
Abstract
Purposes
Abdominal Aortic Aneurysm (AAA) screening via ultrasound in Caucasian males aged 65 and older has proven cost-effective in metropolitan areas. Evidence suggests that with adequate training, individuals without prior sonography experience can achieve accurate aortic measurements. This study evaluates the capability of junior doctors, after brief training, to conduct reliable AAA ultrasound screenings in a rural hospital setting, addressing the gap in speciality surgical services.
Methods
Three junior doctors participated in a 2-hour practical ultrasound training, subsequently performing scans on both inpatients and community volunteers at a regional hospital. The analysis focused on measurement discrepancies within a 5 mm clinically acceptable difference, scanning efficiency, and aneurysm detection accuracy.
Results
A total of 71 participants were included. Among the screenings, 81.7% fell within the clinically acceptable discrepancy range, with 72.7% accuracy in inpatient scans and 95.5% in volunteer scans. Measurement reproducibility improved significantly with the standardisation of ultrasound techniques, and there was excellent agreement among operators in detecting aneurysms. Notably, scanning efficiency improved from the inpatient group to the volunteer group with statistical significance.
Conclusions
Junior doctors demonstrated the ability to efficiently and reproducibly measure the infrarenal aortic diameter at a level comparable to experienced sonographers after only 2 hours of training. A single day of supervised practice is recommended to ensure standardised ultrasound technique. This approach offers a practical, cost-effective supplement to specialist radiology services in rural areas, enhancing access to critical screening procedures without proposing the replacement of professional sonographers.
Introduction
Abdominal Aortic Aneurysm (AAA), defined as an enlargement of the infrarenal abdominal aorta exceeding 3.0 cm, poses a critical risk of life-threatening rupture. 1 In Australia, AAA is responsible for around 1000 deaths annually, underscoring the necessity for effective screening and management strategies. 2 The risk of rupture increases with the aneurysm’s size, with diameters beyond 5.0 cm exhibiting a 3%–5% annual rupture risk. 3 In rural settings, the challenges are compounded by the scarcity of speciality surgical services. A rupture within these contexts necessitates patient transfer to tertiary centres, drastically increasing mortality due to delayed critical care.
Elective AAA repair showcases a markedly lower mortality rate compared to emergency responses to ruptured aneurysms, highlighting the importance of early detection. 4 Ultrasound screening has emerged as a cost-effective strategy for AAA detection, particularly within the Caucasian male population aged 65 and over, showing favourable outcomes compared to other cancer screenings.5–7 Despite the proven efficacy of ultrasound screening in metropolitan areas, the accessibility of such programs in rural Australian settings remains limited, with no formal screening guidelines in place nationally. The variability in ultrasound measurement accuracy between observers has prompted exploration into the potential of non-radiologically trained novices to achieve clinically acceptable measurement variances.8,9
Point-of-Care Ultrasound (POCUS) has shown high sensitivity and specificity when used by emergency physicians and rural generalists for AAA detection.10,11 However, the performance characteristics of ultrasound as a screening tool in remote and rural Australian communities have been inadequately assessed. This study aims to evaluate the capability of junior doctors, following limited POCUS training, to conduct AAA screenings in a rural hospital setting reliably. Additionally, it seeks to explore the demographics and prevalence of AAA in a rural Australian context, hypothesising that junior doctors can maintain inter-observer variability within a 5 mm discrepancy and achieve a consensus on AAA diagnoses in at least 95% of patients.
Methods
Study design
A prospective longitudinal study was conducted at Whyalla Hospital and Health Services, South Australia, from December 14, 2019, to January 5, 2020. Both male and female participants were included in the screening cohort, and an aneurysm was defined as an anteroposterior diameter of greater than 3.0 cm. While standard guidelines typically recommend screening males aged 65 and above, our inclusion criteria starting from age 50 as informed by the high prevalence of cardiovascular risk factors (e.g. smoking and hypertension) within this rural community. This broader inclusion aimed to capture at-risk individuals who might benefit from earlier detection, given the limited access to healthcare resources in these settings. Ethical approval for this study was obtained from the Central Adelaide Local Health Network Human Research Ethics Committee (CALHN HREC).
Contextual background of Whyalla, South Australia
Situated 400 km from Adelaide by road, Whyalla Hospital serves as a regional healthcare entity in rural South Australia. The demographic and health profile of Whyalla, characterised by an ageing population and a relatively high smoking prevalence (36.7%), underscores the critical need for effective AAA screening initiatives within this community. Emergent inpatient transfer by air to the affiliated tertiary centre requires at least 2 hours. Patients with newly diagnosed AAA are referred to a monthly visiting vascular surgeon for either surgical intervention or surveillance.
