
Abstract
Background
Critical limb ischemia (CLI) patients take too many medications because they are elderly and frail patients with multiple comorbidities. Polypharmacy is associated with frailty, although its prognostic significance in CLI patients is unknown. In this study, we aimed to determine the prevalence of hyperpolypharmacy among adults with CLI and its effect on 1-year amputation and mortality.
Methods
A total of 200 patients with CLI who underwent endovascular therapy (EVT) for below-knee (CTC) lesions were included in this study. Hyperpolypharmacy was defined as using ≥10 drugs. Patients were divided into two groups according to the presence of hyperpolypharmacy
Results
We detected hyperpolypharmacy in 66 patients. The incidence of 1-year amputation [24 (36.4) versus 12 (9), p<.001] and mortality [28 (42.4) versus 12 (9), p<.001] were higher in patients with hyperpolypharmacy. Univariate and multivariate cox regression analyses were used to determine the independent predictors of amputation and mortality. In the receiver operating characteristic curve analysis, the cut-off value was defined as 10 or more drug use was able to detect the presence of 1-year mortality with 67.5% sensitivity and 79.4% specificity. The Kaplan–Meier method showed a significant difference (rank p <.001 between log groups), and hyperpolypharmacy was associated with 1-year amputation and mortality.
Conclusion
Hyperpolypharmacy was significantly associated with 1-year mortality and major amputation in CLI patients. Hyperpolypharmacy can be a valuable aid in patient risk assessment in the CLI.
Introduction
Critical limb ischemia (CLI) is a serious complication of the atherosclerotic process in peripheral arteries and can have some consequences that can lead to major amputations and even mortality. 1 Below-knee lesions are the cause of a significant proportion of patients with CLI but there is still insufficient data regarding which revascularization therapy to choose in these patients. 2 However, the use of endovascular treatment (EVT) methods is increasing with the developments in materials and the increase in experience. Despite a successful EVT, reintervention, amputation, and mortality rates remain high.3,4
In addition to the severity of the disease in patients with CLI, the existing comorbid factors in the patients also affect the outcomes. Many factors predicting major amputations and mortality in CLI patients have been demonstrated in previous studies.5–8 Advanced age, presence of diabetes, renal dysfunction, anemia, prior amputation, and tissue loss are some of the risk factors defined for both short-term and long-term mortality and amputations. Besides the adverse effects of all these factors on prognosis, their frequency in CLI patients complicates risk assessment.3,9 Therefore, some of the combined risk scoring systems have been defined to predict the prognostic course in CLI patients. One of the most essential parameters in this regard is frailty. Frailty is quite common among CLI patients and is also associated with the severity of limb threat and mortality. 10 Parameters such as the Charlson comorbidity index, clinical frailty score, and sarcopenia were defined in the determination of frailty. 11 At the same time, polypharmacy, which is an essential determinant of clinical processes in geriatric patients, is closely related to frailty. 12 Polypharmacy, which is defined as the use of ≥5 drugs, is detected in approximately 40% of the population over 65 years of age. 13 In fact, the concept of hyperpolypharmacy, which defines the use of ≥10 drugs, has begun to be used in the geriatric population. 14 As a matter of fact, CLI patients are predominantly elderly patients and represent a group of patients who have many diseases and generally use a large number of drugs. Hence, drug side effects and drug–drug interactions also cause poor outcomes.
Although previous studies have showed the association between the frailty indices and poor outcomes in CLI patients, data on the effect of polypharmacy are limited. Therefore, we aimed to investigate the association of hyperpolypharmacy with 1-year major amputation and mortality in CLI patients.
Methods
Study population
Consecutive patients who underwent below-knee intervention for CLI between January 2016 and October 2022 were retrospectively reviewed. Patients over 18 of age who had undergone below-knee endovascular intervention due to critical leg ischemia were included in the study. Those with a previous history of revascularization (surgery or percutaneous) to the same vascular bed, malignancy, end-stage liver failure, acute extremity ischemia, and those who could not use drugs were excluded. After evaluating the inclusion and exclusion criteria, the remaining 200 patients were included in the study. Demographic data, laboratory findings, and outcomes were obtained through hospital records, file reviews, and telephone interviews. Our study was conducted in accordance with the principles of the Declaration of Helsinki and was approved by the local Ethics Committee.
Definition of hyperpolypharmacy
Drugs were classified according to the Multum Lexicon Drug Database which is used by Unlu et al. 13 on heart failure patients. This system includes three major medication groups: HF medications, non-HF cardiovascular medications, and non-cardiovascular medications. These classifications were based on direct indications. At admission, the drugs were questioned, and the drug containers were checked and recorded in the patient’s file. These files were scanned retrospectively, and the number and types of drug use of the patients were noted. While studies generally accept the presence of polypharmacy (≥5 drugs) as a predictor, the high rate of polypharmacy in patients with CLI forced us to assess hyperpolypharmacy (≥10 drugs).
