
Abstract
Objectives
Endoleaks are important complications of endovascular aortic repair. Usually, endoleaks are judged indirectly by aortography or postoperative computed tomography. However, findings from these modalities are difficult to distinguish because of the divergency of endoleaks. Few studies have reported direct visualization of endoleaks. Herein, we introduce a direct procedure for intraoperatively evaluating endoleaks using angioscopy.
Methods
From April 2023, consecutive patients with an abdominal aortic aneurysm, except emergency cases and those of narrow access, seen at Sunagawa City Medical Center were enrolled in our study. Endoleaks were detected by intraoperative angioscopy using a novel endovascular procedure.
Results
Seven patients underwent endovascular aortic repair of an abdominal aortic aneurysm with intraoperative angioscopy. None of the enrolled patients experienced complications. The procedure revealed types 2, 3a, and 4 endoleaks.
Conclusions
This is the first study to demonstrate intraoperative visualization of endoleaks using angioscopy. Direct findings observed by this novel procedure might provide information on the velocity and volume of the endoleak, providing comprehensive insights into the intra-sac hemodynamics after the endovascular aortic repair.
Introduction
Endoleaks are important complications of endovascular aortic repair (EVAR). 1 In general, endoleaks are judged indirectly by aortography (AG) or postoperative computed tomography (CT). However, findings from AG images or CT scans are difficult to distinguish because of the divergency of endoleaks. 2 Few studies have reported direct visualization of endoleaks. Recently, in the field of aortic intervention, aortic angioscopy has been used to visualize cholesterol crystals 3 and intimal tears after aortic dissection. 4 Here, we introduce a direct procedure for intraoperatively evaluating endoleaks using angioscopy.
Methods
Patient enrollment
The characteristics of enrolled patients.
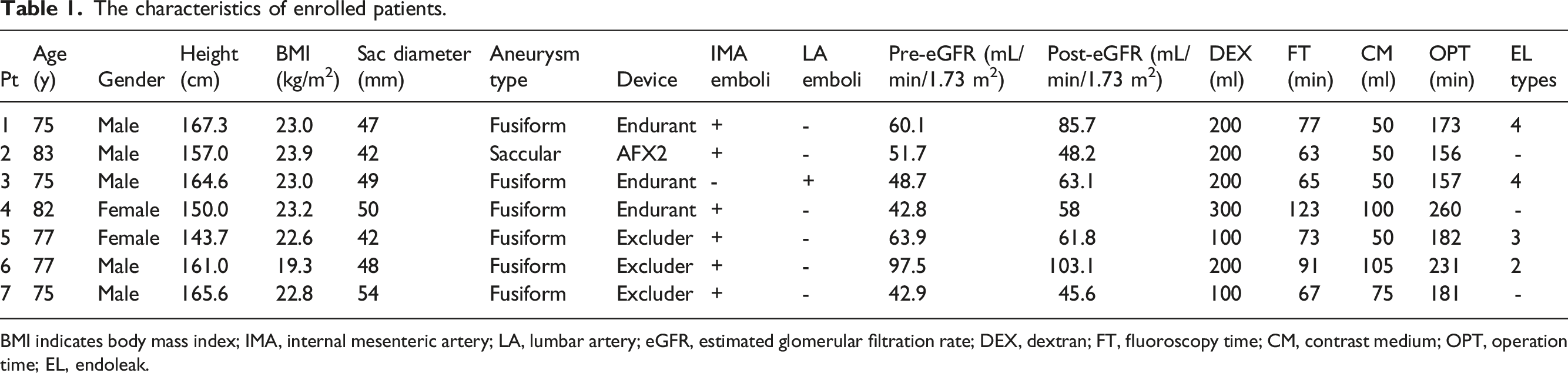
BMI indicates body mass index; IMA, internal mesenteric artery; LA, lumbar artery; eGFR, estimated glomerular filtration rate; DEX, dextran; FT, fluoroscopy time; CM, contrast medium; OPT, operation time; EL, endoleak.