Ultrasound training and data collection
Three medical interns with limited prior ultrasound experience underwent a standardised training program. This program, accredited by the Australasian Society for Ultrasound in Medicine (ASUM), included online modules and a 2-day workshop focussing on Point-of-Care Ultrasound (POCUS) techniques, specifically for abdominal aorta assessment. 12
Ultrasound examinations were performed using a 2–5 MHz convex probe, following a protocol that emphasised the identification of the abdominal aorta in both longitudinal and axial planes. The protocol aimed for consistent measurement of the anteroposterior diameter of the infrarenal aorta, with each measurement repeated three times for accuracy.13,14 Examinations were conducted without requiring patients to fast, except for community volunteers, who were advised to fast for 2 hours prior to their appointments.
Each operator independently scanned patients and was blinded from each other’s measurements, and to the participants’ medical histories, including any prior aneurysm diagnoses. Data collection included aortic measurements, scan duration, challenges encountered (e.g. bowel gas and body habitus), and previous abdominal imaging results. A 5-mm variance was elected to be the clinically acceptable threshold based on its alignment with the existing literatures of screening practices by novices.8,9 This threshold allows novice operators to identify aneurysms with potential clinical significance, ensuring that cases likely to progress towards high-risk categories are flagged for further evaluation. Visualisation success was defined as the operator’s ability to locate the abdominal aorta, while measurement success referred to obtaining accurate and recordable measurements of the aortic diameter.
We collaborated closely with the specialist radiology department at Whyalla Hospital to ensure alignment between our screening measurements and those obtained by accredited sonographers. Any positive findings were confirmed through follow-up imaging by experienced sonographers, allowing us to validate the accuracy of the junior doctors’ measurements. Additionally, we consulted with the visiting vascular surgery unit prior to commencing the study to establish a clear pathway for managing detected AAAs, ensuring that patients received timely and appropriate care.
