
Abstract
Introduction
The in situ fenestration (ISF) technique consists of maintaining the patency of the aortic branch after the endoprosthesis is already in place as a viable, effective, and fast-performing alternative to revascularize the aortic arch arteries.
Objective
To report the experience with a series of cases of endovascular treatment of Acute Aortic Syndromes involving the aortic arch, using the ISF technique in a specialized center.
Methods
We analyzed data collected from patients treated with ISF during TEVAR for Acute Aortic Syndromes involving the aortic arch from June 2020 to January 2022, assessing perioperative outcomes, including immediate and late success rates, complications, morbidity and mortality, and short and medium term aortic branch patency.
Results
Of the 11 patients eligible for the ISF procedure, 9 were successful, with a technical success rate of 81%. No patient had a type 1A endoleak related to fenestration. There was complete thrombosis of the false lumen in the thoracic aorta in 77% cases. No death was related to the fenestration technique.
Conclusion
ISF as feasible and with a high rate of technical success and good results in the short and medium term. Prospective studies with long-term clinical follow-up are still needed to fully assess the durability of these unreinforced fenestrations.
Keywords
Introduction
The term acute aortic syndrome (AAS) refers to a heterogeneous group of conditions that cause a common set of signs and symptoms, the main one being “aortic pain.” Several pathological entities can give rise to this syndrome, but, recently, more focus has been shed on etiologies such as penetrating aortic ulcer, intramural hematoma, and their relationship to aortic dissection. A penetrating aortic ulcer is a focal atherosclerotic plaque that erodes through the intima to the middle layer at variable depths. Intramural hematoma is a collection of blood within the aortic wall that does not communicate freely with the aortic lumen, with restricted flow, which may represent a subcategory of aortic dissection that may behave differently due to limited flow in the false lumen. 1
Thoracic endovascular aortic repair (TEVAR) has transformed the management of diseases related to this aortic segment, allowing for the treatment of patients who, in many situations, would not tolerate an open surgical repair. 1 The endovascular approach avoids the need for thoracotomy, aortic clamping, and cardiopulmonary bypass, in addition to offering a favorable perioperative morbidity profile compared to the conventional open treatment. 2
However, broadening the use of TEVAR becomes limited by the challenges of managing diseases involving the Aortic Arch and its branches. Although endovascular treatment has become the preferred method for most pathologies of the aorta’s descending segment, open surgery remains the gold standard for repair of the ascending aorta and aortic arch. 3 The Society for Vascular Surgery guideline suggests routine preoperative revascularization surgery for planned coverage of the left subclavian artery, especially when collateral (vertebral and spinal cord) perfusion may be compromised, thus reducing the risk of stroke and spinal cord ischemia. 4
With the advancement of endovascular technology, several techniques have been used to preserve the branches of the aortic arch, extending the proximal anchorage zone of the endoprostheses. These strategies include open revascularization (debranching), branched devices, parallel stent graft technique (“Chimney” stent), operating table-modified prosthesis by the vascular surgeon, and in situ fenestration (ISF). 5 Although branched and fenestrated endoprostheses the first choice treatment, they are still difficult to apply, considering the waiting time for the manufacturing of personalized devices. Moreover, studies on the use of parallel stent graft techniques have shown a considerable risk of proximal endoleaks, 6 and operating table-modified prostheses require advanced training by the endovascular surgeon, require prolonged surgical time, and present significant intraoperative difficulties in catheterization and adequate positioning of the devices.
The ISF technique poses as a viable, effective and fast-performing alternative to revascularize the arteries of the aortic arch while maintaining aortic branch patency after the endoprosthesis is already implanted. This technique was initially described for revascularization of the left subclavian artery in Ishimaru zone 2 TEVAR and has been applied to other arch vessels and for several thoracic aorta conditions. 7 Some multicenter studies report a high rate of technical success and promising perioperative results using ISF.3,8 The ISF technique consists of fenestrating the endoprosthesis after its correct positioning in the aortic arch, covering the arch branch’s origin. After the implant, the branch is punctured in a distal retrograde manner, a sheath is interposed and the perforation of the endoprosthesis tissue is performed. Several types of tissue perforation are described—such as laser, radiofrequency, needle, and guide wire (trimmed in bevel). Then, the guidewire is positioned in the Thoracic Aorta, through the hole made. Sequential pre-dilations of the prepared fenestrae are performed and, later, the balloon-expandable stent is implanted, maintaining the patency of the branch. Finally, once the stent is in place, an angiography is taken to assess therapeutic success of implantation.2,3,5,7
Methods
This study aims to report the experience of endovascular treatment of Acute Aortic Syndromes involving the aortic arch, using the in situ Fenestration technique, in a specialized center for the treatment of aortic diseases in Salvador, Bahia, Brazil from June 2020 to January 2022.
We performed an analysis of data collected from patients treated with ISF during TEVAR for Acute Aortic Syndromes involving the aortic arch, from June 2020 to January 2022, at Hospital Geral Roberto Santos (HGRS)—a specialized tertiary center for treatment of Aortic Diseases in Salvador, Bahia, Brazil.
Patients with aortic diseases such as: aortic dissection, intramural hematoma, and penetrating aortic ulcer—all involving a segment of the aortic arch and its branches were included in this study.
Fenestration method, devices used, perioperative and follow-up results of this treatment in its acute and subacute phases including rates of immediate and late postoperative success, complications—especially endoleaks— and morbidity and mortality in the short and medium term of each case were assessed.
All included patients were treated at a single center and signed an informed consent form. This study was submitted to the analysis and approval of the Ethics and Research Committee of the HGRS (CAAE n°55829822.6.0000.5028).
Pre-treatment and control CT Angiographies (CTAs) were performed in the bioimaging sector of our hospital and the images were analyzed using the Osirix® software. For the treatments, several thoracic endoprosthesis devices with a metallic structure in nitinol and coating in polytetrafluoroethylene (PTFE) or polyester, respecting the maximum oversizing of up to 10% of the value of the diameter of the proximal neck of the aorta that are available on the market were used.
