
Abstract
Background
Endovascular procedures requiring large bore access, such as Transcatheter Aortic Valve Replacement (TAVR), Thoracic Endovascular Aortic Repair (TEVAR), and Endovascular Aneurysm Repair (EVAR), have become increasingly common. Despite advancements, complications from these procedures pose clinical challenges, especially in elderly and frail patients. The clinical objective of this paper is to demonstrate the complexities and innovative management strategies for complications that arise from large bore access.
Case Report
This report presents two cases illustrating percutaneous management of complications arising from large bore access during endovascular interventions. The first case involves a 74-year-old Asian female with a history of type A aortic dissection, who underwent TEVAR using a Gore TBE endograft. Post-procedure, the patient developed hemorrhagic shock due to disruption of the right external iliac artery. Interventions included upsizing the left femoral artery sheath, CODA balloon inflation in the distal aorta, and deployment of multiple VBX stents. The second case features a 24-year-old Caucasian female with a large pseudoaneurysm at the cannulation site in the aortic arch following a heart transplant. Successful TEVAR was performed to exclude the pseudoaneurysm. Closure of the right femoral artery access using 6 French ProGlide sutures was complicated, requiring balloon angioplasty to create an opening in the common femoral artery.
Conclusions
These cases highlight the challenges and innovative strategies in managing complications associated with large bore access during endovascular procedures. Insights gained from these experiences contribute to the armamentarium of interventionists, offering valuable guidance in addressing similar scenarios.
Introduction
Over the past few years, there has been a massive increase in endovascular procedures requiring large bore access. 1 Currently, elective Transcatheter Aortic Valve Replacement (TAVR), Thoracic Endovascular Aortic Repair (TEVAR), and Endovascular Aneurysm Repair (EVAR) procedures are being performed utilizing large bore access.2,3 Complications from large bore access remain a clinical problem, particularly in elderly and frail patients who poorly tolerate such complications. 4
