
Abstract
Objectives
We aimed to investigate Piezo1 expression in myofibroblasts in symptomatic and asymptomatic patients undergoing carotid endarterectomy and its relationship with atherosclerotic plaque formation.
Methods
This cross-sectional study analyzed carotid plaques of 17 randomly selected patients who underwent carotid endarterectomy from May 2015 to August 2017. In total, 51 sections (the most stenotic lesion, and the sections 5-mm proximal and distal) stained with hematoxylin-eosin and elastica-Masson were examined. Immunohistochemistry was performed using antibodies to Piezo1. The Piezo1 score of a section was calculated semiquantitatively, averaged across 30 randomly selected myofibroblasts in the fibrous cap of the plaque.
Results
Of 17 patients (mean age: 74.2 ± 7.1 years), 15 were men, 9 had diabetes mellitus, and 13 had hypertension. Symptomatic patients had higher mean Piezo1 score than asymptomatic patients (1.78 ± 0.23 vs 1.34 ± 0.17, p < .001). Univariate linear regression analyses suggested an association between plaque rupture, thin-cap fibroatheroma and microcalcifications and the Piezo1 score (p = .001, .008, and 0.003, respectively).
Conclusions
Increased Piezo1 expression of myofibroblasts may be associated with atherosclerotic carotid plaque instability. Further study is warranted to support this finding.
Introduction
A variety of physiological processes require the ability of cells to sense and respond to mechanical stimuli. 1 Previous studies reported that Piezo1 protein is a mechanically activated ion channel associated with mechanical forces, such as fluid shear stress and membrane stretch.2–4 The Piezo1 channel is a trimer with a central pore that is formed at the interface of its subunits,2,5 and it is gated directly by changes in membrane tension. 6 This channel is located in the plasma membrane and endoplasmic reticulum of vessel walls,3,7 where it senses and transduces mechanical forces.8,9
Myofibroblasts (MFBs), along with fibroblasts and smooth muscle cells, play an important role in the formation of atherosclerotic plaques, via secretion of components of the extracellular matrix, including collagens, proteoglycans, elastic fibers, a variety of glycoproteins, and hyaluronan. 10 A previous study suggested that the proliferation and apoptosis of MFBs along with the increased synthesis of type III collagen may be related to restenosis in peripheral artery disease. 11 He et al. showed that Piezo1 was overexpressed in MFBs in human and rat hypertrophic scar tissues; and mechanical forces, transduced via Piezo1, could promote hypertrophic scar formation. 12 They found that the application of GsMTx4, which is a Piezo1-blocking peptide, decreased excessive scarring in a stretch-induced rat tail model. Since the excessive increase of MFBs and fibroblasts in human artery is an important process in the atherosclerotic development, it is clinically significant to investigate the Piezo1 expression in human atherosclerotic plaques.
Among patients undergoing carotid endarterectomy (CEA), some pathological studies have indicated that those presenting with ischemic stroke or transient ischemic attack have more unstable plaque characteristics, such as plaque rupture, macrophage invasion, thin-cap fibroatheroma, and intraplaque microvessels.13–15 Consequently, there is a growing interest in the mechanisms involved in the development of atherosclerotic carotid arteries presenting with unstable plaque characteristics in humans. However, the expression of Piezo1 in MFBs in atherosclerotic plaques of patients with carotid artery stenosis has not been thoroughly elucidated yet.
Therefore, we conducted this study with the aim of investigating the expression of Piezo1 in MFBs in symptomatic and asymptomatic patients undergoing CEA.
Methods
Sample population
In this cross-sectional study, we retrospectively analyzed carotid plaques of 17 randomly selected patients (12 symptomatic and 5 asymptomatic) who underwent CEA from May 2015 to August 2017. Patients with missing data were excluded from the analysis. The indication for surgery was a recently symptomatic (<6 months) carotid artery with a 50%–99% North American Symptomatic Carotid Endarterectomy Trial (NASCET) stenosis, or an asymptomatic carotid artery with a 70%–99% stenosis. 16 Preoperatively, the degree of stenosis was evaluated by duplex ultrasound. Patients were classified as symptomatic if they had suffered an ischemic stroke or a transient ischemic attack. All patient details were de-identified in this study. Therefore, written informed consent was not obtained from them although they were informed of their entry into the study and were given the option to opt out. The study protocols were approved by the ethics committee of Hokkaido University Hospital (No. 16-036). Furthermore, this study complied with the Declaration of Helsinki on ethical principles for medical research involving human participants.