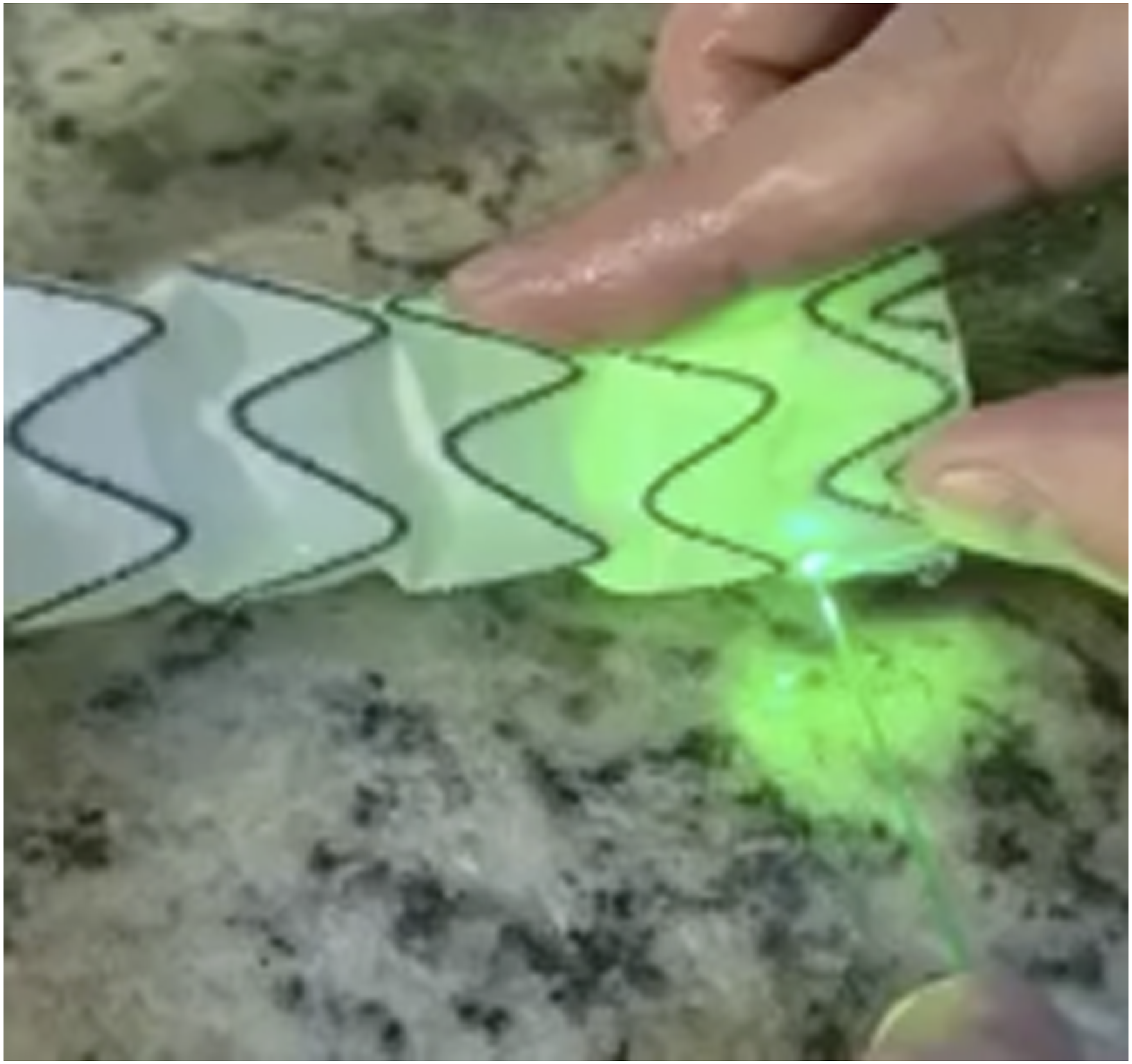
ISF was performed through an ultrasound-guided retrograde puncture of the left brachial artery, with progression of a 5F radial sheath with consequent change to a 7 x 70 cm long sheath until it touched the tissue of the previously implanted endoprosthesis, occluding the left subclavian artery (LSA). After confirming the sheath’s correct positioning, fenestration was performed through a hole in the endoprosthesis tissue, either with a specific laser Schematic diagram portraying steps to perform ISF. Experimental model showing how Laser ISF is applied.
