
Abstract
Background
It is still challenging to perform high-risk cases, such as acute type A dissection, which frequently require blood transfusions. We created perioperative bloodless protocol, but it includes an optimization to increase the preoperative hemoglobin level enough to tolerate cardiopulmonary bypass. However, it would be impossible to optimize such patients using the strategy in the setting of emergent surgery. We sought to create a surgical strategy in an effort to reduce blood loss for acute type A dissection patients refusing blood transfusion.
Methods
We reviewed the records of two patients in our aortic surgery database who presented with acute aortic dissection and refused blood transfusion. These patients underwent two-staged aortic repair with ascending aortic replacement with debranching to the innominate and left common carotid arteries, followed by thoracic endovascular aortic repair (TEVAR).
Results
Conclusion
Two-staged aortic repair in patients refusing blood transfusion can avoid circulatory arrest requiring deep hypothermia so as to reduce the risk of coagulopathy and blood loss.
Introduction
While a number of institutions offer cardiac surgery for patients refusing blood transfusion, there is a tendency to limit surgery only for simple cardiac cases.1–3 In our institution, we have aggressively performed cardiac surgery for this patient population including complex cases and have developed a perioperative bloodless protocol. 4 However, it is still challenging to perform high-risk cases, such as acute type A dissection, which frequently require blood transfusions. The perioperative bloodless protocol includes an optimization to increase the preoperative hemoglobin level enough to tolerate cardiopulmonary bypass. However, it would be impossible to optimize such patients using the strategy in the setting of emergent surgery. We sought to create a surgical strategy in an effort to reduce blood loss for acute type A dissection patients refusing blood transfusion. We presented two consecutive acute type A dissection patients undergoing a two-staged aortic repair strategy including ascending aortic replacement with debranching to the innominate and left common carotid arteries, and subsequent thoracic endovascular aortic repair (TEVAR).
Methods
This study was approved by the Institutional Review Board (IRB) of the University of Chicago Medicine (IRB14-0576). We interrogated our cardiac surgery database to retrospectively review patients undergoing two-staged aortic repair who refused blood transfusion from November 2019 to October 2021 at our institution. We offered surgery for all comers who had an acute type A dissection and survived enough to reach our hospital. In those cases, we performed two-staged aortic repair with open surgery and endovascular aortic repair for two consecutive cases who refused any blood transfusions.
Results
First-stage open aortic surgery
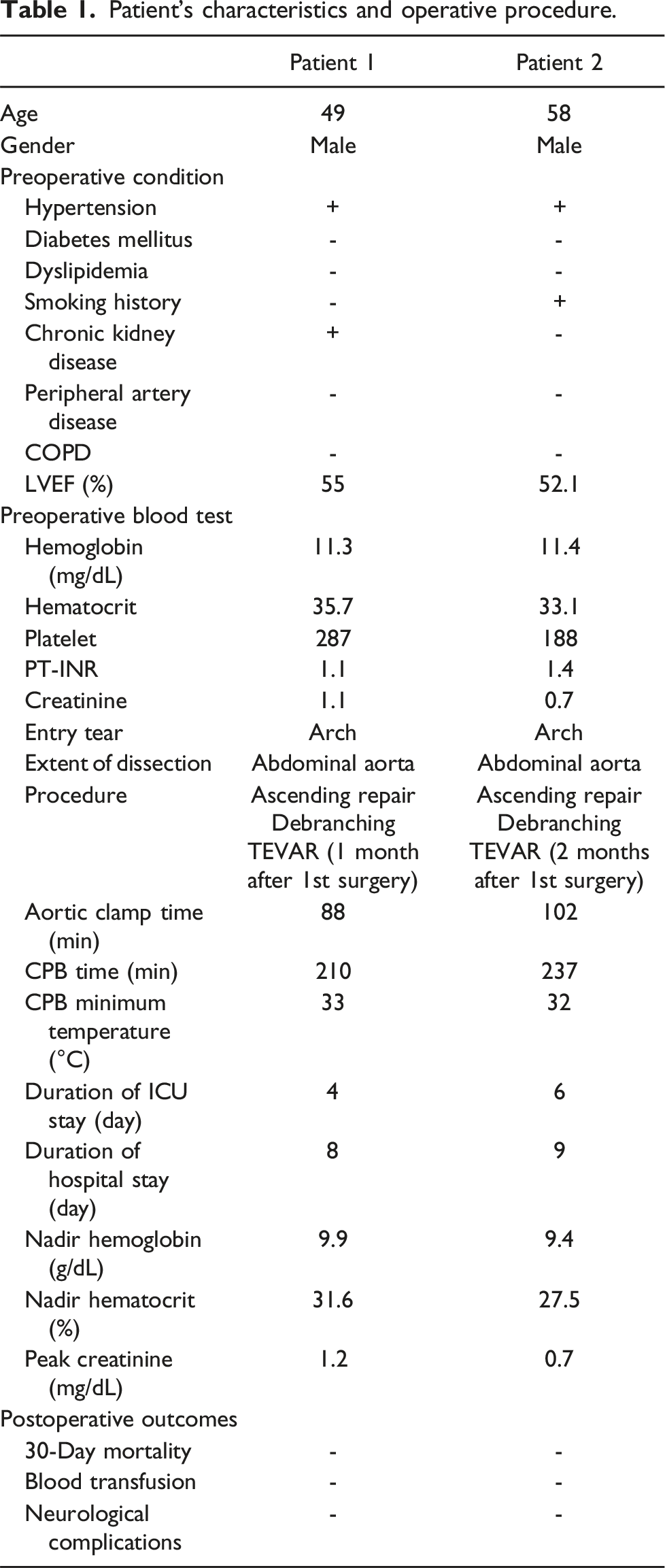
Patient’s characteristics and operative procedure.
