
Abstract
Objectives
Ankle and toe brachial pressure index are recommended globally as first line non-invasive screening tests for peripheral arterial disease. However, they can be inaccurate and have limited utility in patients with incompressible arteries, lower limb wounds and/or lack of digits. This study aims to evaluate BlueDop, a novel device that purports to assess peripheral perfusion without the need for a lower limb tourniquet or patients lying flat.
Methods
Patients attending vascular and podiatry clinic at Aneurin Bevan University Health Board were recruited between May 2022 and May 2023. A BlueDop reading was recorded in addition to ankle and/or toe brachial pressure index. Satisfaction and preference of each method was recorded using an electronic proforma.
Results
176 patients were included. BlueDop ABPI was shown to be moderately correlated with cuff-ABPI (rs = 0.42, p = .001) and weakly correlated with TBPI (rs = 0.22, p = .04). BlueDop had moderate accuracy in diagnosing PAD (C statistic = 0.653) and was more accurate in diagnosing severe PAD (C statistic = 0.706). Diagnostic accuracy appeared to be improved when PAD was defined according to cuff-ABPI only. Patients were more satisfied with BlueDop (mean satisfaction score (MSS) = 4.33) compared to cuff-ABPI (MSS = 2.89, mean difference = 0.544, p < .001) and TBPI (MSS = 3.82, mean difference = 0.579, p < .001) while operator satisfaction was equal.
Conclusions
There is moderate correlation between BlueDop and cuff-ABPI. Patients prefer BlueDop to cuff-ABPI or TBPI. BlueDop appears to be an acceptable method of non-invasive assessment of PAD, although users must appreciate there is a discrepancy between it and cuff-ABPI/TBPI.
Keywords
Introduction
The incidence of peripheral arterial disease (PAD) is increasing worldwide with an increasing physical and psychosocial burden on patients, and a financial burden on health services. 1 Patients with PAD can be asymptomatic; however, they can progress – often in a non-linear fashion 2 – to chronic limb threatening ischaemia (CLTI) with features of ischaemic rest pain and/or tissue loss. 3 Early detection and management of CLTI is imperative as there is an estimated risk of limb loss of 20% at 1 year if left untreated. 3
Ankle-brachial pressure index (ABPI) is currently recommended as a first line non-invasive method of assessment to aid diagnosis of PAD as per European (European Society Vascular Surgery), 4 International (International Working Group on the Diabetic Foot) 5 and Global guidelines. 2 Although ABPI is considered the gold standard in non-invasive screening for PAD, limitations of its accuracy and reproducibility have been documented. 6 Best practice suggests that there should be a pre-ABPI rest time of up to 10-min and readings should be taken with the limbs in a horizontal plane. 7 Other limitations include artificially elevated readings due to medial artery calcification (seen frequently in patients with diabetes mellitus and renal disease 2 ) and inability to perform pressure measurements due to lower limb wounds or patient pain. 8 An alternative pressure reading is the Toe Brachial Pressure Index (TBPI). TBPI utilises digital arteries that are less likely to develop medial sclerosis. 9 It is recommended by several guidelines to assess the presence and severity of PAD.2,10 While TBPI is useful, it requires training to use, and it cannot be undertaken in patients with toe wounds or digital amputations.
The BlueDop is a novel hand-held device that purports to evaluate limb perfusion without the need for a lower limb tourniquet or patients lying flat. 11
There are limited data on BlueDop value as a screening tool for PAD. Korszadeh et al studied 276 limbs in 166 patients and concluded that BlueDop is accurate and sensitive at detecting PAD when compared with Duplex sonography. 12 It is not, however, clearly determined how well BlueDop correlates with cuff-ABPI or TBPI undertaken in an unselected cohort of patients referred to the Vascular/Podiatry clinic, including those with diabetes.
This study aims to evaluate the utility, acceptability and patient/operators experience of using BlueDop as a novel device for assessing PAD by comparing BlueDop to the gold standard of non-invasive screening methods, cuff-ABPI and TBPI.
Materials and methods
Study summary
This study is reported according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. 13 A cross-sectional prospective study was conducted in the Vascular and Podiatry outpatient department at Aneurin Bevan University Health Board, UK, between May 2022 and May 2023. Research and Development approval was sought prior to data collection (SE/1343/21). The approval included designation of the study as a ‘service evaluation’ not requiring formal ethical approval.
The BlueDop device
BlueDop is a Conformité Européene (CE) approved hand-held device that calculates ABPI, perfusion pressure and ‘vascular reserve’ (a percentage measure of arterial ‘redundancy’ within the limb) without the need for a tourniquet or patients lying flat.
It comprises a probe, used to record arterial waveforms of the arteries at the ankle, and a linked tablet which processes the input and provides results (Figure 1). The user inputs the patient’s systolic brachial blood pressure into the tablet, then uses the BlueDop probe, held still over the dorsalis pedis and posterior tibialis arteries, to analyse the doppler waveform. BlueDop uses ‘pressure from flow’ technology, that is, it evaluates the doppler waveform of the distal tibial arteries, and, after inputting the systolic blood pressure, gives an estimate of ABPI and other variables.
