
Abstract
Purpose
The worst complication during cannulation of the contralateral gate during complex endovascular aortic repair is deployment of the limb extension behind the main graft body.
Case report
A patient with a 5.7 cm juxtarenal abdominal aortic aneurysm was taken to the operating room for fenestrated endovascular aortic repair and iliac branch device. Percutaneous femoral access was used to deploy a Gore Iliac Branch Endoprosthesis, followed by a physician modified Cook Alpha thoracic stent graft with four fenestrations. Next a Gore Excluder was deployed to bridge the fenestrated component to the iliac branch and native left common iliac artery creating distal seal. Due to the severe tortuosity, a buddy wire technique, using a stiff lunderquist wire, was used to cannulate the contralateral gate. Unfortunately, after cannulation, the limb was advanced over the buddy lunderquist wire instead of the luminal wire. We used a backtable modified guide catheter to provide the necessary pushability to navigate wires between the aberrantly deployed limb extension and the iliac branch device. Using through-and-through access, we then successfully deployed a parallel flared limb in the correct plane.
Conclusion
Careful communication, wire marking, and attention to intraoperative flow can minimize risks of complication, but knowledge of bail out techniques remains imperative.
Keywords
Introduction
The treatment of complex aortic disease via endovascular methods can present unique challenges. One challenging point intraoperatively remains canulating the contralateral gate after deployment of the main body of the graft. The worst complication when this is not done successfully is deployment of the limb extension behind the main body graft. 1 Techniques demonstrated in few case reports demonstrating salvage techniques often occur during the treatment of occlusive disease but involve contralateral wire access that is used to navigate between the maldeployed stent and arterial wall to obtain through-and-through femoral-to-femoral wire access to deploy the parallel stent.2–5 There are few cases when this occurs for the treatment of aneurysmal disease, and no reported cases for techniques involving complex aortic disease where fenestrated grafts and iliac branch devices are involved. Each case does remain independent and presents its own unique challenges. Here we present a case from our large academic institution involving the inadvertent deployment of a limb extension during complex endovascular reconstruction of a patient with a juxtarenal abdominal aortic aneurysm requiring physician modified endograft and iliac branch device, and technique for success placement of a parallel limb extension. IRB approval for the review and presentation of this case report was not required, and appropriate informed consent was obtained from the patient prior to publication.
Case report
The patient was a 74-year-old gentleman who was initially referred to our Vascular Surgery clinic for evaluation of abdominal aortic aneurysm. He had a past medical history of significant COPD and longstanding smoking history. He had been admitted previously with significant respiratory complications