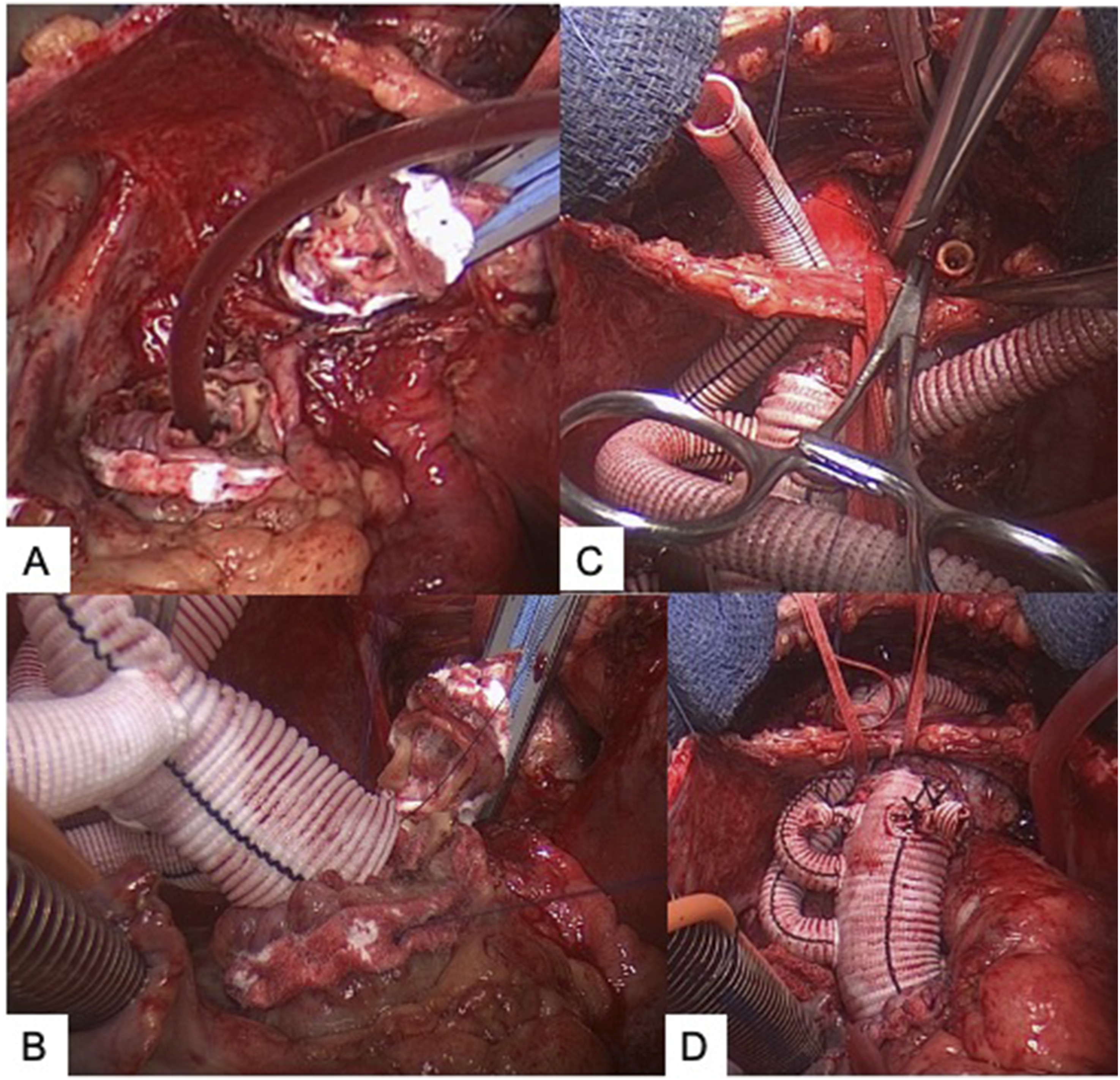
A: Proximal and distal ascending aorta were trimmed and reinforced with the Teflon sandwich. B: Four-branch artificial graft was anastomosed on both sides. C: Anastomosis for common carotid artery. D: Two branches were anastomosed.
