
Abstract
Objective
Many techniques are available for the intraoperative assessment of brain perfusion during carotid endarterectomy, such as carotid stump pressure, near-infrared spectroscopy, somatosensory evoked potentials, transcranial Doppler, electroencephalography, and clinical assessment. The decision for selective carotid shunt insertion is dependent on clinical deterioration or the detection of cerebral hypoperfusion after cross-clamping of the internal carotid artery. Monitoring cerebral oximetry using near-infrared spectroscopy is a noninvasive technique for cerebral oxygen saturation measurement, reflecting changes in cerebral blood flow during carotid endarterectomy. The aim of this study was to evaluate the reliability of near-infrared spectroscopy as a predictor of selective shunting during carotid endarterectomy.
Methods
In total, 47 conventional carotid endarterectomy surgeries were performed at our hospital between March 2016 and December 2021. All surgeries were performed under a regional cervical block supplemented with local infiltration anesthesia. All patients were monitored by cerebral oximetry using bilateral near-infrared spectroscopy probes and clinical assessment through communication with the patient (numerical, visual, and verbal) to indicate a selective shunt. Near-infrared spectroscopy values were recorded before and after internal carotid cross-clamping and after declamping. Any decrease in ipsilateral cerebral oximetry-near-infrared spectroscopy values equal to or more than 20% from the pre-clamping baseline reading associated with deterioration in neurological status (hemiparesis, aphasia, or deterioration in level of consciousness) after internal carotid artery cross-clamping was considered an indication for intraluminal carotid shunting
Results
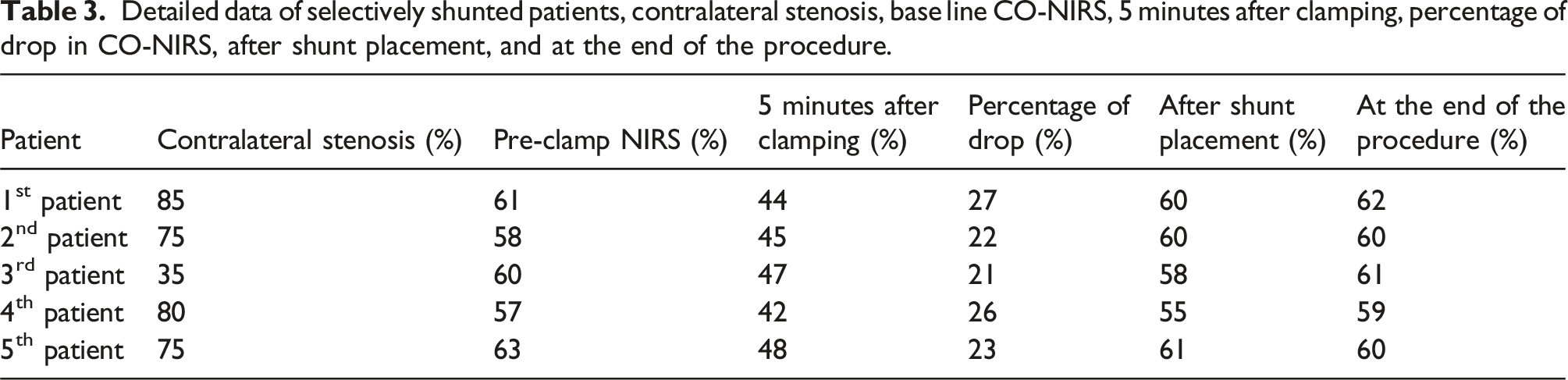
After internal carotid artery cross-clamping, 5 of 47 patients (10.6%) developed a significant drop in cerebral oxygen saturation associated with obvious clinical assessment deterioration in verbal communication and weakness in contralateral arm power. A Pruitt-Inahara carotid shunt was subsequently inserted, and 42 patients remained stable throughout surgery. The average decline in ipsilateral near-infrared spectroscopy values was 23.8% in patients with clinical deterioration. The average decline was 8.6% in patients who remained stable.