Procedure details
Procedural details are illustrated in Figure 1. Under general anesthesia, bilateral percutaneous common femoral artery access was obtained using suture-mediated ProGlide closure devices (Abbott, Abbott Park, Ill, USA). To prevent type 2 endoleaks, the inferior mesenteric artery (IMA) was embolized, unless obstructed, and lumbar arteries (LAs) with a diameter of more than 2 mm were also embolized, if possible. This embolization was performed pre-emptively using the same anesthesia as the EVAR before the endograft deployment. Subsequently, the bifurcated endograft and the ipsilateral leg were deployed with flush abdominal AG. An 18 F DrySeal Flex sheath (W. L. Gore & Associates, Inc., Santa Clara, CA, USA) was inserted through the contralateral access. Following cannulation of the contralateral gate, another 0.035-inch Radifocus guidewire (Terumo Corp, Tokyo, Japan) was placed outside the main device in a perigraft manner from the same access (Figure 1(A)). After deployment of the contralateral leg device (Figure 1(B)), a 4 or 5F angiographic catheter was inserted into the AAA using the previous Radifocus guidewire (Figure 1(C)). The angiographic catheter was perfused with a low-molecular-weight dextran-L injection (Otsuka, Tokushima, Japan). VISIBLE angioscopy (Intertech Medicals, Osaka, Japan), also known as non-obstructive general angioscopy (NOGA),
5
can be delivered through the catheter. Findings were obtained, and the contralateral leg was expanded using a balloon to prevent a type 1b endoleak. Based on the alignment between NOGA and stent graft, we named this method the angioScopy-esCORted Perigraft and Intra-sac ObservatioN (SCORPION) procedure. Schematic of the SCORPION procedure. Before deployment of the endograft, IMA and/or LA embolization was performed pre-emptively and under the same anesthesia that was given for the