Participants were thoroughly informed about the potential consequences of aneurysm screening, including the clinical significance of an AAA diagnosis, follow-up requirements, and treatment options. Information leaflets were provided outlining the next steps if an aneurysm was detected. For patients diagnosed with an AAA, a streamlined referral process ensured timely follow-up with both radiology and vascular surgery services, minimising delays in care.
Statistical analysis
Statistical analysis was conducted using IBM SPSS Statistics. Continuous variables are represented as mean ± standard deviation (SD), with a p-value of less than .05 considered statistically significant. Our analysis focused on assessing the reproducibility and accuracy of ultrasound measurements for detecting AAA across different operators (1 vs 2, 1 vs 3, and 2 vs 3). We used paired t-tests to discern any significant mean differences in measurements and Bland−Altman plots to examine agreement between operators. In the context of AAA analysis, the coefficient of repeatability is compared with a clinically accepted difference (CAD) of 5 mm, and the range of limits of agreement (LOA) [−5 mm; +5 mm]. The proportion, measured in percentages, of the inter-operator measurements that were within 5 mm was calculated. 15
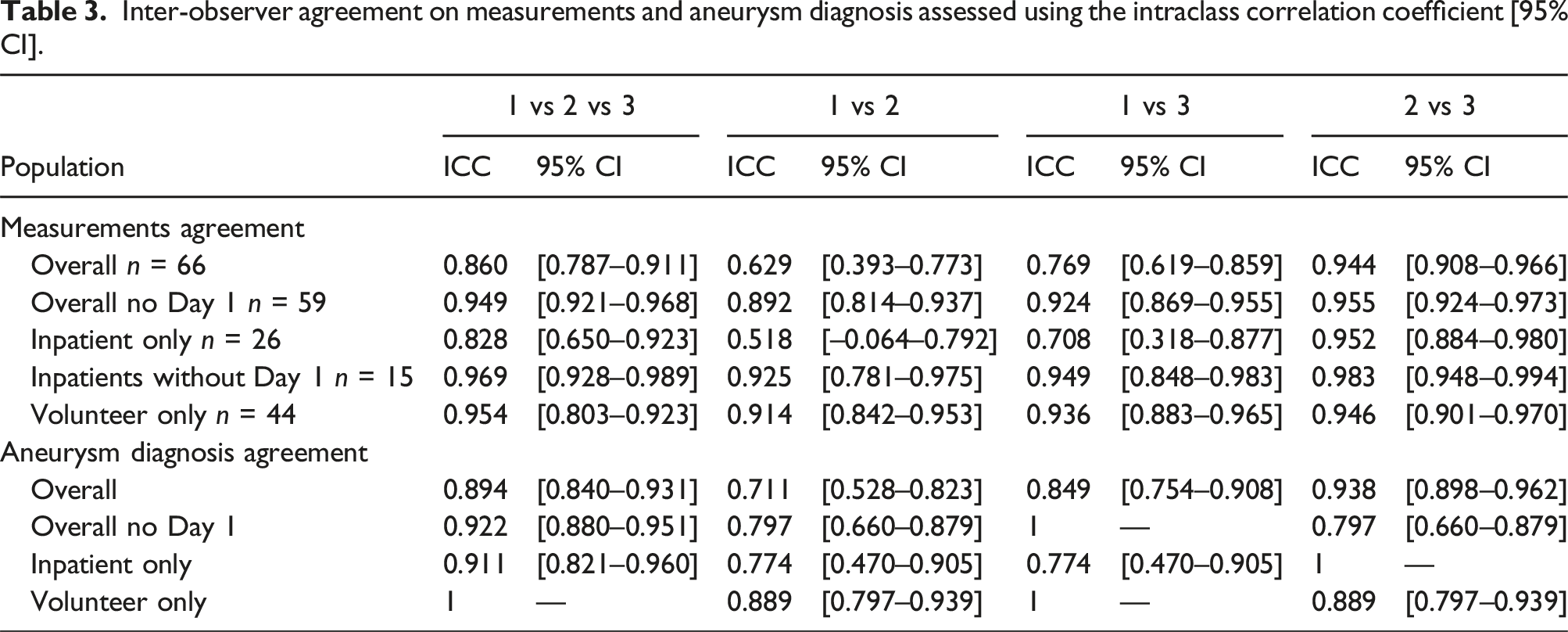
Intraclass correlation coefficients (ICCs) were calculated to gauge the degree of correlation and consistency between operators in measuring the aortic diameter and diagnosing AAA. 16 Furthermore, we explored the sensitivity, specificity, and predictive values for diagnosing AAA, comparing our ultrasound results against previously conducted investigations and the outcomes of radiology referrals. In addition, we employed one-way and two-way ANOVA to investigate any correlation between the differences in measurements, the volume of participants scanned by each operator, and the demographics of the recruiting population.
Results
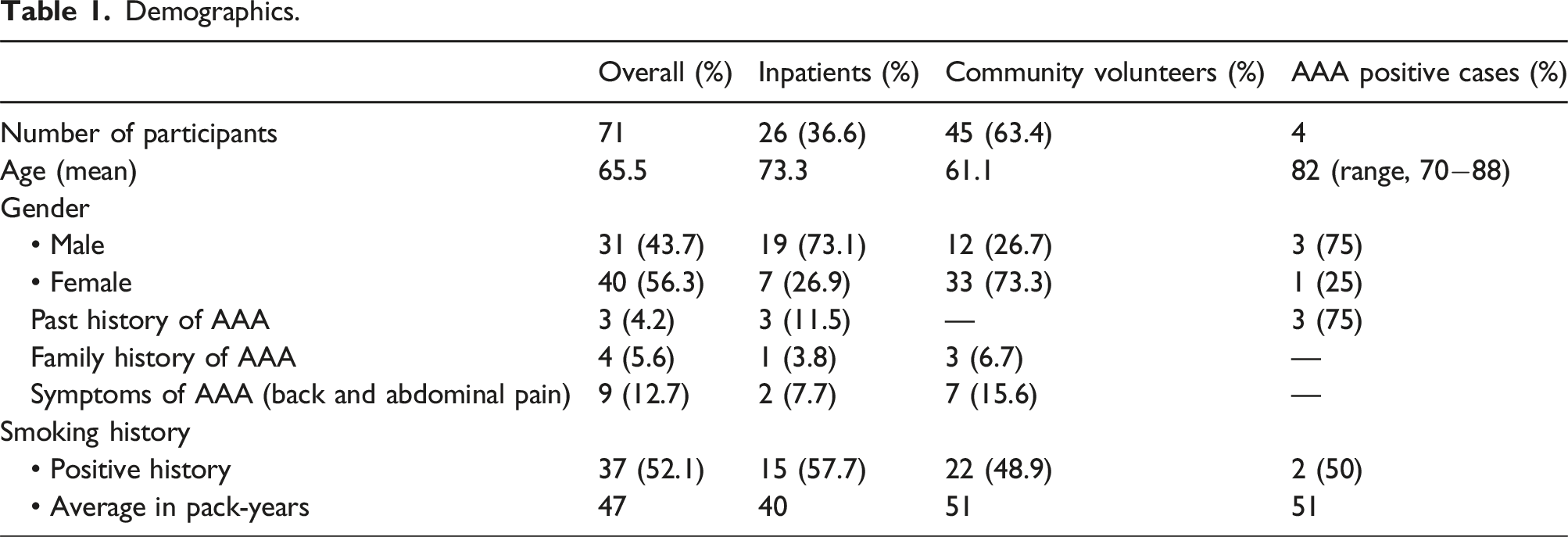
Demographics.
Reproducibility and measurement accuracy
The mean difference and variability between pairs of operators’ measurements of the infrarenal aorta in mm.