Conclusions
Monitoring ipsilateral cerebral oximetry using near-infrared spectroscopy is an easy and reliable method for indicating selective shunting during carotid endarterectomy. A 20% decrease in ipsilateral brain tissue oximetry after internal carotid artery cross-clamping provides a reliable cut-off value for selective intraluminal carotid shunting during carotid endarterectomy.
Introduction
Carotid endarterectomy (CEA) is the standard treatment for high-grade asymptomatic carotid stenosis and accounts for the treatment of more than 50% of symptomatic carotid stenosis cases; however, it is associated with a low but significant risk of complications. 1 Intraoperative stroke is a considerable complication due to insufficient collateral flow, which requires the insertion of a carotid shunt during CEA. 2 However, routine carotid shunting may result in unnecessary shunt use in approximately 85% of patients due to sufficient collateral cerebral perfusion during carotid clamping. 3 Shunt placement can be technically difficult and may lead to complications such as nerve injury, hematoma, infection, and long-term restenosis. 4 An intraluminal carotid shunt adds complexity to the operation process and is associated with a significant risk of stroke, carotid artery dissection, shunt plaque embolization, and air embolism or shunt thrombosis. Some authors prefer to use selective shunting based on reliable monitoring of cerebral perfusion. 5 The decision for selective carotid shunt insertion is dependent on clinical deterioration by awake testing during local anesthesia or detection of cerebral hypoperfusion by different monitoring techniques, such as carotid stump pressure, monitoring of cerebral oximetry using near-infrared spectroscopy (NIRS), somatosensory evoked potentials, or transcranial Doppler and electroencephalogram. 6 NIRS is based on measuring the oxyhemoglobin fraction in the microvasculature under the cerebral cortex. NIRS can monitor the cerebral oxygen saturation of brain tissue continuously and indirectly, reflecting cerebral blood flow changes after carotid cross-clamping during CEA. NIRS has recently been adopted as a monitoring technique in many carotid surgery centers. 7
The aim of our study is to examine the efficacy of NIRS assessment as an indicator for selective shunting during CEA and to set a cutoff NIRS value for selective carotid shunting.
Methods
This was a prospective observational study, after obtaining the approval of the ethical and research committee. All patients were continuously monitored by awake testing and cerebral oximetry-near-infrared spectroscopy (CO-NIRS) during CEA under cervical block supplemented with local anesthesia.
In total, 47 conventional carotid endarterectomy surgeries were performed at our hospital between March 2016 and December 2021. All patients underwent routine preoperative clinical, radiological, and laboratory examinations, and they received dual antiplatelet therapy. All patients underwent duplex arterial ultrasound scan using Konstantinos A. Filis et al. classification criteria depending on the hemodynamical blood flow peak systolic velocity considering more than 250 cm/second at the area of morphological tight stenosis is severe stenosis that were our inclusion criteria for all patient included in the study. 8 At the same time, computed tomographic study during the arterial phase contrast injection using automated cross-sectional view for the head and neck covered the area between the aortic arch and including circle of Willis also the additional radiological including study for all the patients included in this paper using the same NASCET principle by dividing the narrowest internal carotid artery diameter in stenotic segment over the diameter of normal distal internal carotid artery. 9
The inclusion criteria in this study were symptomatic with internal carotid artery stenosis of more than 70% using PSV more than 250 cm/second, cross-sectional tight stenosis ICA more than 70% stenosis without other tandem lesions and intact circle of Willis, and all resolved symptomatic stroke patients depending on Rankin score with 2 and less.
All surgeries were performed under a regional cervical block supplemented with local infiltration anesthesia. Routine monitoring with ECG and pulse oximetry was performed. Intra-arterial blood pressure was continuously measured and recorded. All patients were administered 5000 IU heparin intravenously before carotid clamping. All patients were monitored by cerebral oximetry (CO) using NIRS and awake testing.
