
Abstract
Objectives
The effectiveness of postoperative medication for the prevention of late graft failure is controversial. We conducted the present study to investigate whether cilostazol improved the mid-term outcomes after infrainguinal autologous vein bypass for chronic limb-threatening ischemia (CLTI).
Methods
From April 1994 to March 2022, we performed 590 de novo infrainguinal bypass procedures using autologous vein grafts (AVGs) in three hospitals. The bypass grafts were classified according to the postoperative prescription of cilostazol. The loss of graft patency and major adverse limb events (MALEs) were set as endpoints. Patients who died within 30 days and grafts that lost primary patency within 30 days after surgery were excluded. Data up to 3 years were analyzed. The cumulative primary patency (PP), assisted primary patency (AP), secondary patency (SP), and freedom from MALE (ffMALE) rates were calculated by the Kaplan–Meier method and compared between the cilostazol group and the non-cilostazol group. After a propensity score matching, same statistical analyses were performed. In addition, a Cox proportional hazards regression analysis that included preoperative factors, intraoperative factors, and postoperative medications was performed to identify whether cilostazol is an independent predictor for the outcomes.
Results
A total of 523 AVGs met inclusion criteria. Kaplan–Meier curves showed that the cilostazol group was superior to the non-cilostazol group in all outcomes, while the cilostazol group was superior to the non-cilostazol group in AP and SP after a propensity score matching. A multivariable analysis showed that non-use of cilostazol was identified as an independent predictor for loss of AP, SP, and ffMALE.
Conclusions
Cilostazol improved the mid-term outcomes after infrainguinal autologous vein bypass.
Introduction
Various drugs are used to maintain the graft patency of infrainguinal bypass for lower extremity arterial disease (LEAD) in the clinical setting. Although anti-platelet drugs (APDs) are commonly used, there is inconclusive evidence that they specifically enhance the lower extremity vein graft patency. 1 Multiple studies have attempted to determine whether APDs are beneficial, and some subgroup analyses suggested that the effect of individual drugs on graft patency differs according to the graft materials; the greatest beneficial effect of anti-platelet agents was observed in prosthetic bypasses, and anti-platelet regimens were less effective for autologous vein bypasses.2–4
Aspirin (ASA), dipyridamole (DIP), and clopidogrel were used as anti-platelet drugs in such trials.1–4 In Japan, besides ASA and P2Y12 inhibitors including clopidogrel, cilostazol is commonly used as a medication with anti-platelet action for LEAD. In the field of endovascular intervention, the effectiveness of cilostazol in the inhibition of restenosis has been reported by many authors.5–8 However, the efficacy of cilostazol for enhancement of vein graft patency has remained obscure.
We conducted this retrospective study to investigate whether cilostazol prevented the late graft occlusion after infrainguinal autologous vein bypass for chronic limb threatening ischemia (CLTI).
Materials and methods
This study was approved by the Institutional Review Board of Saiseikai Yahata General Hospital (approval number: 183). The approval document was not obtained because personal information was not clear.
Database and patient selection
Data on patients who underwent infrainguinal bypass for LEAD using an autologous vein graft (AVG) at Steel Memorial Yawata Hospital between April 1994 and March 2007 and between April 2011 and March 2015, at Kokura Memorial Hospital between April 2007 and March 2011, and at Saiseikai Yahata General Hospital between April 2015 and March 2022 (at these time points, Mii S was working at these hospitals as a vascular surgeon) were retrospectively reviewed.
Analyzed variables
The following variables were retrieved from the patients’ charts or electronic medical records: age, sex, de novo or redo bypass, indication for surgery (rest pain or tissue loss), etiology of LEAD, medical history (hypertension [HT], diabetes mellitus [DM], coronary artery disease [CAD], cerebrovascular disease [CVD], dialysis-dependent end-stage renal disease [ESRD], and dyslipidemia [DL]), intraoperative information (operator, vein conduit [single vein or spliced vein], and distal target artery), postoperative medication (APDs [ASA, P2Y12 inhibitors (ticlopidine, clopidogrel, prasugrel, and ticagrelor), and cilostazol], anti-coagulant agent [ACA], and statin), date of surgery, date of first reintervention, date of major adverse limb event (MALE), and final date of confirmation of graft patency.
Prescription of postoperative medications
The prescription of postoperative medications was left to the discretion of each attending doctor. Basically, when APDs were prescribed before surgery, the same drugs were continued after surgery. After discharge, the same medication was continued as long as side effects did not occur. Consequently, APDs used after surgery were affected by the preoperative ischemic level of LEAD and medical history. Cilostazol was not always prescribed as a de novo medication after bypass surgery.