Studies have shown that the frequency of vascular complications and bleeding can be up to 20% in TAVR and 12%–22% in EVAR.1,5 These complications are associated with longer hospital stay and significant increase in short- and long-term risk of mortality. 6 Common risk factors for large bore access complications include female gender, obesity, past history of renal failure, and anti-coagulant use.7,8
Complications related to large bore access during endovascular procedures are well known. However, there are few case reports that provide detailed percutaneous management strategies for such complications. Our study addresses this gap in the literature and offers critical insights into the effectiveness of various interventions in addressing complications associated with large bore access.
Case presentation
The first case is that of a 74-year-old Asian female patient who had undergone open repair for a type A aortic dissection. She now presents with progressive aneurysmal degeneration of the descending thoracic aorta, which was favorable for TEVAR in zone 2 of the aorta using a Gore TBE 40 × 40 × 150 cm endograft (Figure 1(a)). A branch endoprosthesis for the left subclavian artery was performed using a 12 × 15 × 61 mm endograft and VBX 11-mm stents (Figure 1(b)). Coverage of zones four and five of the descending thoracic aorta was completed using Terumo 44 × 40 × 209 mm and 40 × 40 × 150 mm endografts. (a) Aneurysmal dilation of the descending thoracic aorta measuring 6.0 cm; (b) Gore endoprosthesis for Lt. Subclavian 12 × 15 × 61 mm and VBX 11 mm stents.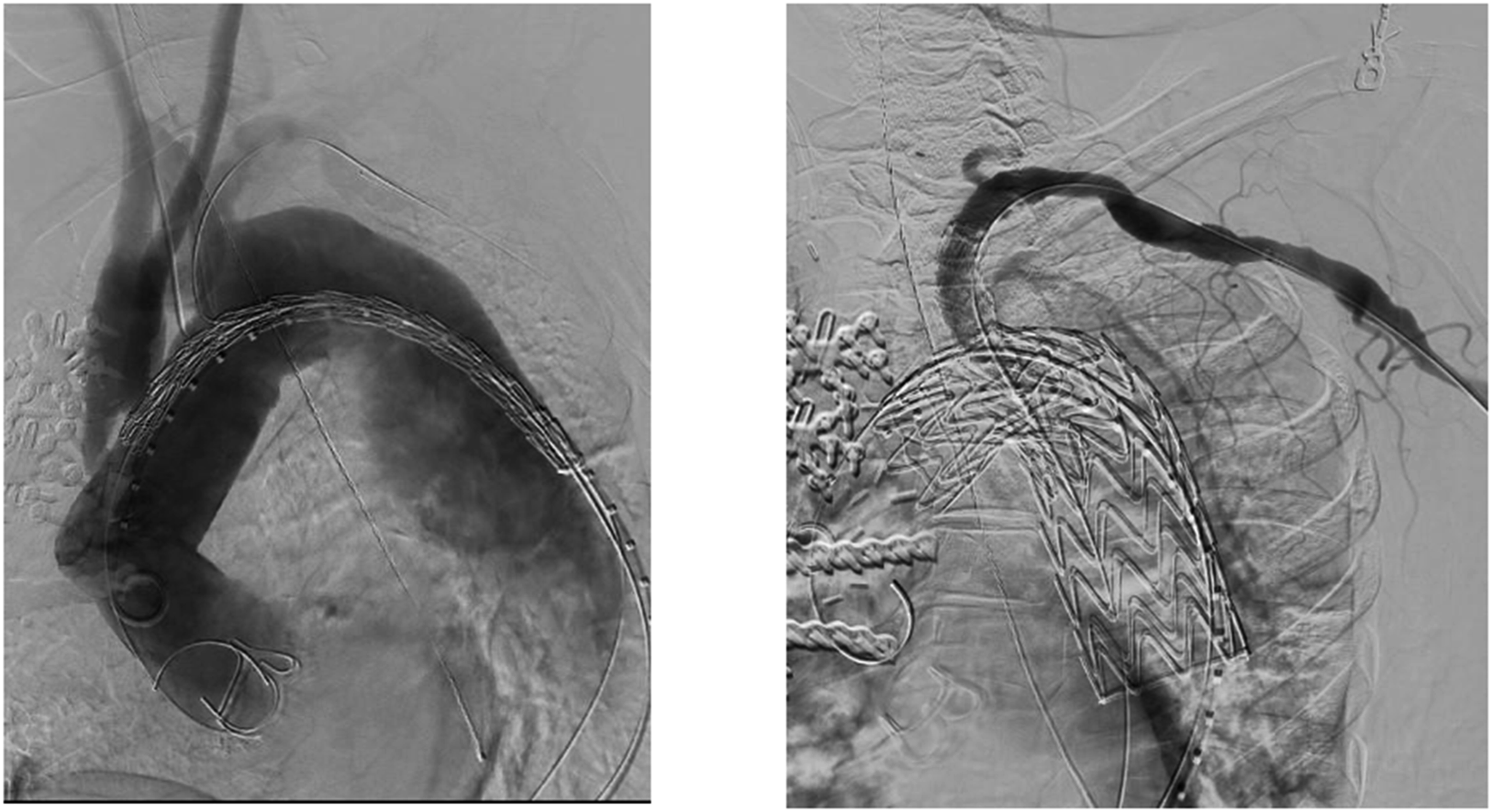
Following the removal of the 26 French dry seal sheaths from the right common femoral artery, the patient went into shock. Cardiopulmonary resuscitation was started. An angiogram performed from the left femoral artery access demonstrated disruption of the right external iliac artery with massive hemorrhage. The 6 French sheath in the left common femoral artery was upsized to an 11 French sheath, and a CODA balloon was inflated in the distal aorta as resuscitation of the patient continued.