Histopathological examinations
CEA was performed under general anesthesia with routine patching and shunting, distal intimal tacking sutures, and minimal handling of the specimens. The plaques were removed en bloc, fixed in 10% buffered formalin, transected transversely into 5-mm specimens, and embedded in paraffin. After staining with hematoxylin-eosin and elastica-Masson, the most stenotic lesion, as well as the sections 5-mm proximal and distal to that lesion (3 sections per patient, 51 sections in total) were examined. The sections were examined by two independent observers, one of whom was an experienced histopathologist unaware of the clinical information. The sections were also immunohistochemically stained with anti-CD34 antibodies and primary antibodies for Piezo1 (Proteintech, Rosemont, IL).
Definitions of histopathological characteristics and semi-quantification for Piezo1-antibody staining of myofibroblasts
Plaque rupture is an area of fibrous cap disruption, where the underlying necrotic core is exposed to the vessel lumen. 17 Plaque erosion is an area of luminal thrombi that is not in continuity with the necrotic core. 17 A calcified nodule is a plaque with luminal thrombi containing a calcific nodule protruding into the vessel lumen, accompanying fibrous cap disruption. 17 Foamy macrophages within the cap are the aggregation of foam cells in the fibrous cap of the intima. In thin-cap fibroatheroma, the fibrous cap is <65 μm thick. 18 Intraplaque hemorrhage is an area with microscopically visible red blood cells and fibrins inside the plaque. Intraplaque microvessels refer to neovascularization in a carotid plaque. Nodular calcifications are fragmented calcium components that are separated by fibrin. 19 Microcalcifications are calcifications of 0.5–15 μm in diameter. 20
The Piezo score was calculated as a semi-quantitative measurement of Piezo1 expression in MFBs. Specifically, Piezo1-antibody staining of each MFB was semiquantitatively scored as none (=0); positive but weaker staining than that of resident macrophages (=1); positive staining equal to that of resident macrophages (=2); or positive and stronger staining than that of resident macrophages (=3). For such scoring, we used cross-sectional images of the lesions, with resident macrophages stained with Piezo1-antibody as internal controls (Figure 1). The Piezo1 score