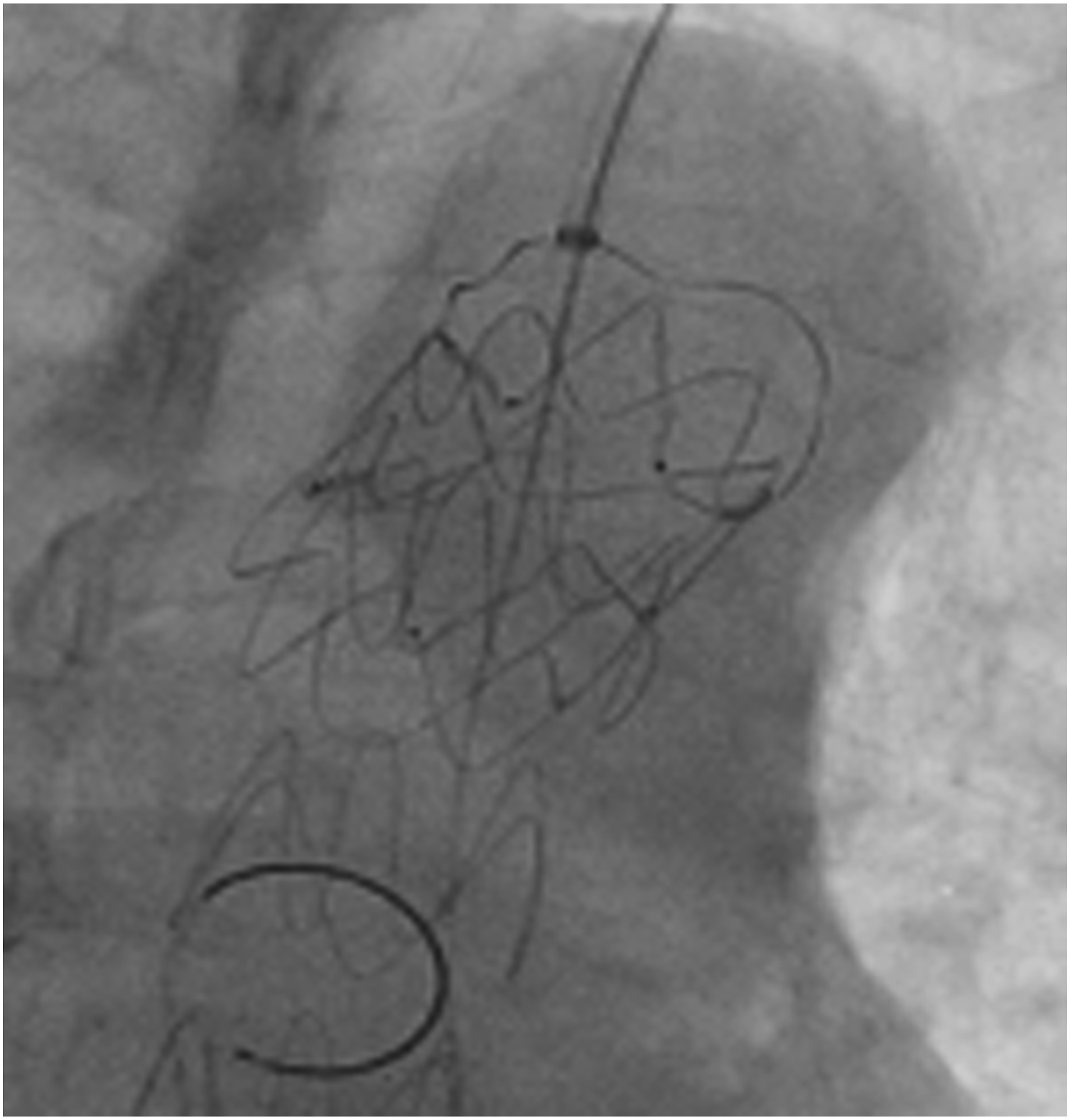
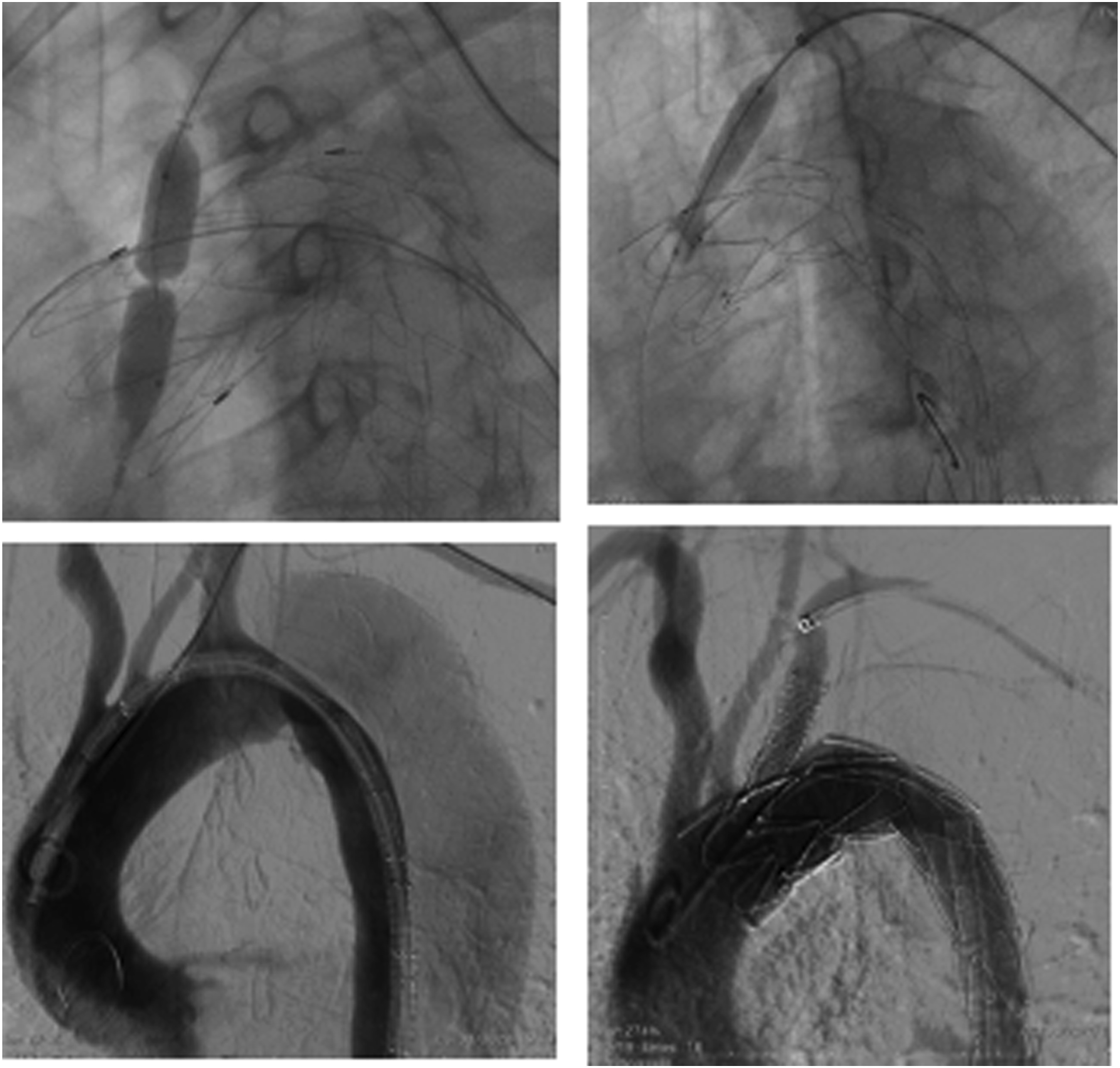
To confirm that the guidewire was positioned inside the fenestrae, it is essential to change the angiograph’s angulation to an anteroposterior (AP) position in order to avoid passing the guidewire parallel to the device (as seen in Figures 3 and 4). Procedure photographically depicted in Figure 5. In none of the cases the endograft was ballooned, since we routinely avoid ballooning in acute aortic syndromes, as in our case