EVAR. Following deployment of the bifurcated device and ipsilateral leg, the contralateral gate is cannulated using a stiff wire, and a 0.035-inch Radifocus guidewire (Terumo Corp, Tokyo, Japan) is placed outside the main device from the same sheath (a). After the contralateral leg device is deployed, the Radifocus guidewire is placed in a perigraft manner (b). A 4 or 5F angiographic catheter is inserted into the AAA using a Radifocus guidewire, and Smart-i angioscopy (Intertech Medicals, Osaka, Japan) is performed through the catheter (c). SCORPION, angioScopy-esCORted Perigraft and Intra-sac ObservatioN; IMA, inferior mesenteric artery; LA, lumbar artery, EVAR, endovascular aortic repair, AAA, abdominal aortic aneurysm.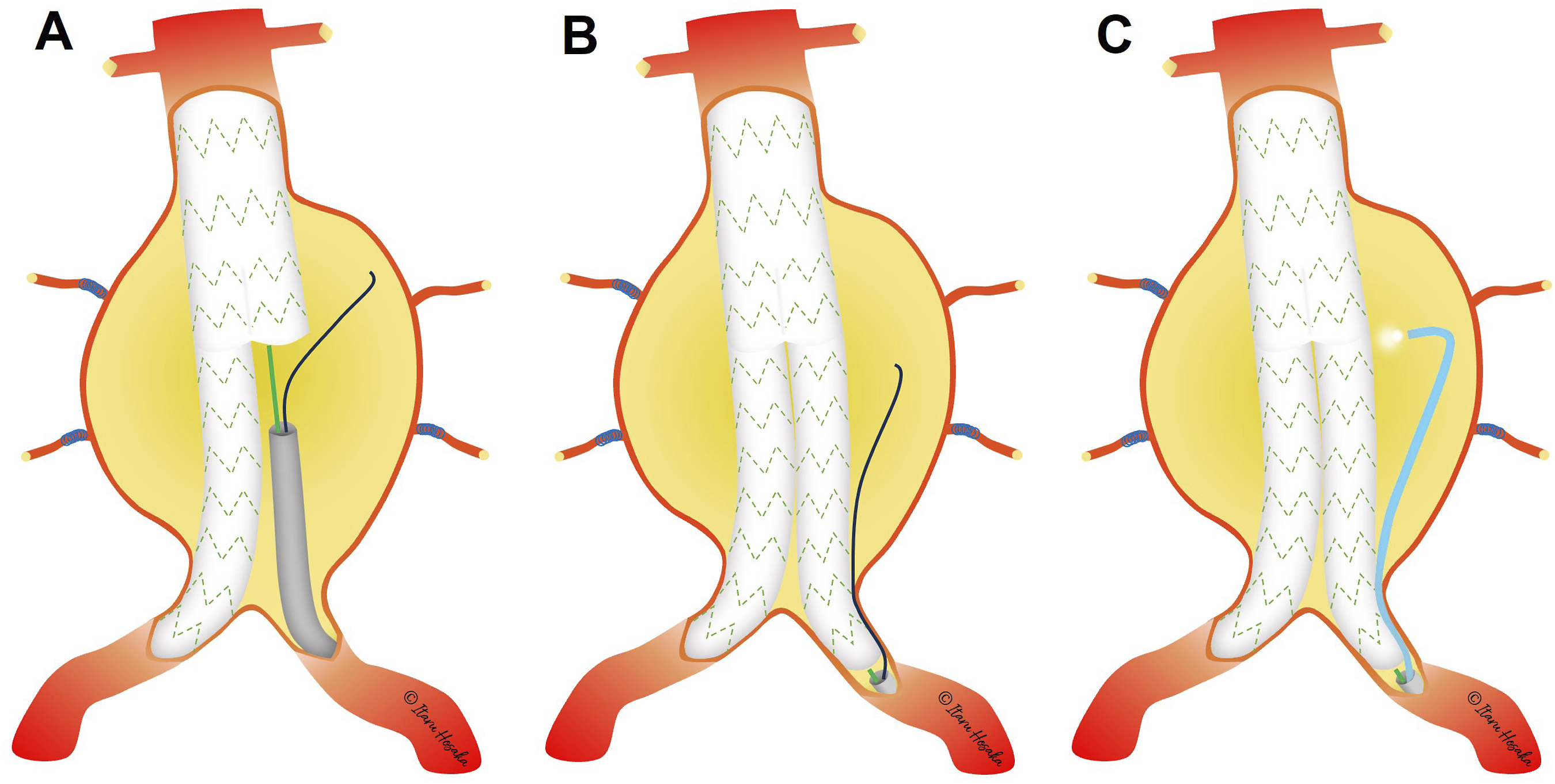
Results
The baseline characteristics of the seven consecutive patients (5 men and 2 women) who underwent EVAR in Sunagawa City Medical Center from April 2023 are shown in Table 1. Endoleaks were confirmed in cases #1, #3, #5, and #6 by the SCORPION procedure. Representative images (case #6) of the detection of a type 2 endoleak by the procedure are shown in Figure 2. In this case, the AAA had a patent IMA and several LAs (Figure 2(A)). An Excluder C3 (W. L. Gore & Associates, Inc., Santa Clara, CA, USA) was deployed after embolization of the IMA, and an angiographic catheter was positioned using the SCORPION procedure (Figure 2(B)). Embolization of the LA was unsuccessful. Intra-sac angiography showed contrast medium washout in the LA and pooling in the sac (Figure 2(C)). Simultaneously acquired findings from intra-sac angioscopy revealed a small hole with a pulsatile blood flow in the AAA wall (Figure 2(D) and Supplementary Video 1). These findings suggested a type 2 endoleak from the ostium of the LA. Postoperative CT showed that the endoleak persisted (Figure 2(E)) and tranexamic acid was prescribed.