associated with his COPD and was taking home inhalers. Additional medical history included hypertension, CKD, GERD, BPH, and arthritis. CT angiography demonstrated a 5.7-cm juxta renal abdominal aortic aneurysm and 3.1-cm right common iliac artery aneurysm (Figure 1). Given the size of the patient’s aneurysm, as well as his significant respiratory comorbidities, the decision was made to take the patient to the operating room for fenestrated endovascular aortic repair paired with an iliac branch device on the right side for an associated iliac artery aneurysm. 3-D rendering of pre-operative CT angiography that demonstrates abdominal and iliac portions of the patient’s aneurysm.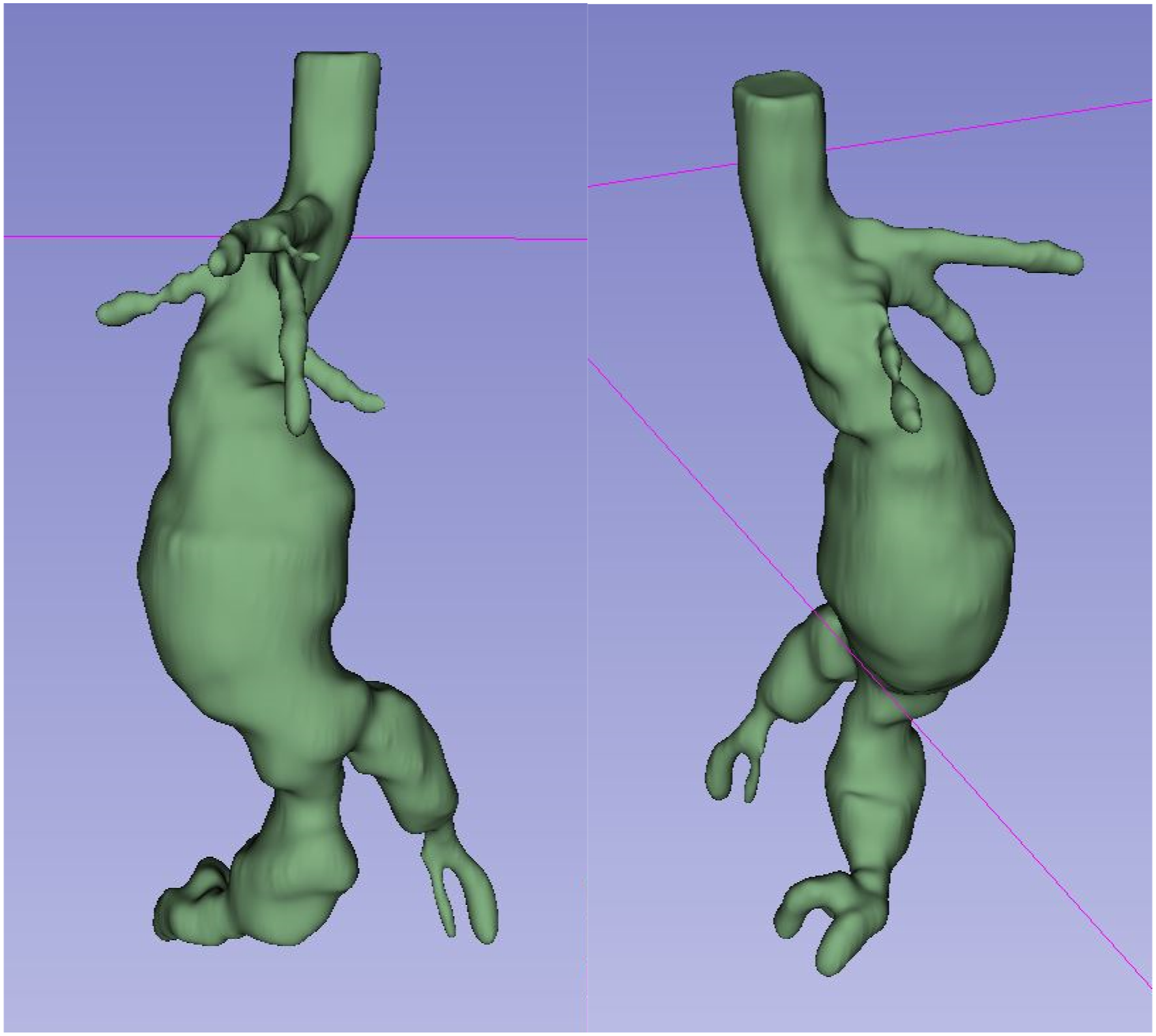
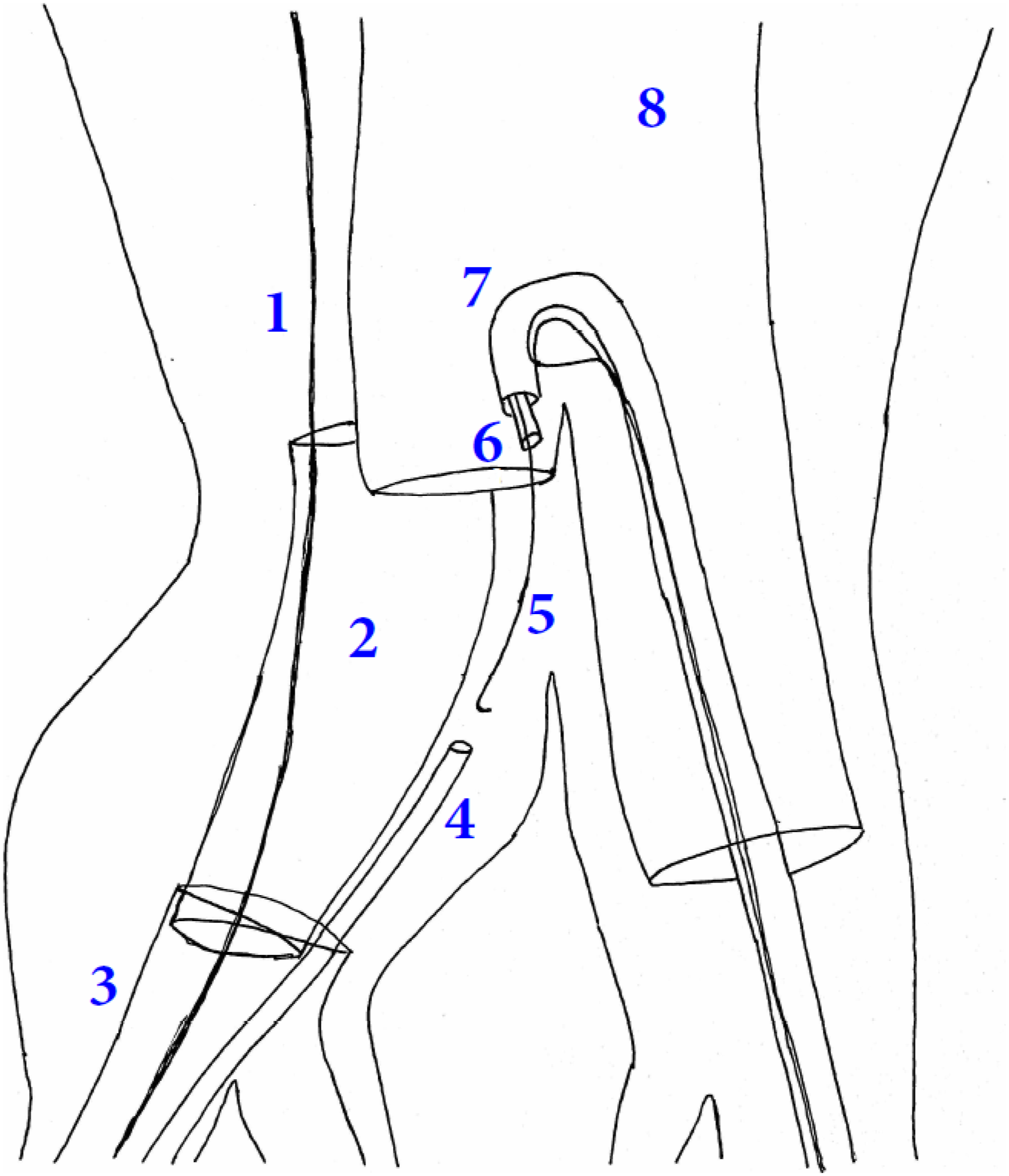
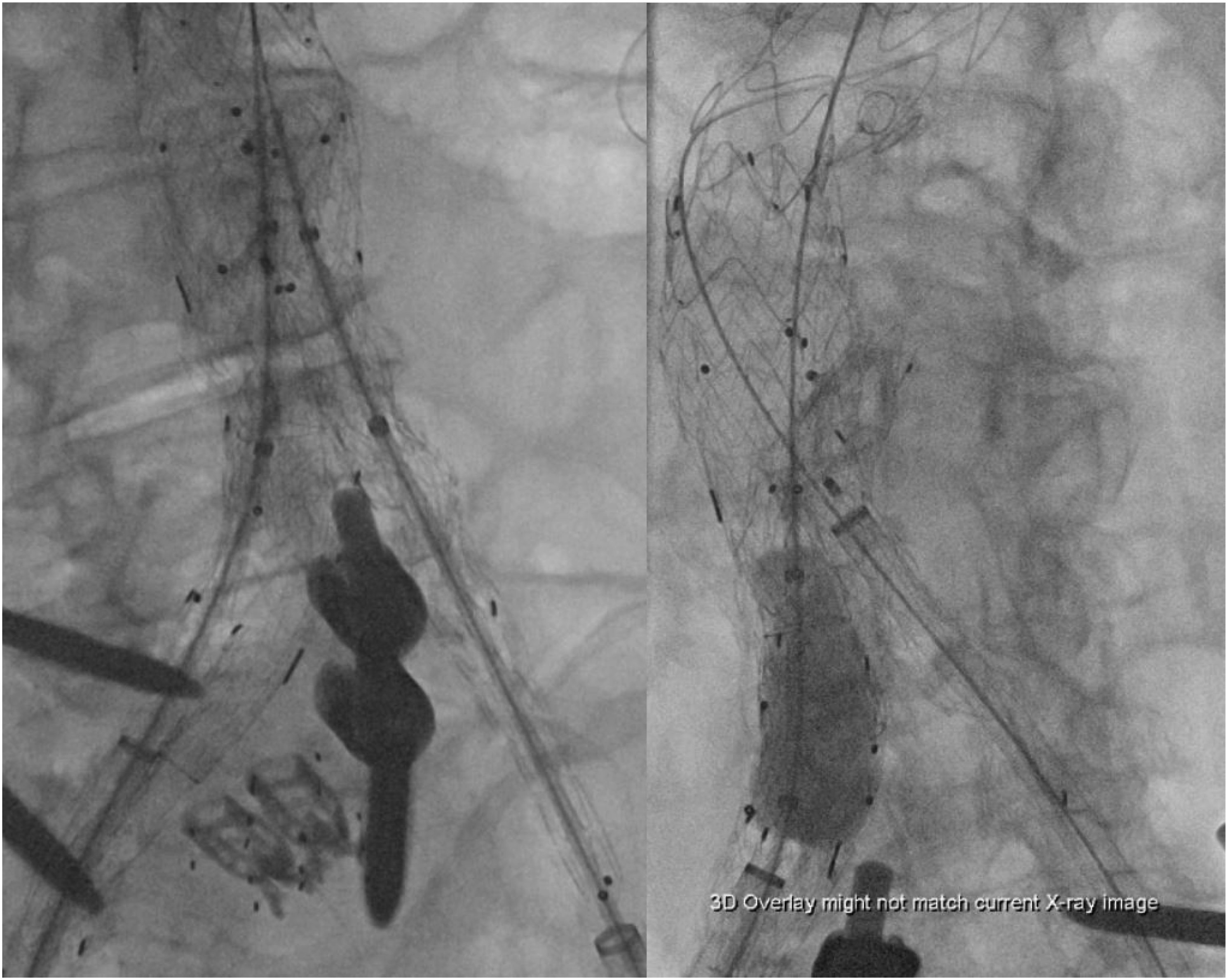
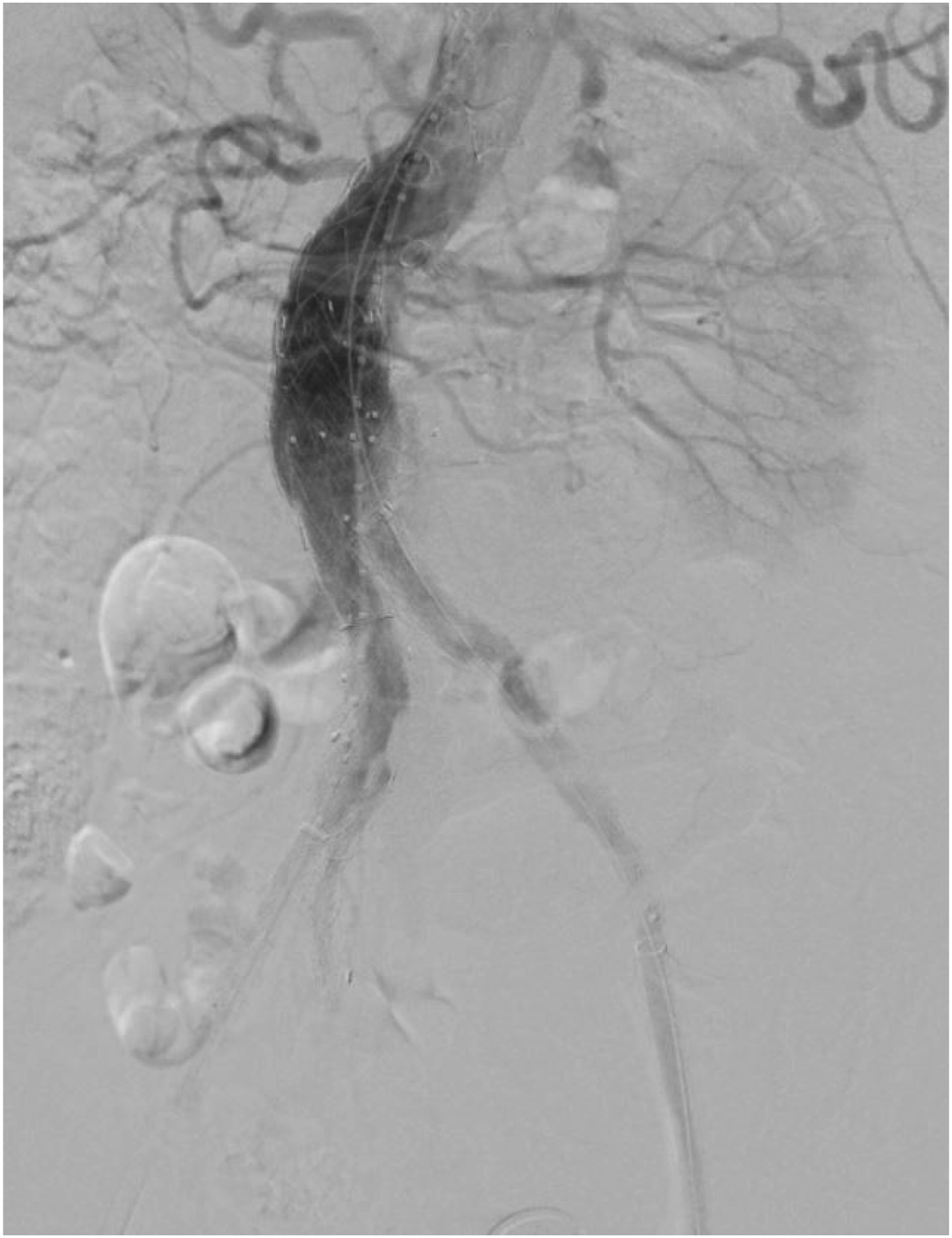
After placement of the fenestrated stent graft, the right sided iliac branch device was deployed according to IFU. Via the left femoral access, the bridging bifurcated Gore Excluder graft was deployed just below the lowest renal fenestration with adequate overlap. Via the right femoral access, the gate was cannulated and confirmed via intravascular ultrasound. Of important note, in order to aid in cannulation a stiff lunderquist buddy wire had been left behind the bifurcated stent graft due to the significant aortic and iliac tortuosity. An appropriately sized flared limb extension was selected and deployed on this right side with the distal portion landing in the iliac branch device, removing the buddy wire prior to deployment. It was realized at this point