series. Schematic diagram showing on the left, an image of the angiograph in the AP position with the guidewire parallel to the endoprosthesis. Right image showing guidewire inside the endoprosthesis. Image of the angiograph in the AP postion showing the guidewire inside of the fenestrae. (A) Dilation of the fenestra orifice with a balloon catheter. (B) Opening balloon-expandable stent. (C) Angiography showing type B aortic dissection. (D) Postoperative control angiography showing fenestration to the Left Subclavian Artery.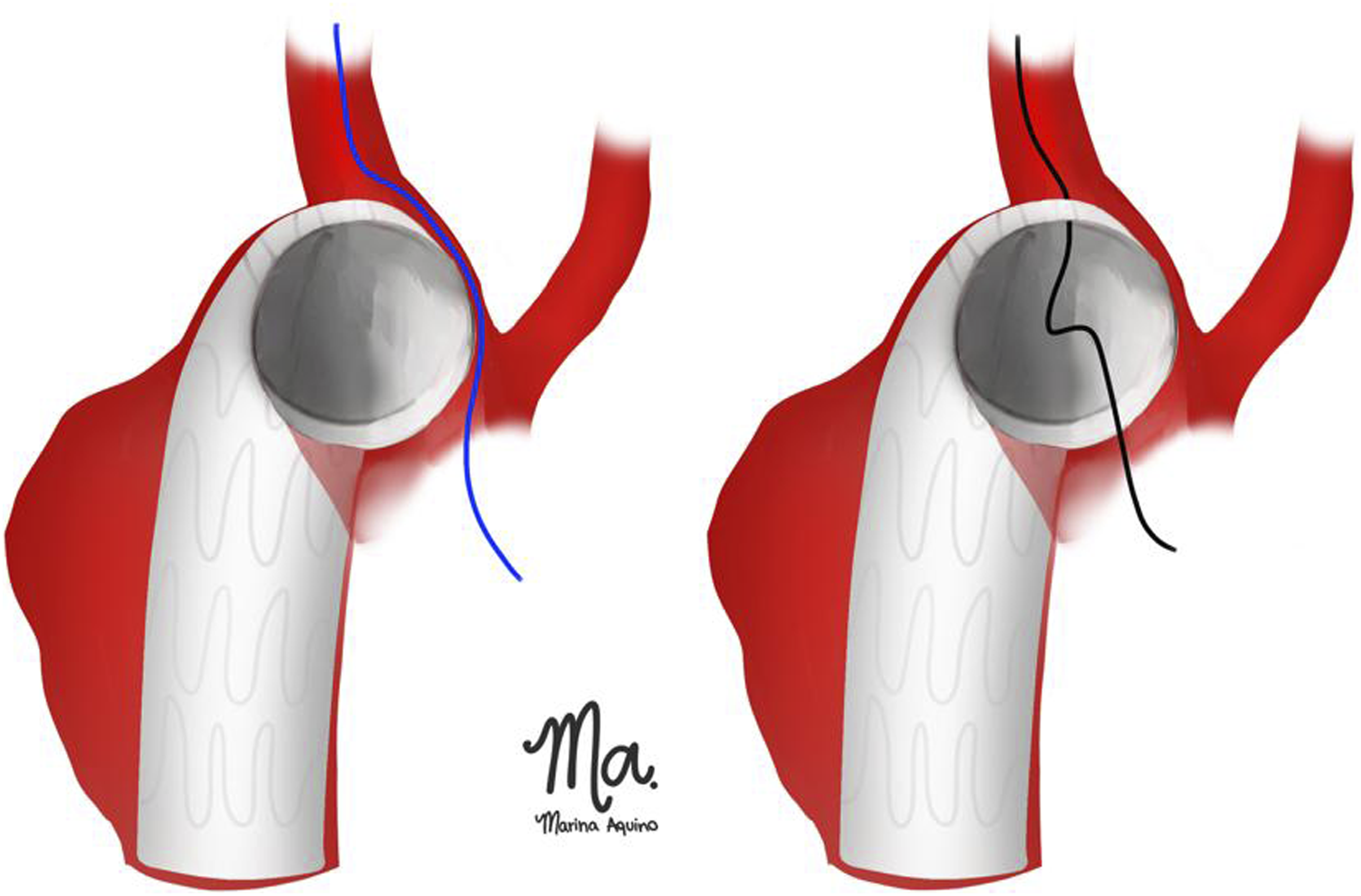