of each section was calculated as the average score of 30 randomly selected MFBs in the fibrous cap. Semi-quantitative determination of Piezo1 expression in myofibroblasts. Resident macrophages stained with Piezo1-antibodies were used as internal controls (arrow). The following scores were assigned: A, score = 0, no staining; B, score = 1, positive but weaker than the staining of resident macrophages; C, score = 2, positive staining equal to that of resident macrophages; and D, score = 3, positive and stronger staining than that of resident macrophages.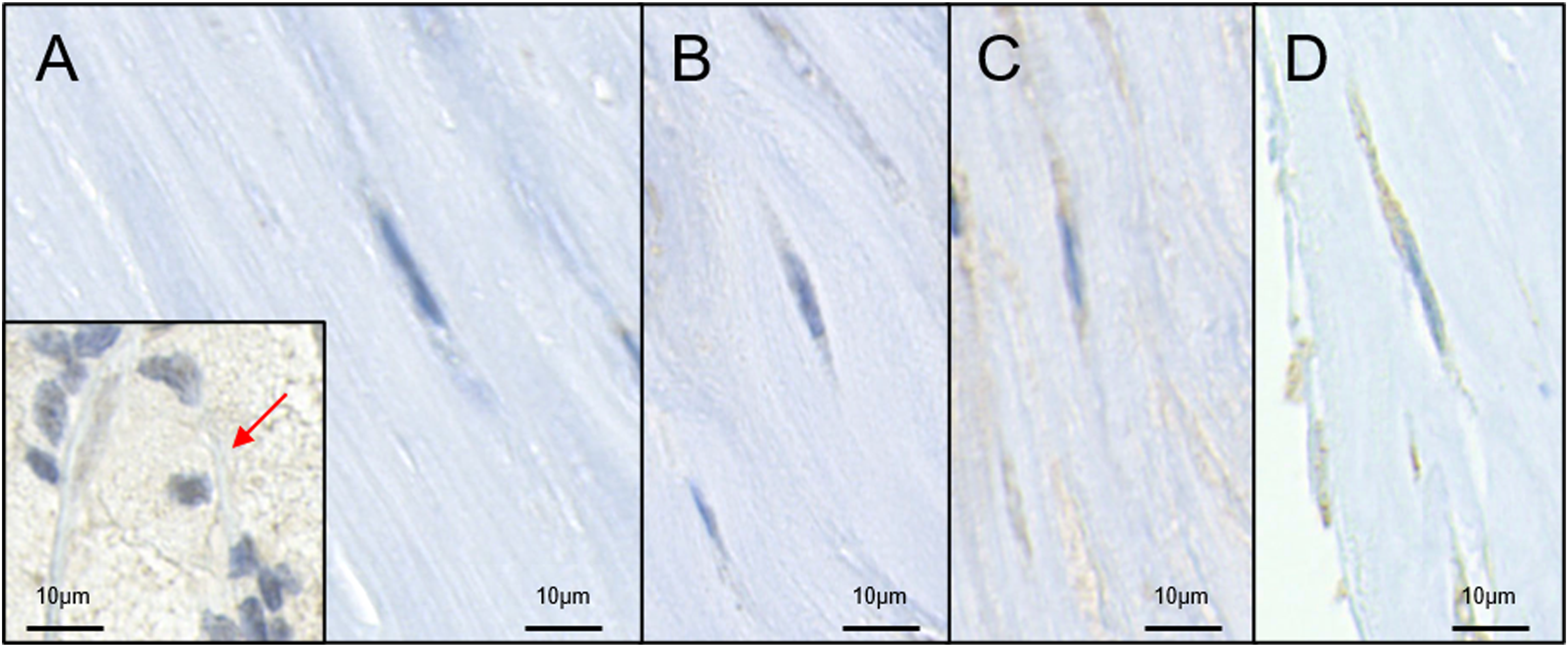
Statistical analyses
Results are presented as means ± standard deviations when normally distributed and as medians and interquartile ranges when non-normally distributed. Between-group differences were analyzed using the Pearson chi-square test or Fisher’s exact test for categorical variables and the Student t test or Mann–Whitney U test for continuous variables, as appropriate. Univariate linear regression analysis was performed to explore the factors associated with the Piezo1 score. All tests were two-tailed, and a p-value <.05 was considered statistically significant. All analyses were performed using Stata IC version 16 (StataCorp, College Station, TX).