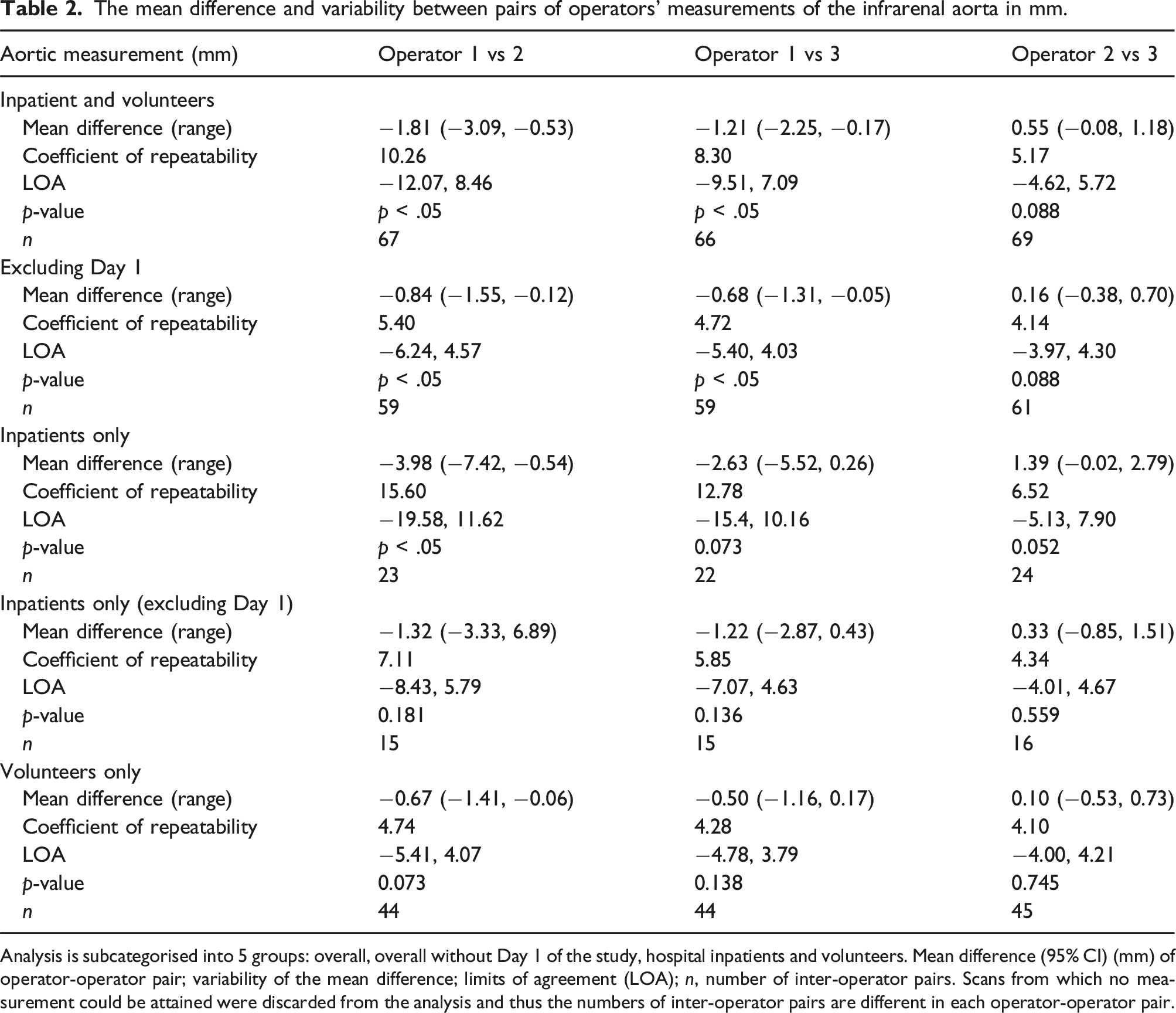
Analysis is subcategorised into 5 groups: overall, overall without Day 1 of the study, hospital inpatients and volunteers. Mean difference (95% CI) (mm) of operator-operator pair; variability of the mean difference; limits of agreement (LOA); n, number of inter-operator pairs. Scans from which no measurement could be attained were discarded from the analysis and thus the numbers of inter-operator pairs are different in each operator-operator pair.