Graft surveillance
The surveillance protocol was described in a previously published paper. 9 Briefly, graft patency was checked at regular intervals of 1–3 months. Until March 2007, pulsation of the arteries in the lower extremity and ankle brachial pressure index (ABI) were examined. Duplex ultrasonography (DUS) was added from April 2007. When pulsation of the graft became obviously weak, ABI became >0.15 lower in comparison to previous data, or DUS visualized obvious stenosis with peak systolic velocity >300–350 cm/s or velocity ratio >3.0–3.5, angiography and a revision procedure (if necessary) were actively recommended. Regarding the revision strategy, surgical repair was selected first until March 2015; thereafter, percutaneous intervention was selected first. A final review was conducted in the period from September to October 2022, and data up to 3 years were analyzed.
Outcome measures and data analysis
Primary patency (PP), assisted primary patency (AP), and secondary patency (SP) of the bypass graft and freedom from MALE (ffMALE) rates were set as outcome measures. The grafts that lost PP and those in patients who died within 30 days after surgery were excluded.
The grafts were classified into two cohorts, according to the prescription of cilostazol after bypass surgery.
Definitions
Preoperative complications were defined according to generally used clinical definition. Operators were divided into two groups based on the years of practice after graduation from a medical college: experienced surgeons (>10 years). PP was defined as uninterrupted patency with neither a procedure performed on the graft nor a procedure to deal with disease progression in the adjacent native vessel, AP was defined as uninterrupted patency with any prophylactic intervention before graft occlusion, and SP was defined as patency with any intervention to protect patency before or after graft occlusion. 10 Ligation of the patent graft due to infection or major amputation was regarded as graft occlusion. MALE was defined as major amputation (above the ankle) of the revascularized limbre or reintervention (new bypass graft, jump/interposition graft revision, or thrombectomy/thrombolysis) on the revascularized segment. 11
Statistical analyses
Characteristics of cilostazol and non-cilostazol cohorts.
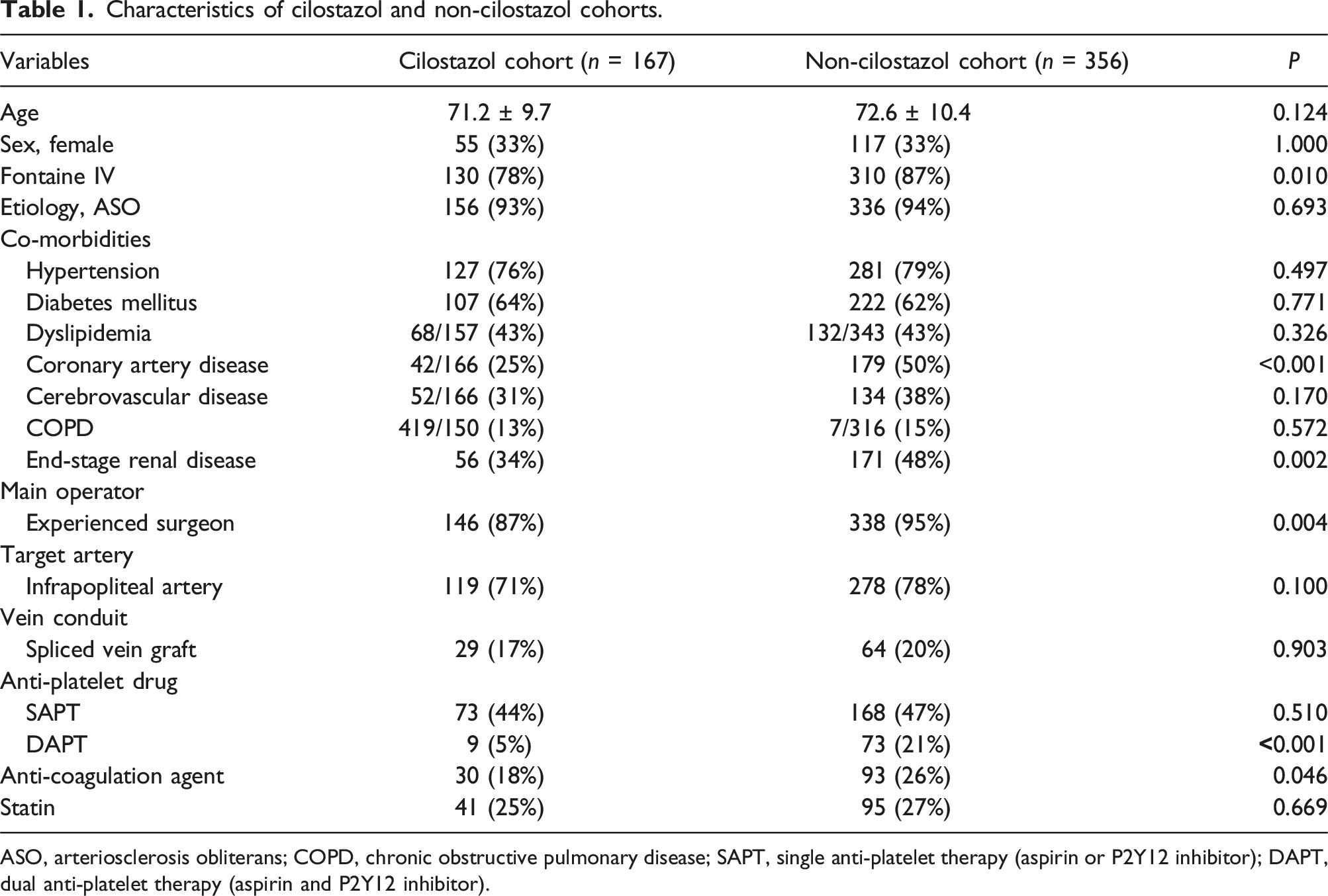
ASO, arteriosclerosis obliterans; COPD, chronic obstructive pulmonary disease; SAPT, single anti-platelet therapy (aspirin or P2Y12 inhibitor); DAPT, dual anti-platelet therapy (aspirin and P2Y12 inhibitor).
