
Abstract
Background
Lower extremity peripheral arterial disease (LEAD) is characterized by the narrowing and occlusion of arteries in the lower extremities. The most severe form of LEAD is chronic limb-threatening ischemia (CLTI), which carries a poorer prognosis for major amputation. The systemic immune-inflammation index (SII) is an index developed to simultaneously reflect the inflammatory and immunothrombosis status of patients, based on platelet counts and the neutrophil-to-lymphocyte ratio.
Objective
Our study aimed to investigate the relationship between elevated SII and major limb amputation.
Method
The study included 140 patients with foot wounds (Rutherford 5 or 6) due to LEAD who were scheduled for endovascular intervention between 2018 and 2023. Major amputation was required in 27 patients (19.2%). The neutrophil-to-lymphocyte ratio (2.1/2.8/3.8 vs 3.8/6.6/9.3, p < .001), platelet-to-lymphocyte ratio (103.8/128.8/162.9 vs 132.8/212.3/314.6, p < .001), and SII (527/720/1055.5 vs 1108/1951/3807, p < .001) were higher in the major amputation group. ROC curve analysis determined that the optimal cut-off value for SII to predict major amputation in LEAD patients was 1018, with a sensitivity and specificity of 81% and 73%, respectively (AUC: 0.84, 95% CI: 0.74–0.92, p < .001). Logistic regression analysis showed that high SII (OR = 1.001, 95% CI = 1–1.001, p = .009) was identified as an independent predictor of major amputation in LEAD patients.
Conclusion
This study establishes that a high SII value is associated with major amputation in LEAD patients with foot wounds.
Result
SII is a valuable and straightforward parameter for predicting major amputation risk and guiding treatment decisions in LEAD patients.
Introduction
Lower extremity peripheral arterial disease (LEAD) is characterized by the narrowing and occlusion of arteries in the lower extremities due to various etiologies. 1 LEAD affects over 202 million people worldwide, with more than 20% of individuals aged 65 and older suffering from this condition.2–5 The disease is increasingly recognized as a global issue due to its high prevalence in low- and middle-income countries. 1 The most severe form of LEAD is chronic limb-threatening ischemia (CLTI), which carries a poorer prognosis. 6 Major limb amputation and mortality are the most alarming outcomes for these patients. Pathologically, LEAD is primarily caused by atherosclerosis-induced stenosis of the lower extremity arteries. 7 Following coronary heart disease and cerebrovascular disease, atherosclerosis commonly affects the lower extremities. 8 Inflammation plays a crucial role in atherosclerosis, mediating all stages from initiation to progression.9,10 The systemic immune-inflammation index (SII) is an index developed to simultaneously reflect the inflammatory and immunothrombosis status of patients, based on platelet counts and the neutrophil-to-lymphocyte ratio. Elevated SII values are associated with poor prognosis in oncology patients,11,12 and its prognostic value has been demonstrated in various cardiovascular diseases related to atherosclerosis, such as coronary artery disease.13–17 However, no study has yet examined the association between SII and major amputation in LEAD. Our study aimed to investigate the relationship between elevated SII and major limb amputation, a critical cause of morbidity in LEAD patients with foot wounds. As a secondary aim, we explored the relationship between SII values and wound healing in this patient group.