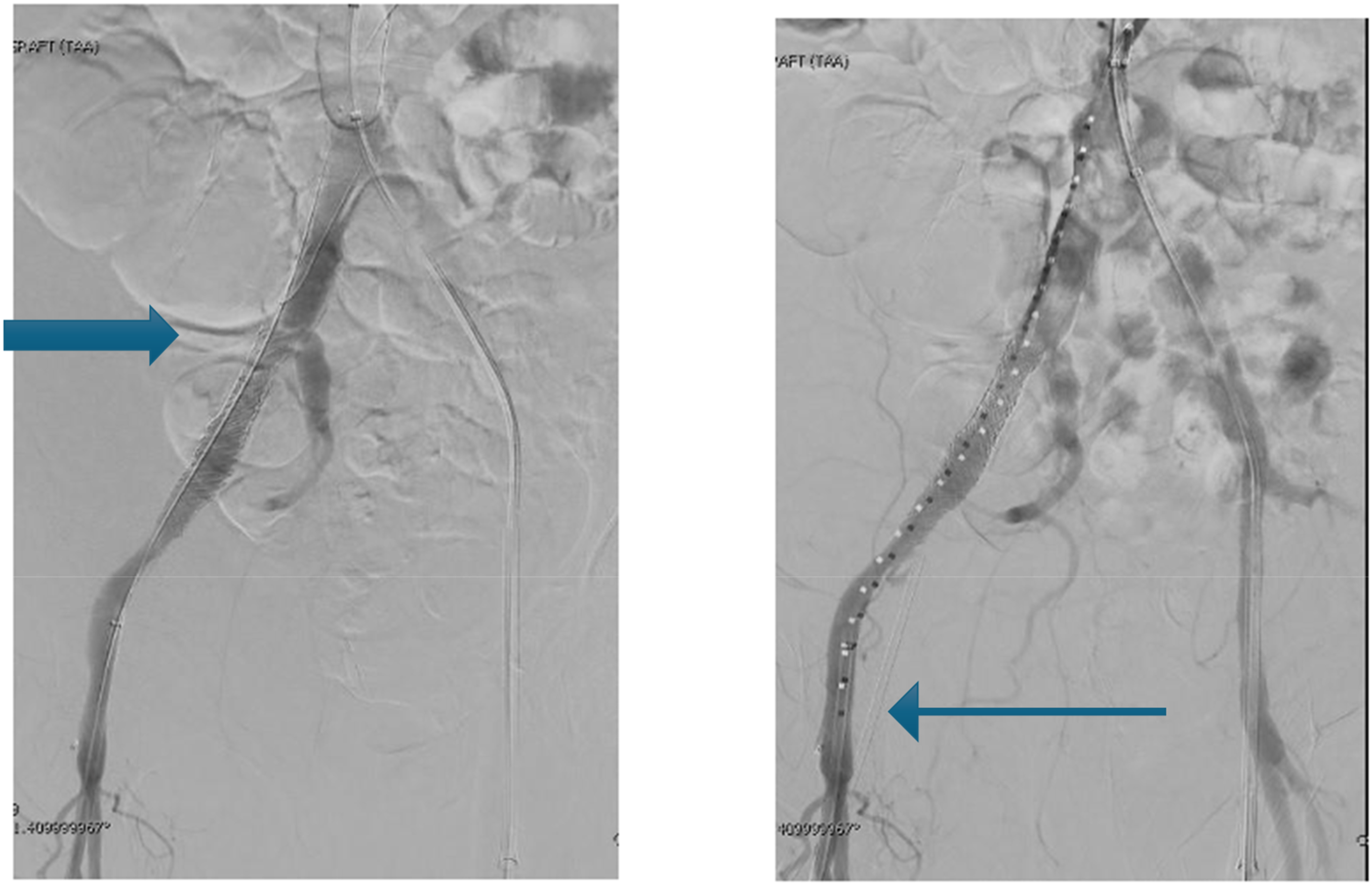
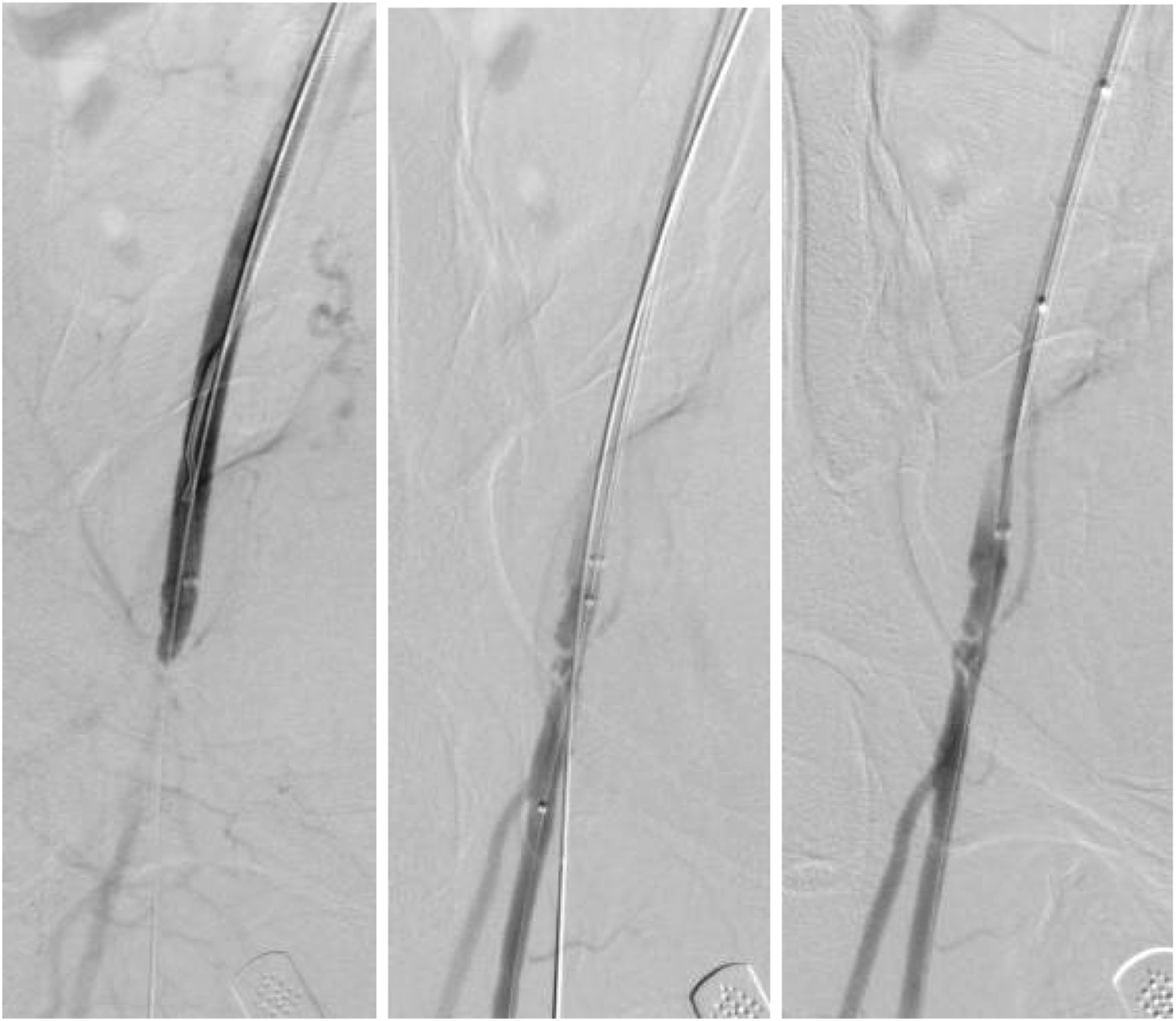
The proximal right superficial femoral artery was accessed under ultrasound guidance, and a short 8 French sheath was placed. Through this sheath, a VBX stent 10 × 59 mm was deployed in the external iliac artery (Figure 2(a)). Three additional VBX stents, 10 × 59 mm, 10 × 39 mm, and 8 × 59 mm, were required to complete the repair of the disrupted EIA (Figure 2(b)). The patient was now hemodynamically stable and transferred to the cardiovascular intensive care unit. Later that evening, the patient was hypotensive again and returned to the interventional radiology suite for additional imaging. Ongoing bleeding between the previously deployed VBX stents (type III endoleak) was noted (Figure 3), requiring additional placement of a VBX 10 × 39 mm stent in the distal EIA extending into the