Results
Patient flow for analysis
A total of 590 de novo infrainguinal bypasses using AVG were performed for LEAD. Since 67 AVGs were excluded due to the exclusion criteria (graft occlusion or revision for prevention of graft occlusion or death within 30 days after surgery), 523 AVGs were finally included in the analysis and cilostazol was prescribed in 167 patients (cilostazol group) and was not prescribed in 356 patients (non-cilostazol group) (Figure 1). Patients' flow for analysis. AVG, autologous vein graft; CLTI, chronic limb threatening ischemia.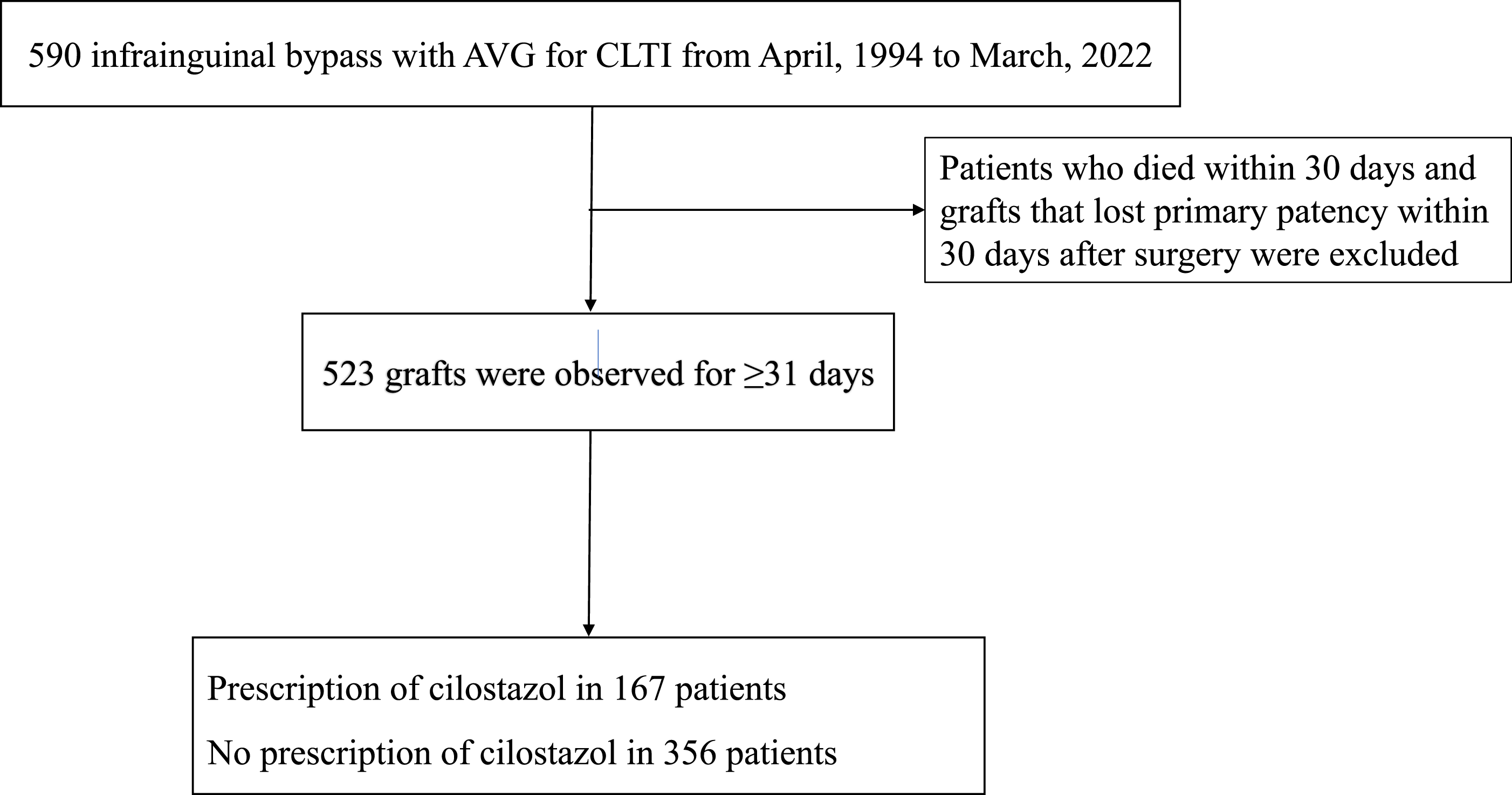
Comparison of characteristics between the cilostazol group and the non-cilostazol group
There were significant differences in Fontaine classification, CAD, ESRD, main operator, DAPT, and ACA.