Patient selection
The study included 185 patients with foot wounds (Rutherford 5 or 6) due to LEAD who were scheduled for endovascular intervention between 2018 and 2023. We excluded 45 patients due to death, oncological diseases, or end-stage liver failure, leaving 140 patients for retrospective evaluation. The diagnosis of LEAD was based on clinical presentation and objective examinations, including Doppler ultrasonography, computed tomography, and the ankle brachial index (ABI). The local ethics committee approved the study protocol in accordance with the Declaration of Helsinki. Foot wounds were classified according to the Society for Vascular Surgery WIfI classification system based on the opinions of 2 blinded and independent providers at the time of initial presentation. The WIfI classification is a scoring system that scores wounds according to wound, infection, and ischemia characteristics and predicts wound healing, prognosis, and amputation. 18 NLR, PLR, and SII values were calculated according to the following equations: NLR = neutrophil count/lymphocyte count; PLR = platelet count/lymphocyte count, and SII = (neutrophil count × platelet count)/lymphocyte count. Patients were considered hypertensive if they were taking antihypertensive medications or had a blood pressure above 140/90 mmHg. Diabetes was defined as being on antidiabetic medication or having fasting blood glucose levels above 126 mg/dL. Hyperlipidemia was defined as fasting total cholesterol >200 mg/dL, low density lipoprotein cholesterol >130 mg/dL, or chronic use of lipid-lowering drugs. Coronary artery disease (CAD) was defined as stenosis of more than 50% in at least one coronary artery, with a history of percutaneous coronary intervention and/or coronary artery bypass surgery. Heart failure was defined as an ejection fraction <40% on echocardiography. Chronic renal failure (CRF) was defined as a glomerular filtration rate (GFR) < 60 mL/min/1.73 m2 for more than 3 months.
Patient data
Demographic characteristics, comorbidities, and medication information were obtained from hospital records. Prior to the procedure, complete blood count, serum lipids, creatinine, albumin, and high-sensitivity C-reactive protein (Hs-CRP) levels were measured from venous blood samples. The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) were calculated from complete blood count. SII was calculated as the ratio of the multiplication of the neutrophil count and the platelet count to the lymphocyte count. 11
Patient classification and amputation
Pre-procedure ABI measurements were retrieved from hospital records. Rutherford classification of patients was obtained from clinic records and photographs of foot wounds. Patients classified as Rutherford class 5 (minor tissue loss) and class 6 (major tissue loss) were included in the study. 19 Amputation risk was evaluated using the Wound, Ischemia, Foot Infection (WIfI) score, which categorizes risk into four stages: stage 1 (very low), stage 2 (low), stage 3 (moderate), and stage 4 (high). 18 We divided patients into two groups based on the WIfI score: stage 4 (high risk) and others. Major amputation was defined as surgical removal of the extremity above the ankle, consistent with previous studies, while amputation at or distal to the Lisfranc level (tarsometatarsal joints) was not considered limb salvage failure. 20 Wound healing was defined as complete epithelialization of the tissue defect.
Statistical analysis
Statistical analysis was performed using SPSS for Windows (version 21.0; SPSS Inc., Chicago, Illinois, USA). The continuous data were expressed as the mean ± standard deviation or median (interquartile range) depending on normality, assessed using the Kolmogorov–Smirnov test. The categorical variables were expressed as counts (n) and percentages (%). According to normality, the group means for continuous variables were compared using either the independent samples t-test or the Mann–Whitney U test. Pearson’s correlation coefficients were used to determine the SII and major amputation correlations.
As appropriate, the categorical variables were compared using the chi-square or Fisher’s exact test. We determined the optimal cutoff value for SII for predicting major amputations with maximum sensitivity and specificity using the area under the curve (AUC) from the receiver operating characteristic (ROC) curves. The association of different variables with major amputations and wound healing was calculated in univariate analysis. Variables showing marginal associations with the no-reflow and wound healing on univariate testing (p < .50) were included in the multivariate regression analysis. The stepwise method with backward elimination was used. Odds ratios with 95% confidence intervals were also calculated. A two-sided p < .05 was considered statistically significant.
Results
Baseline demographic and clinical characteristics.