Second stage endovascular aortic repair
After a few months from the discharge (mean index hospital stay 9 days), the patients were readmitted for 2nd stage TEVAR with a bypass between the left carotid artery and the left subclavian artery with a 8 mm Dacron graft. A stent (Valiant Captivia, Medtronic, 34 × 200 mm and 34 × 150 mm for patient 1) (CTAG 37 × 150 mm, W.L. Gore for patient 2, who has a history of a stent placement for descending aorta) was placed from the distal portion of the surgical graft to the distal descending aorta that allowed coverage of the dissected aorta as long as possible with arterial access via bilateral femoral arteries in a percutaneous manner (Figure 2(C) and (D)). A: Preoperative CT scan with contrast. B: Postoperative 3D CT scan (ascending replacement and debranching). C: Aortic angiography before stent graft placement. D: Aortic angiography after stent graft placement. E: Postoperative 3D CT scan (after TEVAR) footnotes.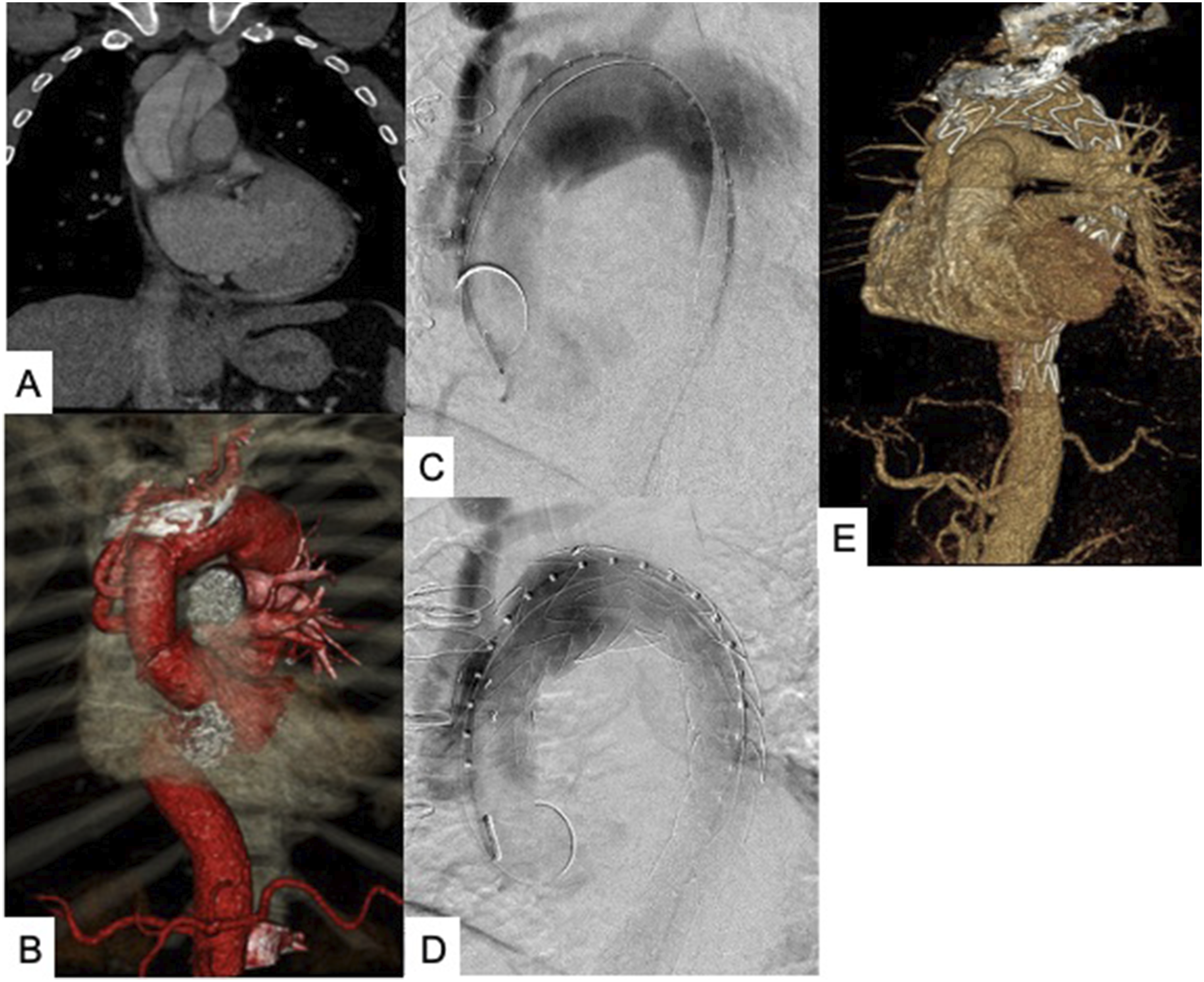
The two-staged procedure was successfully completed in two patients without any significant complication. The patients’ data is summarized in Figure 1. The postoperative course was uneventful for both patients. Figure 2 shows the pre- and postoperative CT scans and aortic angiography.