Graft patency and freedom from MALE rates
The PP, AP, SP, and ffMALE rates at each interval are shown in the tables of Figure 2. The cilostazol group was superior to the non-cilostazol group in all outcomes: PP (p=.008), AP (p<.001), SP (p < .001), and/or ffMALE rates (p=.005). Graft patency and freedom from MALE rates in patients with or without prescription of cilostazol. PP, primary patency; AP, assisted primary patency; SP, secondary patency; ffMALE, freedom from major adverse limb event.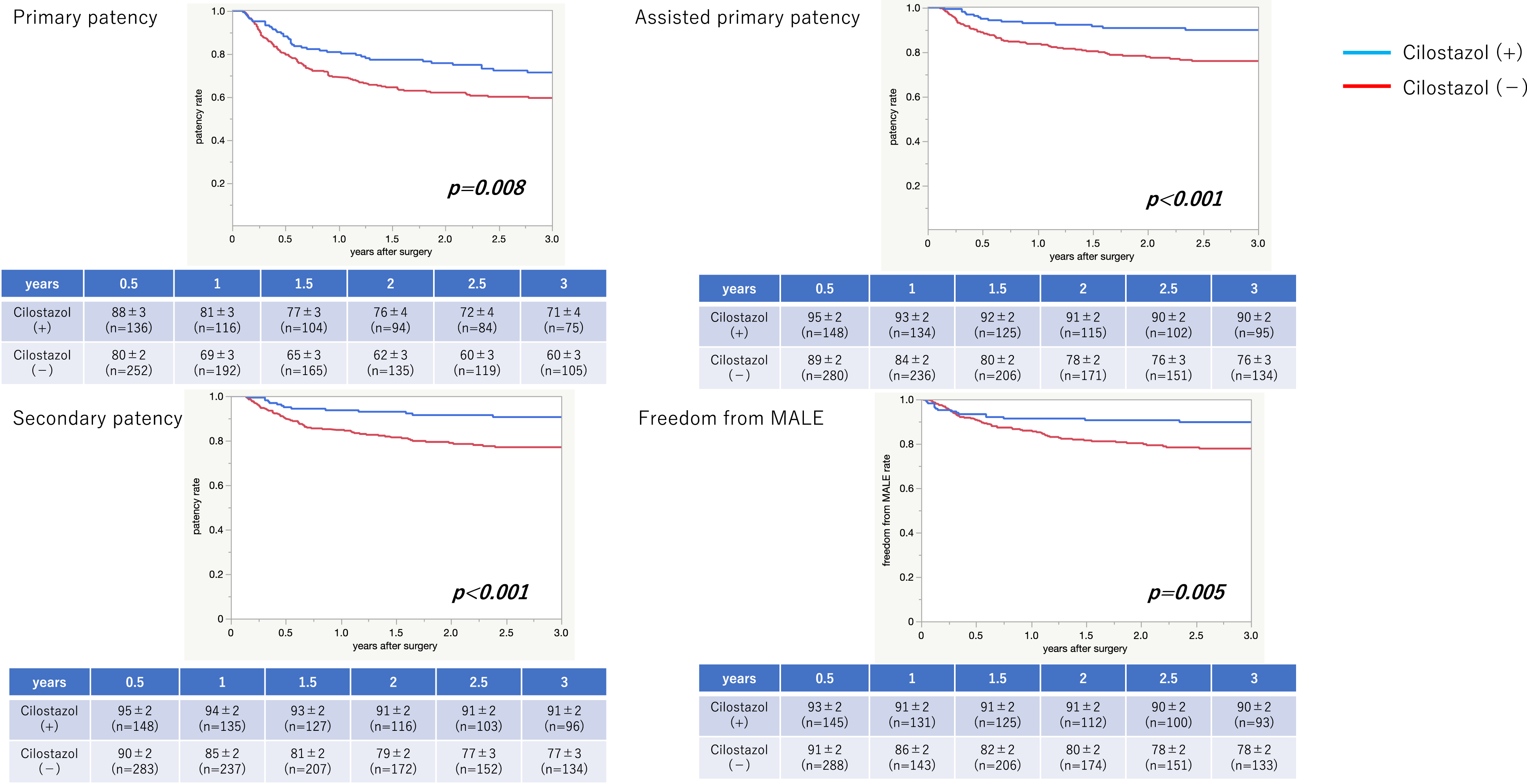
A propensity score matching
Characteristics of cilostazol and non-cilostazol cohorts after a propensity score matching.