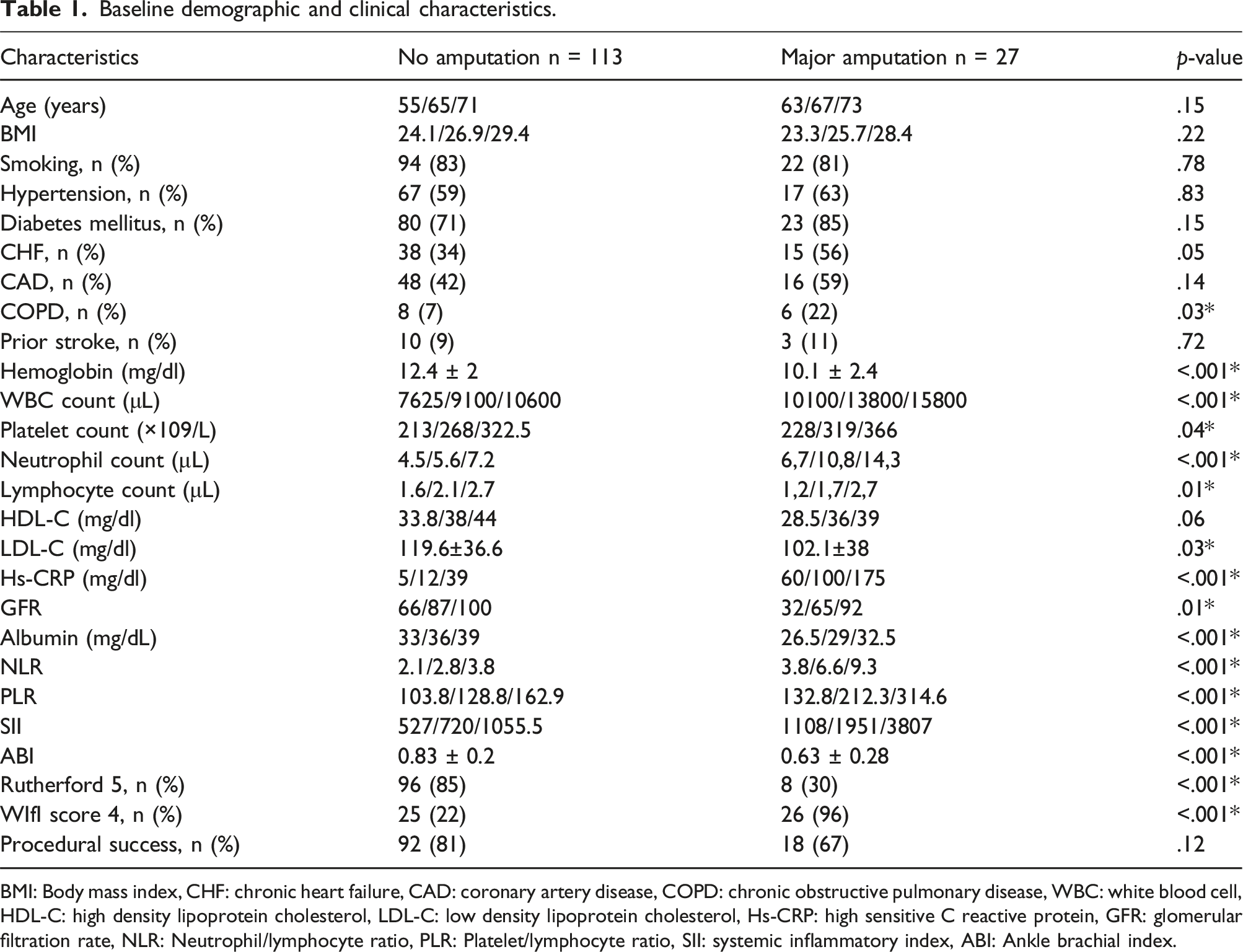
BMI: Body mass index, CHF: chronic heart failure, CAD: coronary artery disease, COPD: chronic obstructive pulmonary disease, WBC: white blood cell, HDL-C: high density lipoprotein cholesterol, LDL-C: low density lipoprotein cholesterol, Hs-CRP: high sensitive C reactive protein, GFR: glomerular filtration rate, NLR: Neutrophil/lymphocyte ratio, PLR: Platelet/lymphocyte ratio, SII: systemic inflammatory index, ABI: Ankle brachial index.