Endovascular treatment and follow-up
The vascular team (cardiologist, cardiovascular surgeon) decided the treatment method in accordance with current guidelines and recommendations.15,16 Dual antiplatelet therapy (in general clopidogrel and aspirin) was administered before the procedure. If the patient was using a potent P2Y12 inhibitor such as ticagrelor or prasugrel before the procedure, the treatment was not changed. The dual antiplatelet strategy after 1 month was evaluated independently of below-the-knee endovascular therapy. Only aspirin was added to the treatment of patients under oral anticoagulant therapy. All EVT procedures were performed under local anesthesia by interventional cardiologists with at least 5 years of experience. The operator decided on the EVT approach during the procedure. In general, a 6F sheath was used for the antegrade approach from the ipsilateral common femoral artery. However, the retrograde approach was performed for patients who could not be treated with the antegrade approach. In addition, the cross-over method with a contralateral puncture was applied for the patients who had insufficient ipsilateral iliac flow or who also required an above-the-knee procedure. After the arterial access site was obtained, a bolus dose of unfractionated heparin (70–100 units/kg) was administered after the sheath was placed. After successful 0.014 inch guidewire intraluminal or subintimal crossing, extended balloon dilatation was performed for 2–3 min. Selective cases were safely re-canalized by either the transcollateral approach or the retrograde approach, especially after unsuccessful re-entry into the true distal lumen after subintimal wiring. Balloon dilatation was performed using low-profile