A comprehensive neurological exam was performed by vascular and anesthesia team; it was performed at 5, 10, and 15 minutes from the moment of internal carotid clamping. The exam was including numerical, naming, verbal, sensory, and motor examination for the contralateral side including the muscle power grading on addition to visual examination test.
Intraoperative continuous cerebral oximetry monitoring using bilateral NIRS probes (Invos Oximeter, Somanetics-Covidien) over the forehead and below the hairline was performed in all patients. NIRS values were recorded before and after internal carotid cross-clamping and after declamping.
Any decrease in ipsilateral CO-NIRS values equal to or more than 20% associated with deterioration in neurological status (hemiparesis, aphasia, or deterioration in level of consciousness) after ICA cross-clamping was considered an indication for intraluminal carotid shunting. The clamp was released, preparation for shunt insertion was performed, and the lowest NIRS values above both frontal lobes were recorded. A Pruitt-Inahara carotid shunt was inserted in patients who met the previously mentioned criteria for shunting. After the endarterectomy, all arteriotomies were closed using a synthetic bovine pericardial patch.
The patients were observed for one night in the intensive care unit (ICU) after surgery. Vital sign monitoring, neurological examination, and wound observation were also performed. In cases of uneventful stay in the ICU, the patient was transferred to a regular ward for at least two days before discharge.
The statistical analysis was done using SPSS version 26 for statistical analysis; we performed a chi-square test to compare groups of categories and a non-parametric test because the data was less than 30 and Mann–Whitney for others.
Results
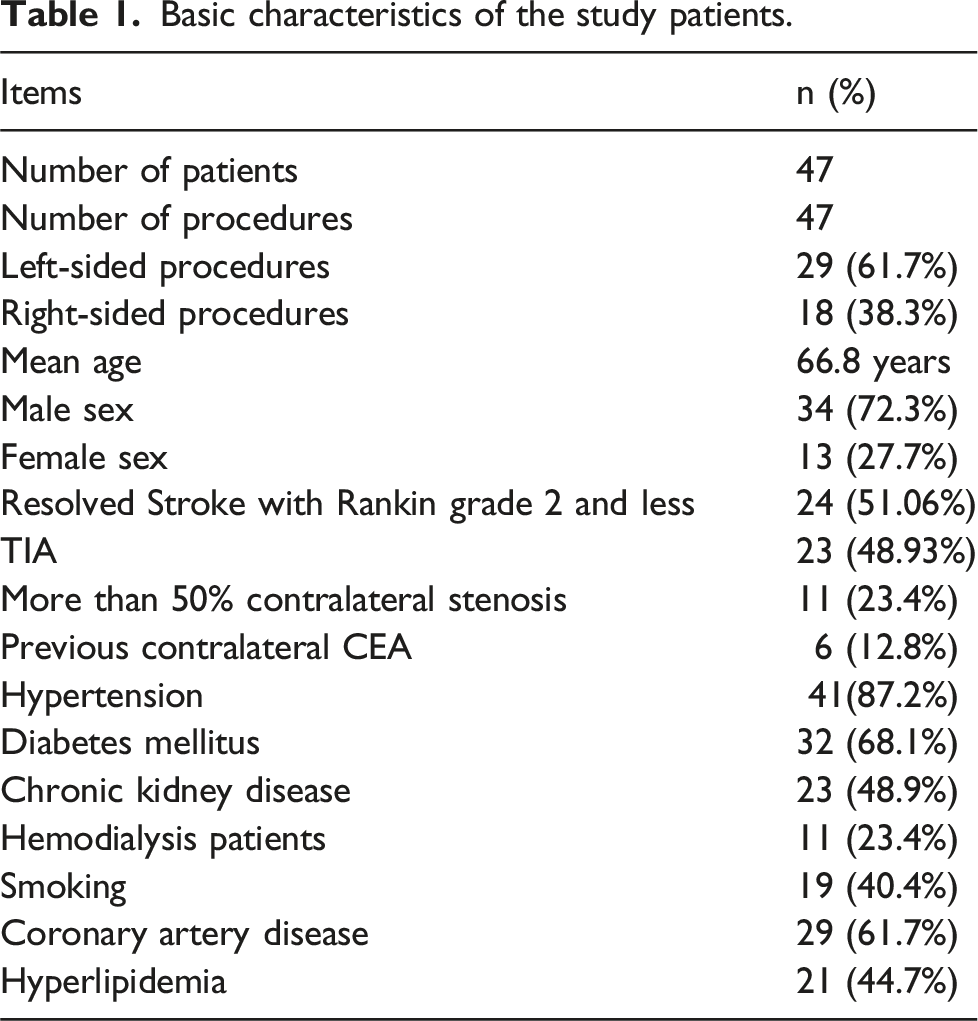
Basic characteristics of the study patients.