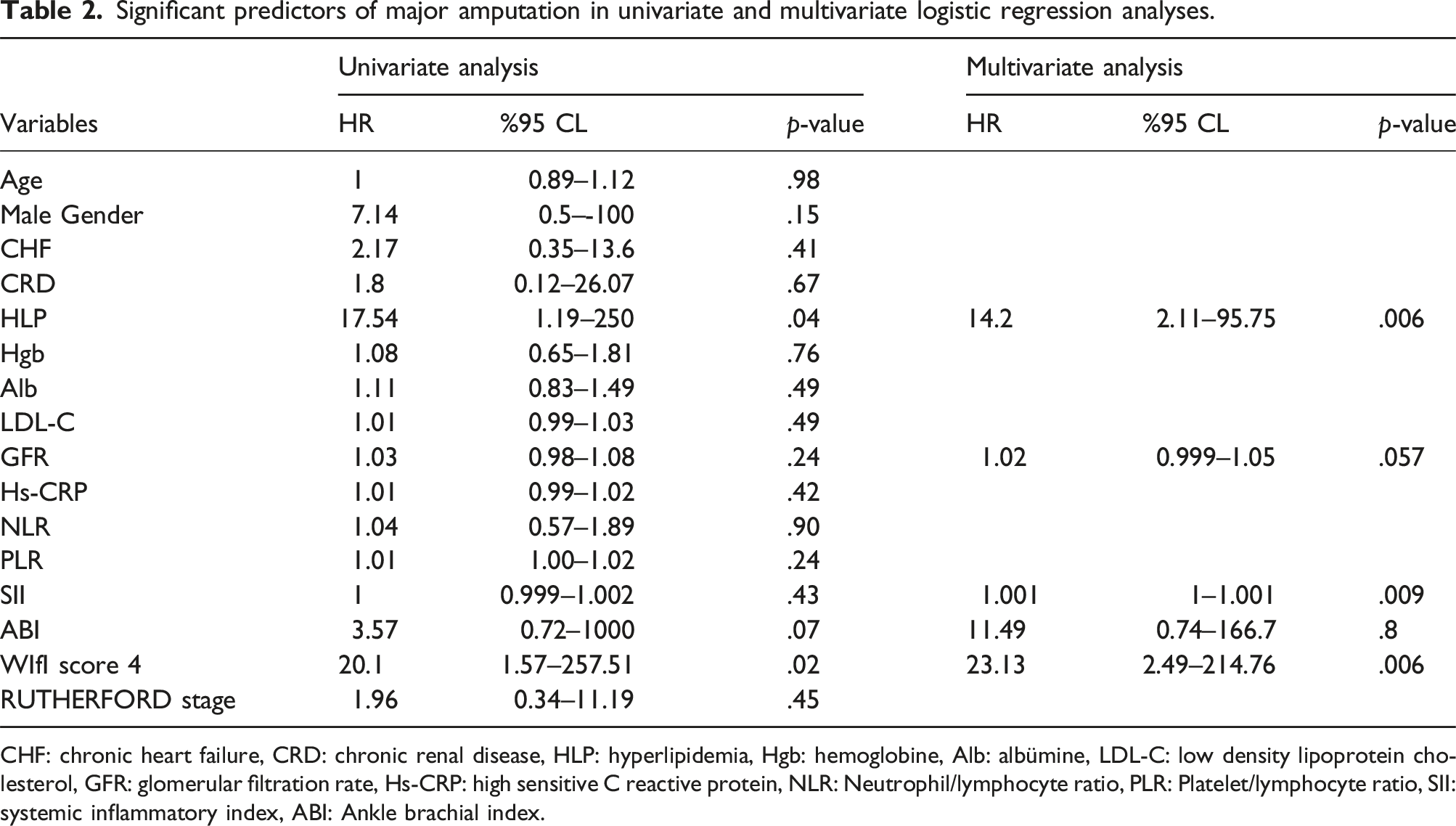
ROC curve analysis determined that the optimal cut-off value for SII to predict major amputation in LEAD patients was 1018, with a sensitivity and specificity of 81% and 73%, respectively (AUC: 0.84, 95% CI: 0.74–0.92, p < .001) (Figure 1). Logistic regression analysis evaluated potential risk factors for major amputation, including age, gender, CHF, CRF, HLP, hemoglobin, albumin, GFR, CRP, NLR, PLR, SII, ABI-L, WIfI, and Rutherford classification. Variables correlating with major amputation in univariate analysis (HLP, GFR, SII, ABI-L, and WIfI) were further analyzed using multivariate logistic regression. High SII (odds ratio (OR) = 1.001, 95% confidence interval (CI) = 1–1.001, p = .009) was identified as an independent predictor of major amputation in LEAD patients (Table 2). ROC curve analysis for systemic immune-inflammation index (SII), and neutrophil to lymphocyte ratio (NLR), platelet to lymphocyte ratio (PLR). Significant predictors of major amputation in univariate and multivariate logistic regression analyses. CHF: chronic heart failure, CRD: chronic renal disease, HLP: hyperlipidemia, Hgb: hemoglobine, Alb: albümine, LDL-C: low density lipoprotein cholesterol, GFR: glomerular filtration rate, Hs-CRP: high sensitive C reactive protein, NLR: Neutrophil/lymphocyte ratio, PLR: Platelet/lymphocyte ratio, SII: systemic inflammatory index, ABI: Ankle brachial index.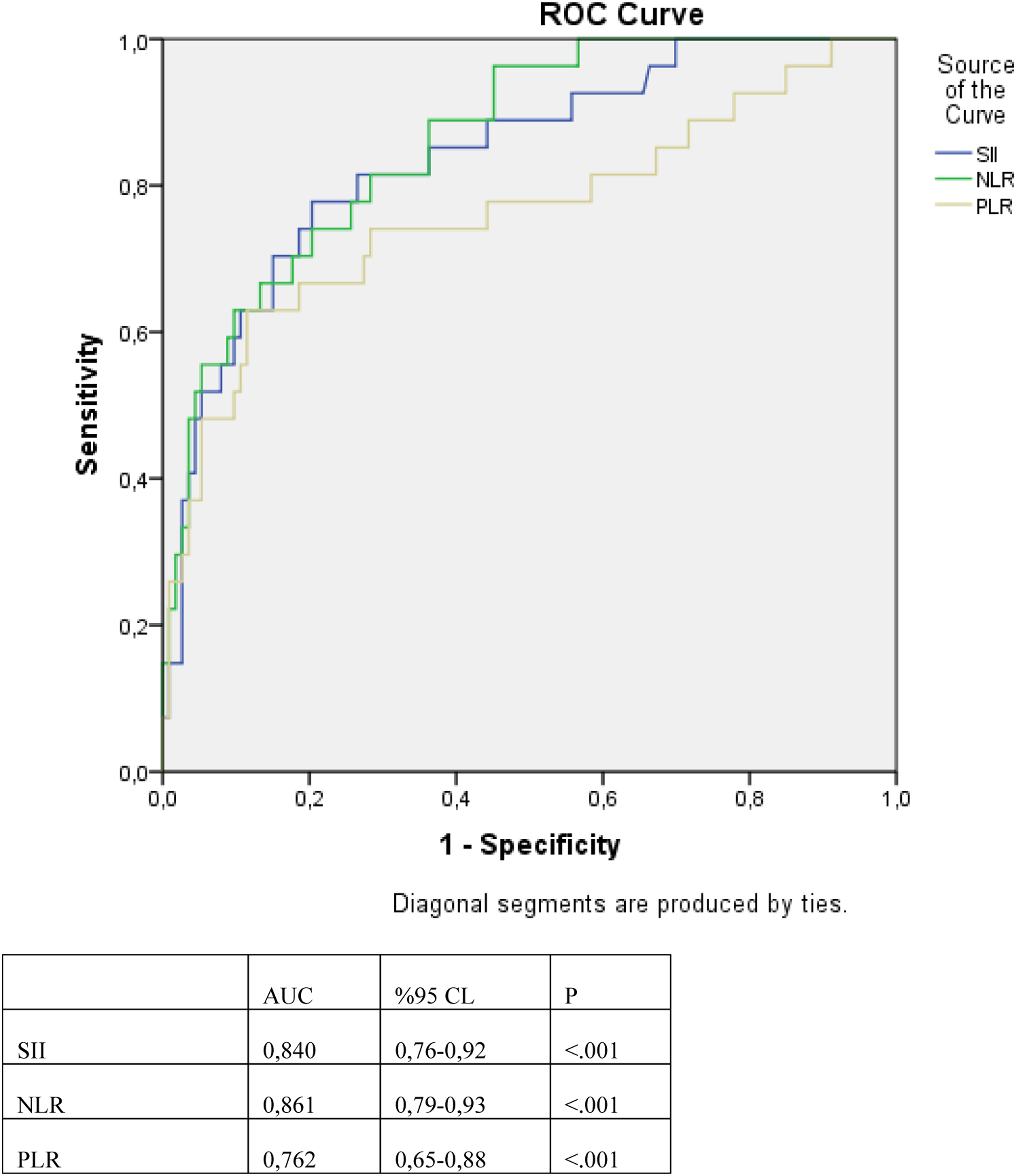
Significant predictors of wound healing in univariate and multivariate logistic regression analyses.
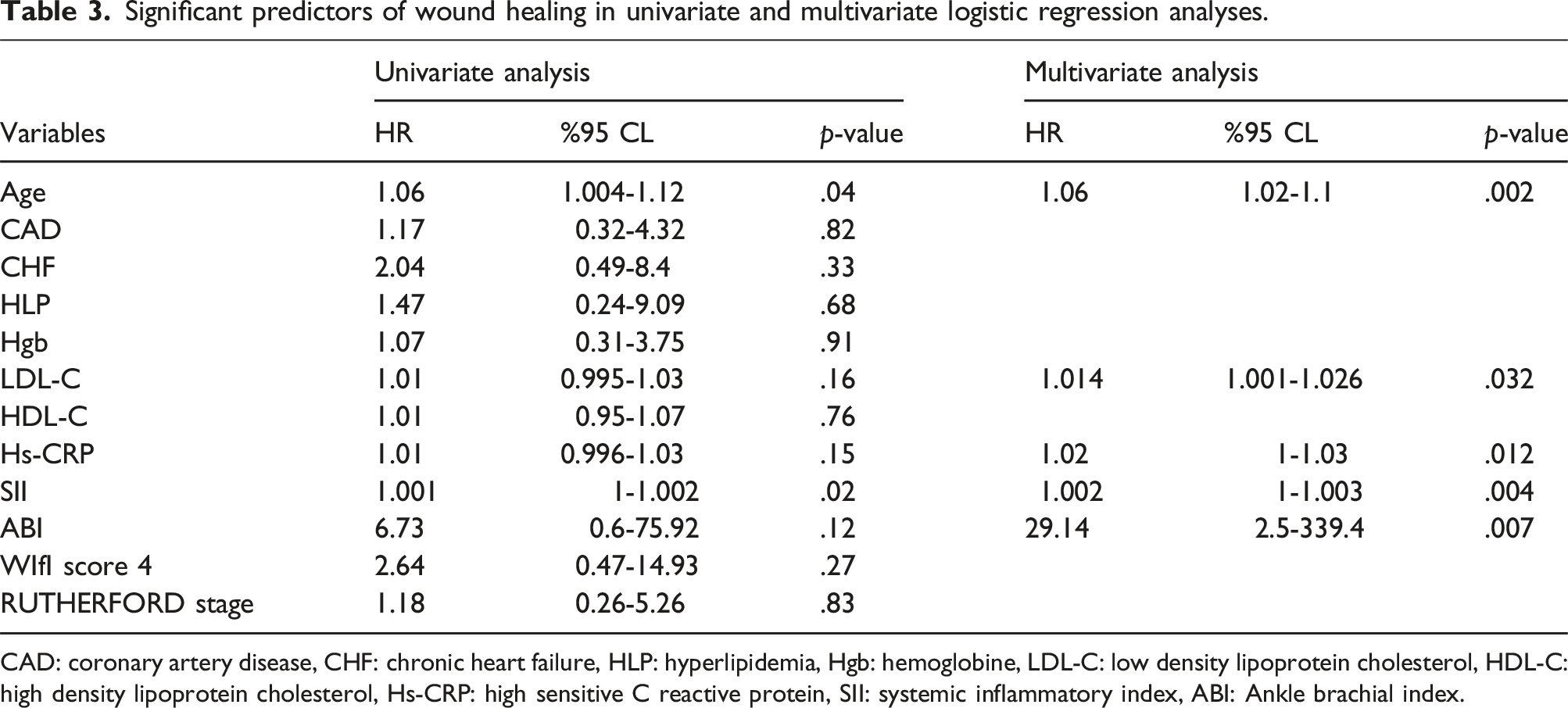
CAD: coronary artery disease, CHF: chronic heart failure, HLP: hyperlipidemia, Hgb: hemoglobine, LDL-C: low density lipoprotein cholesterol, HDL-C: high density lipoprotein cholesterol, Hs-CRP: high sensitive C reactive protein, SII: systemic inflammatory index, ABI: Ankle brachial index.