6
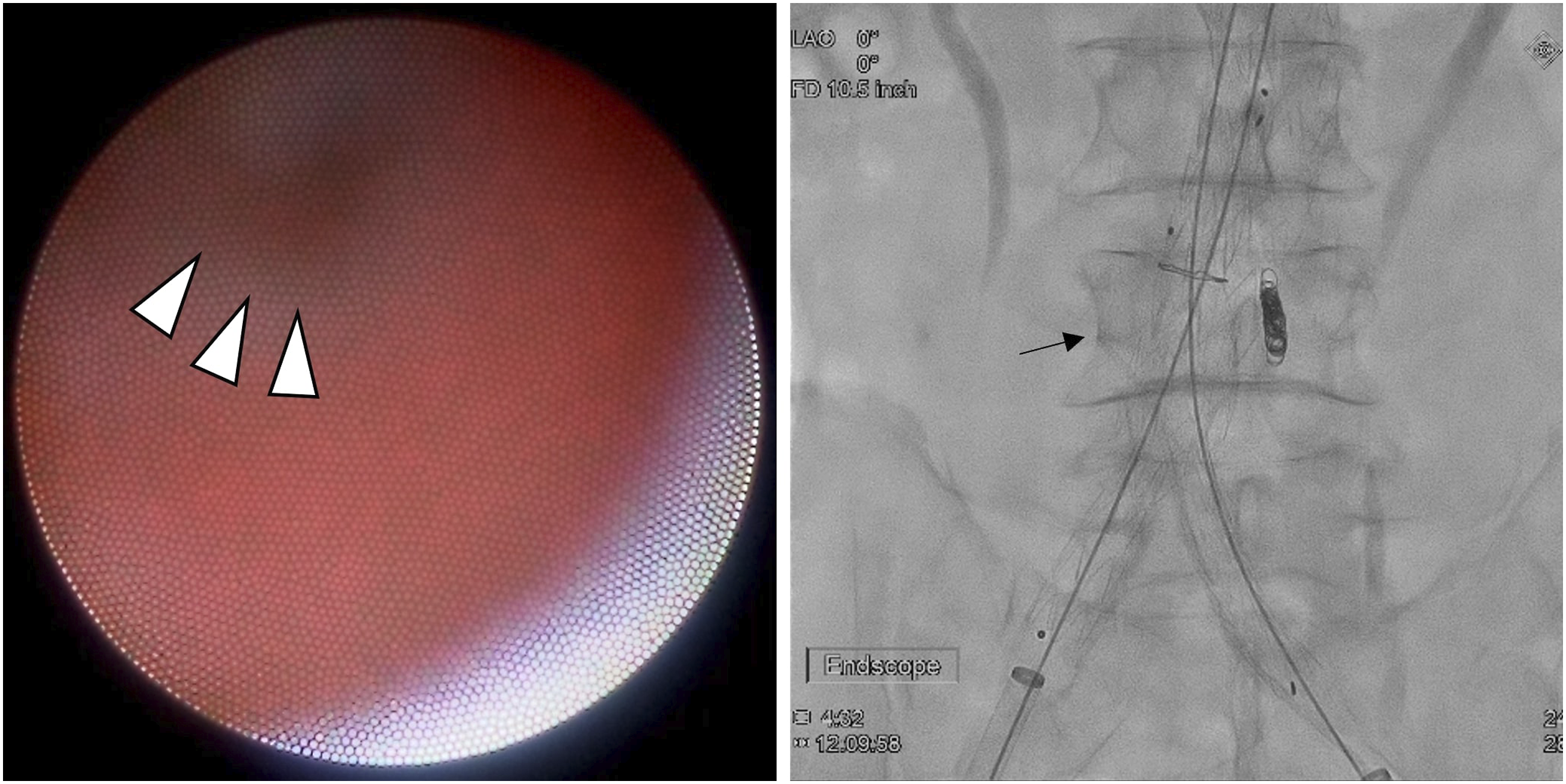
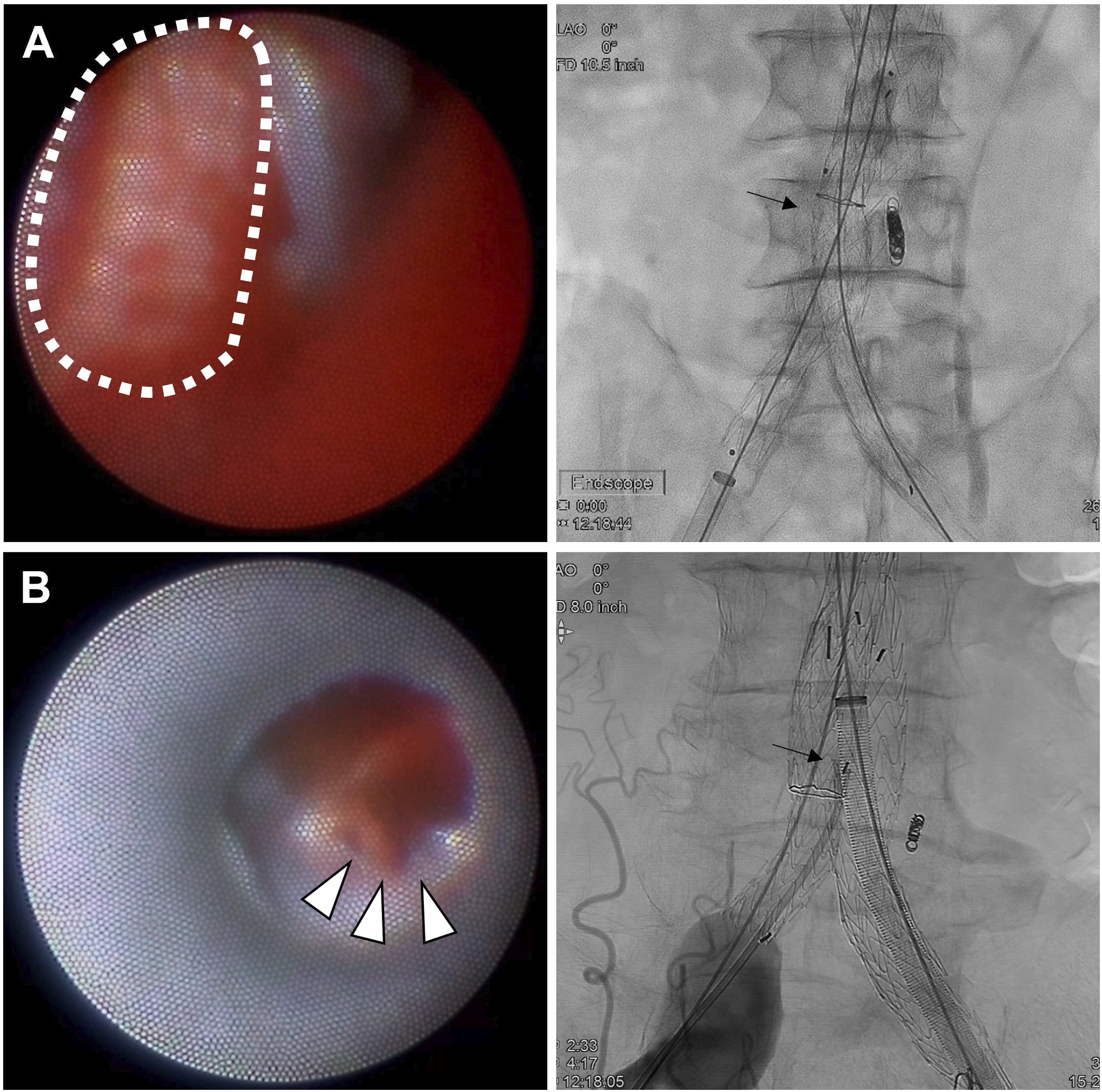
On the other hand, using an Endurant 2 (Medtronic Vascular, Santa Rosa, CA, USA) with the same procedure in case #1, the ostium of the LA was observed without obvious blood flow (Figure 3). In this case, pulsatile blood leakage from the surface of the graft, indicating a type 4 endoleak, was also observed (Figure 4(A) and Supplementary Video 2). A type 4 endoleak was also indicated in case #3 (Table 1). Another endoleak was detected in case #5 using the Excluder C3. A small hole with pulsatile blood flow from the graft surface suggested a type 3 endoleak but uncertainly (Figure 4(B)). Because this finding was located near the leg and not the main body of the endograft, we suspected a type 3a endoleak and performed balloon inflation within the leg of the endograft. The endoleak was unclear in the final AG and undetected in the postoperative CT scan. No complications, including graft migration, access injury, acute kidney injury, and acute heart failure, were confirmed in the present study. In cases #2, #4, and #7, no apparent endoleaks were found (Table 1). Representative images showing the detection of a type 2 endoleak using the SCORPION procedure during intraoperative angioscopy, while simultaneously obtaining fluoroscopy and postoperative CT scans. The three-dimensional model of the abdominal aorta shows an AAA with patent IMA and LA (a). The tip of the angiographic catheter is placed within the sac using the SCORPION procedure after deploying an EVAR device (b; black arrow). Intra-sac angiography shows contrast medium washout (c; upper panel) and pooling in the sac (c; bottom panel), suggesting a type 2 endoleak from the LA. Intraoperative angioscopy reveals