Results
Clinical characteristics
Clinical characteristics.
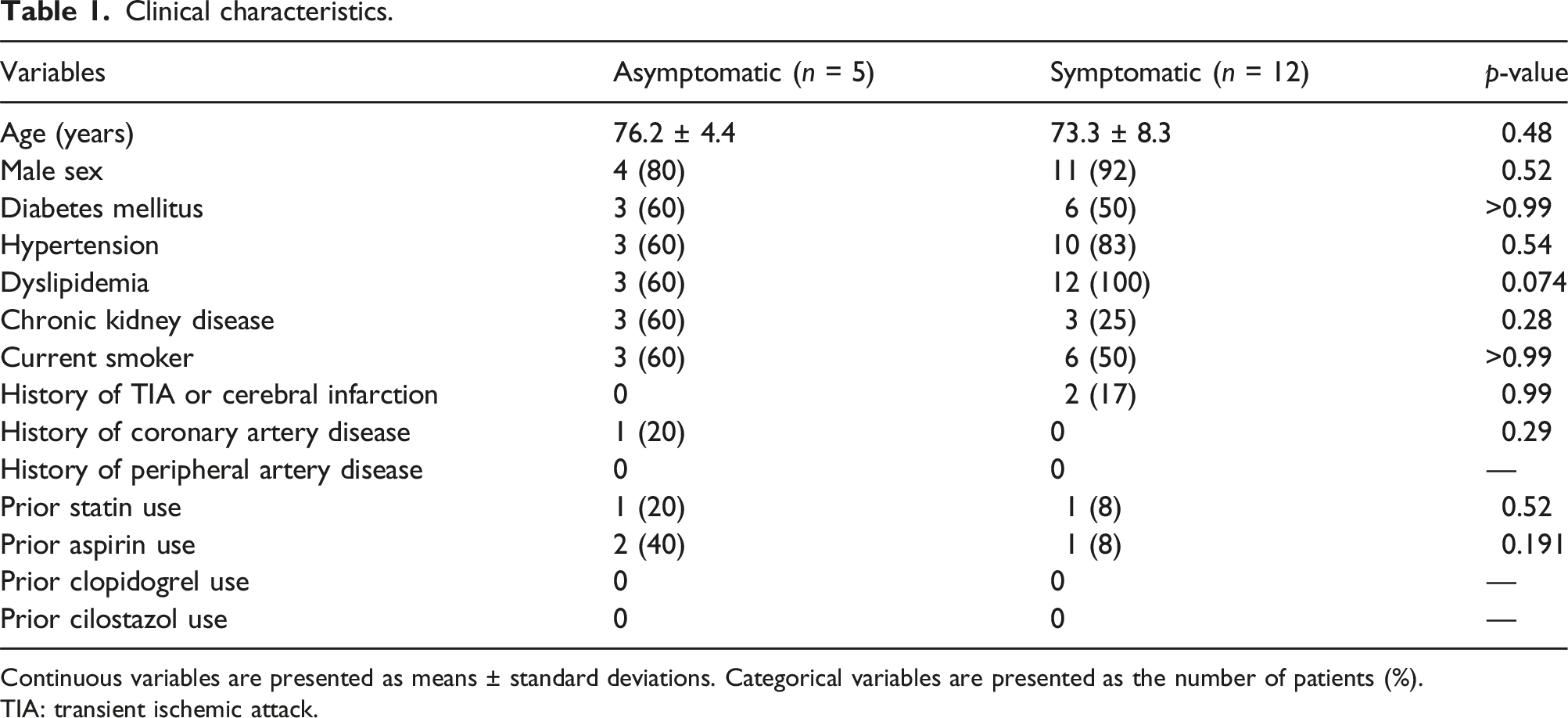
Continuous variables are presented as means ± standard deviations. Categorical variables are presented as the number of patients (%).
TIA: transient ischemic attack.
Pathological characteristics of carotid artery plaques
Pathological characteristics of plaques derived from patients undergoing carotid endarterectomy.
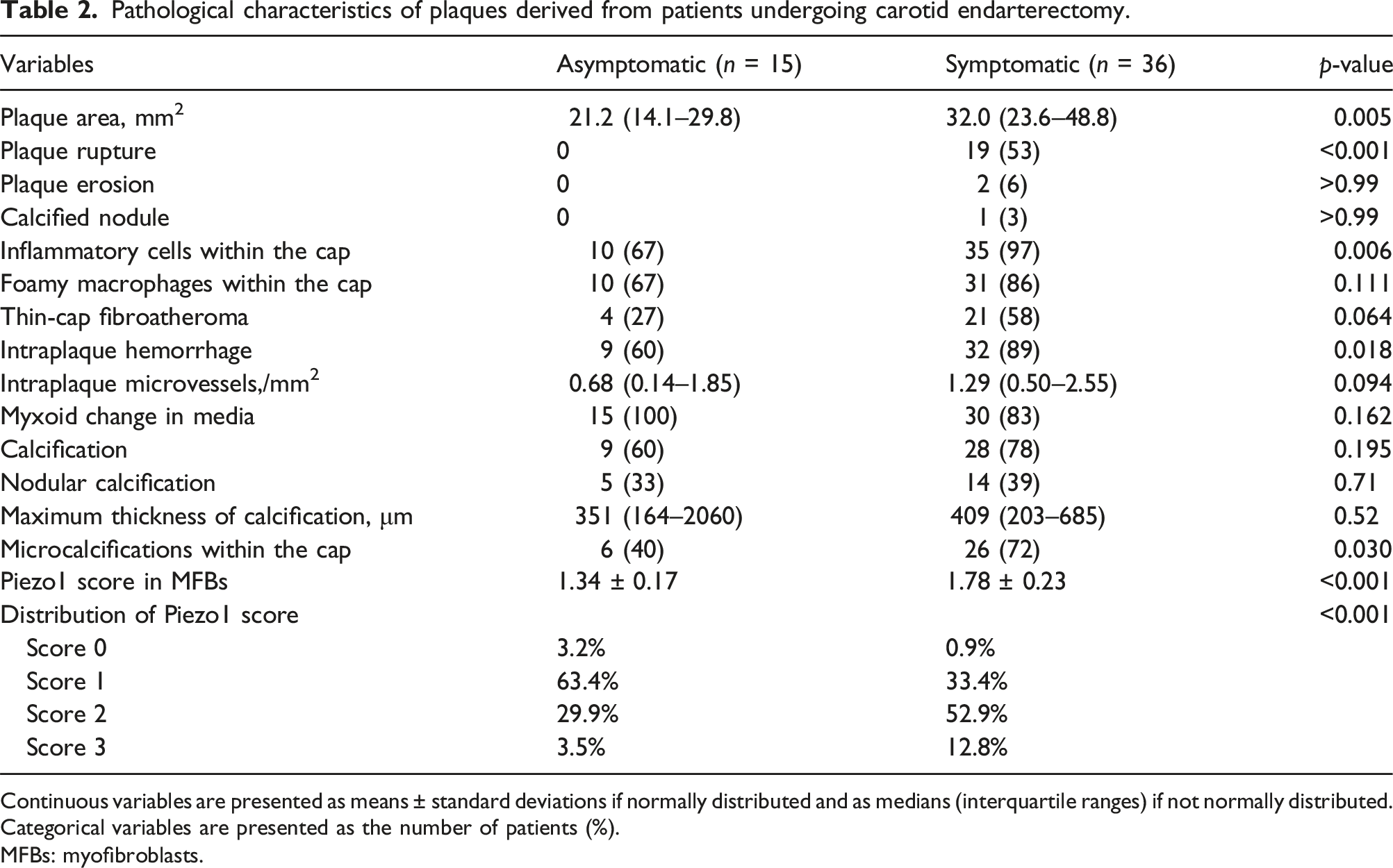
Continuous variables are presented as means ± standard deviations if normally distributed and as medians (interquartile ranges) if not normally distributed. Categorical variables are presented as the number of patients (%).
MFBs: myofibroblasts.
Pathological characteristics and Piezo1 score
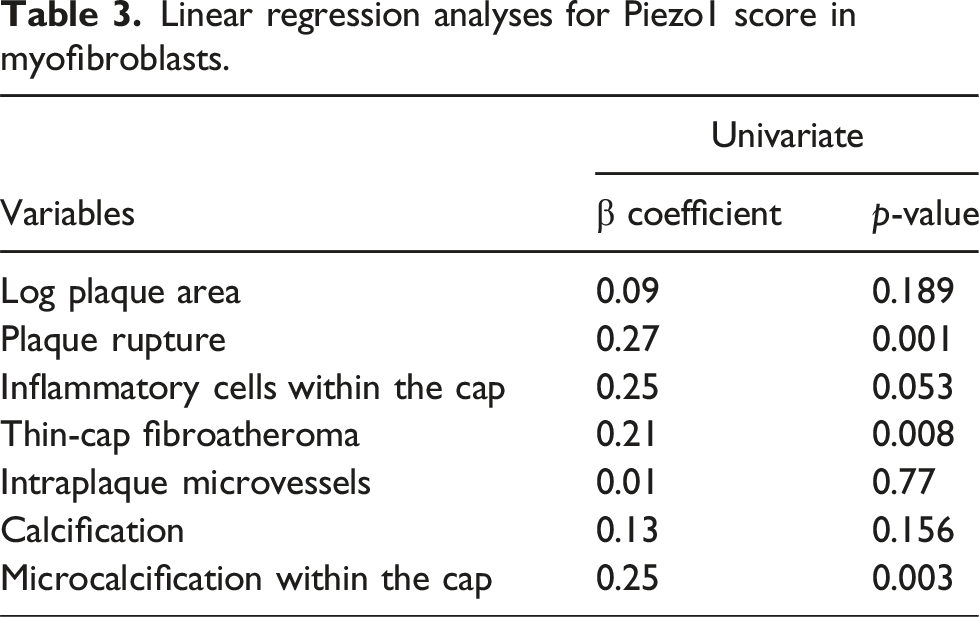
Linear regression analyses for Piezo1 score in myofibroblasts.
Discussion
In this study, Piezo1 expression in MFBs was higher in symptomatic plaques than in asymptomatic plaques among patients undergoing CEA. Our results suggested a link between Piezo1 expression in MFBs and the development of carotid atherosclerosis.