Discussion
This study offers significant insights into the relationship between Systemic Immune-Inflammation Index (SII) and major amputation outcomes. Our findings indicate that SII is an independent predictor of major amputation in patients with foot wounds and lower extremity arterial disease (LEAD). Furthermore, a significant correlation was observed between wound healing and SII.
Major amputation, resulting from LEAD, represents a highly undesirable outcome that adversely affects patients’ quality of life. A recent meta-analysis published in 2024 examined nine studies, revealing that major amputation-free survival was 79.2% (429/542) in patients undergoing direct revascularization based on the angiosome concept, compared to 60.8% (247/406) in those receiving indirect revascularization. 21 Li et al. reported a major amputation rate of approximately 5% among 312 LEAD patients. 22 Similarly, Lida et al. (2012) found that about 19% of LEAD patients experienced limb loss due to major amputation. 20 Variations in major amputation rates across studies may be attributed to differences in patient classification according to LEAD severity and the type of revascularization performed. Our cohort predominantly included patients with severe LEAD, specifically Rutherford grade 5–6, with 25.7% classified as Rutherford grade 6. Among the 140 patients, 36.4% had WIfI stage 4, and nearly half (50.9%) of these required major amputation. Previous studies have documented an increased risk of amputation in advanced WIfI stages, with Cull et al. reporting 40% and 23% amputation rates in WIfI stage 4 and stage 3 patients, respectively, at one-year follow-up. 23 Our analysis of patients with and without endovascular intervention showed that major amputation occurred in approximately 20% of the cohort.
