
Abstract
Objective
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) is a resource-intensive approach for the management of refractory cardiogenic shock. Within this population exists a substantial cohort of patients with peripheral artery disease (PAD), which independently increases the risk of complications and all-cause mortality. We studied 10-year national trends of the impact of PAD among VA-ECMO recipients to better understand the prevalence of PAD and implications on outcomes in this vulnerable population.
Methods
This 10-year retrospective, propensity score-matched study identified all adult patients (≥18) who underwent VA-ECMO between 2009 and 2018, from a large US database (National Inpatient Sample). Patients with an ICD diagnosis of PAD were identified. The primary endpoints of in-hospital mortality, bleeding complications and major limb loss (above- or below-knee amputation) were compared between patients with PAD to those without.
Results
A total of 6768 patients were identified, of which 342 (5.3%) had PAD. The median age at admission was significantly higher in PAD patients [64 years vs. 55 years; p < .01], as was male gender [71% vs. 64%; p < .01]. Patients with PAD had higher rates of smoking (38.9% vs. 23.3%), hypertension (71.1% vs. 50%), diabetes (37.4% vs. 27.0%), chronic kidney disease (30.1% vs. 18.0%), coronary artery disease (76.0% vs. 35.0%) and dyslipidemia (76.0% vs. 35.0); all p < .01. After propensity-matching 2:1 for comorbidities, PAD patients were found to have significantly greater overall complications, including in-hospital mortality, bleeding, surgical wound infections, pseudoaneurysms, and major adverse limb events [71.9% vs. 63.9%; p < .01]. Subgroup analysis revealed greater in-hospital mortality [62.2% vs. 55.3%; p < .05], major amputations [4.1% vs. 0.3%; p < .01] and blood transfusions [32.2% vs. 26.2%; p < .05] in PAD patients. Over 2014–2018, the non-PAD group demonstrated statistically discernable trends in a 51.1% decrease in overall complications and a 28.1% increase in survival to discharge (all p < .01). Over the same time period the PAD cohort experienced a modest, nonsignificant, decrease in complications [7.0%, p = .40] and a decrease in those surviving to discharge [47.1% vs. 40.5%, p = .91].
Conclusion
Patients with PAD on VA-ECMO are sicker at baseline and experience significantly greater major amputations and higher in-hospital mortality. They have not benefitted from the considerable decrease in complication rates and increase in survival to discharge over time as compared to their non-PAD counterparts. These findings demonstrate the substantial frailty of the PAD population within an already high-risk cohort, and highlight the need for better procedural approaches and innovative technologies.
Keywords
Introduction
Venoarterial extracorporeal membrane oxygenation (VA-ECMO) represents the most resource-intensive and technically advanced form of intensive support for refractory cardiopulmonary shock. 1 Although advances in ICU care and ECMO pump engineering has allowed for the evolution of cardiopulmonary bypass to leave the operating room, subject-specific anatomical and comorbid pathology frequently results in procedural complications, higher mortality, and the need for operative management.2–5 Thus, early identification of those at highest risk for complications is imperative to optimization of treatment paradigms.2,6
Within the population of patients experiencing cardiogenic shock and needing VA-ECMO support exists a substantial, understudied and high-risk cohort with concomitant peripheral artery disease (PAD). Both symptomatic and asymptomatic PAD are strong prospective predictors of cardiovascular morbidity and mortality, independent of other adjusted risk factors. 7 Patients with PAD are at a sixfold increased risk to die from cardiovascular disease as compared to patients without PAD. 8
Although it has been demonstrated that patients with PAD experience higher rates of certain complications associated with VA-ECMO, such as acute limb ischemia, the demographic composition, rate of overall complication and survival metrics in this cohort are ill-defined. 9 Importantly, while there have been trends toward improved morbidity and mortality in patients undergoing VA-ECMO over time, it is known if these improvements have reached the PAD cohort. 10
Given that PAD is endemic globally at >200 million worldwide, with a prevalence that is only increasing in our aging population, we aimed to study 10-year national trends using a large national database to understand the prevalence of PAD and its impact on outcomes among VA-ECMO recipients. 11
Methods
Data source, study population and comparison groups
This 10-year retrospective cohort analysis attained data from the National Inpatient Sample (NIS), which is maintained by the Agency for Healthcare Research and Quality as part of the Healthcare Cost and Utilization Project (HCUP). The data in the NIS are derived from a stratified sample of 20% of the discharges from all community hospitals in the US, and is estimated to account for a diverse range of 35% of all hospitalizations.