proximal common femoral artery (Figure 3(b)). With this, the patient remained hemodynamically stable, and the remainder of her hospital course was free of additional complications. She remains well 1 year from the time of this intervention. (a) VBX stent 10 × 59 mm deployed in the right EIA; (b) three VBX stents—10 mm × 59 mm, 10 mm × 39 mm, and 8 × 59 mm. (a) Type III endoleak between previously placed VBX stents as shown by arrow. (b) Placement of VBX stent 10 mm × 39 mm in the distal EIA extending into the proximal CFA as shown by arrow.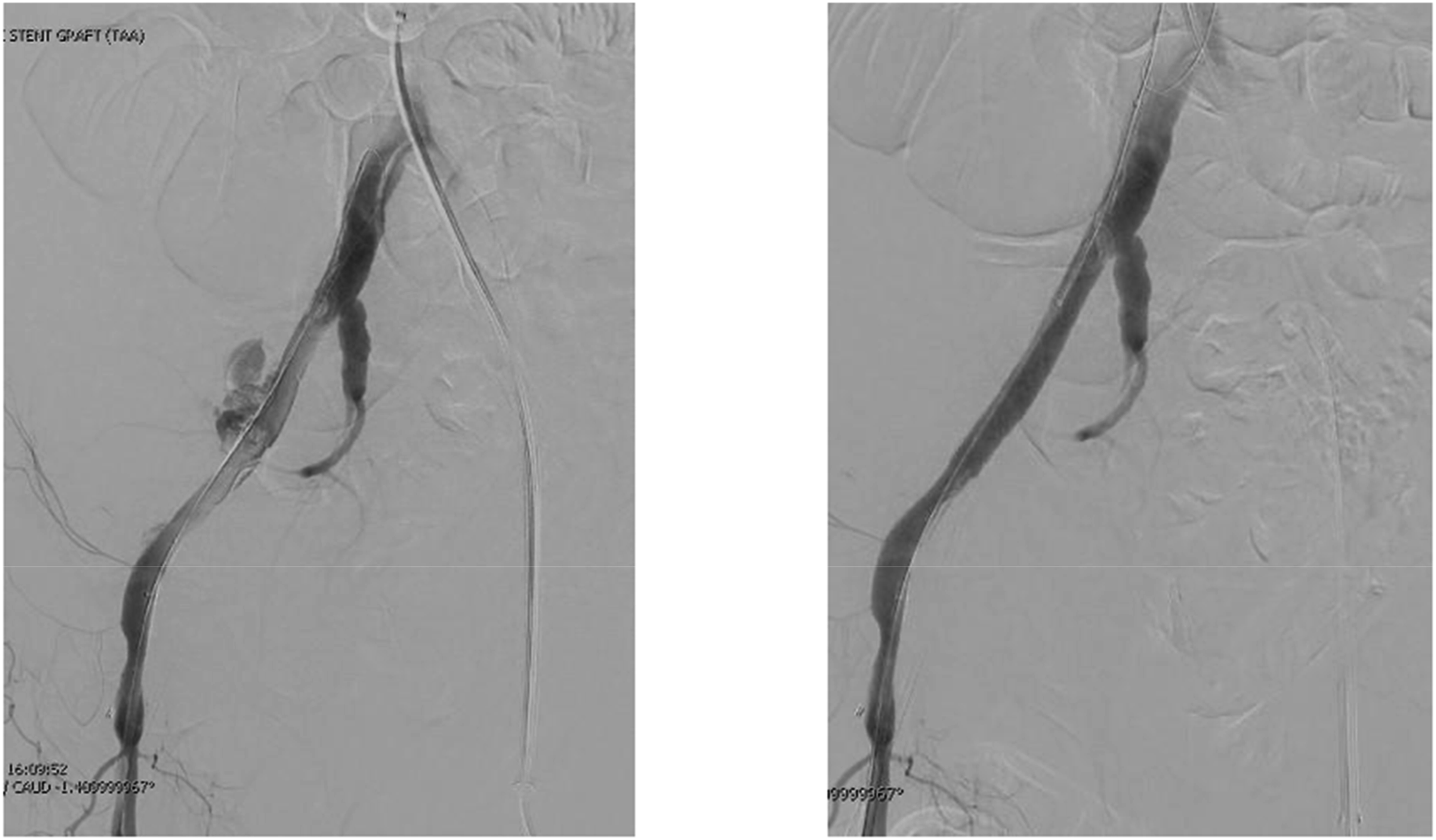
The second case is that of a 24-year-old Caucasian female who was noted to have a large pseudoaneurysm at the cannulation site in the arch of the aorta from the time she underwent a heart transplant for cardiomyopathy (Figure 4(a)). She underwent successful TEVAR for exclusion of the pseudoaneurysm (Figure 4(b)). Closure of the right femoral artery access using 6 French ProGlide sutures resulted in complete closure of the access vessel (Figure 5). Importantly, wire access was retained throughout the procedure, which allowed prompt recognition and correction once the CFA was identified as occluded. The dilator of the 6 French sheath was advanced over the wire to create an opening in the common femoral artery. This allowed a 0.018″ wire to be advanced from above using the up-and-over approach from the left common femoral artery access. The opening in the right common femoral artery was then treated with a 4 mm angioplasty balloon followed by a 6 mm angioplasty balloon. Ultrasound imaging of the right proximal superficial femoral artery demonstrated normal triphasic flow with a normal velocity profile. (a) Pseudoaneurysm at cannulation site of the aortic arch; (b) TEVAR performed to exclude the pseudoaneurysm. Closure of the right femoral artery with 6 French ProGlide sutures.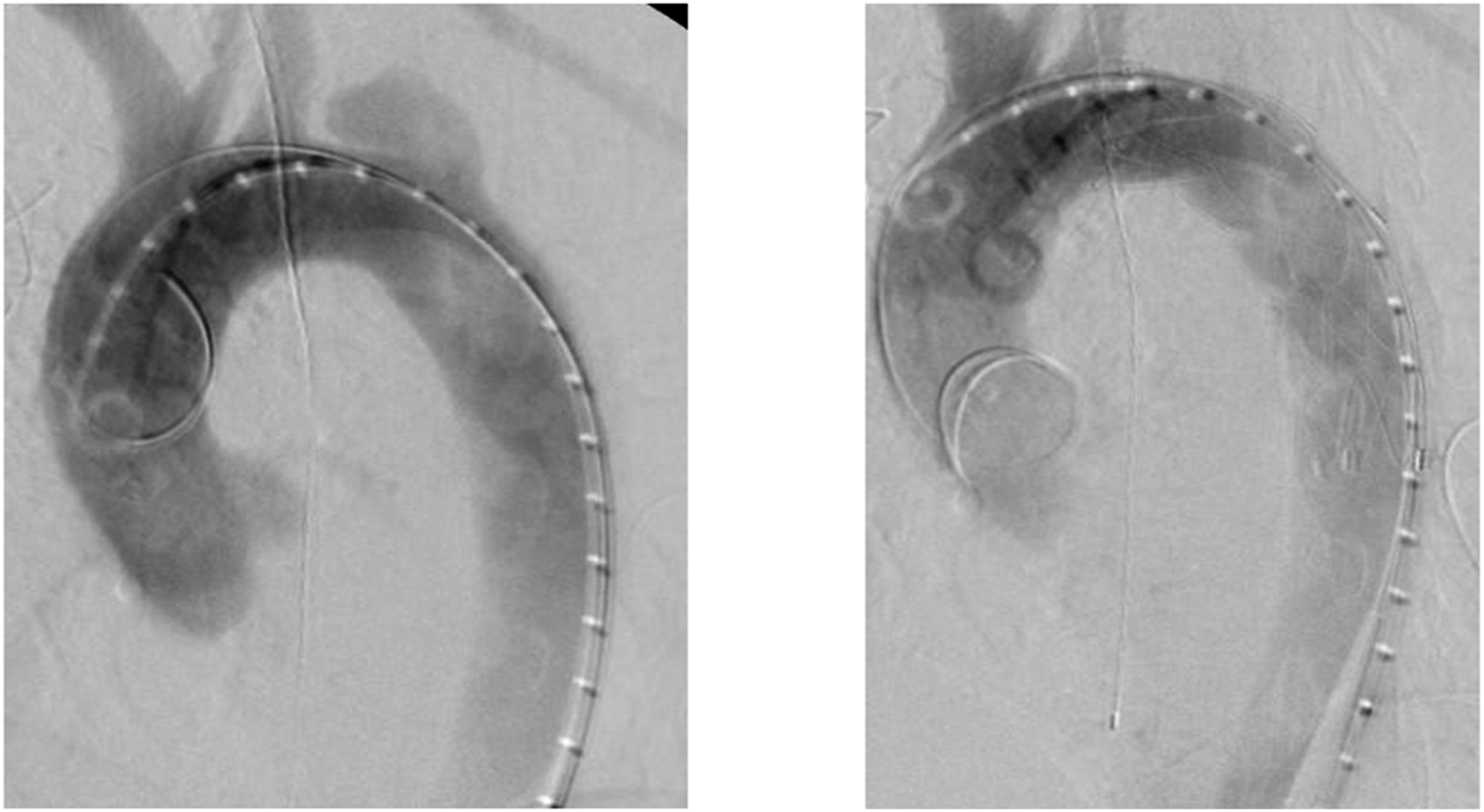
While a flexible Viabahn stent could be considered in this scenario, caution must be exercised regarding its use in the CFA. The deployment of Viabahn stents in this region is off-label (off-IFU) and carries limitations due to the high mobility and flexion in this vascular segment, which may predispose the stent to failure. In this case, open repair was not an option due to patient factors, which further necessitated endovascular management.
The patient had the return of normal peripheral pulses, and a follow-up CT angiogram demonstrated patency of the common femoral artery and run-off vessels below the access vessel. She has remained well over a year since this intervention without any claudication symptoms.