Currently, there are studies indicating that vessels revascularized according to the angiosome concept in infrapopliteal endovascular procedures have more favorable wound healing results, but the effect of this treatment on limb salvage is still controversial.. 20 In a study by Soares et al. evaluating 95 infrapopliteal endovascular procedures, it was concluded that the angiosome concept in endovascular treatment was no longer important for limb salvage rates or ulcer/wound healing rates. Furthermore, in the same study, WIfI classification 0-1 was associated with faster and higher wound/ulcer healing rates than WIfI classification 2-3. 24
In our study, there was no statistically significant difference in major amputation rates between those who underwent successful endovascular intervention and those who did not (92 (81%) versus 18 (67%), p = .12). This lack of significance may be attributed to the study’s sample size and the lack of stratification based on direct versus indirect revascularization. In fact, studies have shown that direct revascularization is a more effective method in terms of preventing major amputation. 21
Inflammation plays a critical role across all stages of LEAD, with studies indicating that LEAD may be more strongly associated with inflammation than coronary artery disease. 25 Cauley et al. found higher prevalence of LEAD in patients with elevated levels of inflammatory markers such as interleukin-6, tumor necrosis factor-α, and CRP. 26 Additionally, activated neutrophils and platelets contribute to microvascular damage and thrombus formation, further exacerbating inflammation and coagulation. 27
Recent research has highlighted the clinical utility of inflammatory ratios in predicting outcomes in LEAD. Onofrei et al. demonstrated that NLR and PLR values are valuable for assessing obstruction severity and amputation risk. 28 Cosarca et al. identified NLR values above 3.48 as having 60% sensitivity and 72.44% specificity for predicting amputation post-revascularization. 29 In several studies, increased absolute neutrophil counts relative to lymphocyte counts are associated with a worse prognosis in interventionally treated LEAD patients.30,31 Similarly, Tasoglu et al. associated high NLR and PLR values with increased amputation risk. 32
SII, a composite marker incorporating total platelet count and neutrophil/lymphocyte ratio, reflects overall immune and inflammatory status. Previous studies have established SII as a robust prognostic indicator for various malignancies and cardiovascular diseases.11,12 Vatan et al. showed that SII was an independent determinant of the development of no-reflow phenomenon in patients who presented with STEMI and underwent primary PCI. 15 In a similar study, Cakmak et al. found that SII was an independent determinant in showing the development of no-reflow in patients who presented with acute coronary syndrome and underwent percutaneous intervention into saphenous vein grafts. 16 Selçuk et al. showed that SII was an independent determinant of postoperative atrial fibrillation in patients who underwent coronary artery bypass grafting. 33 A study by Tosu et al revealed that SII was an independent predictor of major adverse cardiac events in aortic stenosis patients after trans-catheter aortic valve implantation. 17 In the study conducted by Zhang et al., SII was found to be an independent determinant of the presence of LEAD. 34 In a study by Oflar et al., it was shown that high SII was associated with the complexity of LEAD, which they determined according to the Trans-Atlantic Intersociety Consensus (TASC II) classification. 35
In our study, high preoperative SII values independently predicted major amputation in LEAD patients (odds ratio = 1.001, 95% CI = 1–1.001, p = .009). Furthermore, WIfI clinical stage 4 emerged as an independent risk factor for major amputation (odds ratio = 23.13, 95% CI = 2.49–214.76, p = .006). While endovascular pedal arch revascularization showed promising results, our findings indicated no statistically significant difference in major amputation rates among patients undergoing this procedure (13 (100%) versus 0 (0%), p = .73), potentially due to the small sample size.
Foot wounds significantly impact patient quality of life and healthcare resource utilization. Our study revealed that SII is a valuable parameter for predicting wound healing, with lower SII values associated with successful wound healing (odds ratio = 1.002, 95% CI = 1–1.003, p = .004).
However, this study has limitations. It is a single-center, retrospective, and cross-sectional analysis with a relatively small patient cohort and limited follow-up duration. We assessed only pre-procedure SII levels, without considering post-procedure or follow-up SII values. Additionally, patients were not stratified by revascularization type based on the angiosome concept. This relatively small-size and retrospective study has shown that SII is a marker predicting major amputation in CTLI. In order to demonstrate the clinical efficacy of SII and its effectiveness in follow-up after endovascular treatment with different treatment modalities, prospective studies with larger populations should be conducted.
Conclusions
This study establishes that a high SII value is associated with major amputation in LEAD patients with foot wounds. Moreover, SII was found to correlate with wound healing at the 6-month follow-up in this patient group. These findings suggest that SII is a valuable and straightforward parameter for predicting major amputation risk and guiding treatment decisions in LEAD patients.
Footnotes
Author contributions
All authors take responsibility for all aspects of the reliability and freedom from bias of the data presented and their discussed interpretation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.