Adult patients ≥18 years of age from 2009 to 2018 were identified using the International Classification of Diseases, 9th (ICD-9) and 10th Editions (ICD-10) diagnosis codes for PAD with procedure codes for VA-ECMO. The control group comprised of adult VA-ECMO patients without a PAD diagnosis, and included patients from 2014 to 2018.
Records with missing outcomes were excluded from the analysis. The use of the NIS database was conformed to the data-use agreement from HCUP. This study met criteria for exemption under Tufts Medical Center’s Institutional Review Board.
Baseline variables
Demographic covariates included age at admission, sex and race. Relevant comorbid conditions were identified through ICD diagnosis codes (Supplemental Table 1) and included current or former tobacco use, hypertension (HTN), diabetes (DM), chronic kidney disease (CKD), coronary artery disease (CAD), chronic obstructive pulmonary disease (COPD) and dyslipidemia.
Study outcomes and definitions
Primary outcomes were in-hospital complications and survival to discharge. Bleeding complications were defined as separate outcomes either as a hematoma/hemorrhage requiring operative intervention for management, or need for blood transfusion. Major limb loss was defined as above-knee or below-knee amputation. Surgical complications included development of surgical site infections and arterial pseudoaneurysms.
Statistical analysis
Continuous variables were reported as mean (± standard deviation) or median (interquartile range) where appropriate while binary variables were expressed as a frequency (percentage). Demographics and comorbidities were compared between VA-ECMO patients with PAD to those without using a Student’s t test for continuous variables and Pearson chi-squared or Fisher’s exact tests for binary variables.
To compare complication rates between patients with PAD and those without, propensity-score matched groups between patients with PAD to patients without PAD were created at a ratio of 1:2, utilizing the nearest-neighbor method with a caliper of <0.15. Patients were matched for age, sex, race, DM, HTN, CKD, CAD, and dyslipidemia.
Temporal trends of events of overall complications over time were reported as absolute values for each calendar year and assessed for significance over time using a Cochran-Armitage test. All data extraction and analysis were performed using SPSS version 25.0 (IBM Corp., Armonk, NY) and JMP version 14.0 (SAS Institute Inc., Cary, NC) except PSM which was performed using R version 4.0.5 (https://www.r-project.org) via MatchIt package, version 4.1.0. Two-sided p value of <0.05 was used for statistical significance.
Results
Study population and demographics
Baseline demographics and comorbidities for the non-PAD and PAD groups (unmatched cohort).