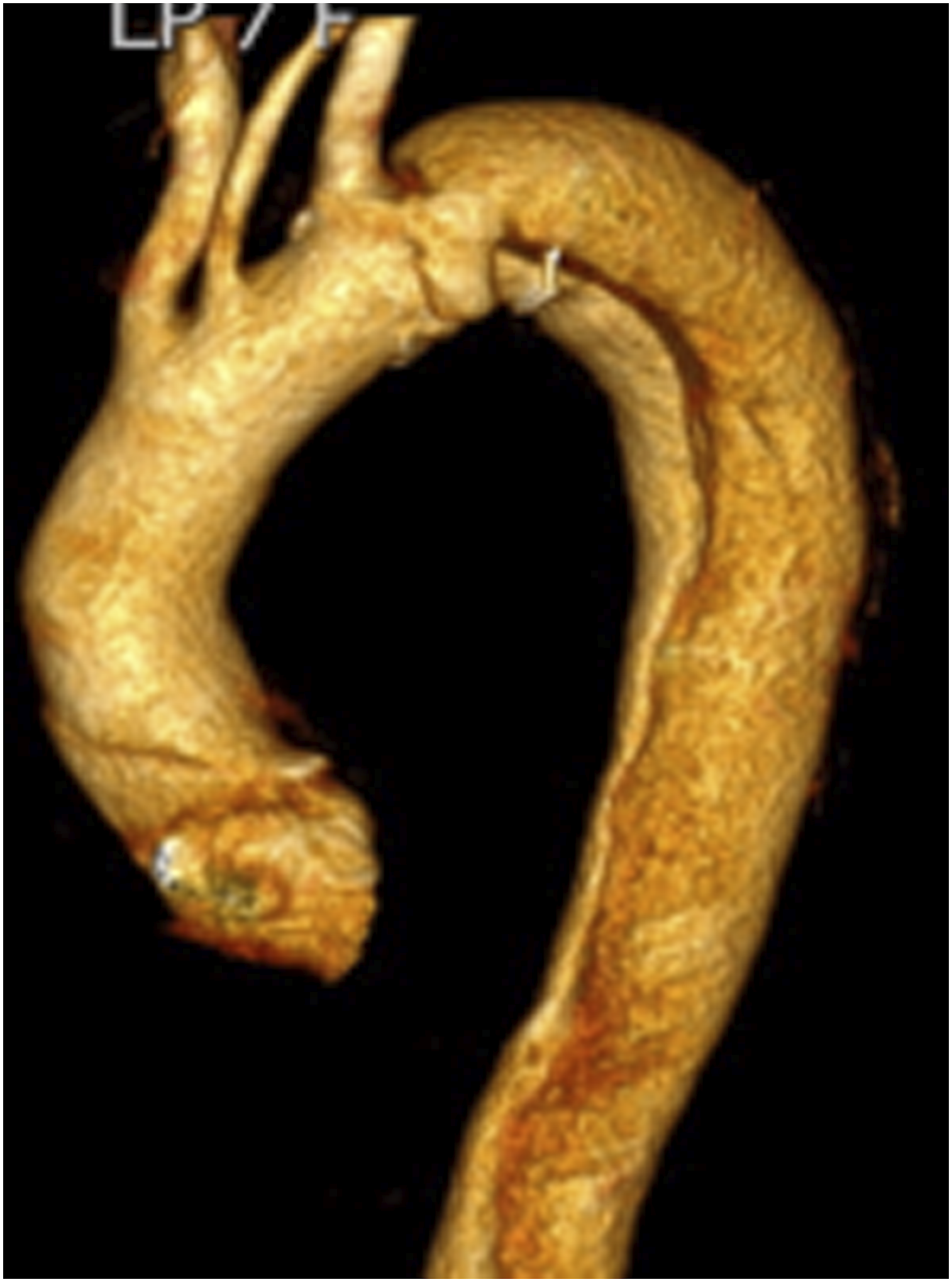
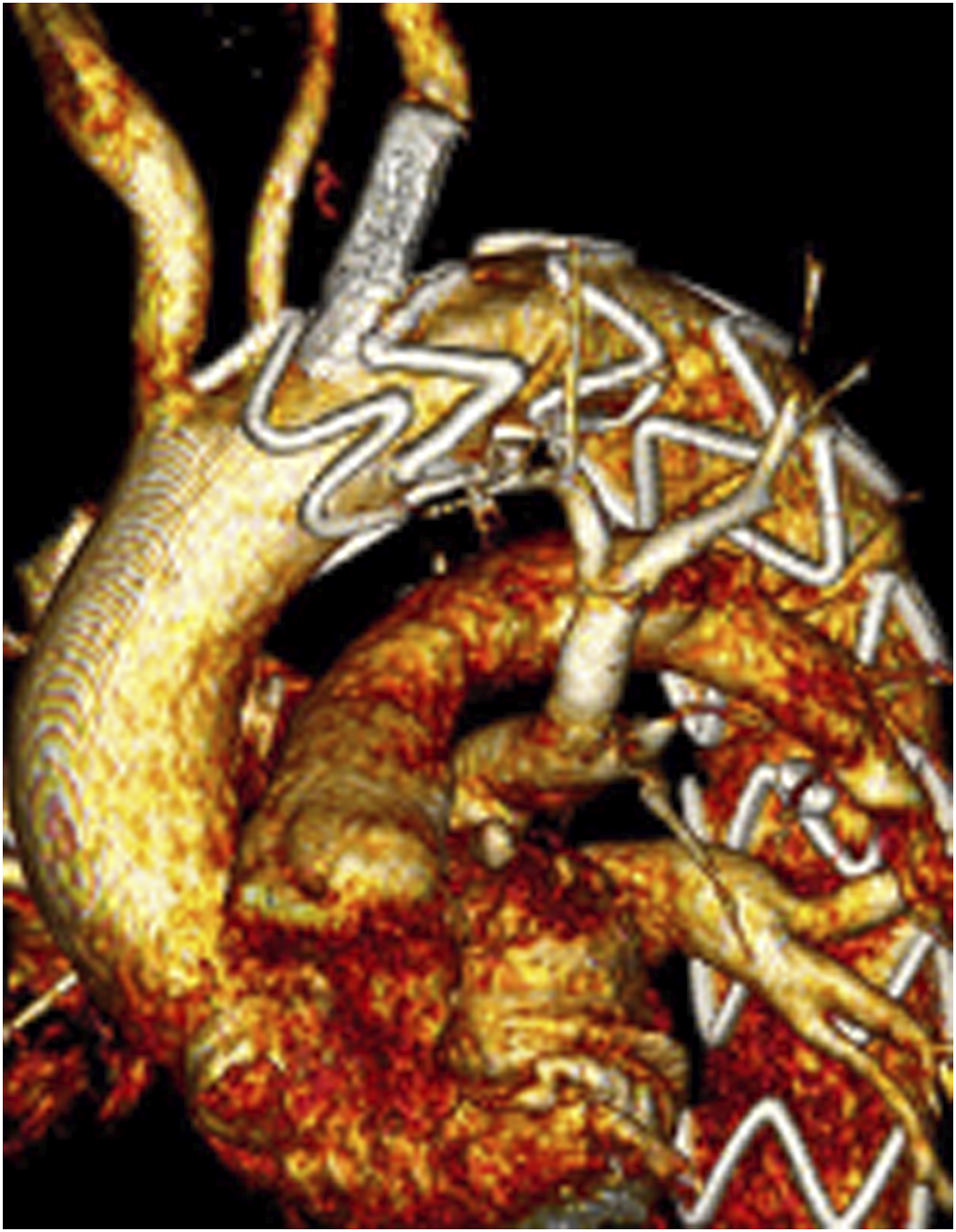
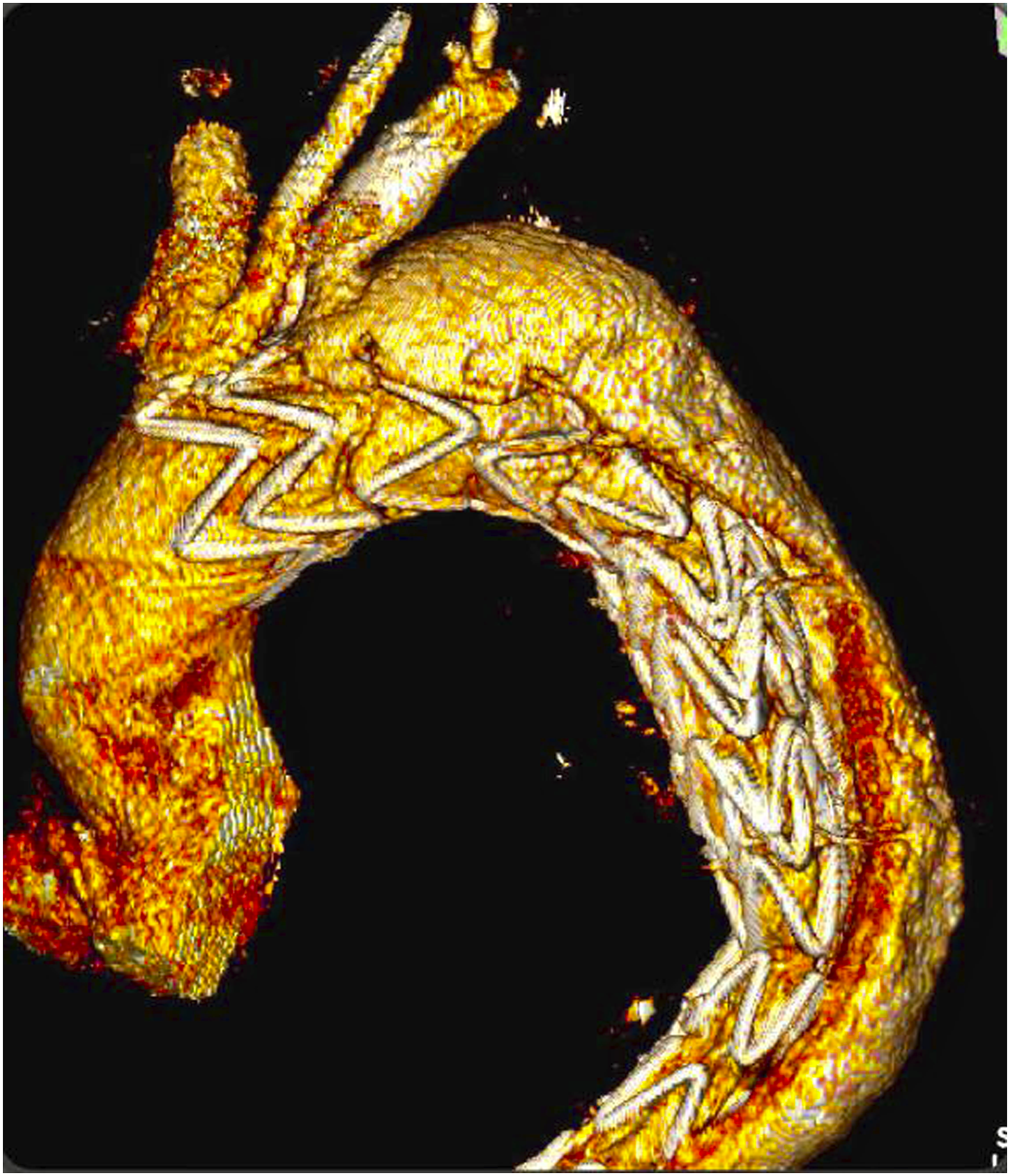
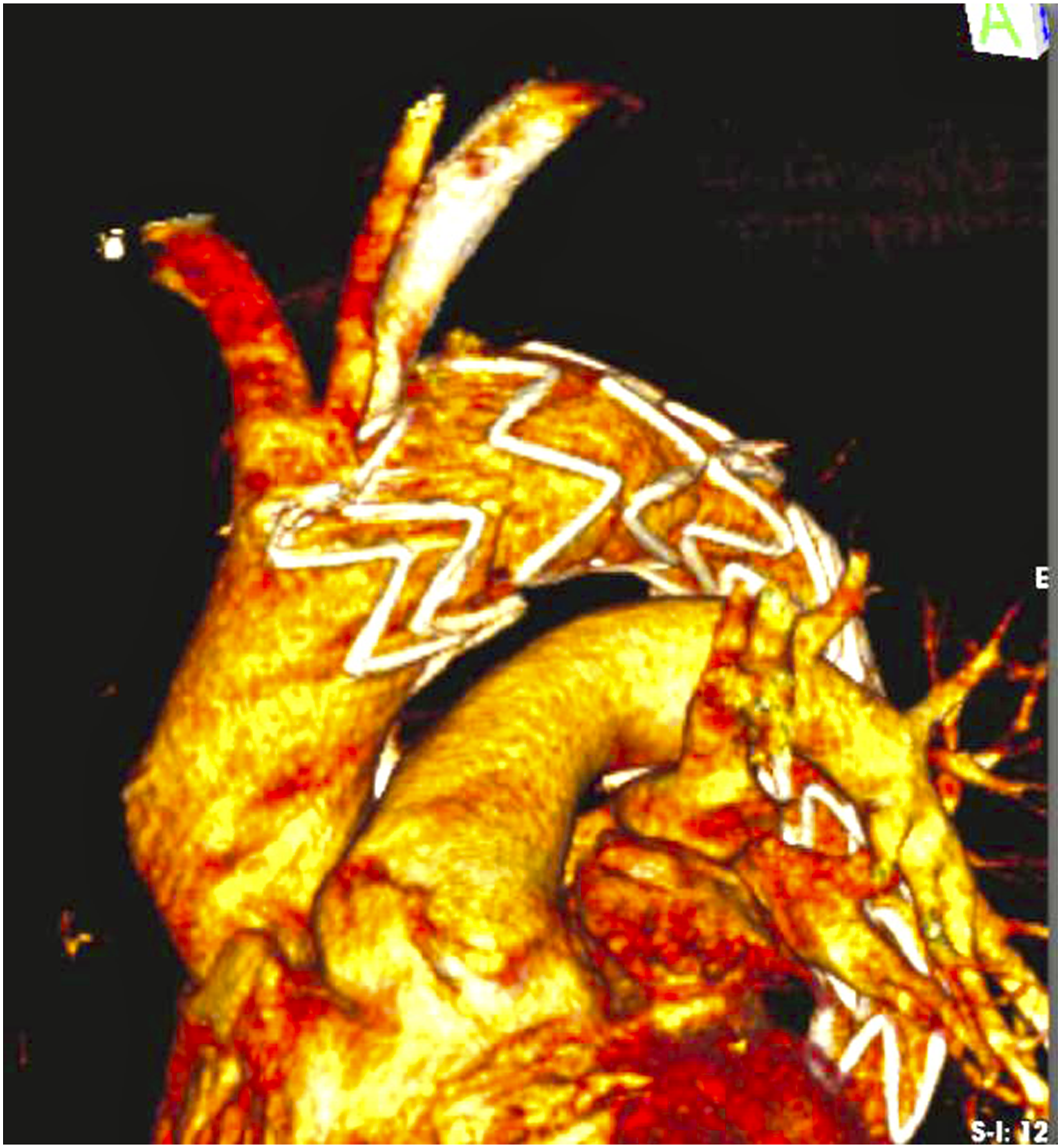
We performed control CTA at 3, 6, and 12 months after the procedure and, from 12 months onwards, CTs were performed annually. The clinical parameter to assess left subclavian stent patency was the presence of a brachial pulse associated with blood pressure measurement, compared with the right upper limb, in addition to tomographic control. Patients were maintained on dual