The Bland−Altman plots further supported these findings, demonstrating no significant bias across the range of aortic sizes measured. Notably, Day 1 data indicated a learning curve, which was quickly surmounted, evidenced by the improvement in measurement consistency from the second day onwards; all of the measurements were within 10 mm discrepancy between operators. All three pairs achieved limits of agreement within CAD when measuring abdominal aorta diameter for volunteers (Figure 1). Bland−Altman plots. Bland−Altman plots for 3 operator-operator pairs including D1 versus excluding D1 (Figures A–F), and inpatients versus volunteers (Figures G–K). (A) Bland−Altman plot for Op 1 versus 2, including D1. (B) Bland−Altman plot for Op 1 versus 3, including D1. (C) Bland−Altman plot for Op 2 versus 3, including D1. (D) Bland−Altman plot for Op 1 versus 2, excluding D1. (E) Bland−Altman plot for Op 1 versus 3, excluding D1. (F) Bland−Altman plot for Op 2 versus 3, excluding D1. (G) Bland−Altman plot for Op 1 versus 2, inpatients only. (H) Bland−Altman plot for Op 1 versus 2, volunteers only. (I) Bland−Altman plot for Op 1 versus 3, inpatients only. (J) Bland−Altman plot for Op 1 versus 3, volunteers only. (K) Bland−Altman plot for Op 2 versus 3, inpatients only. (L) Bland−Altman plot for Op 2 versus 3, volunteers only.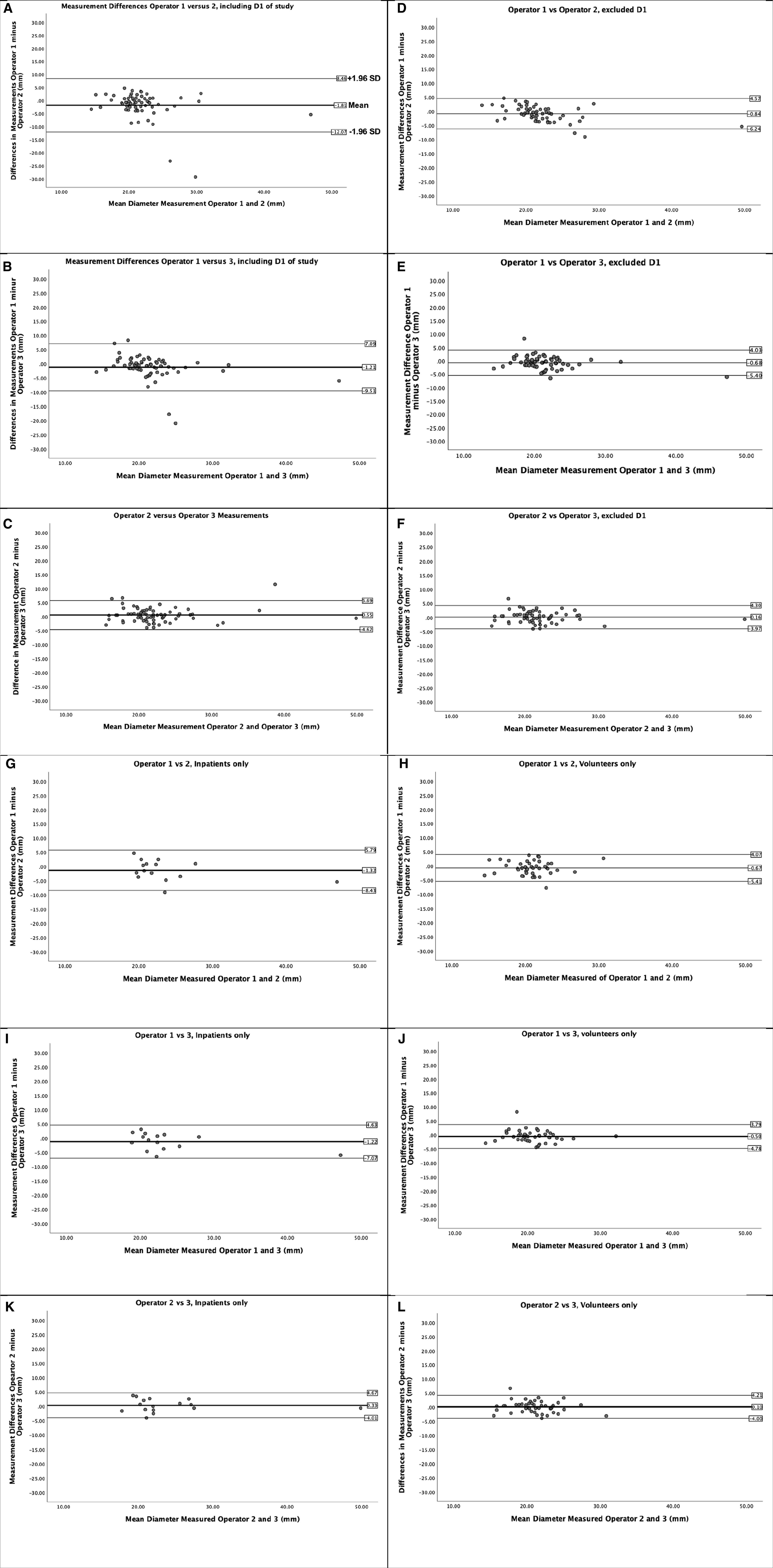