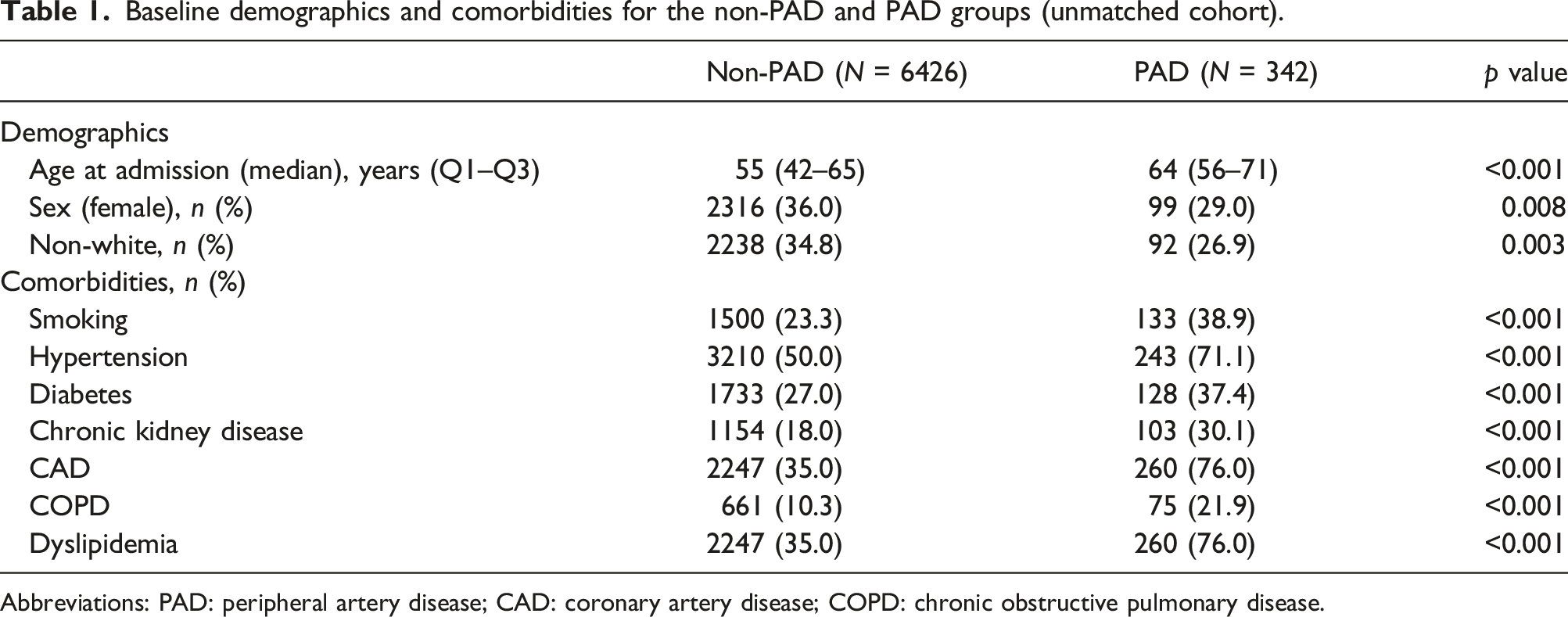
Abbreviations: PAD: peripheral artery disease; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease.
Comorbid conditions
Baseline demographics and comorbidities for the non-PAD and PAD groups (matched cohort) a .
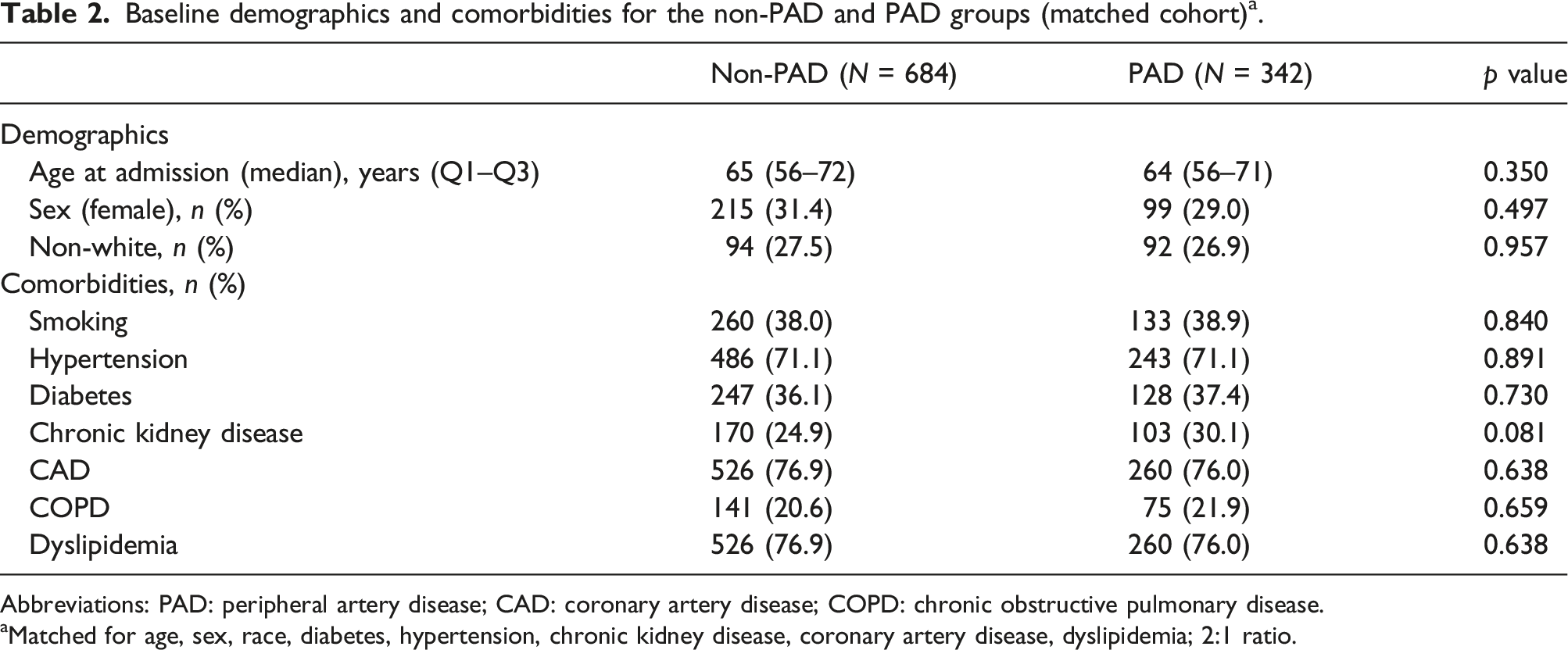
Abbreviations: PAD: peripheral artery disease; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease.
aMatched for age, sex, race, diabetes, hypertension, chronic kidney disease, coronary artery disease, dyslipidemia; 2:1 ratio.