Discussion
Percutaneous EVAR, TEVAR, and TAVR have become common endovascular procedures. However, they are often associated with large bore access complications which can lead to adverse postoperative events and a higher mortality. 9
Outside of our study, Parker et al suggested new vascular access methods to improve the effectiveness of TAVR procedures, resulting in fewer open repairs and better outcomes for patients. The presented techniques involved gaining access to the mid common femoral artery just slightly above the profunda femoris and then performing angiography post-the TAVR, to identify and remediate the issues with stent deployment. In TAVR performed between January 1, 2016, and June 30, 2018, at a tertiary care facility, 4.4% of 699 TAVR required access-related interventions. The major forms of intervention were represented by covered stents at 58.1%, open repairs at 35.5%, and thrombin injections at 6.5%. Most of the interventions were successful, but there were some complications and even one in-hospital mortality. 10
Our institution has described our experience with recommendations of percutaneous access and repair of access-related complications. We follow the same protocol for procedures requiring all large bore access. The complications described above were detected by angiography from the contralateral side. Both complications were in female patients with small access vessels, however deemed adequate to accommodate the devices required for repair.
In the first-case, the type III endoleak noted between over lapping VBX stents may have been averted by using Viabahn stent instead as demonstrated in Figure 6). The outpouching of the Viabahn stent conforms to the defect in the wall of the artery.
11
Avulsion of the external iliac artery is known to occur in cases of “iliac on a stick” results in absence of an arterial wall for a balloon expandable stent (VBX) to buttress against. The self-expanding covered stent graft (Viabahn) reconstructs the vessel in the absence of a scaffold
12
(Figure 6). Previous studies have already demonstrated the effectiveness of Viabahn stent involving management of subclavian artery aneurysm (SAA) and type I endoleak. Despite successful exclusion of the SAA, a slight endoleak persisted at 6 months, along with stent graft dislodgement. A subsequent intervention with a 10 × 50-mm Gore Viabahn stent graft, utilizing the pull-through technique, resolved the type Ia endoleak.
13
For such reasons, we believe Viabahn stent can be effective in the management of our case, involving the type III endoleak. Successful deployment of Viabahn 10/50-mm and profound femoris not compromised. Note the out pouching of the Viabahn stent where the native vessel wall is absent or disrupted (blue arrows).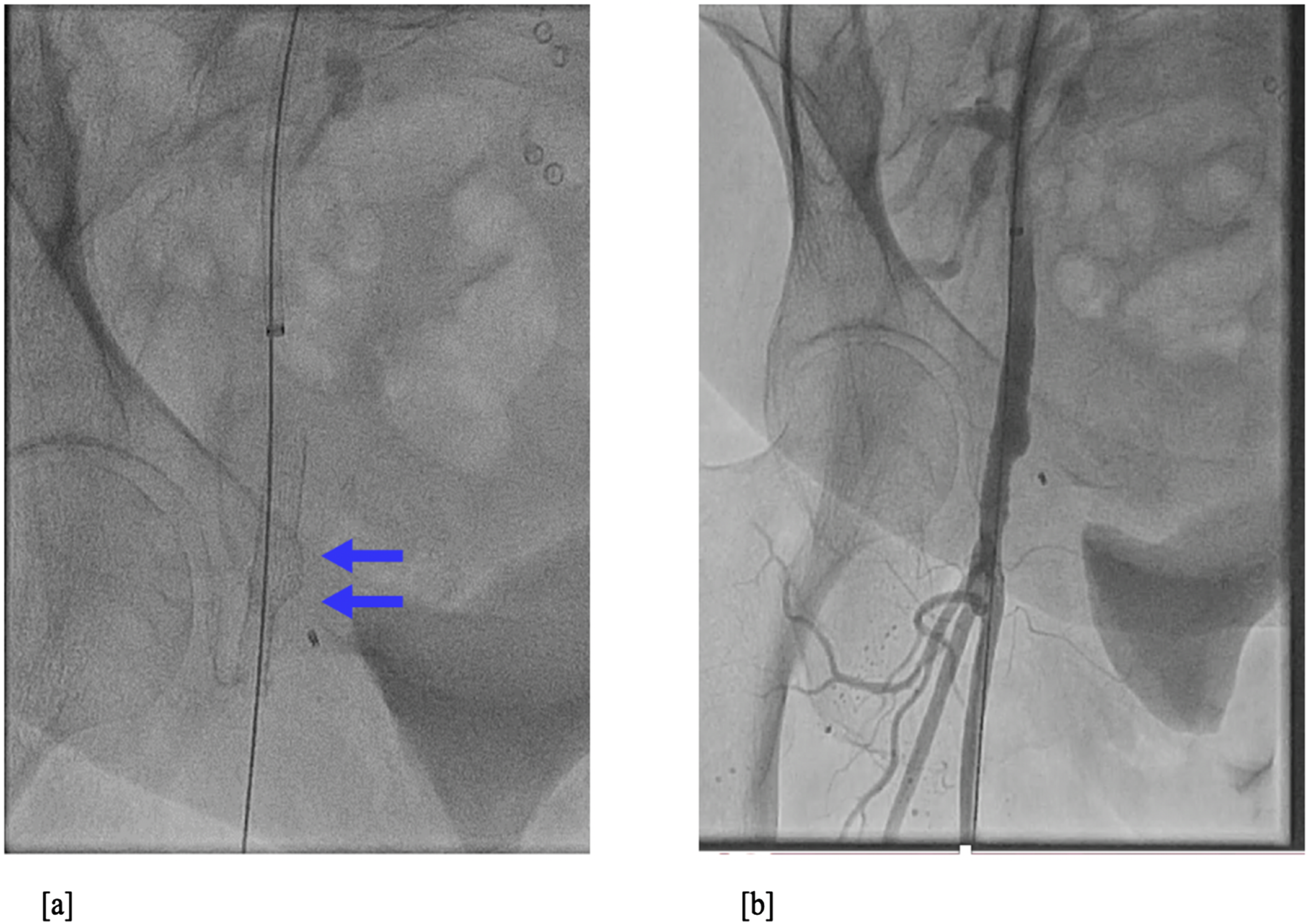
It is important to note that the VBX stent was selected due to its balloon-expandable nature, which provides precise deployment and better control in the confined anatomy of the distal EIA. While a Viabahn stent may have mitigated the type III endoleak, the VBX was chosen to prioritize immediate hemodynamic stabilization and procedural efficiency. This highlights the need to tailor stent selection to the clinical and anatomical context.