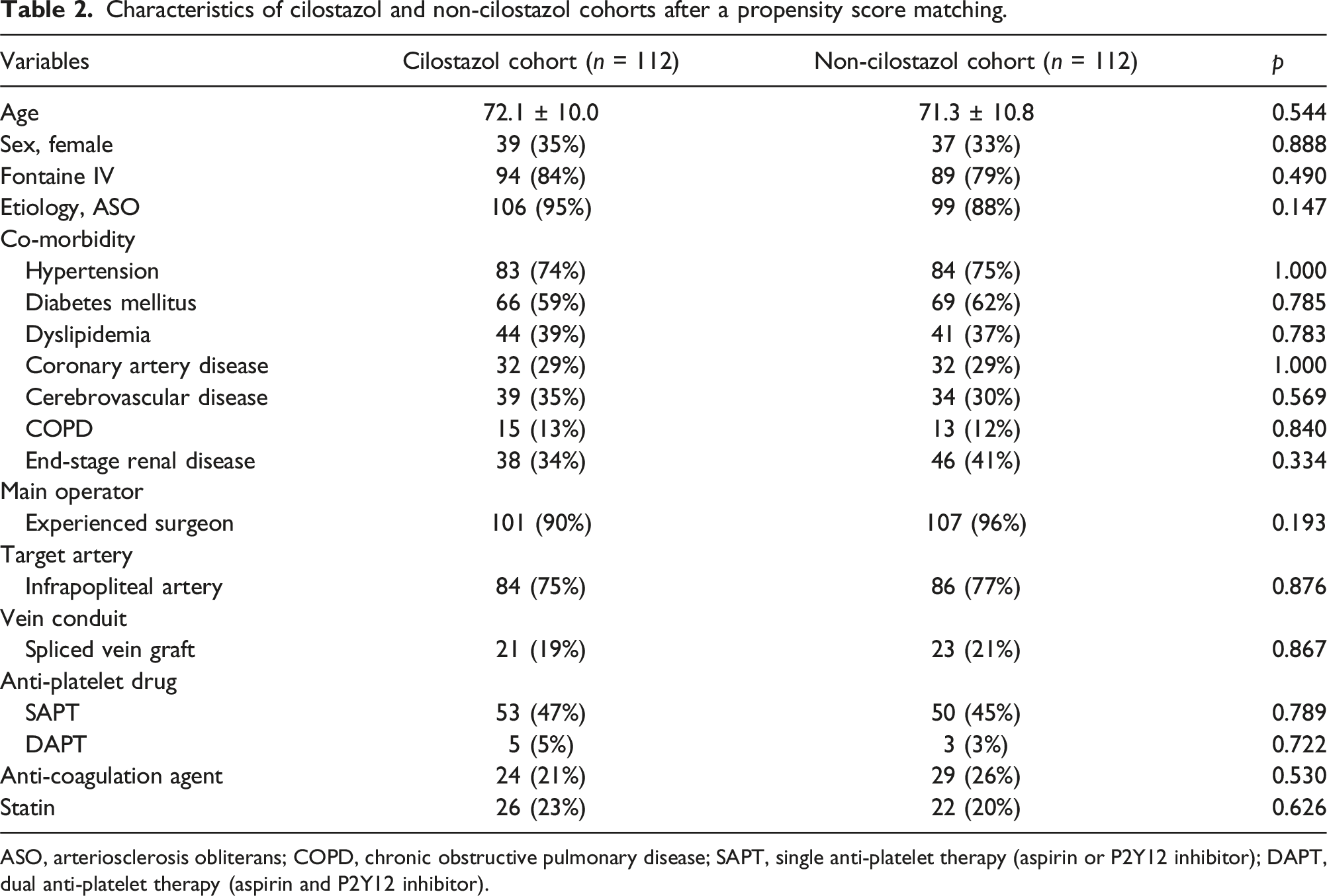
ASO, arteriosclerosis obliterans; COPD, chronic obstructive pulmonary disease; SAPT, single anti-platelet therapy (aspirin or P2Y12 inhibitor); DAPT, dual anti-platelet therapy (aspirin and P2Y12 inhibitor).