In-hospital complications
To compare complications between patients with PAD to those without, propensity score-matching was performed 2:1 for relevant demographics and comorbid conditions resulting in 684 non-PAD VA-ECMO patients as compared to the 342 PAD VA-ECMO patients.
Outcomes following VA-ECMO initiation.
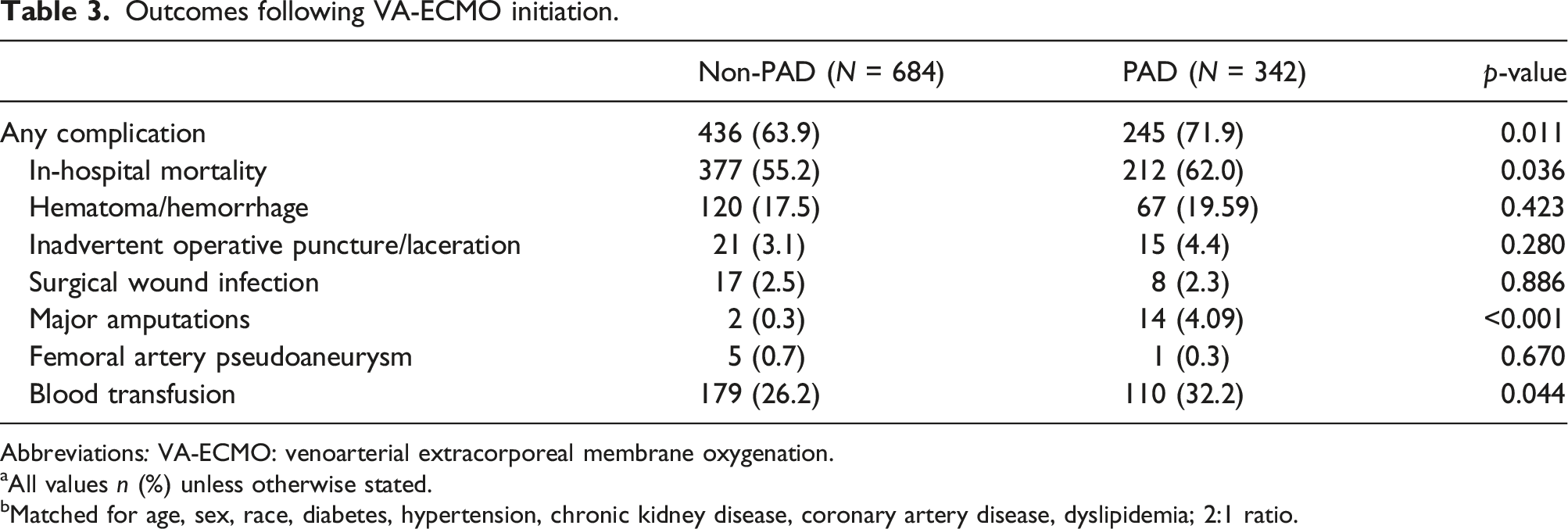
Abbreviations: VA-ECMO: venoarterial extracorporeal membrane oxygenation.