antiplatelet therapy for 6 months; after this period, patients were descaled to single antiplatelet therapy. Pre and postoperative CTA images are shown in Figures 6–8. Control CTA performed 24 months after the procedure, displaying a well-positioned stent without endoleaks. 3D Reconstruction of preoperative CTA. 3D Reconstruction of postoperative CTA after 24 months.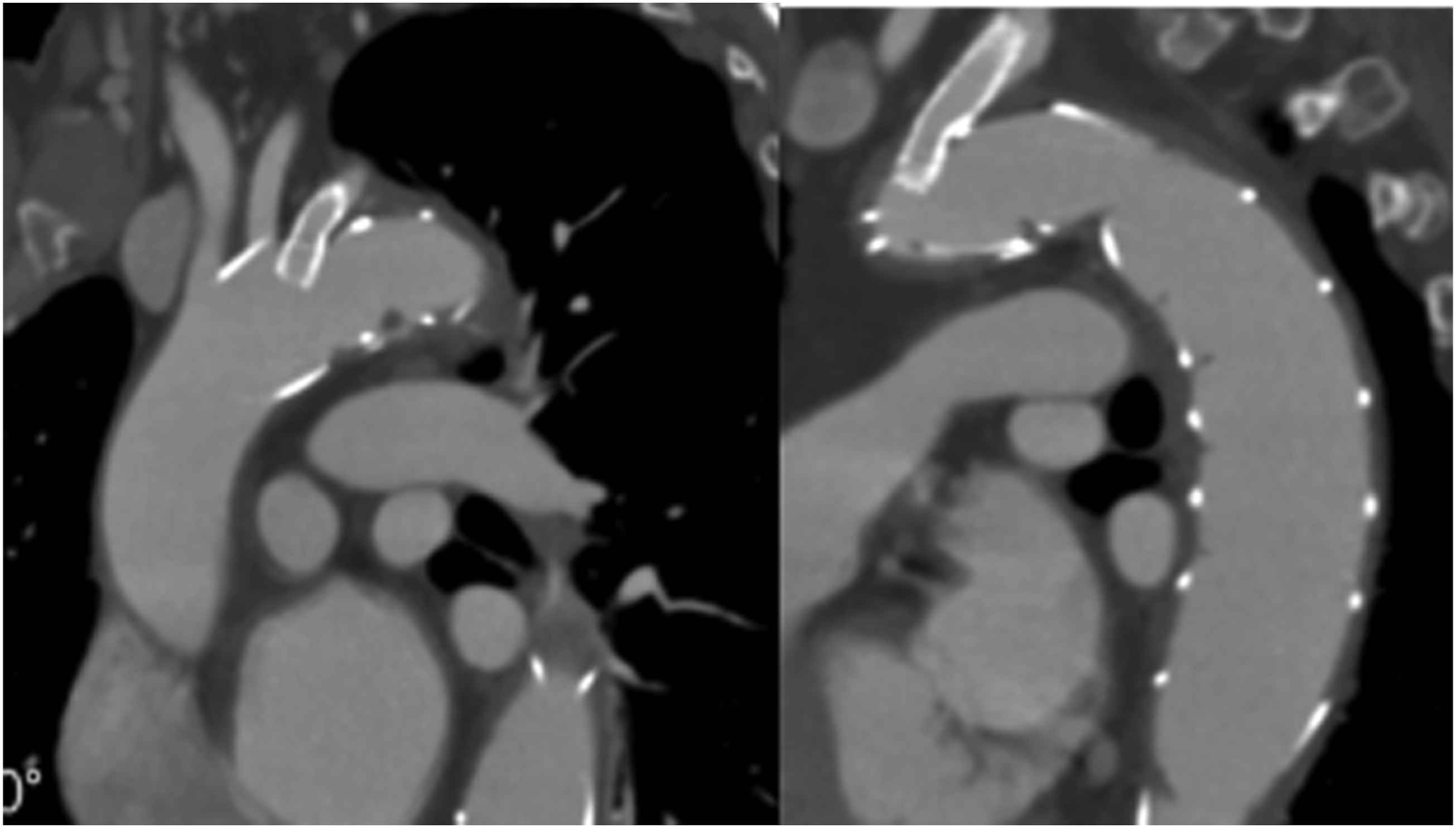
Results
Patient demographic data, aortic condition, anchorage zones, devices used, stents, and types of fenestrae performed during the study.