balloons depending on the reference vessel size. Technical success was defined as blood flow to the distal vascular bed with 40% or less stenosis. Following EVT, all patients received aspirin (100 mg) and clopidogrel (75 mg) or other P2Y12 inhibitors (ticagrelor or prasugrel) as maintenance dual antiplatelet regimens for at least 1 month. Cilostazol (100 mg) treatment was left to the discretion of the physician. Before discharge, all patients underwent clinical examination and duplex ultrasound if necessary. As part of the hospital practice, follow-up visits of the patients at our institution were planned every 3–6 months.
Endpoints of the study
The primary endpoint of the study was all-cause mortality at 1-year follow-up, and the secondary endpoint was index artery-related amputation at 1-year follow-up.
Statistical analysis
Study data were analyzed using the Statistical Package for the Social Sciences, version 26.0 (SPSS Inc., Chicago, IL, USA). Primarily, whether the variables were normally distributed or not was evaluated by visual (histograms and probability curves) and analytical methods (Kolmogorov–Smirnov and Shapiro–Wilk). Normally distributed numerical variables were expressed as mean ± standard deviation (SD), non-normally distributed numerical variables were expressed as median (interquartile range), and categorical variables were expressed as percent (%). ROC (receiver operating characteristic) curve and Youden index [max (Sensitivity + Selectivity 1)] were used to determine the cut-off value of the number of drug use and the area under it, which best detects the presence of 1-year mortality. A ROC curve above 0.5 was considered significant. Statistical analysis of numerical variables between the