The PP, AP, SP, and ffMALE rates at each interval are shown in the tables of Figure 3. AP and SP of the cilostazol group were significantly higher than those of the non-cilostazol group: AP (p = .005) and SP (p = .016) rates, while there was no significant difference between the groups in other outcomes: PP (p = .098) or ffMALE (p = .147) rates. Graft patency and freedom from MALE rates in patients with or without prescription of cilostazol. PP, primary patency; AP, assisted primary patency; SP, secondary patency; ffMALE, freedom from major adverse limb event.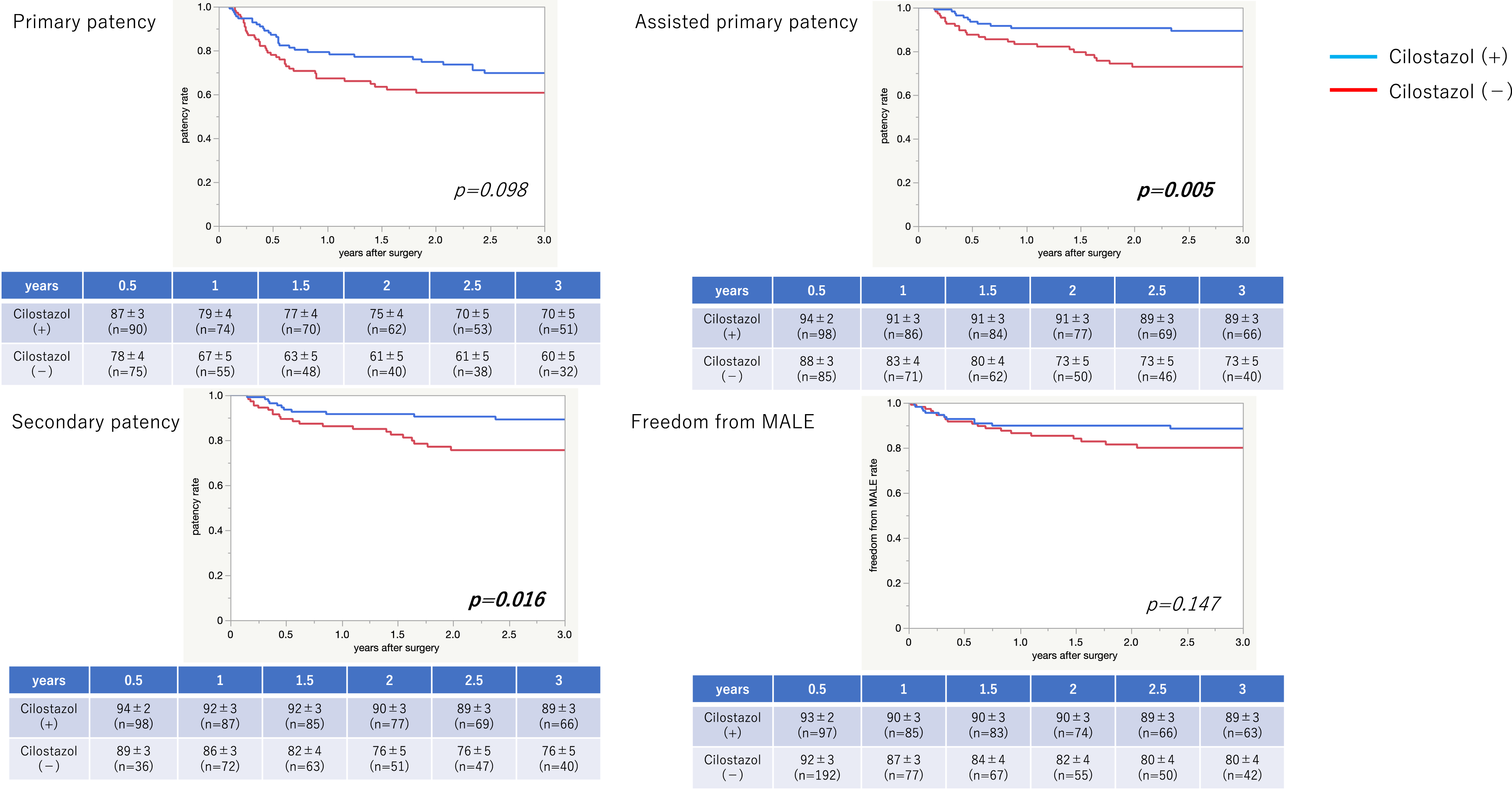
A Cox proportional hazards regression analysis
A Cox proportional hazard analysis for each outcome.