Discussion
In general, most institutions would not offer surgery for acute type A dissection patients that refuse blood transfusions due to the nature of the disease and complex surgery which frequently requires blood transfusion. The principle of surgery for type A dissection is to close the initial entry tear and replace the aorta as needed like either hemi-arch or total arch replacement. Therefore, it would not be possible to achieve the principle without using the circulatory arrest technique. However, it is well known that circulatory arrest with deep hypothermia could cause severe coagulopathy. The two-staged technique included the following: 1. Ascending aortic replacement and debranching for the innominate and left carotid artery and 2. TEVAR at zone 0 to cover the entire aortic arch and the proximal descending aorta. The technique allows us to avoid a circulatory arrest with deep hypothermia and to get rid of or cover the initial entry.
Regarding hypothermia-induced coagulopathy, Ise et al. reported that the incidence of perioperative bleeding and the requirement of intraoperative transfusion were significantly higher in patients undergoing hypothermic circulatory arrest (HCA) than non-HCA even though cardiopulmonary bypass times were not significantly different. Rotational thromboelastometry (ROTEM), which allows to analyze the details of coagulopathy, showed that clot firmness was significantly reduced in patients with HCA, consistent with platelet dysfunction. 5 Ming et al. reported that deep hypothermia resulted in significant reduction of coagulation factors such as FXI and FVII, compared to mild hypothermia. 6 It would be important to avoid the circulatory arrest technique for successful bloodless surgery in acute type A dissection patients.
Isolated ascending aorta replacement might be one of surgical options for a salvage purpose. However, in case that the entry tear is located in the aortic arch, it would not be able to achieve the primary entry resection and result in a premature treatment.
The 2nd stage TEVAR procedure provides several benefits. Since it covers the entire aortic arch to descending thoracic aorta (zones 0-4), the two-staged strategy can treat the proximal entry regardless of its location. Also, the concept allows an “easy” distal anastomosis at zone 0 during the 1st stage surgery. When performing a total arch replacement in acute type A dissection patients in general, the frozen elephant technique has been reported to provide a good mid- to long-term remodeling of descending aorta. While the frozen elephant technique cannot be applied without a circulatory arrest, the 2nd stage TEVAR could provide the same mid- and long-term benefit. Also it would reduce the risk of requiring surgical reintervention in the future, which is particularly important in patients refusing blood products. We performed the 2nd stage TEVAR at 1 month for patient 1 and at 2 months for patient 2 after the first surgery. The staging of the procedure is believed to assist with reducing the risk of paraplegia compared to performing the TEVAR in the acute phase like during the index admission. However, there might be a risk of aortic rupture from remaining dissection site while waiting for the 2nd stage TEVAR procedure. It is important to be thoughtful about the timing of the 2nd stage on a case-by-case basis to balance the risk and benefits.
There are some limitations in this study. First, it is a single-center retrospective study. Second, the number of cases is limited. Most of medical centers would not even offer any surgical intervention for patients with acute type A aortic dissection who refuse blood transfusions, and therefore only a handful of care reports are available. We hope this study could contribute to establishing a treatment option in such a category of sick patients.7,8
Conclusion
We presented this two-staged aortic repair strategy for acute type A dissection. It could facilitate bloodless surgery with achieving the primary purposes to treat acute type A dissection. The technique may have benefits for patients refusing blood transfusion as well as elderly and other operative high-risk patients.
Footnotes
Acknowledgments
We thank the team WADA for editorial editing.
Author contributions
TW wrote original draft. RM and VJ performed surgeries. TO and VJ supervised. All authors read and agreed with the final version of the manuscript. RM is a consultant for Endospan, Medtronic, and WL Gore.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.