a small hole with pulsatile influx from the ostium of the LA (d, upper panel; systolic phase, bottom panel; diastolic phase, asterisk; tunica intima of the AAA, white arrowhead; ostium of the LA). The type 2 endoleak confirmed intraoperatively persists on the postoperative CT scan (e). SCORPION, angioScopy-esCORted Perigraft and Intra-sac ObservatioN; AAA, abdominal aortic aneurysm; IMA, internal mesenteric artery; LA, lumbar artery; EVAR, endovascular aortic repair. Representative images from intraoperative angioscopy and fluoroscopy in a patient without a type 2 endoleak from the ostium LA using the SCORPION procedure. The white arrowheads indicate the ostium of the LA (left panel). In this case, no apparent influx is observed. The black arrow shows the tip of the angiographic catheter (right panel). LA, lumbar artery; SCORPION, angioScopy-esCORted Perigraft and Intra-sac ObservatioN. Representative images showing the detection of other endoleak types using the SCORPION procedure during intraoperative angioscopy and fluoroscopy. Oozing blood suggests a type 4 endoleak (left panel in A, dashed white line; the area of bleeding from the graft surface). A small hole in the graft surface with pulsatile influx indicates a type 3 endoleak (left panel in B, white arrowhead; small hole in the graft). The black arrowheads in the right panel both A and B represent the tip of the angiographic catheter. SCORPION, angioScopy-esCORted Perigraft and Intra-sac ObservatioN.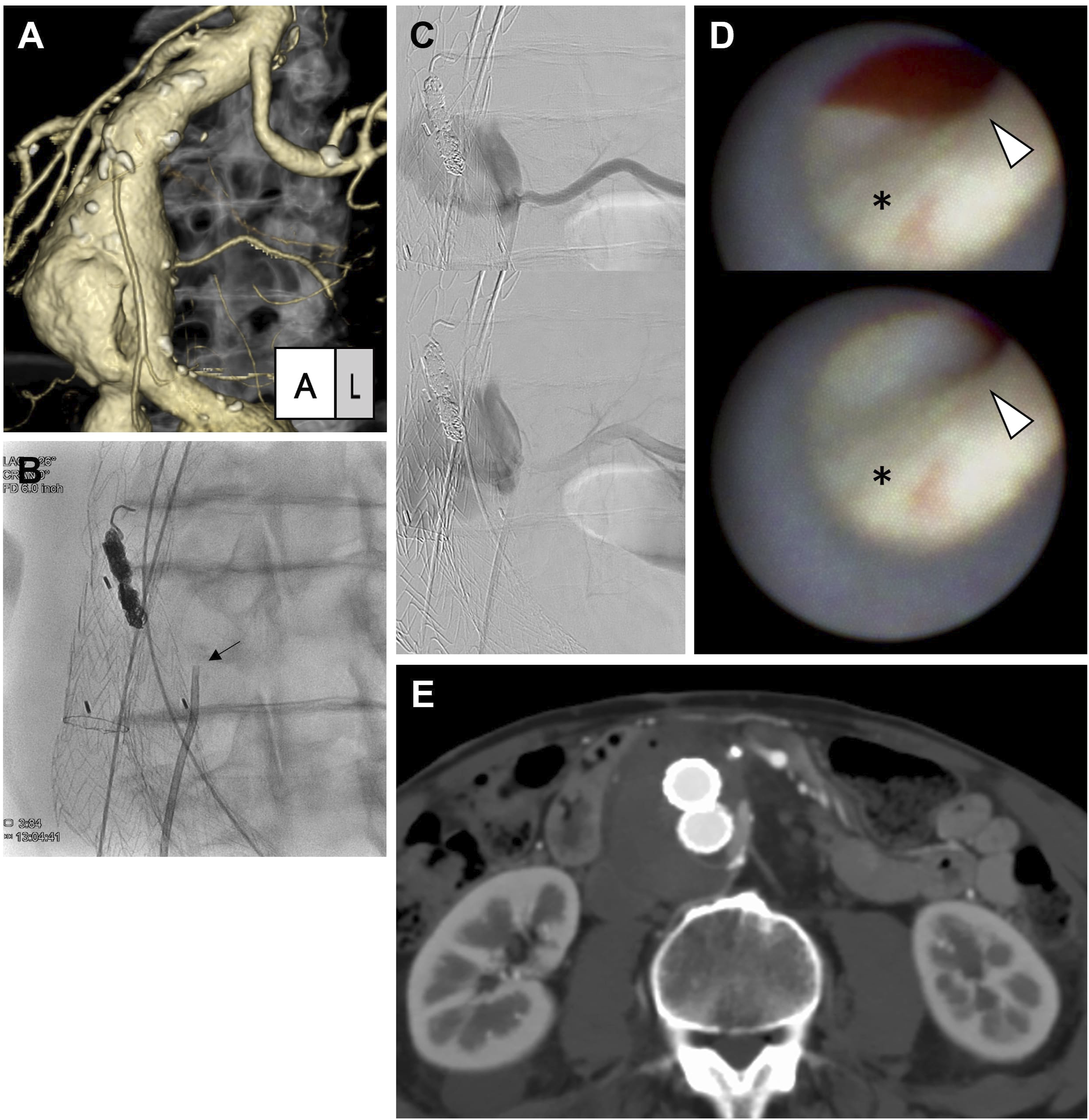
Discussion