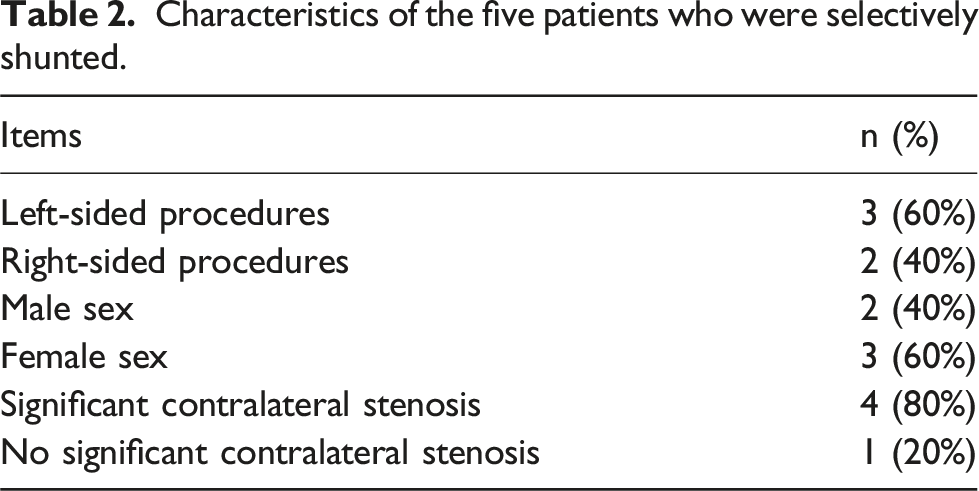
Characteristics of the five patients who were selectively shunted.
Detailed data of selectively shunted patients, contralateral stenosis, base line CO-NIRS, 5 minutes after clamping, percentage of drop in CO-NIRS, after shunt placement, and at the end of the procedure.