One-way ANOVA showed a substantial reduction in measurement differences between operators after scanning the first ten participants (p < 0.01), with a mean inter-observer variability within 5 mm and no statistically significant difference seen from the 11th participant onwards (Figure 2A). Two-way ANOVA negated the potential confounding effect by different participant populations on measurement differences (Figure 2B). . One-way (A) and two-way (B) ANOVA analysis between mean measurement differences and number of participants scanned by each operator and recruited populations.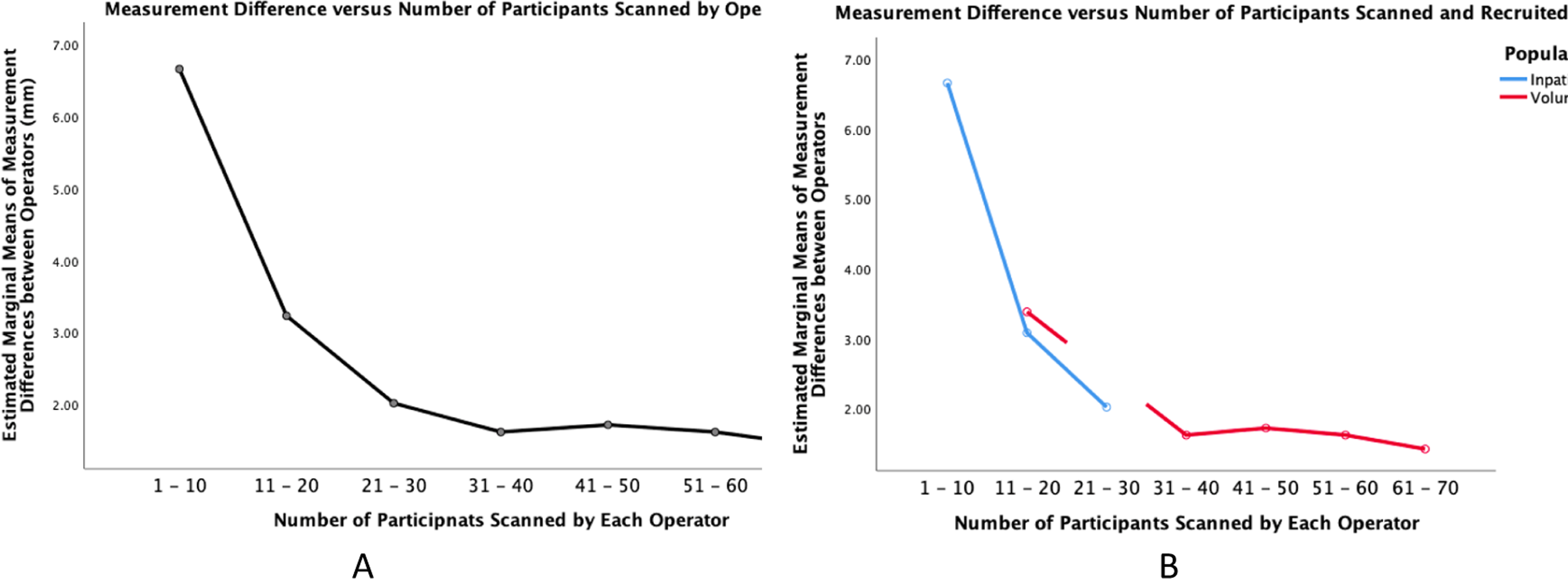
Aneurysm detection efficacy
Operators identified 5 (7.0%) infrarenal aneurysms, with 4 confirmed by formal radiology and 1 false positive due to overestimation of the aorta size. This represents a 20% false positive rate among detected cases but equates to approximately 1.4% when considering all 71 participants. Of the 5 cases, 4 (15.4%) were inpatients and 1 (2.2%) was a volunteer. The aneurysm sizes ranged from 3.11 to 4.80 cm. All confirmed cases were hospital inpatients, with a mean age of 82 years (range: 70–88 years), and positive smoking history, averaging 51 pack-years.
Inter-observer agreement on measurements and aneurysm diagnosis assessed using the intraclass correlation coefficient [95% CI].