two groups was performed with the Student’s t test or Mann–Whitney U test, and analysis of categorical variables with chi-square or Fisher’s exact test. To identify independent predictors of 1-year mortality and amputation, univariate cox regression analysis was performed first, followed by multivariate cox regression analysis using parameters that were significant in this analysis. The 1-year survival and amputation curve using hyperpolypharmacy was analyzed using the Kaplan–Meier method, and statistical analysis was done with the log-rank test. Throughout this data evaluation, a p-value <.05 was considered significant.
Results
Baseline clinical and echocardiographic characteristics according to the presence of hyperpolypharmacy.
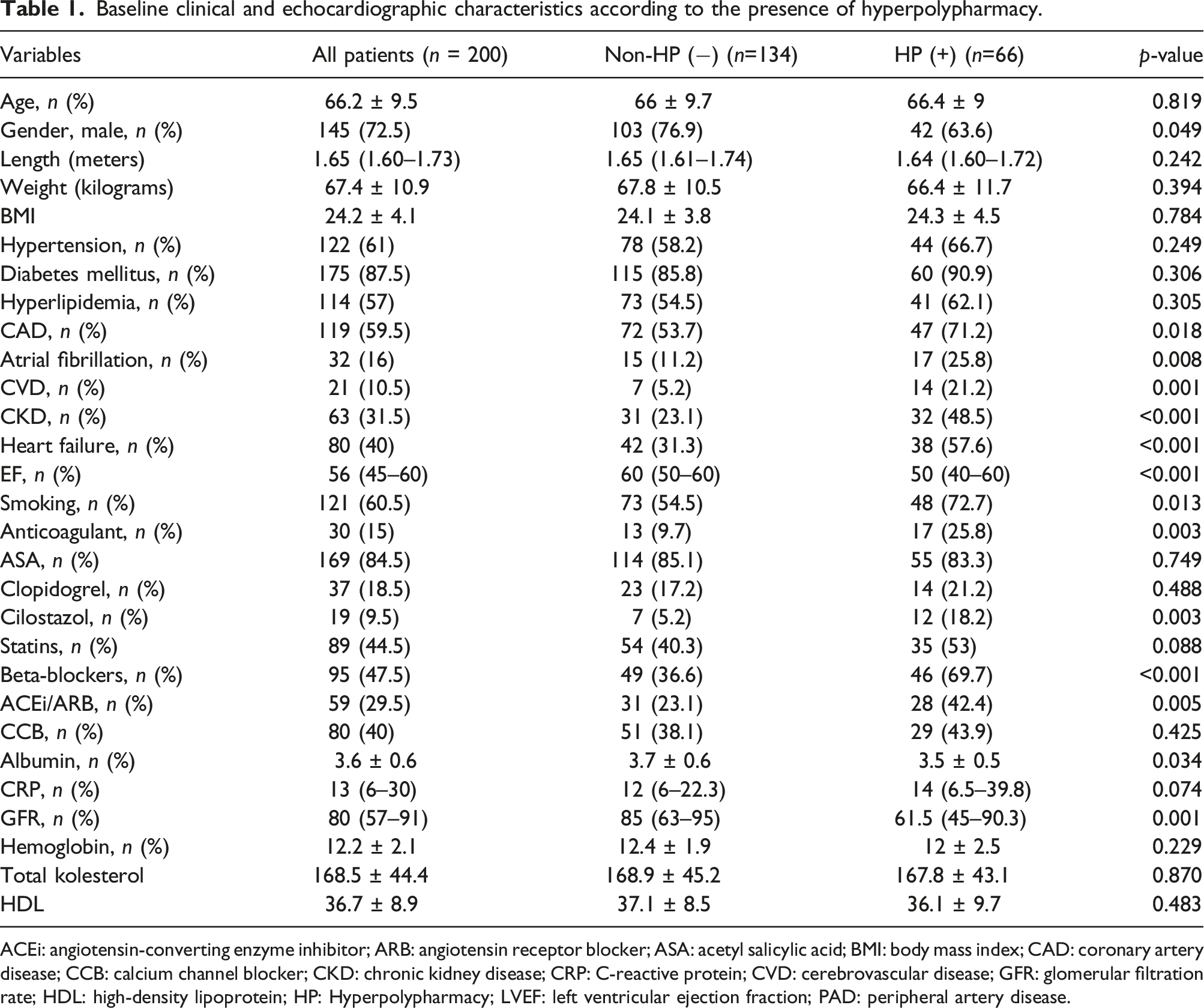
ACEi: angiotensin-converting enzyme inhibitor; ARB: angiotensin receptor blocker; ASA: acetyl salicylic acid; BMI: body mass index; CAD: coronary artery disease; CCB: calcium channel blocker; CKD: chronic kidney disease; CRP: C-reactive protein; CVD: cerebrovascular disease; GFR: glomerular filtration rate; HDL: high-density lipoprotein; HP: Hyperpolypharmacy; LVEF: left ventricular ejection fraction; PAD: peripheral artery disease.
Medication profile according to hyperpolypharmacy.
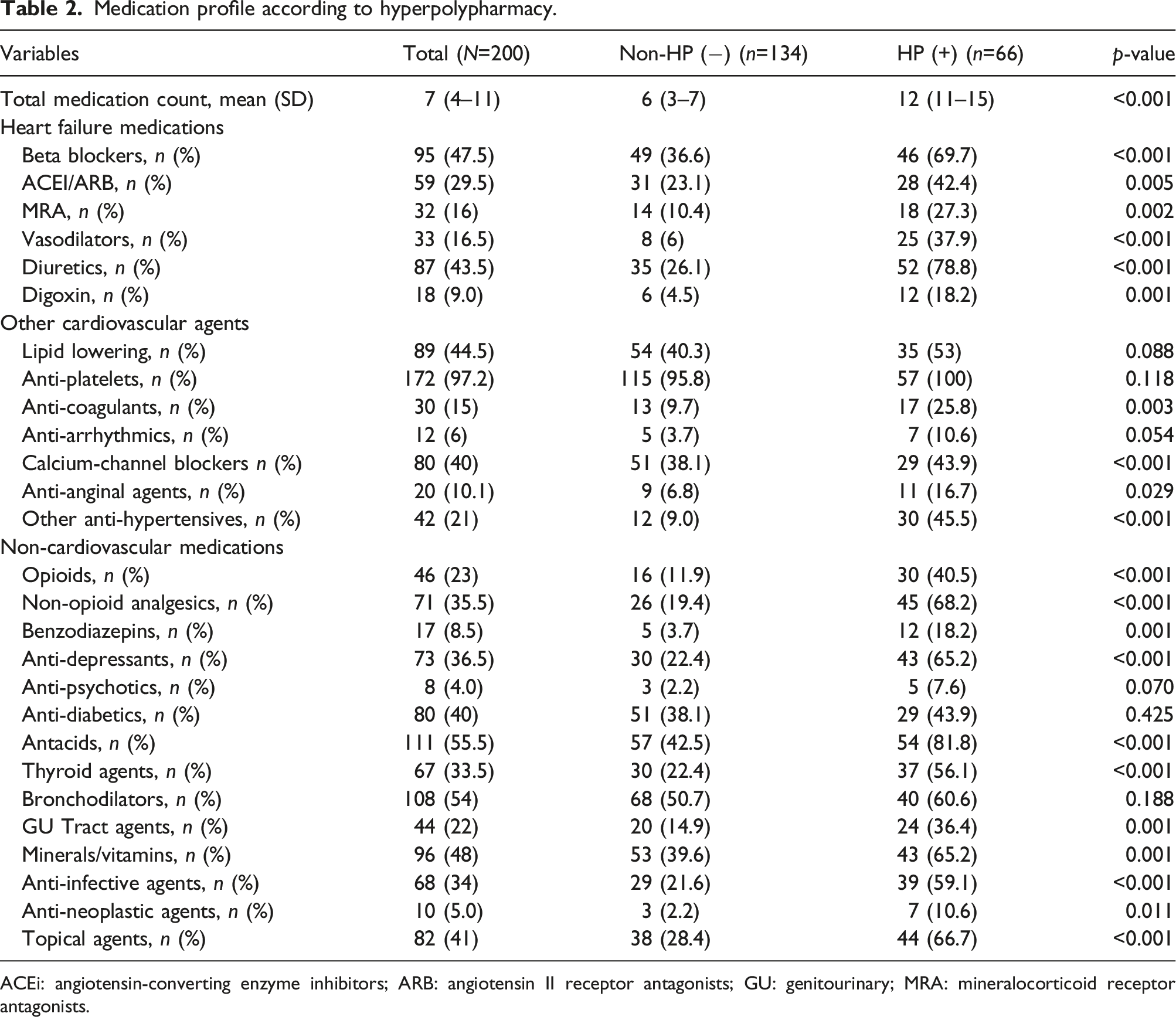
ACEi: angiotensin-converting enzyme inhibitors; ARB: angiotensin II receptor antagonists; GU: genitourinary; MRA: mineralocorticoid receptor antagonists.

Dispersion of drug groups according to Multum database.
Procedural and clinical follow-up variables of whole study population.
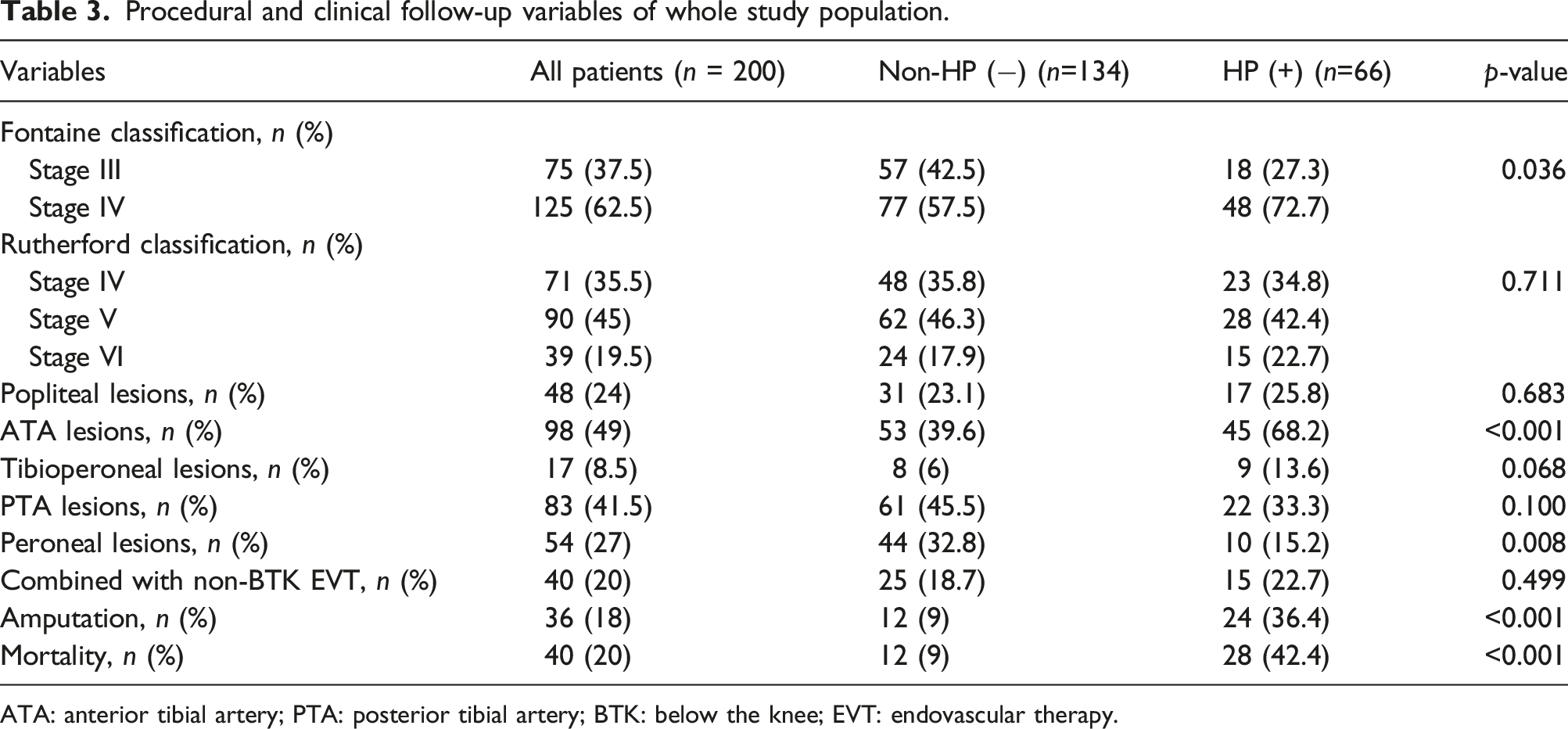
ATA: anterior tibial artery; PTA: posterior tibial artery; BTK: below the knee; EVT: endovascular therapy.