The present study showed that intraoperative observation using perigraft-type angioscopy can detect endoleaks without complications. In the cases presented here, types 2, 3, and 4 endoleaks were evident directly by the procedure. Few studies have evaluated endoleaks directly. For the first time, angioscopy revealed an influx of blood from the LA from a type 2 endoleak. This finding suggests that type 2 endoleaks can affect intra-sac hemodynamics after implantation of an EVAR device. Direct intraoperative visualization using an angioscopy-based procedure may be used to clarify the pattern of endoleaks.
Type 2 endoleaks are recognized as a potentially significant entity if the AAA sac diameter enlarges. 7 In recent years, several studies have demonstrated the efficacy of embolization of the aortic side branch artery.4,8 However, the optimal range of intervention remains controversial. Retrospective analyses show that the larger branch vessels (IMA diameter > 3 mm 9 and LA diameter > 2 mm) 10 were at high risk for significant type 2 endoleaks; however, the pathophysiological mechanism behind the relationship between the diameter of the side branch and sac growth has remained unclear. 11 In this study, intra-sac angioscopy enables observation of the velocity and amount of blood flow from the arterial ostium (Supplementary Video 1), leading to the identification of type 2 endoleak functionality. Although cases without postoperative type 2 endoleaks showed no or little influx of blood from the LA by intraoperative angioscopy, pulsatile influx as in case #6 indicated significant type 2 endoleaks (Figure 2(E)). From direct findings by the SCORPION procedure, the larger branches might have contributed to the worse aortic outcome in terms of velocity and volume of blood flow. The proposed procedure could provide novel insights into the pathophysiology of type 2 endoleaks in terms of the direct visualization of intra-sac hemodynamics. Because this pilot study had a small sample size, further studies are needed to clarify the correlation between the functionality of type 2 endoleaks obtained from the procedure and the long-term outcome after EVAR with side branch embolization.
The study has several limitations. First, the observation area by intra-sac catheter-guided angioscopy is restricted owing to the sandwich between the arterial wall and leg graft. When another catheter with a larger diameter is added, the angioscopy may become more flexible. Second, the number of patients was small, and the selection bias of patients would have existed. Type 4 endoleaks are considered a rare phenomenon; however, 2 out of the 7 cases in our study were detected with type 4 endoleaks using the SCORPION procedure. Due to the small sample size in the study, we might have overestimated the incidence of type 4 endoleaks. Alternatively, occult small type 4 endoleaks may actually be more common than previously thought. In several months of outpatient follow-up, these patients have not shown sac expansion. Therefore, the long-term outcome of these endoleaks should be monitored with routine imaging studies. Finally, because the enrolled patients were only Japanese people, it is unclear whether the present findings can be generalized to other ethnicities.
Conclusion
In the present study, intraoperative NOGA enables visualization of endoleaks during EVAR for the first time. Direct findings by the procedure might provide information on the velocity and amount of endoleaks, leading to comprehensive insights for intra-sac hemodynamics after EVAR. Further studies are required to discern whether various patterns of endoleaks can be determined using the procedure.
Supplemental Material
Supplemental Material
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.