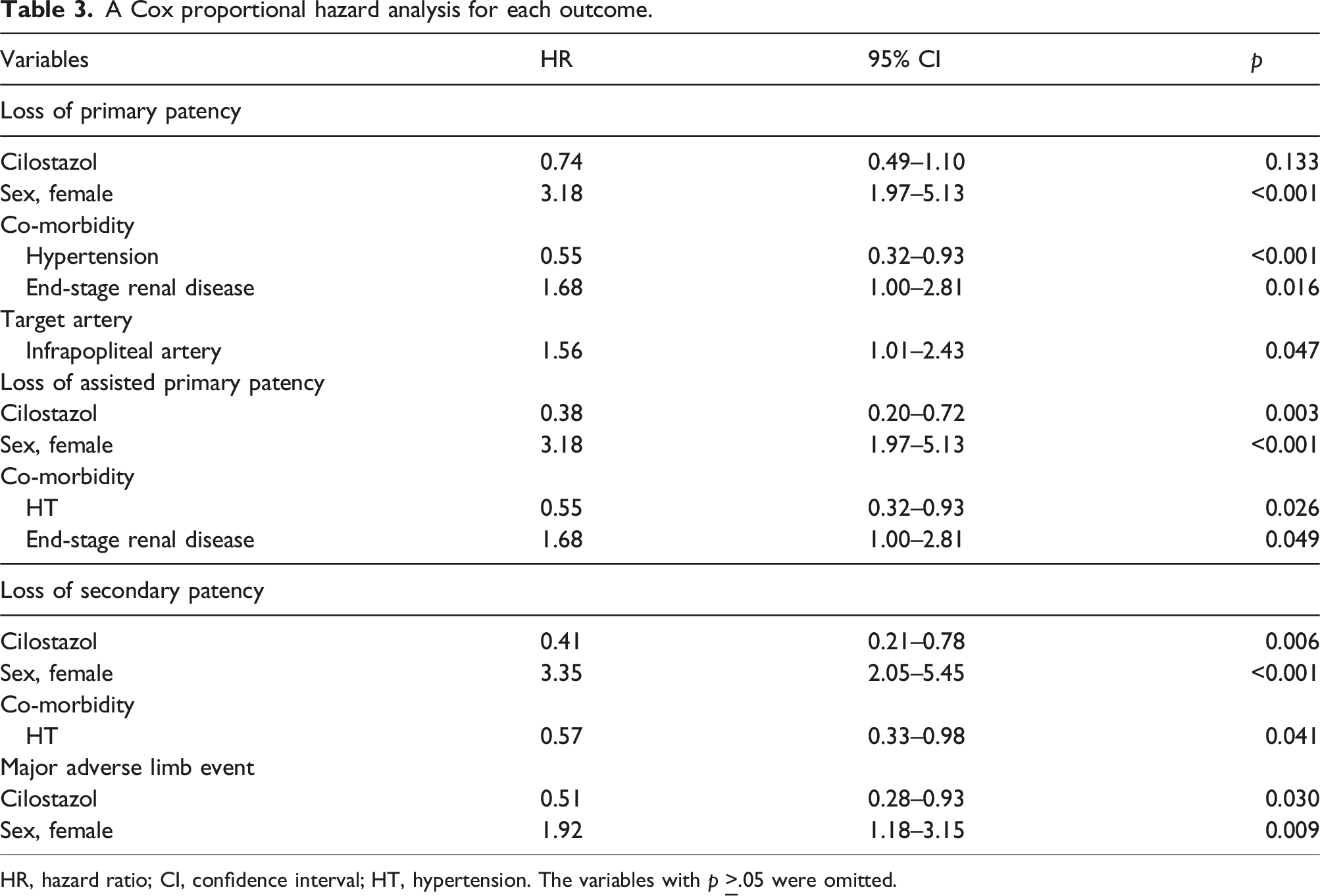
HR, hazard ratio; CI, confidence interval; HT, hypertension. The variables with p
Discussion
The present study shows that cilostazol improved all outcomes in crude data. However, after a propensity score matching, the cilostazol group was superior to the non-cilostazol group only in AP and SP. In addition, a multivariable analysis demonstrated that non-use of cilostazol was an independent predictor for loss of AP, SP, and MALE.
In past studies, ASA was the main anti-platelet agent used for the prevention of graft occlusion after bypass surgery. Cochrane systematic review and meta-analysis, which included six trials, demonstrated that ASA or ASA/DIP was more effective than placebo or nothing in the prevention of graft occlusion in patients who received infrainguinal bypass. 2 However, the superiority of ASA or ASA/DIP was observed in prosthetic grafts but not in vein grafts. 2 In a subgroup analysis of the Clopidogrel and Acetyl Salicylic Acid in Bypass for Peripheral Arterial Disease (CASPER) trial, clopidogrel plus ASA was shown to be superior to ASA in reducing graft occlusion in prosthetic bypass, but not in venous bypass. 12 In a subgroup analysis of the Dutch Bypass Oral Anti-coagulants or Aspirin (BOA) Study, which was a prospective randomized study to investigate the effect of warfarin and ASA on graft patency, ASA was associated with better results in non-venous grafts but not in vein grafts. 13 In addition, Hess et al. also showed, based on their structured review of antithrombotic therapy, that ASA improved patency after lower limb revascularization procedures using prosthetic conduits and that the effect of ASA alone after autologous vein bypass was questioned. 4
Although ASA and P2Y12 inhibitors including clopidogrel are most frequently used drugs after bypass surgery, cilostazol is also one of the most frequently used drugs after revascularization in Japan. Several reports on the inhibitory effect of cilostazol for stenosis after endovascular intervention have been published mainly from Japanese institutes.5–7 However, the efficacy of cilostazol for enhancement of vein graft patency has remained obscure.