148 patients reached 1-year follow-up. A total of 40 patients were lost. The incidence of 1-year amputation [24 (36.4) versus 12 (9), p<.001] and mortality [28 (42.4) versus 12 (9), p<.001] were higher in patients with hyperpolypharmacy.
Univariate and multivariate cox regression analysis of independent predictors of 1-year amputation.
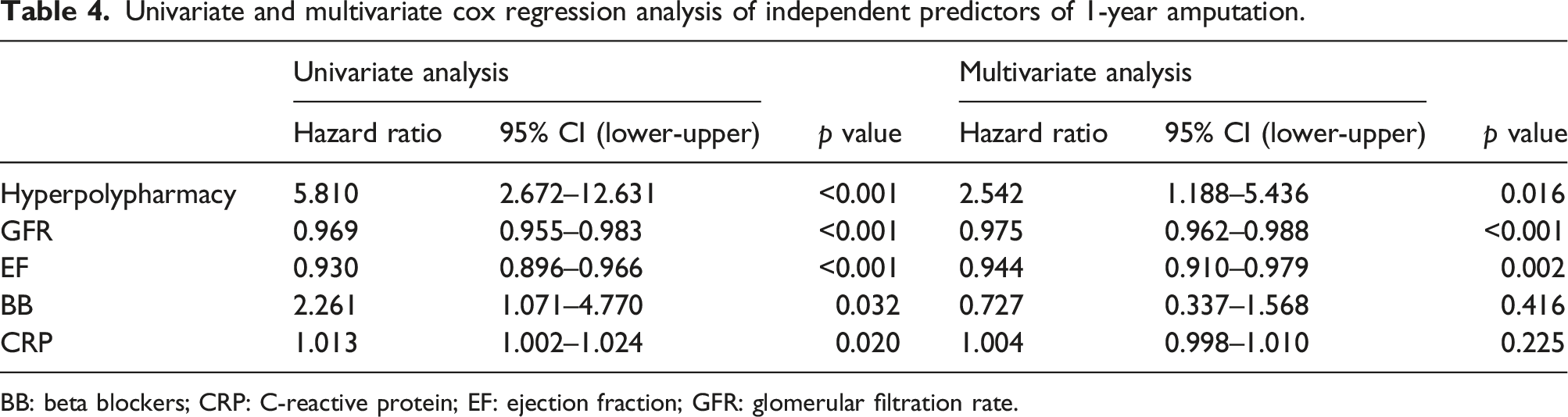
BB: beta blockers; CRP: C-reactive protein; EF: ejection fraction; GFR: glomerular filtration rate.
Univariate and multivariate cox regression analysis of independent predictors of 1-year mortality.
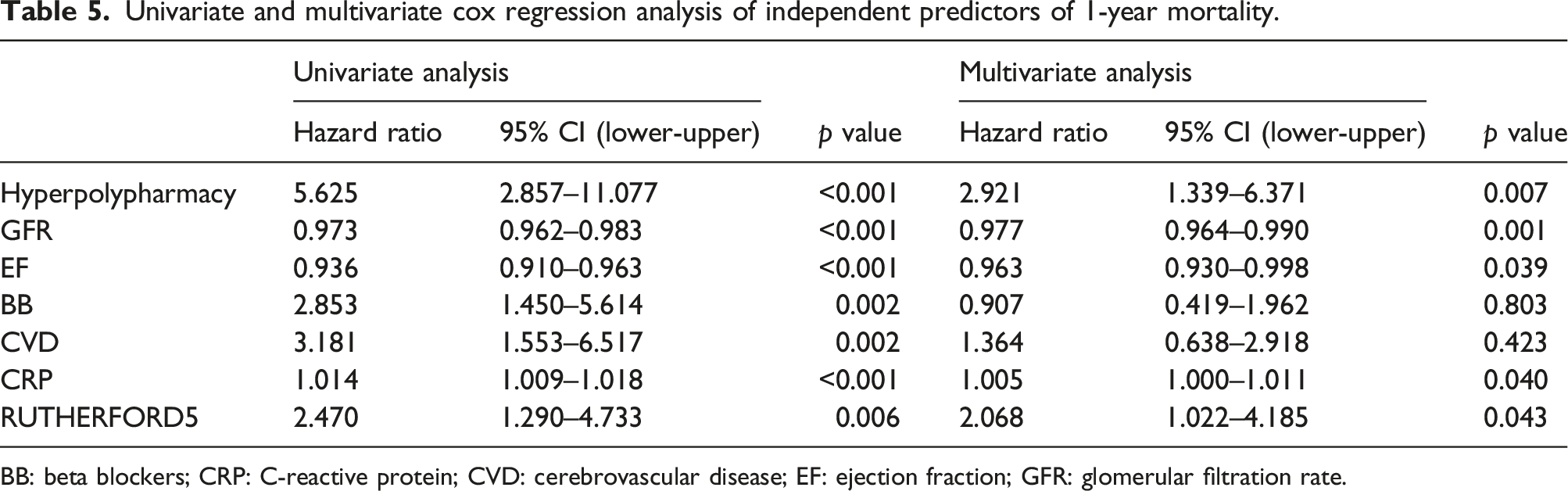
BB: beta blockers; CRP: C-reactive protein; CVD: cerebrovascular disease; EF: ejection fraction; GFR: glomerular filtration rate.