Ultrasound scanning efficiency
In this study, visualisation of the aorta was unsuccessful in 6 (2.82%) cases, mainly due to time constraints or patient discomfort. The average scan duration was 4.7 min, with a slight increase for inpatients (5.4 min) compared to volunteers (4.3 min). Presence of bowel gas and increased body habitus were contributing factors. A significant improvement in scanning efficiency was observed over time, and a notable difference between inpatient and volunteer groups (p < 0.01). Although there was not statistically significant correlation between scan duration and number of participants scanned, operators were able to attain successful measurements in 100% of participants from the 31st patient onwards (Figure 3). Scanning efficiency in relation to number of participants scanned by each operator. Average time spent for each ultrasound examination +/− standard deviations, and percentages of cases with successful measurements for every ten patients scanned.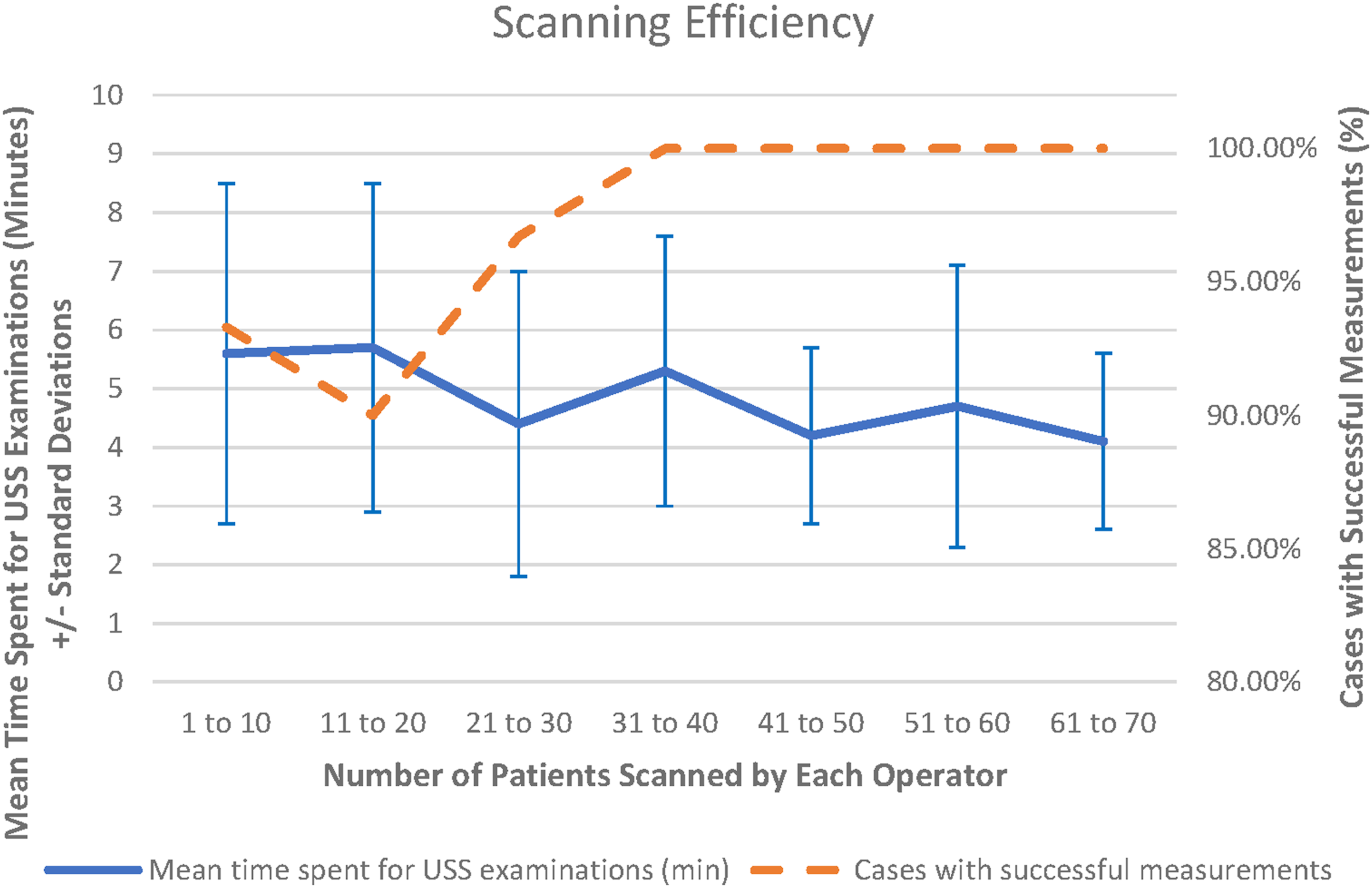
Discussion
Our study corroborates the pivotal role of ultrasound screening for Abdominal Aortic Aneurysms (AAA) in rural Australian settings, especially given limited access to speciality surgical resources and high mortality associated with ruptured aneurysms. Notably, despite having no prior sonographic training, the medical interns achieved a 97.2% visualisation rate of the abdominal aorta after a brief intensive course, demonstrating the feasibility of junior doctors performing AAA screenings in rural settings. We demonstrated that novice operators, after brief training, can accurately detect AAAs with high sensitivity and specificity, consistent with existing research on Point-of-Care Ultrasound (POCUS) in trained hands.10,11 The feasibility and effectiveness of this approach highlight the potential for expanding screening programs in resource-limited settings.
The impact of junior doctors performing these scans on their clinical duties was minimal. On average, each scan took 4.7 min, fitting seamlessly into existing workflows, showing that scaling such programmes in regional centres is feasible with proper scheduling. Larger-scale implementation would require thoughtful integration to avoid disrupting routine services.
While guidelines typically target males aged 65 and above for AAA screening, our inclusion of participants aged 50 and older was informed by rural demographic profiles, where high rates of smoking and cardiovascular disease heighten the risk of aneurysm progression. Early detection in such populations, even if outside conventional guidelines, potentially offers significant benefits. Future studies should explore the cost-effectiveness of broader screening in these rural communities.