Discussion
CEA is the standard treatment for high-grade asymptomatic carotid stenosis and for moderate- to high-grade symptomatic carotid artery stenosis. 10 Any benefit of CEA is closely related to peri-procedural stroke rates, which ideally should be less than 4% in patients with symptomatic carotid artery stenosis. 11 Carotid clamping during CEA may cause critical cerebral ischemia, and even complete stroke, in patients whose collateral circulation is poorly developed, such as those exhibiting an incomplete circle of Willis. 12 Intraluminal carotid shunting is the best method to reduce this stroke risk due to hypoperfusion, but carotid shunting during CEA is also associated with shunt-related stroke.4,13
Some authors suggest the use of selective shunting based on reliable monitoring of cerebral perfusion. 5 The clinical monitoring of neurologic status in an awake patient is considered the gold standard for the detection of cerebral ischemia after carotid clamping during CEA when performed under regional or local anesthesia, but other noninvasive cerebral perfusion measurements should be taken into consideration because clinical neurological deterioration might go unnoticed due to missed diagnosis of minor neurologic deficits. 6 For example, cerebral oxygen saturation, monitored by NIRS, can effectively evaluate cerebral blood flow after carotid cross-clamping. 14 NIRS can be used in all patients, is easy to use, and can be interpreted by the anesthesiologist and surgeon to decide the need for selective shunting. 15
The mechanism of NIRS is based on the fact that oxygenated and deoxygenated hemoglobin have characteristic and different absorption spectra in the near-infrared region, and their relative concentrations in tissues can be determined by their relative absorption of light at specific wavelengths. NIRS systems have been developed to directly measure both light scattering and absorption in tissues. Time domain systems measure the time of flight of photons through tissue, whereas frequency domain NIRS measures the phase shift of intensity-modulated sources.16,17 The primary light-absorbing molecules in tissue are metal complex chromophores, hemoglobin, bilirubin, and cytochromes. 18 The first commercial cerebral oximetry device (INVOS3100w) was introduced in 1993 by Somanetics Corporation (Troy, Michigan). Several authors have shown that cerebral oximetry monitoring could be a valuable tool for the detection of cerebral ischemia during CEA. 7 The clinical interest in NIRS remains for monitoring critical surgical patients during CEA, cardiac surgery, and neurosurgery. 19
The first comparison between NIRS and the established (gold standard) clinical neurological examination was published by Samra et al. 19 in 2000. In a retrospective analysis of 94 CEA cases performed under regional anesthesia, 10 patients who developed neurological symptoms of cerebral ischemia had significantly greater reductions in cerebral oxygen saturation from baseline compared with those with no neurologic symptoms. Using logistic probability analysis, the authors suggested that a reduction in cerebral oxygen saturation of 20% from baseline provided the optimum sensitivity–specificity balance, with a sensitivity and specificity of 80% and 82.2%, respectively. However, in a subsequent study of 594 patients undergoing CEA under general anesthesia, the authors used receiver operating characteristic analysis and identified a much smaller reduction of 11.7% points from baseline as the optimal predictor of post-operative neurologic dysfunction. 20
Another study conducted by Ali et al. 6 used triple assessment techniques (cerebral oximetry, transcranial Doppler, and awake testing) to assess the reliability of cerebral oximetry and transcranial Doppler for carotid shunting. In the aforementioned study, 8 out of 49 patients (16.3%) needed carotid shunting based on awake testing, and 6 of these patients had a >20% drop in cerebral oxygen saturation and a >50% drop in mean flow velocity on transcranial Doppler. However, 2 patients had a non-significant drop in both cerebral oxygen saturation and mean flow velocity (false negative). In the non-shunted group (41 of 49), only one patient had a significant drop in cerebral oxygen saturation (false positive), while 10 of 41 patients had a >50% drop in mean flow velocity. This represents a sensitivity of 75% and a specificity of 97.5% for cerebral oxygenation, compared with a sensitivity of 75% and a specificity of 75% for transcranial Doppler in the detection of the need for shunting. 21 They concluded that a combination of both methods does not add to the accuracy of detecting carotid shunting. 6 In 2017, a study by Jonsson et al. 22 included 185 patients who underwent CEA under local anesthesia with stump pressure and compared the process with NIRS. The authors concluded that NIRS was highly sensitive with acceptable specificity, which makes NIRS a good alternative to stump pressure and even better for continuous assessment. When the stump pressure is less than 30 to 40 mmHg, it is associated with a drop in cerebral oxygenation by 10% to 20% from the baseline after cross-clamping. 21
Conclusion
Monitoring ipsilateral cerebral oximetry using NIRS is an easy and reliable method for indicating selective shunting during carotid endarterectomy. A 20% decrease in ipsilateral brain tissue oximetry after ICA cross-clamping provides a reliable cut-off value for selective intraluminal carotid shunting during CEA.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.