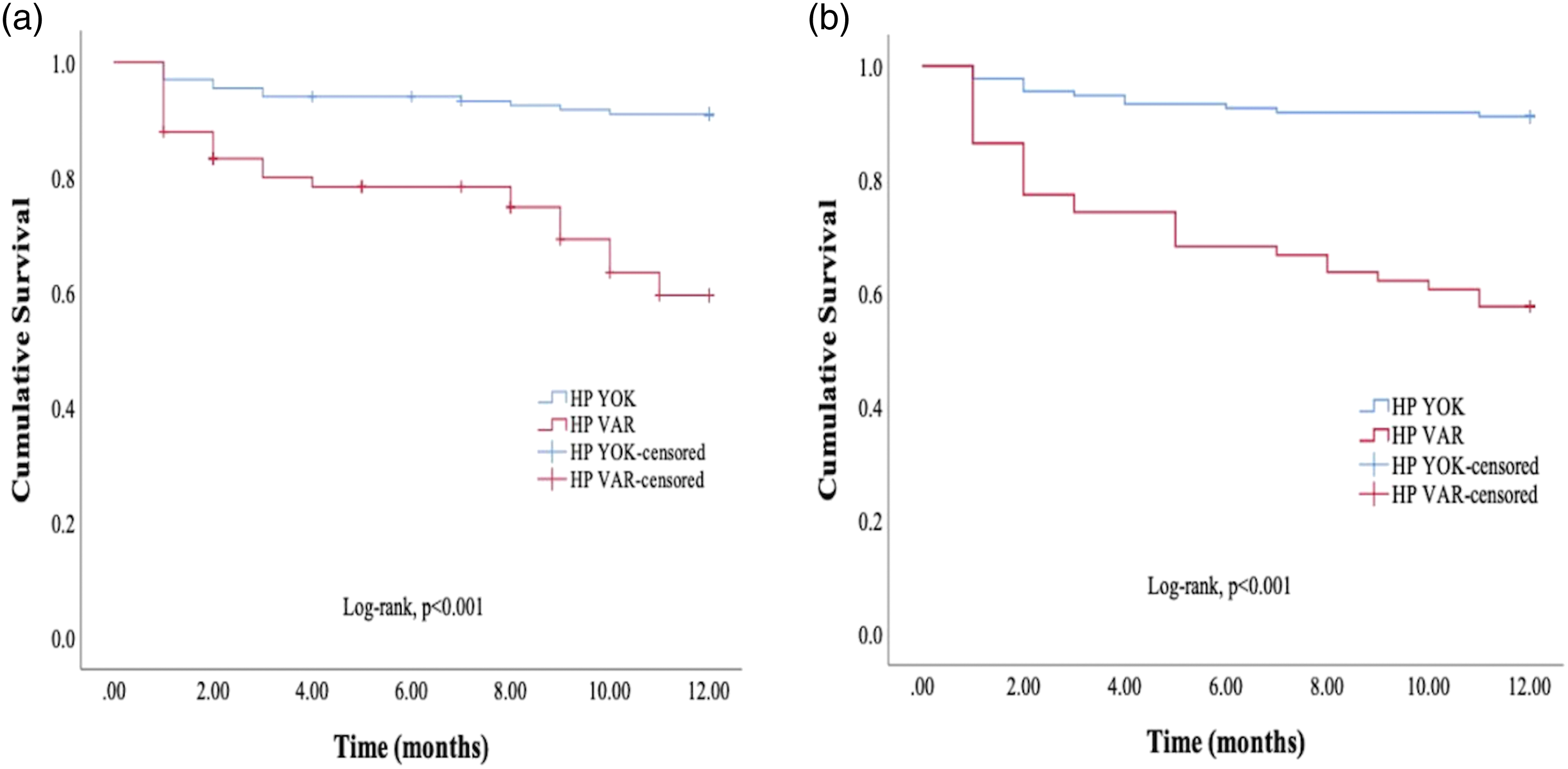
To determine the cut-off value for the hyperpolypharmacy that best detects the presence of 1-year mortality, the (ROC) curve was drawn (Figure 2) and the cut-off value was determined as the use of 10 or more drugs the using Youden index (AUC; 0.795, 95% CI: 0.729–0.861, p <.001). This cut-off value could detect the presence of 1-year mortality with 67.5% sensitivity and 79.4% specificity. The Kaplan–Meier method showed a significant difference (rank p <.001 between log groups) (Figure 3), and the presence of hyperpolypharmacy was associated with 1-year amputation and mortality. ROC curve for hyperpolypharmacy, a predictor of 1-year mortality. Kaplan–Meier survival curves for hyperpolypharmacy in 1-year mortality (a) and 1-year amputation (b).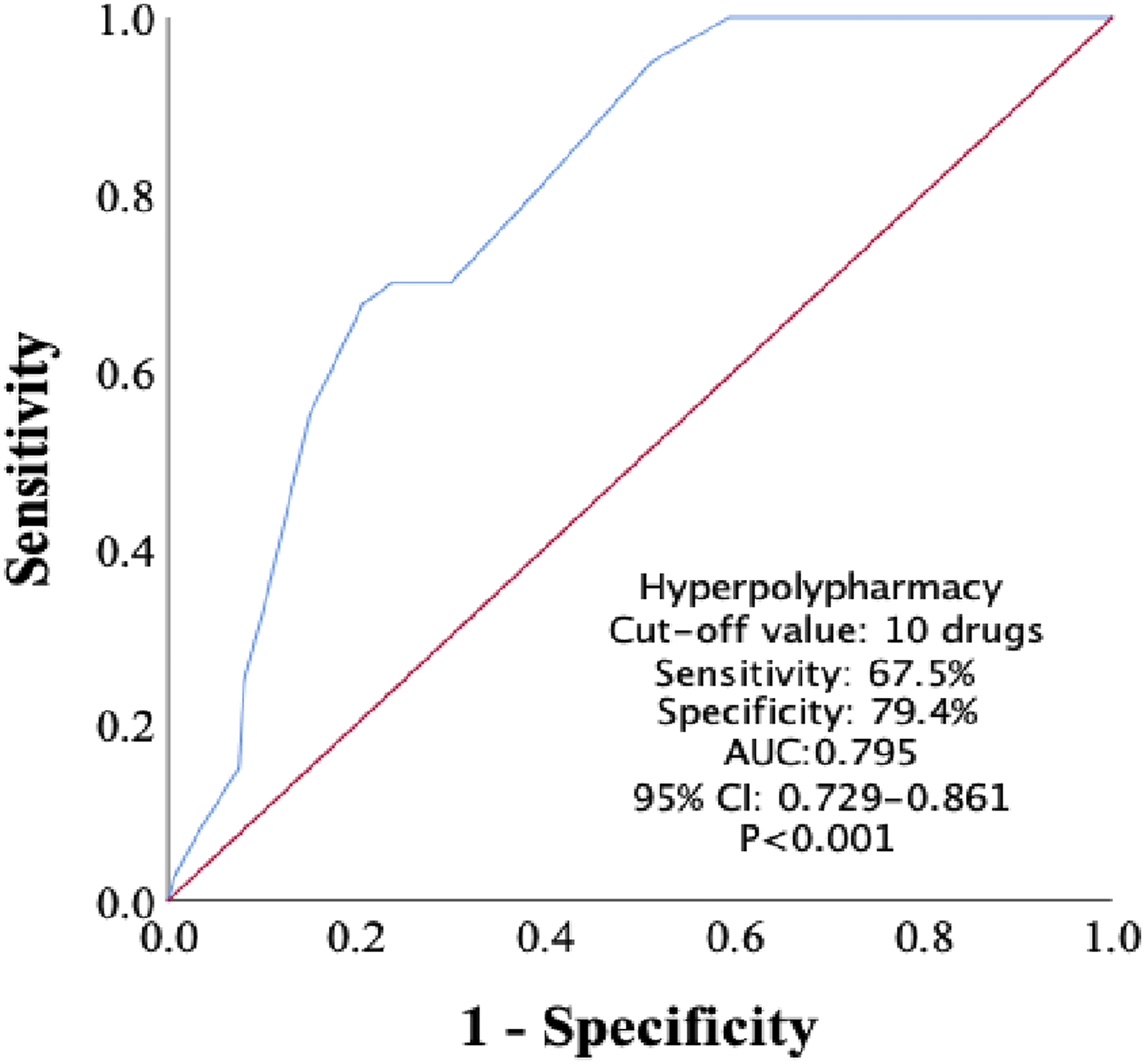
Discussion
To our knowledge, this is the first study to examine the predictive value of medication burden in patients who underwent endovascular therapy for CLI. In our single-center study in which patients with critical leg ischemia with below-knee lesions were analyzed retrospectively, we found hyperpolypharmacy in 33% of the patients. The results of the present study show that hyperpolypharmacy is highly prevalent among CLI patients with below-the-knee lesions. Importantly, our findings demonstrate that hyperpolypharmacy is associated with 1-year mortality and index artery-related amputation in CLI. Hyperpolypharmacy together with low LVEF and low GFR, which are well-known factors in this regard, were determined as independent predictors of poor outcomes in our study population.