Several factors may explain the higher Piezo1 score in MFBs in symptomatic atherosclerotic plaques than in asymptomatic plaques in patients undergoing CEA. When endothelial cells and vascular smooth muscle cells sense a variety of mechanical stresses via the Piezo1 channel, atherosclerosis develops by various pathways in response to the stimuli. Previous studies have demonstrated the association of Piezo1 with a variety of inflammatory pathways, which are key to the development of atherosclerosis.21,22 It has been reported that Piezo1 plays an important role in the activation of T cells and the assembly of the Nod-like receptor protein 3 (NLRP3) inflammasome.21,22 The assembly of the NLRP3 inflammasome causes the release of the proinflammatory cytokines, interleukin (IL)-1β and IL-18. 22 Piezo1 is strongly associated with the flow shear stress-induced phosphorylation of PECAM-1 and vascular endothelial growth factor receptor 2. 23 Cyclical force signals, transduced via Piezo1 into myeloid cells, cause a Ca2+ influx and AP-1 induced EDN1 expression, resulting in the stabilization of HIF1α, followed by facilitation of proinflammatory transcription. 24 HIF-1α, colocalizing with vascular macrophages, is involved in the increase of foam cells, neovascularization, and intraplaque hemorrhage.25,26 In a mouse model, the activation of Piezo1 increased the expression of IL-6 via p38 MAP kinase. 27 Furthermore, Piezo1 reportedly modulates cell proliferation, MFB differentiation, and extracellular matrix turnover, which is an important process in atherosclerotic plaque formation. 28 Consistent with these previous reports, our study found that compared to the plaques derived from asymptomatic patients, the Piezo1 score was higher in symptomatic plaques, which contained larger plaque areas (Table 2).
Although the number of analyzed plaques was small, our results suggest that plaque rupture and microcalcifications within the fibrous cap may be the relevant plaque characteristics to Piezo1 scores in MFBs. This could be explained by the turbulent shear stress, reportedly associated with the plaque burden and plaque disruption in a rabbit model. 29 Furthermore, the oscillating flow-induced shear affects the biomechanical stability of the endothelium, contributing to plaque progression and, eventually, disruption of the fibrous cap. 30 Therefore, the expression of Piezo1 in MFBs in carotid atherosclerotic plaques may be higher at rupture-prone sites because they face the greatest degree of turbulent shear stress. In addition, smooth muscle cells and other vascular cells, including MFBs, can synthesize a mineralized matrix and undergo osteoblastic differentiation, causing calcified deposits. 31 Previous studies have shown, using multimodal assessments including computational flow modeling and optical coherence tomography, that a low shear stress is associated with small calcifications, including microcalcifications.32,33 Therefore, we hypothesize that the increased Piezo1 expression in MFBs in the fibrous cap may reflect the higher extent of turbulent shear stress they are exposed to, which may also lead to their association with microcalcifications.
This study has several limitations. First, this was a small, retrospective, observational study performed at a single university hospital, thereby limiting the generalizability of the results. Therefore, larger, multicenter, prospective studies are needed to verify the present findings. Second, it was mainly performed via morphological analysis of excised specimens derived from carotid atheromatous plaques, and no functional analysis was performed with inflammatory biomarkers related to carotid plaque instability, such as IL-6. 34 Third, in this study, fewer patients were on an aspirin or a statin preoperatively, compared to previous studies.15,35,36 Several studies suggested that Piezo1 channel may cause various cellular activities such as proliferation, apoptosis vascular remodeling, and inflammatory responses, which are fundamental processes in atherosclerotic development.37,38 Because statins have the anti-inflammatory effect on the formation of atherosclerotic plaque, the results may be different in a patient population that should be on a high-intensity dose of statins.
Conclusions
Our analyses’ results may suggest that the Piezo1 expression of MFBs is higher in symptomatic plaques among patients undergoing CEA. Further research is warranted to support this finding.
Footnotes
Acknowledgments
The authors are grateful for the contributions of all investigators, clinical research coordinators, and laboratory technicians involved in this study.
Author contributions
TK wrote the manuscript. KK, TO, TY, TA, TA, and ST were responsible for the conception. All authors have read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant from The Ito Foundation (2021 Foundation Grant) (to T.K.). The funding sources had no involvement in any research process.