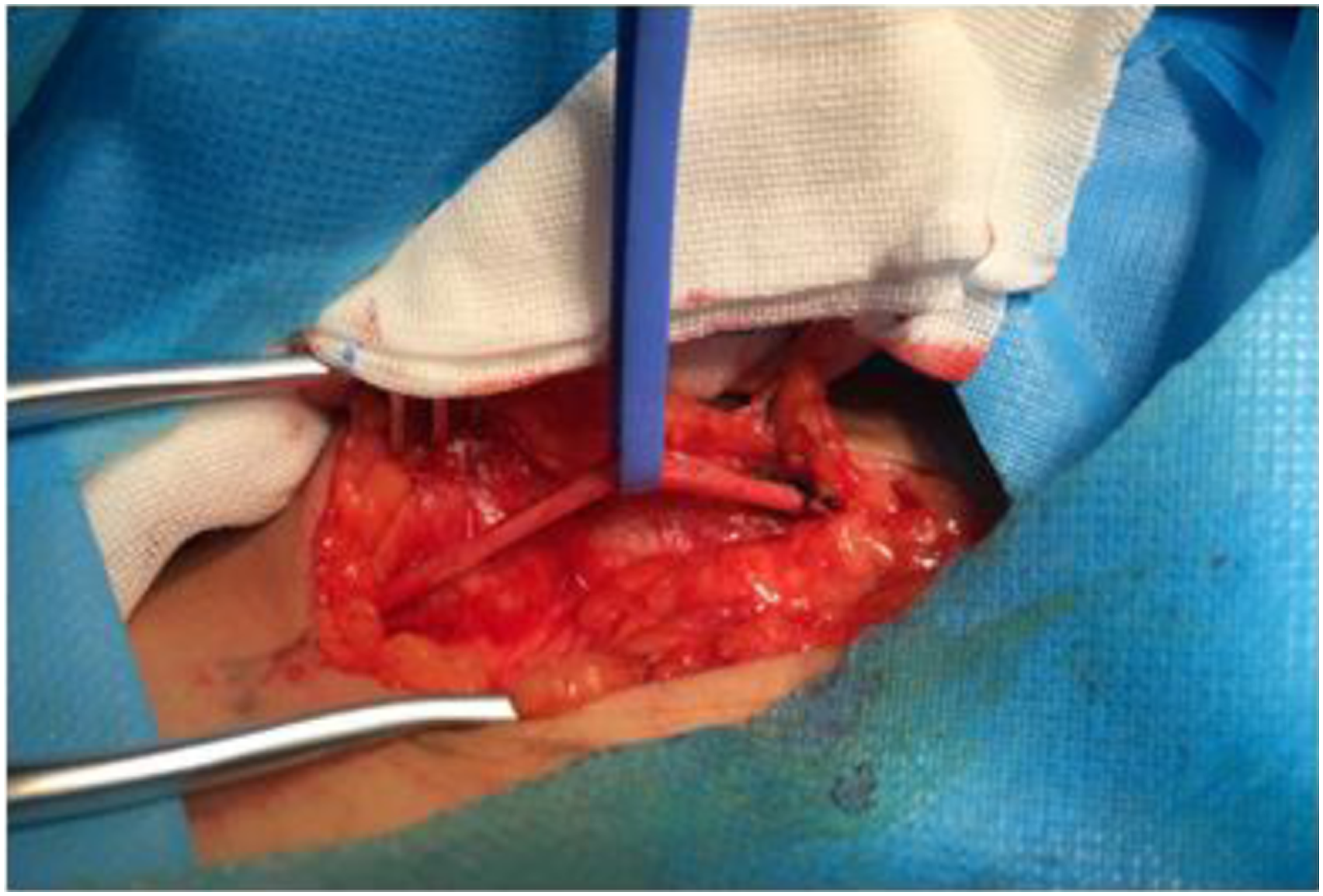
Following discharge, the patient continued to consume oral antiplatelet drugs for 1 year (aspirin, 100 mg QD; clopidogrel bisulfate, 75 mg QN). At 2 years post-surgery, a color Doppler ultrasound of the operative site revealed normal blood flow (Figure 4). The ABI of the right leg at this follow-up time point was 0.93, while the left leg remained free of any abnormalities with an ABI of 0.96. Color Doppler ultrasound test for right popliteal artery 1 month after the operation.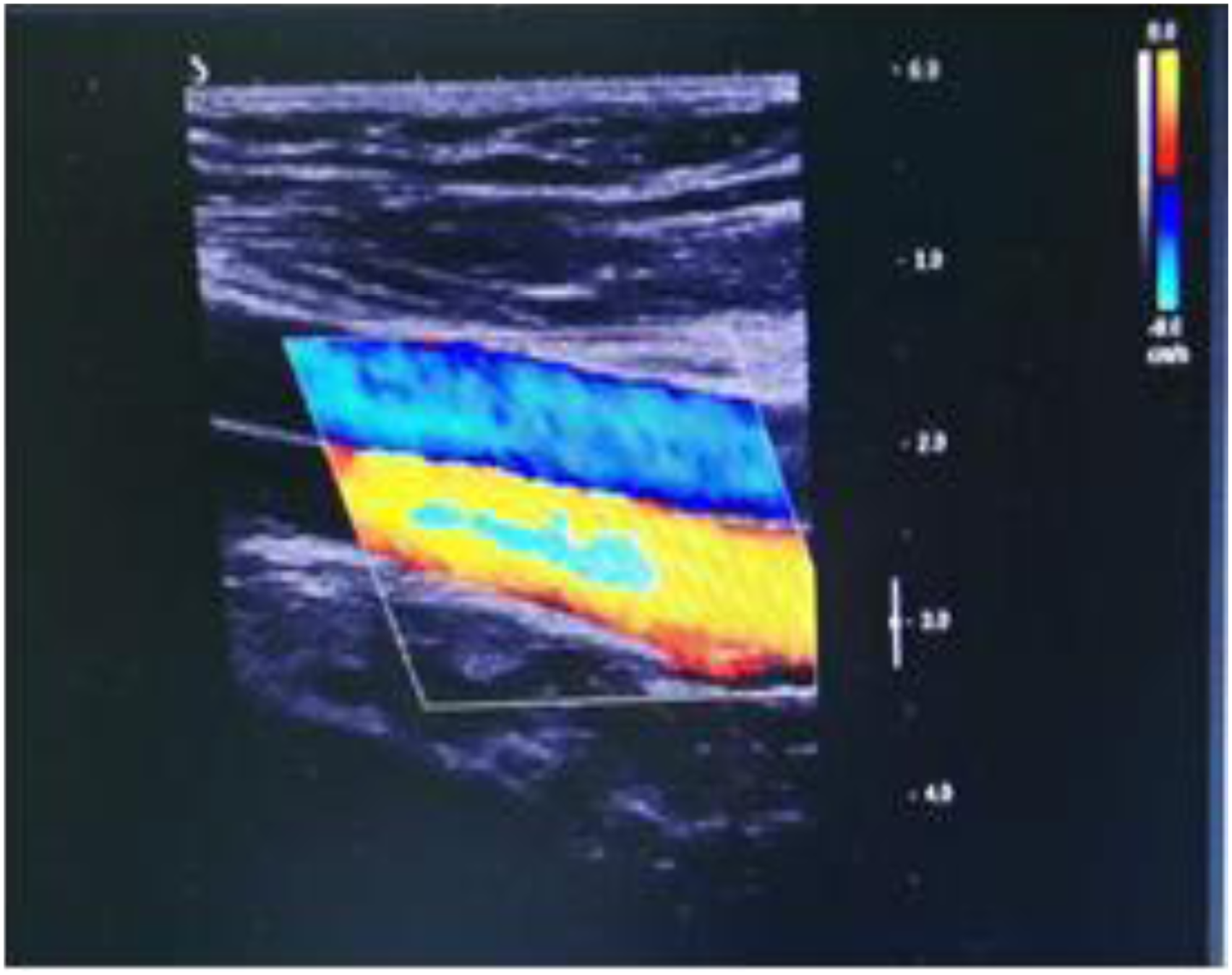
Discussion
PAES is a rare venous disease that is primarily driven by one of two main causes. The first such cause is the existence of an abnormal relationship between the PA and proximal musculotendinous structures,14-15 while the other consists of factors including obesity, hypercoagulability, trauma, and vigorous exercise.16-17 The precise relationship between these two causes is not fully understood. PAES can be definitively diagnosed through the use of CTA, MRI, or DSA-based imaging approaches.7-8 When not adequately treated, PAES can result in acute limb ischemia as a consequence of the thrombosis, embolization, or aneurysmal degeneration of the PA. 18 Accordingly, diagnosing and treating PAES as quickly as possible are generally considered critical to optimal patient outcomes. 19