that this had been aberrantly deployed behind the contralateral gate of the Gore Excluder due to loading it on the buddy wire rather than onto the wire that had been IVUS confirmed inside of the gate. To salvage the stent graft repair, we first attempted to cannulate from the contralateral side using a 6.5 Fr TourGuide sheath (Medtronic) with multiple wire and catheter combinations, but the sheath lacked sufficient support to advance catheters alongside the maldeployed limb, kicking up into the aorta with each attempt. Having exhausted most options prior to converting to a cross femoral bypass, we modified an 8 Fr MP1 guidecatheter (Boston Scientific) (Figure 2) by making two side wall holes using an 18-gauge needle. One hole was at the distal end, and one a few centimeters proximal. The modified system was then created by passing a V14 wire antegrade through the guidecatheter, out the distal hole, in the proximal hole, and then retrograde out the end of the guidecatheter. This created a steerable catheter that would have more support to maintain its reverse curve. We advanced this steerable catheter up the left sided femoral access and used it to direct wires access down the contralateral gate. Utilizing a 2.6 CXI catheter and 0.018″ stiff angled glide wire nested within this steerable catheter, we were able to navigate wires between the aberrantly deployed limb extension and the iliac branch device. After successfully getting though, we externalized the wire out the right femoral access and using this strong support were able to advance a lunderquist wire from the right femoral