Critical limb ischemia is the progressive form of atherosclerotic peripheral artery disease, and increasing age and comorbid factors accelerate the emergence of this process. 1 Although surgical treatment is frequently used in the treatment of lower knee lesions, advances in interventional treatments have increased the success of the endovascular approach and reduced the frequency of complications.17,18 However, the outcome of lesions that have reached CLI is still not promising. Treatment approaches in patients with CLI are developing day by day. Despite developments such as endovascular developments, the production of new catheters, the discovery of new guidewires, an increase in experienced operators and centers in this field, as well as innovations in surgical techniques, long-term outcomes continue to be troubling. 1-year mortality rates vary between 12%–26%, and the 20% mortality rate in our study seems to be compatible with the current literature.9,19 Major amputation rates are still at levels, with the rate of 18% in our study similar to the rates of 16%–20% shown in previous studies.1,20 However, the fact that these rates were 42% and 36%, respectively, in the hyperpolypharmacy group, which determines fragility, emphasizes the importance of drug use as a prognostic factor.
Algorithms for preoperative risk assessment and estimation of outcomes are changing and renewing every day. Since the prognostic aspect of fragility in cardiovascular diseases was understood, many studies have confirmed and expanded this topic.11,21 As a matter of fact, the role of fragility in peripheral arterial patients has been demonstrated by recent studies.5,22 There are many different parameters used to describe fragility, and tools such as the Charlson comorbidity index, sarcopenia, and comorbidity polypharmacy index have been defined in this regard. As the elder population increases, drug use increases, and an essential part of the geriatric evaluation is to detect and prevent polypharmacy.23–25 Also, the increase in the aging population has caused polypharmacy, which for long periods was only a part of geriatric studies, to become a clinical entity that has been evaluated in many fields. Recently, the importance of polypharmacy in cardiovascular diseases has begun to be understood. The adverse effects of multiple drug use in heart failure patients were demonstrated in the study of Unlu et al. 13 The literature on the definition of polypharmacy has a consensus on the use of ≥5 drugs. 26 However, the increasing burden of disease causes the five drug cut-off values to be very low for many patient groups. For this reason, the concept of hyperpolypharmacy emerged and expressed the use of ≥10 drugs. Multiple drug use in cardiovascular patient groups also causes studies on this population to be conducted on hyperpolypharmacy. ATC and Multum are the most frequently used criteria in drug classification, and in our study, we adopted the classification used by Unlu et al.
Besides hyperpolypharmacy, low GFR and low LVEF were also detected as independent predictors for 1-year amputation in multivariate analysis. Renal dysfunction is an essential factor that determines the prognosis of peripheral artery disease patients both in the early and long term. 27 Not only the presence of renal failure but also its severity causes an increase in both amputation and mortality rates. 28 Worsening of the left ventricular ejection fraction continues to be one of the main criteria determining the outcome in all cardiovascular diseases, and the results of our study once again prove this. 29 In our study, CRP, which is one of the other factors that have predictive value in terms of 1-year mortality, was also found to be an important prognostic factor in previous studies as an indicator of the inflammatory process.22,30 Similarly, the Rutherford class, which shows the severity of PAD, stands out as an essential factor showing the 1-year survival of the patients in our study population.
The present study has several limitations. First of all, this was a single-center and retrospective study. The partially low sample size in our study is one of the important limitations. Due to the insufficient number of the study population, patients were not ideally balanced for demographics, comorbidities, and severity of CLI. Thus, large prospective cohort studies are needed to fully appreciate and validate our findings. In addition, other parameters evaluating frailty, such as the Charlson comorbidity index, albumin levels, and sarcopenia, were not used in our study. Also, we were unable to capture any post-procedure management, which could also have affected long-term clinical endpoints. When determining the medication count, more than one pharmacologically active ingredient in a single pill (e.g., combination pills) and pill load (more than one pill of the same drug) was not taken into account. In addition, drug dosages have not been fully determined. All these factors may further contribute to medication burden and complexity in drug regimens and thus may be a topic for future research.
Conclusion
We found a high prevalence of drug use in patients' CLI. Hyperpolypharmacy was significantly associated with 1-year mortality and major amputation in CLI patients. The number of drug use in CLI patients should be taken into account, and unneeded drug use should be prevented and the drug count of the patients should be decreased. Frailty is highly prevalent among CLI patients and is related to the severity of limb threat. Hyperpolypharmacy may be a valuable adjunct to patient risk assessment in CLI.
Footnotes
Acknowledgments
All authors contributed to the understanding and design of the study. Material preparation and data collection studies were carried out by Muammer Karakayalı, Ceren Yildirim Karakan, Seda Tükenmez Karakurt, and Gökhan Demirci. Language assistance was provided by Arda Güler, and Ali Evsen. Statistical analysis was made by Serkan Aslan. The first draft of the article was written by Mehmet altunova and all authors commented on previous versions of the article. The proof reading of the article was made by Mehmet Ertürk. All authors have read and approved the final article. The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted in accordance with principles of the Declaration of Helsinki and approved by the Clinical Trials Ethics Committee.