Most of CLTI patients have multiple co-morbidities in their cardiovascular system. It is not uncommon for the patients to already take some APDs before undergoing bypass surgery. Patients with a history of CAD or CVD had been generally prescribed ASA, P2Y12 inhibitor, or ACA. In contrast, few patients with a history of CAD or heart failure had taken cilostazol. Although the postoperative medication was left to the discretion of the attending doctors, the APDs prescribed before bypass surgery were basically continued after surgery in the present study. When the condition of reconstructed arterial anatomy and vein conduit was considered to be poor, a new APD or ACA was added without hesitation, except for patients with ESRD because of polypharmacy issues. Similarly, heterogeneity in patients’ background had caused bias in prescription of APDs, which might have affected the results of the present study. Notwithstanding, the effect of cilostazol on improving AP and SP was observed after a propensity score matching analysis, and a multivariable analysis also demonstrated the positive effect of cilostazol on improving AP, SP, and ffMALE.
Intimal hyperplasia (IH) causing loss of PP can be divided into two types: local IH (valve site, anastomotic site, and injury site) and whole-length IH. Postoperative medication can affect both kinds of IH: local IH, which is affected more intensely by intraoperative injury, can be revised by a local procedure and the graft patency might be maintained thereafter, while whole-length IH cannot be revised effectively and ultimately results in graft occlusion, namely, the loss of AP or SP. Considering the results of the present study, the effect of cilostazol might not be sufficient to prevent local IH leading to loss of PP, while it might contribute to prevention of whole-length IH. This is a noteworthy result, as specific data on CLTI are lacking.
Owens et al. demonstrated that one of the mechanisms of late graft failure of AVGs was negative remodeling with exudative IH. 14 It had been clinically proved that the negative remodeling at 1 month after bypass surgery significantly influenced the mid-term patency. 15 He et al. noted a positive association between cilostazol and positive remodeling of the vein graft at 1 month after surgery. 16 The inhibitory effect of cilostazol on IH of an implanted vein graft was also shown in animal models. 17
The effectiveness of oral vitamin K antagonist on vein bypass has been reported in several studies.13,18 However, the present study did not show the effectiveness of ACA on the prevention of vein graft occlusion. As Jackson et al. noted, the INR may affect the results. 19 We generally adjusted the INR in the range of 1.5–2.0 to avoid the side effect of bleeding. 20 In contrast, in the BOA trial, which demonstrated the effectiveness of anti-coagulant therapy on the improvement of the patency, the target INR was 3.5–4.0. 13 Current subanalysis of Voyager PAD trial reported a favorable benefit of adding low-dose rivaroxaban to APDs, regardless of conduit type. 21
Of note, female sex was identified as one of the independent predictors for loss of graft patency and MALE. Some have reported the inferiority of women on graft patency,22,23 and others denied sex-based discrepancy. 24 The progression of arteriosclerosis might be faster in menopausal Japanese women, and smaller artery in nature, compared with men, may be associated with poor outcomes. Further study is necessary to elucidate the influence of gender on the outcomes, and if there is a sex-based discrepancy, combination of drugs to prevent graft failure in CLTI women has to be considered.
The present study was associated with some limitations. First, the present study was retrospective in nature. In addition, all registered cases underwent bypass surgery at the facilities where one of the authors (S.M.) worked, during the period in which that author worked there. Although no differences in patency rates among the facilities were present (data not shown), the evidence level obtained from this retrospective study performed based on a private experience is low. Second, the registration period of the study was considered too long, and a total of 16 vascular surgeons performed bypass surgery as a main operator during this period. There was no difference in graft patency between experienced and less-experienced surgeons. Whenever a less-experienced surgeon operated, an experienced surgeon assisted as a teaching assistant director. Third, the study population was small. Fourth, the grafts were divided based on the medication prescribed at discharge. However, compliance or changes in the administered medications were not taken into consideration. Fifth, drugs, which have antithrombotic action, other than ASA, P2Y12 inhibitors, and cilostazol were not taken into consideration. We used eicosapentaenoic acid, sarpogrelate (5HT2 blocker), and beraprost/limaprost (prostaglandin E1/I2 analog) as antithrombotic agents in Japan, but they were ignored in the present study because they were not deemed as antithrombotic agents in the Western world. Sixth, important factors affecting graft patency such as graft size, graft quality, and prolonged inflammation were not included in the variables. Cilostazol did not contribute to improvement of graft patency in high-risk anatomic cases such as infrapopliteal bypass or spliced vein graft (data not shown), in which small diameter veins or poor quality veins were occasionally used and complication of inflammation was not uncommon. It can be speculated that cilostazol could not overcome such strong negative factors for graft patency. Seventh, there was no safety evaluation.
Conclusions
Cilostazol might improve the mid-term graft patency of infrainguinal autologous vein bypass for CLTI. A large prospective randomized trial is needed to confirm the effect of cilostazol on the mid-term outcomes.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Patient’s approval was not obtained because it did not include private information. The present study was approved by the IRB.