access alongside the maldeployed limb into the gate over which a new flared limb was deployed in proper position. (Figures 3 and 4). Alignment was confirmed with intravascular ultrasound and secured with Coda balloon post-dilation. Using a 22 mm Amplatzer plug, the origin of the maldeployed iliac limb extension was embolized to prevent endoleak. Completion angiography confirmed exclusion (Figure 5). Modified steerable catheter design. Depiction of modified guidecatheter used to navigate over the Gore Excluder flow divider and down the contralateral gate, offering access to further navigate between the aberrantly deployed limb extension and the iliac branch device. (1) stiff support wire, (2) maldeployed limb extension, (3) iliac branch device, (4) access sheath. (5) 0.018 Glide Advantage wire, (6) 2.6 CXI catheter, (7) modified steerable catheter, (8) main graft body. Stiff wire secured and snared up into the lumen of the Gore Excluder and thoracic stent grafts (left), and effective deployment of a new limb extension for salvage of the endovascular repair (right). Completion angiography.
The patient did well post-operatively with no complications associated with lower extremity perfusion. Surveillance CT angiography performed post-operatively demonstrated patent repair with no endoleak and effectively excluded maldeployed limb extension (Figure 6). 3-D reconstruction of post-operative CT angiography demonstrating appropriate exclusion of the maldeployed right sided iliac limb extension.
Discussion