aAll values n (%) unless otherwise stated.
bMatched for age, sex, race, diabetes, hypertension, chronic kidney disease, coronary artery disease, dyslipidemia; 2:1 ratio.
Temporal trends
To assess for trends over time, complication rates and survival to discharge was assessed between 2014 and 2018. In the non-PAD group a notable trend toward improvement was found. Overall complications decreased at a statistically discernable rate in the non-PAD group by 28.2% from 79.3% in 2014 to 56.9% in 2018 [p < .01]. The PAD cohort experienced a modest, nonsignificant, decrease in complications over the same time period, with a 9.5% decrease from 73.5% in 2014 to 66.5% in 2018 [p = .40] (Figure 1). Trends in overall complication rates in VA-ECMO patients from 2014 through 2018 (matched cohort). Abbreviations: VA-ECMO: venoarterial extracorporeal membrane oxygenation; PAD: peripheral arterial disease.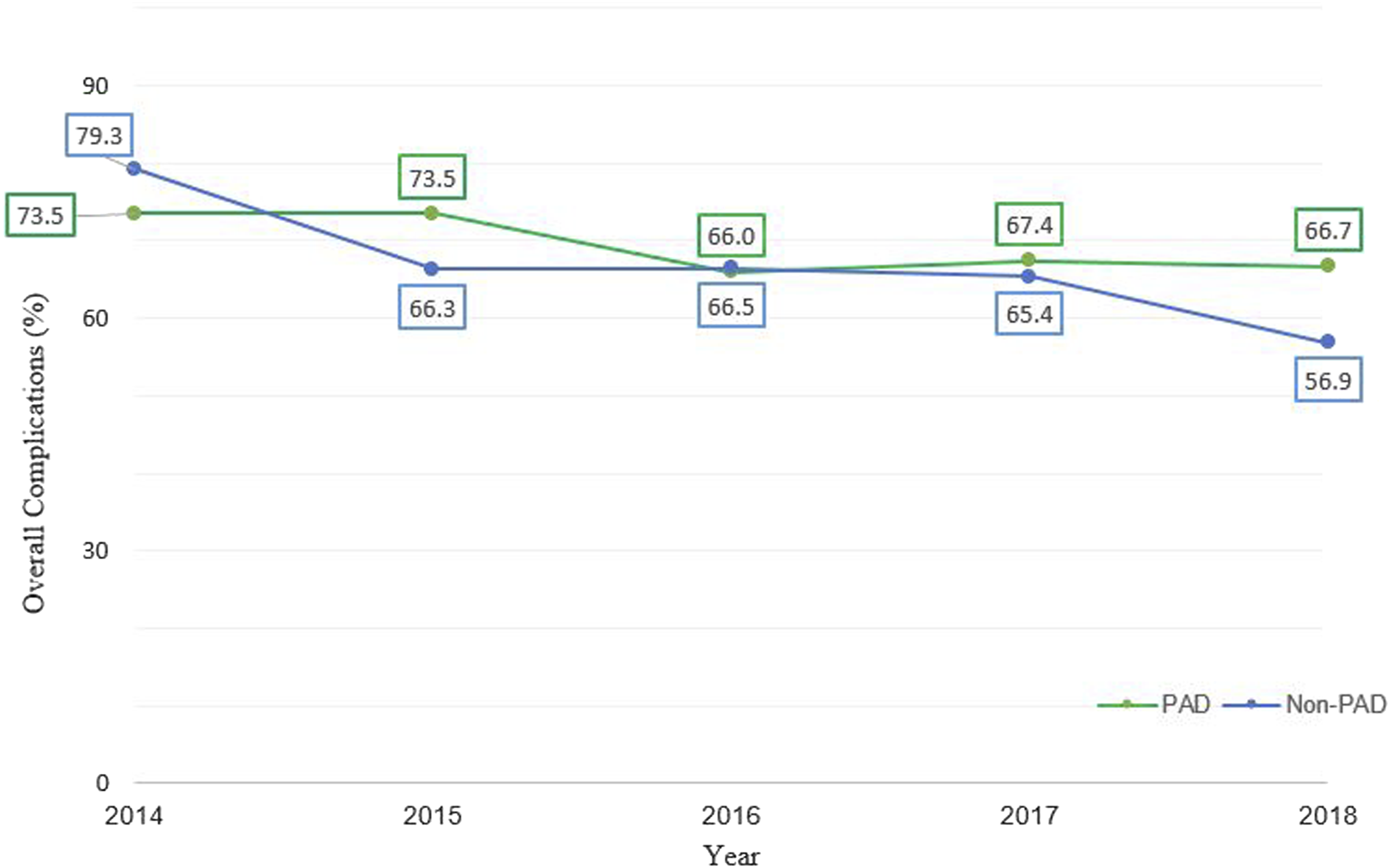
Assessment of those surviving to discharge revealed similar trends. In the non-PAD group patients on VA-ECMO experienced a 28.1% increase in survival to discharge from only 37.9% in 2014 as compared to 52.7% in 2018 [p < .01]. And although not significant, patients with PAD experienced a 14.0% decrease