Comparative analyses with other cancer screening programs reveal that AAA screening offers a favourable Incremental Cost-Effectiveness Ratio (ICER), suggesting that investment in such initiatives could yield significant public health benefits, especially in resource-constrained rural environments.17,18 Although cost-effectiveness analyses were not performed, targeted screening programmes could be justified in the context of the high mortality associated with ruptured AAAs in remote settings. Selective screening in high-risk rural populations could be invaluable where specialist vascular services are scarce and transport delays could be fatal.
The 5 mm threshold used aligns with the goals of a screening study. Screening aims to identify aneurysms requiring further assessment, rather than achieving precise measurement as expected in diagnostic contexts with professional sonographers. Given that the difference between a small aneurysm (≥3.0 cm) and a high-risk aneurysm (≥5.5 cm) is over 2 cm, a 5 mm variance remains clinically meaningful in screening settings. Despite using a 5 mm threshold, most operator measurements in our study fell within a 2 mm variance, underscoring the potential effectiveness of novice operators after minimal training.
Standardised training emerged as a critical determinant of screening accuracy and efficiency. Our observations suggest that a structured approach, encompassing both theoretical knowledge and practical skills, significantly enhances the reliability of measurements and the overall success rate of aneurysm visualisation. As evidenced by our dramatic improvement in inter-observer variability and interclass correlation coefficients after when study methodology was established on Day 1; operators avoided visiting inpatients around hospital meal-serving times, limited each study to within ten minutes, and informed the community volunteers to fast before the procedure. This is consistent with literature advocating for supervised practice to refine ultrasound techniques, highlighting the necessity of tailored training programs that address the specific requirements of AAA screening.
Expanding future screening efforts could involve nurses and general practitioners trained in POCUS. While requiring initial investment, such model could sustainably enhance access to preventive care in rural areas. Innovative approaches such as mobile screening units, telehealth-supported screening, and community outreach programmes could further enhance feasibility in geographically dispersed areas.
Reflecting on the limitations, our study acknowledges several factors that may affect the interpretation of our findings. Firstly, there is the potential for measurement inaccuracies and the risk of overlooking AAAs, particularly in the absence of a professional sonographer’s benchmark measurements. While we confirmed all positive findings through formal imaging by accredited sonographers, we did not systematically verify all negative scans due to resource constraints in the rural setting. This lack of external validation introduces the potential for false negatives, which could affect our conclusions regarding the screening’s efficacy. Future studies should include verification by accredited sonographers of both positive and negative scans to enhance accuracy and reliability.
Secondly, although the junior doctors were unaware of participants’ prior aneurysm status, the inclusion of patients with known aneurysms may influence the study’s outcomes and the perceived effectiveness of the screening programme. In our study, three out of the four confirmed aneurysm cases were previously diagnosed and under surveillance. While this demonstrates the ability of junior doctors to accurately detect AAAs, it raises questions about the additional value of the screening programme in identifying new aneurysm cases. However, the primary aim of our study was to evaluate whether junior doctors without prior sonographic experience could reliably perform AAA screenings after brief training. In resource-limited rural areas, empowering junior doctors to perform screenings could lead to earlier detection of AAAs in patients who might otherwise remain undiagnosed until presenting with life-threatening ruptures. Future research should consider stratifying data between known and new cases to provide a clearer assessment of the screening’s impact on new aneurysm detection rates.
Furthermore, our screening focused on infrarenal AAAs, and future initiatives should expand to include juxtarenal, suprarenal, and iliac aneurysms. Incorporating these aspects into a more comprehensive screening protocol requires careful consideration of cost, training, and time, particularly in resource-limited rural settings. These factors underscore the need for further research into the cost-effectiveness and scalability of AAA screening programmes in rural contexts.
Conclusion
This study marks the first investigation in AAA screening in rural Australia, utilising junior doctors as novice screeners. Our findings advocate for the integration of AAA ultrasound screening within rural healthcare frameworks, highlighting the critical role of novice operators in enhancing early detection efforts. This strategy not only aligns with the imperative for cost-effective healthcare solutions in underserved areas but also capitalises on the available workforce to mitigate the challenges posed by geographic and resource constraints. Future research should aim to incorporate rigorous quality control measures, such as systematic verification by accredited sonographers, to validate both positive and negative findings, refine training methodologies, explore the scalability of screening programs, and evaluate the long-term impacts on patient outcomes and healthcare systems in rural contexts.
Footnotes
Authors’ contributions
Mei Ping Melody Koo − conceptualisation, data curation, investigation, methodology, project administration, resources, validation, visualisation, writing − original draft, and writing − review and editing drafts. Hansraj Riteesh Bookun – conceptualisation, data curation, formal analysis, methodology, supervision, and writing − review and editing drafts. All authors have participated to drafting the manuscript, and all authors read and approved the final version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.