PAES is broadly classified into five main types. Type I is characterized by a PA that bypasses the beginning of the medial head of the gastrocnemius, running down the deep side of this muscle. Type II is characterized by PA oppression as a result of the dislocation of the medial gastrocnemius head toward the lateral aspect. Type III corresponds to the oppression of the PA by abnormal chordae tendineae extending from the medial cephalic margin of the gastrocnemius/Type IV results from PA oppression by either abnormal chordae tendineae or the popliteal muscle. Type V PEAS is defined by the entrapment of both the PA and the PV by any of these causes.20-22 Surgical intervention is the first-line approach to treating PAES, 23 although the operative approaches employed vary as a function of disease type. Type I and II PAES cases are often treated via venous graft arterial bypass surgery, whereas type III and IV cases are generally treated via fasciotomy, myotomy, or fibrous band sectioning. When appropriately performed, the definitive surgical treatment of PAES yields effective long-term symptom relief. 25
Other possible approaches to treating PAES have been discussed in recent years, including PA stent implantation 13 and the preventative treatment of asymptomatic PAES cases. 26 The use of PA stent implantation procedures has remained a contentious topic throughout the world, 27 and improvements in stent performance have led this procedure to be increasingly common over the past 5 years.28-30 The benefits of PA stent implantation, however, remain controversial, with some studies reporting encouraging outcomes 31 while others report disappointing results. 