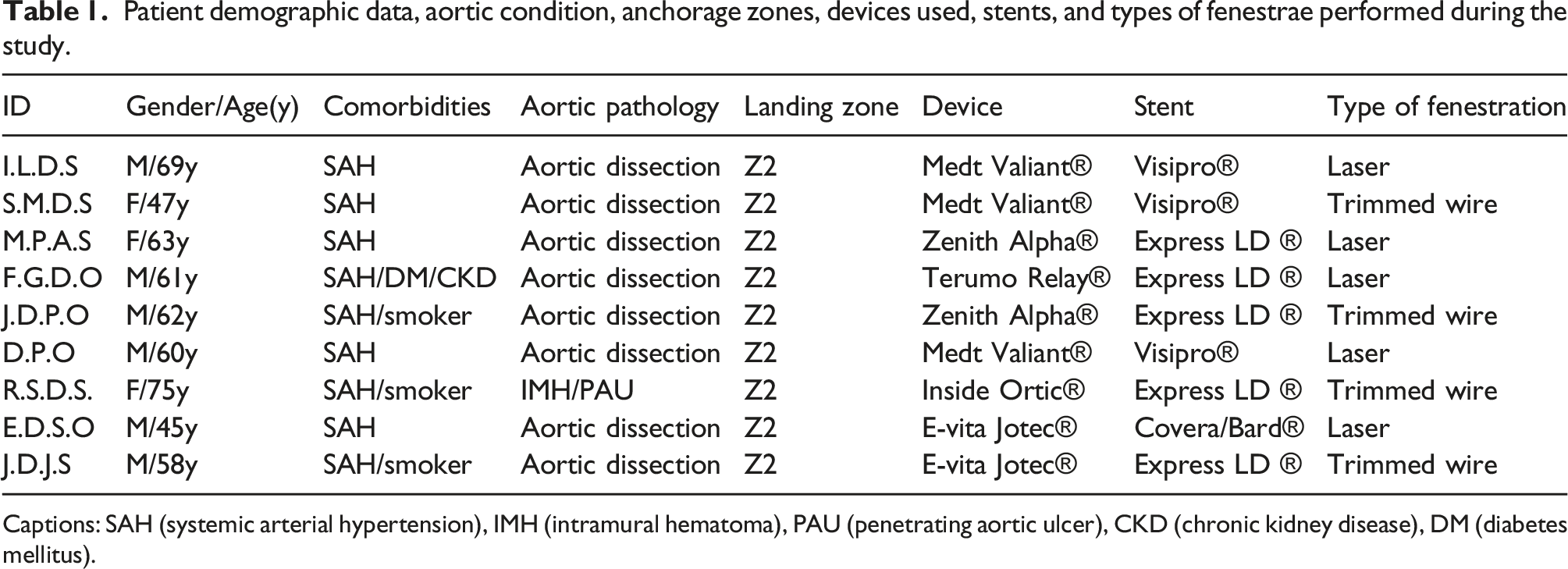
Captions: SAH (systemic arterial hypertension), IMH (intramural hematoma), PAU (penetrating aortic ulcer), CKD (chronic kidney disease), DM (diabetes mellitus).
Of the 11 patients eligible for the ISF procedure, 9 were successful, with a technical success rate of 81%. The 2 failures that occurred in the attempt of in situ fenestration were due to significant tortuosity in the ostium of the left subclavian artery (LSA), not allowing proper positioning of the catheter to perform the fenestra. Patient follow-up time was between 6 and 24 months. In the analysis of demographic data, in relation to sex, there were 7 men and 4 women. Systemic arterial hypertension was the most prevalent condition, being present in all patients. The mean age was 60 years (45–75 years).
Regarding the aortic conditions presented, 10 were cases of aortic dissection and 1 was a case of intramural hematoma associated with penetrating aortic ulcer.
All fenestrations were performed for the left subclavian artery (LSA), with endoprosthesis anchorage in zone 2; in the 2 cases in which fenestration was not possible (due to significant tortuosity in the ostium of the left subclavian artery), the parallel stent graft technique was chosen.
No patient had a type 1A endoleak related to fenestration. There was complete thrombosis of the false lumen in the thoracic aorta in 7 patients (77%, 7 of 9 cases), being more common in cases with aortic dissection treated in the subacute phase. In 2 patients, there was retrograde false lumen refill seen on 3-month control CTA; in one of them, spontaneous thrombosis of the false lumen occurred and in another, an additional endograft was needed in a distal segment to close a large reentry orifice of the thoracic aorta. There was one case of type 1C endoleak portrayed on the 12-month control CTA, unrelated to the fenestra orifice in the endoprosthesis tissue; the extravasation was distal to the stent implanted in the LSA. A new coated balloon-expandable stent with the Flare technique was implanted at the distal end of the stent, stopping the endoleak (as seen in Figures 9–12). There were no cases of LSA stent occlusion or endoleak related to tissue damage caused by fenestration (type 3). Angiography showing endoleak 1C unrelated to the fenestra orifice in the endoprosthesis tissue (distal to the stent implanted in the LSA). Postoperative control angiography showing treated endoleak 1C (implant new coated balloon-expandable stent with the Flare technique at the distal end of the stent). 3D Reconstruction of 12-month control CTA showing endoleak 1C. 3D Reconstruction of postoperative CTA after 13 months (1 month after solving endoleak 1C).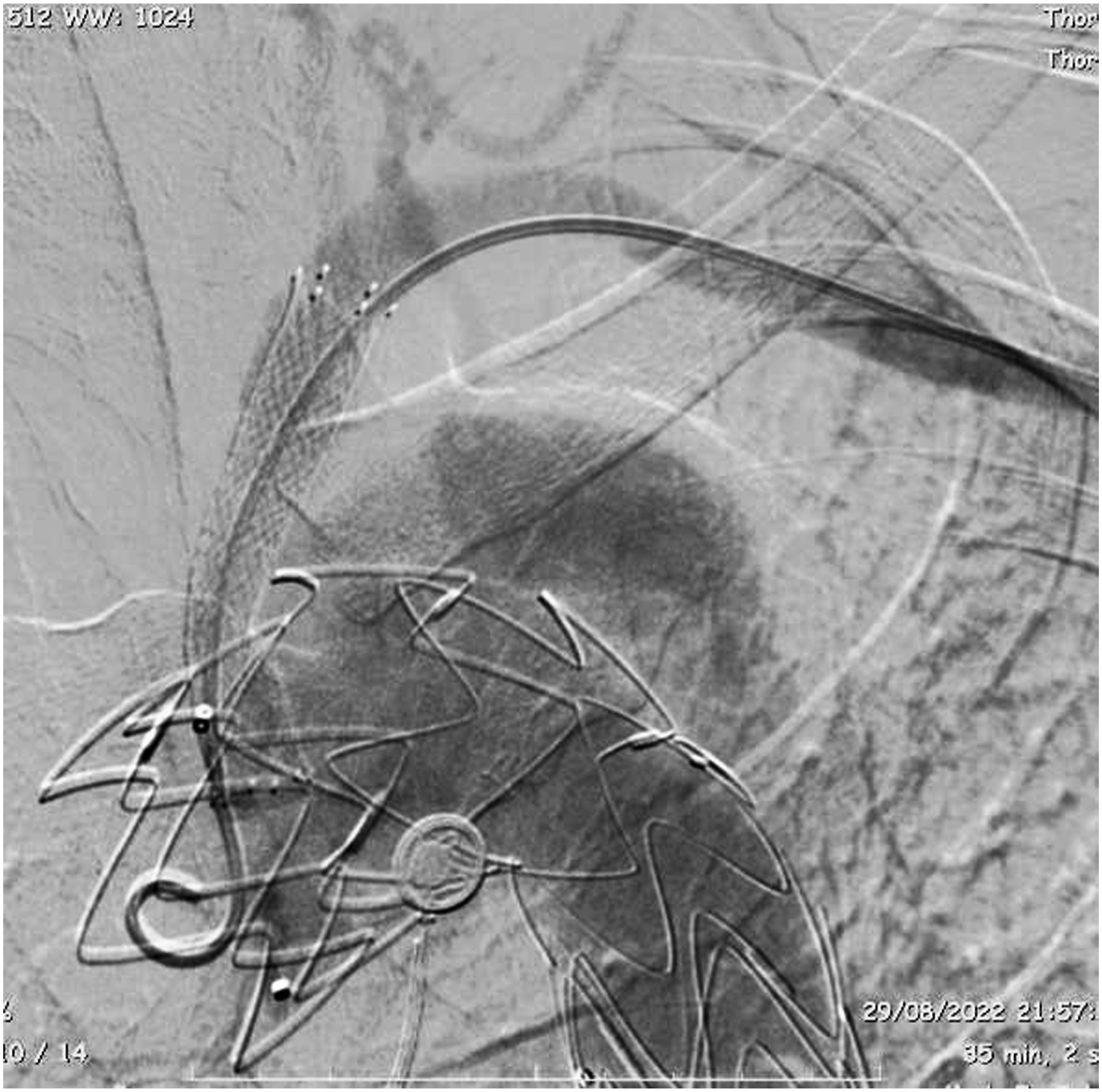

One patient developed thrombosis of the left brachial artery on the first day after the procedure and underwent thrombectomy and left upper limb revascularization without further complications. The fenestration was successful in this patient and the thrombosis probably occurred due to the thin caliber of the artery (3.8 mm) after passage of the 7f introducer sheath.
There was no case of stroke or paraplegia in the whole series; in our department, CSF drainage is performed on demand and not as a routine.
One death was reported during the series, due to case of COVID-19 acquired after the procedure, and therefore not related to the fenestration technique.
Discussion
Aortic arch diseases are a major challenge for vascular surgeons. Several techniques such as customized endoprostheses, bench fenestrations, and parallel stent grafts have been performed over the years with the aim of preserving the supra-aortic trunks. Although they are the gold standard, in our reality, customized endoprostheses have a high cost and long manufacturing time—on average 6 months to be available for use.
The specialized center where the study was carried out is accredited to the Brazilian public health system, where, sometimes, there is a financial limitation of materials, and it is not always possible to perform the gold standard treatment for complex pathologies of the aorta.