over the same time period, with 47.1% reaching survival to discharge in 2014 as compared to only 40.5% in 2018 [p = .91] (Figure 2). Trends in survival to discharge rates in VA-ECMO patients from 2014 through 2018 (matched cohort). Abbreviations: VA-ECMO: venoarterial extracorporeal membrane oxygenation; PAD: peripheral arterial disease.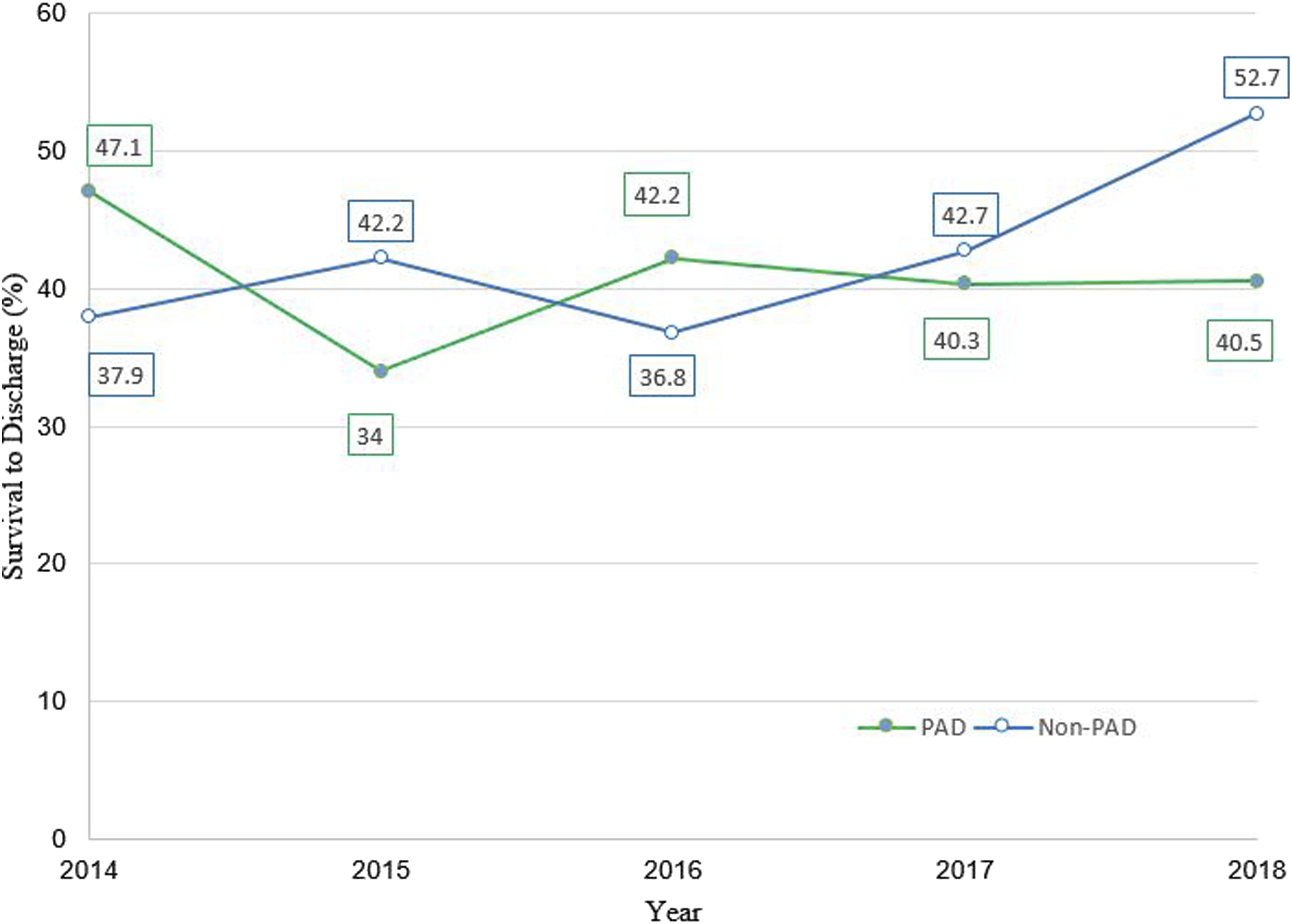
Discussion
We now report one of the largest analyses focused on the demographic and comorbid composition and in-hospital outcomes of VA-ECMO patients with concomitant PAD. Our data are consistent with what is known about PAD patients in general, in that these patients are typically older and sicker with higher rates of existing comorbid conditions such as smoking, hypertension, diabetes, chronic kidney disease, coronary artery disease, and dyslipidemia. 12
Similarly, we identified greater overall complications within the PAD cohort as compared to the non-PAD cohort, which is also typical in other types of procedural interventions for PAD patients such as non-vascular surgeries. 13 Patients with PAD undergoing VA-ECMO in this cohort were more likely to require blood transfusions, undergo major limb amputations and experience in-hospital mortality.
Bleeding is a common complication in patients with cardiogenic shock given the use of thrombolytics, anticoagulation, and antiplatelets for both treatment of inherent pathology and thromboprophylaxis when using large-bore catheters in VA-ECMO. 14 And transfusions are of significant interest in clinical outcomes for patients with myocardial infarction, with some data reporting increased 1-year mortality in transfusion recipients. 15 Our outcomes demonstrate that PAD patients underwent transfusions at a significantly higher rate (32.2% vs. 26.2%, p < .05), which may be largely attributed to a higher risk of access-site complications. 16
Acute limb ischemia and major amputations portends a poor outcome in VA-ECMO patients. 5 The nature of percutaneous mechanical support devices harbors a risk of acute limb ischemia given the increased utilization of femoral access, prolonged instrumentation, as well as the inherent vascoconstrictive state of multiorgan failure associated with cardiogenic shock.17–19 Yet, the stark difference between the PAD and non-PAD cohorts in terms of major amputation rates in this cohort at 4.1% vs. 0.3% (p < .01) prompts intentional considerations of both patient selection and arterial cannulation strategies.