The deployment of the iliac limb extension occurred after we inadvertently removed the stiff intraluminal wire and instead deployed the extension over a wire that had been left behind the thoracic and abdominal stent grafts that had already been deployed. We had left a buddy wire up behind the thoracic and abdominal grafts that we intended to remove prior to deployment of the iliac limb extension, but instead we removed the intraluminal wire. This error can occur with difficult cannulation of the short limb of the bifurcated aortic graft. 6 Understanding the different techniques that can be used to salvage an endovascular repair when this occurs is important. The techniques published previously, as well as in this case, utilize through-and-through femoral wire access to provide leverage for advancing a parallel limb.2–4 In the case presented here, one important technical point was the use of the modified steerable sheath to provide support for maneuverability of wires through the challenging space between grafts. Open salvage is also an option in these cases, and techniques described include conversion to aorto-uni-iliac stent graft with femoral-femoral bypass, or embolization of the contralateral gate with femoral-femoral bypass. 4
Conclusion
In conclusion, successful endovascular salvage of maldeployed iliac limb extension can be achieved. During more complex aortic repairs, wire management with multiple visceral branch wires or buddy wires becomes an elevated skill. Careful communication, wire marking, and attention to intraoperative flow can minimize these risks but knowledge of bail out techniques remains imperative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.