The first in situ fenestration technique for the LSA was described in 2004 by Mcwilliams 9 where ISF was performed on a Cook® device, with technical success. In the last 5 years, there has been a progressive increase in publications on this topic. Most, however, are meta-analyses with few prospective studies. In addition, we did not find in the literature studies with long-term follow-ups, the largest of which was 56 months of follow-up.
In 2016, a systematic review was carried out including 44 patients and 46 fenestrae, of which 42 were retrograde and 4 anterograde. As a result, there were 2 complications related to vascular accesses, 4 type 1C endoleaks related to the fenestrae, in addition to 1 case of paraplegia and 2 deaths, unrelated to the procedure, therefore, suggesting that this is a feasible and effective method to extend the anchorage zone, preferentially recommending the energy-based fenestra (laser or radiofrequency). 1 However, in our study, the type 1C endoleak was not related to the orifice of the fenestra, even though cases where a fenestration technique was performed with a guide wire trimmed in a bevel were included.
In 2017, another review was published comparing ISF with the parallel stent graft technique. In all, there were 85 cases, 67 of which were Chimney stent techniques and 18 ISF, with 100% technical success and an average follow-up of 38 months. The study had a mortality of 3.6%, all in the chimney stent group, not related to the procedure. Primary patency was 98.8% in the chimney stent group x 98.5% in the ISF group. A 1 A endoleak was identified in the chimney stent group. This review does not suggest superiority between techniques; however, it raises the hypothesis that ISF may represent a more favorable option, especially among aortic dissections. 10
The first case performed at HGRS was described in August 2020, a female patient with subacute aortic dissection with an entry hole in a tight left subclavian position, making it impossible to implant the endoprosthesis in zone 3. The procedure was performed using a Zenit Alpha endoprosthesis (Cook®). This patient has been followed up for approximately 2 years, with the last 24-month CT angiography conveying the sustained complete thrombosis of the false lumen in the thoracic aorta, patent stent and no signs of 1A or 1C endoleaks, suggesting what is seen in the main literature reviews: ISF as a technique with good short- and medium-term durability.1,11
Regarding the lining tissue of the endoprosthesis, there was no difference between PTFE and polyester, but only one of the procedures was performed with a PTFE prosthesis and, therefore, it is not possible to suggest the superiority of this device.
Although the ISF technique is feasible and has shown good technical success, some steps cannot be left undone, specifically the correct positioning of the angiograph into AP position after fenestration in order to confirm that the guidewire is inside the endoprosthesis and not in a path parallel to the device.
In fact, the long-term durability of unreinforced fenestrae is still controversial. Prospective studies and long-term series are still scarce in the literature, which is why we aimed to report our current work. As for the device used for fenestration, the laser cuts the tissue more linearly, which may favor greater durability of the fenestra when compared to perforation with a guide wire trimmed into a bevel.10,11 Therefore, our preference is always for the laser when available as opposed to the guide wire trimmed into a bevel, as we agree with the current literature that laser provides a more linear cut in the endograft tissue.
Conclusion
Diseases involving the aortic arch remain a major challenge for endovascular treatment. In the absence of dedicated devices, in urgent cases, ISF is a safe option for the treatment of complex aortic lesions. The case series described depicts ISF as feasible and with a high rate of technical success and good results in the short and medium term. Prospective studies with long-term clinical follow-up are still needed to fully assess the durability of these unreinforced fenestrations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.