Improvements in mortality for patients on VA-ECMO have dramatically improved over time, with percent survival being under 10% at the beginning of the millennia, and having increased to greater than 40% in recent years, reflecting a combination of technologic and procedural advancements. 20 Compared with surgical cannulation, for example, percutaneous ultrasound and fluoroscopic based endovascular approaches are associated with lower in-hospital mortality and fewer complications, and this modality has quickly become the technique of choice for many institutions. 21 Cannula engineering, such as coating with non-thrombogenic substances have vastly improved the inflammatory response formerly associated with circuit-surface interactions, and the transition to centrifugal pump systems have vastly increased the safety profile of the machine. 22 Our review of this large national database mirrors these promising improvements for patients managed with VA-ECMO in terms of a significant decrease in overall complications and a significant increase in survival to discharge over time. Yet PAD patients have not enjoyed these same benefits, with no significant decrease in complications and a trend towards decreased survival to discharge.
Our findings suggest that a deliberate focus on collaboration with vascular and peripheral intervention specialists combined with the pursuit of technologic advances that may avoid or mitigate the high anatomical risks inherent to the PAD population is integral to improving outcomes for PAD patients managed with VA-ECMO.
Limitations
The National Inpatient Sample database was chosen given its breadth, covering approximately 95% of the geographic United States with a large and diverse range of hospitalization data. However, unlike other vascular databases, sure as the Vascular Quality Initiative, it fails to capture certain vascular-specific diagnostics and outcomes. By relying on an admission ICD-classification diagnosis of PAD, instead of more inclusive metrics such as ankle-brachial indices, many patients with PAD may have been missed. A validation study of using ICD codes for the diagnosis of PAD found only a 34.7% highest sensitivity when compared with using an ABI <0.9 as the gold standard. 23
And as with any database study, there is a paucity of clinical detail when searching for outcomes. For example, while there were significantly greater transfusions in the PAD cohort as compared to the non-PAD cohort, in the real-world there is significant individual and institutional variability regarding transfusion thresholds. The NIS database does not provide any data or definitions with respect to transfusion thresholds. But it is our hope that the statistical significance of this outcome over a large number of patients supports this as an adequate marker for blood loss within this study population. In addition, the NIS focuses on inpatient data and thus readmissions and long term outcomes are missed. Similarly, the use of a registry to calculate complications is at risk of coding errors. 24 However, there is an absence of reporting bias in protocolized database collection. And given the large sample size we feel these limitations are counterbalanced in that we were able to answer important questions about this very high-risk cohort.
Conclusion
Using a large national database, our study demonstrated that patients with peripheral artery disease are older and sicker at baseline, and at risk of higher complications when undergoing VA-ECMO as compared to those patients without PAD. Most importantly, PAD patients have not enjoyed the same benefits of technologic and management advancements overtime, with a lack of improvement in morbidity and survival to discharge as compared to the non-PAD cohort.
Supplemental Material
Supplemental Material for - Peripheral artery disease and extracorporeal membrane oxygenation: Examining a high-risk cohort over time
Supplemental Material for Peripheral artery disease and extracorporeal membrane oxygenation: Examining a high-risk cohort over time by Khaled I Alnahhal, Monica Majumdar, Ali Irshad, Navin Kapur, Shivani Kumar, and Payam Salehi in Vascular.
Footnotes
Author contributions
KIA, MM, and PS were involved in study design, data collection, data analysis, and manuscript writing. MM, AI, NK, SK, and PS were involved in proof reading. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.