The second case is an example of closure device (two 6 French ProGlide) failure, angiography from contralateral side allowed prompt recognition of the complication. Retaining the wire on the side of closure until the very end provided an avenue for correction of the problem. Once a channel had been created, progressive dilation resulted in unobstructed flow lumen of the common femoral artery. Increasingly, vascular procedures are being performed by the endovascular route. Access-related complications will be inevitable as a result. Management of the complications with minimal morbidity and mortality must be our common goal.
Despite the effectiveness of the interventions we propose, there are limitations in our case report. For example, the retrospective nature and small sample size of our case report may limit the generalizability of our findings. To overcome these limitations, upcoming research should focus on multicenter studies with larger sample sizes. In addition, our cases demonstrate management of large bore access issues, but it also highlights the importance of having standardized protocols and guidelines in this area. Therefore, it is crucial for studies to establish consensus guidelines for preventing, diagnosing, and managing large bore access complications across diverse patient groups and procedural settings. Additionally with advancements in interventions, it becomes important to explore the long-term outcomes and effectiveness of repair strategies for large bore access problems. This may involve evaluating recurrence rates need for intervention and overall patient outcomes, over follow-up periods.
Conclusion
In summary, our case report highlights effective treatment options for endovascular complications arising from large bore access. While our cases exhibit favorable outcomes, further research is necessary to overcome limitations, such as small sample size and retrospective design, and to advance our understanding of optimal management strategies.
Footnotes
Acknowledgment
We thank the patient for providing their informed consent.
Author contributions
DM: Concepts, design, definition of intellectual content, literature search, data acquisition, data analysis, manuscript preparation, manuscript editing, and manuscript review; BA: Definition of intellectual content, literature search, data acquisition, data analysis, manuscript preparation, manuscript editing, and manuscript review; ML: Definition of intellectual content, literature search, data acquisition, data analysis, manuscript preparation, manuscript editing, and manuscript review; NB: Data acquisition, data analysis, manuscript editing, and manuscript review.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Institutional review board statement
The need for the approval of an ethics committee was waived since this is a consented individual case report in which the privacy of the infant is guaranteed. Informed Consent Statement: The authors certify and confirm that they have obtained patient information based on an informed consent. Patient has given their respective consent for their images and other clinical information to be reported in the journal. The patient has been informed that their names and initials will not be published, and due efforts will be made to conceal their identity.