32 PA stent implantation is rarely used to treat PAES given that these stents are unlikely to resolve the underlying structural abnormalities and due to the fact that most patients affected by this condition are relatively young. 33 In our opinion, the preventative surgical treatment of asymptomatic PAES is not required. While asymptomatic PAES does, by definition, correspond to some abnormal relationship between the PA and surrounding structures, patients may live a normal life without experiencing limb ischemia in the absence of predisposing factors.34-35 This opinion is partially supported by the present case in which the treated patient exhibited a satisfactory prognosis. As such, autogenous saphenous venous graft arterial bypass represents a feasible and effective means of treating symptomatic PAES, whereas there is no need to treat asymptomatic PAES.
Conclusion
Bilateral PAES is a rare condition that can result in progressive limb ischemia over the course of months, but that may also remain asymptomatic. In symptomatic PAES cases, venous graft arterial bypass surgery remains the most common treatment, whereas endovascular treatment strategies are rarely employed, and further study is warranted. In general, asymptomatic PAES cases do not warrant preventative surgical treatment, although routine observation and follow-up of these cases is important.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Natural Science Foundation of Gansu Province( 2020-0405-JCC-1467), Natural Science Foundation of Lanzhou (20JR10RA742), “Cuiying Science and Technology Innovation” project of Lanzhou University second hospital (CYXZ2019-25).