11
The device uses these data to calculate an ABPI and other outputs (see supplemental material 1 for details of these calculations). The precise methods used to calculate these results are not available in the public domain to the best of the author’s knowledge. The resultant ‘BlueDop-ABPI’ reading is from 0 to 1 with >0.8 implying no significant PAD, <0.8 implying PAD and <0.5 implying critical limb ischaemia. As the pressure in the ankle arteries is assumed to not be greater than the brachial systolic blood pressure, BlueDop does not produce ABPI values >1. BlueDop in use with linked tablet.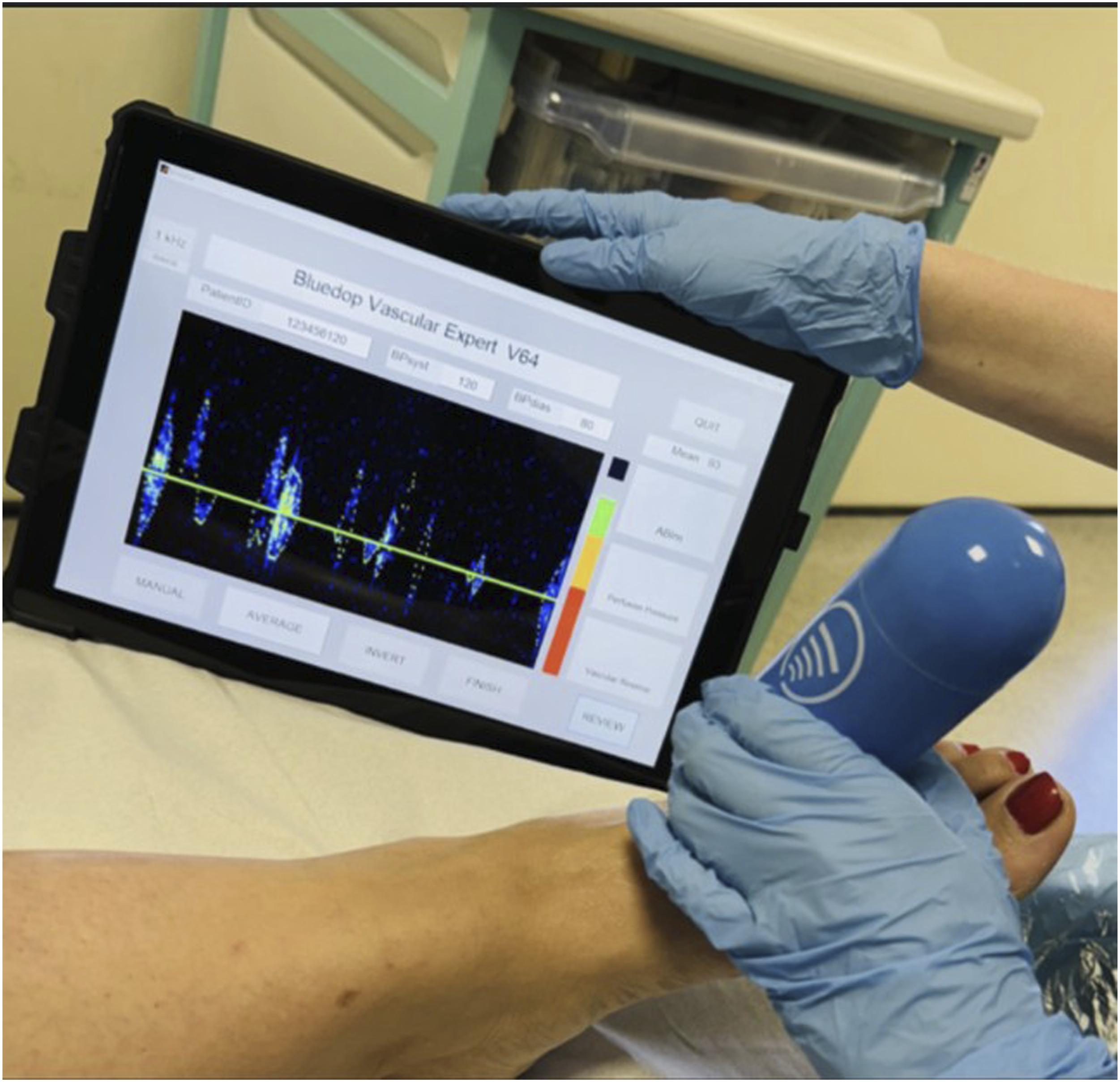
BlueDop requires simple training to use, and costs approximately £5000 (equivalent to €5,700 or $6300). Prior to commencing this study operators received device training from BlueDop Medical and those not in attendance received cascade training. Those undertaking ABPI/TBPIs were experts and were well versed in these skills as part of their clinical role. They were the same operators as those undertaking the BlueDop.
Participant identification
Participants suitable for inclusion were patients referred to the vascular and podiatry clinic with possible or suspected PAD undergoing investigation with traditional cuff-ABPI and/or TBPI. Recruitment was by convenience sampling on attendance to clinic. Patients without an indication for ABPI or TBPI were excluded.
Verbal consent was obtained prior to any recording of lower limb arterial supply (BlueDop, cuff-ABPI, TBPI), as per General Medical Council guidelines. 14 Data were collected at a single time point. A BlueDop reading was taken in addition to cuff-ABPI and/or TBPI. In cases where neither a cuff-ABPI nor TBPI could be recorded, and a BlueDop reading was taken, these data were not used for comparative analysis. Patient and operator experience of BlueDop, cuff-ABPI and TBPI were evaluated using a simple satisfaction questionnaire.
Data capture
Data were collected using an electronic proforma, which was completed at the time of data capture by the operator. This comprised indication for investigation(s)/reason for referral, cuff-ABPI and/or TBPI, BlueDop ABPI, time taken for each investigation, patient/operator satisfaction and patient/operator preference for each investigation. Reason for inability to perform an investigation was documented (e.g. wounds or incompressible calf vessels). Patient presenting symptoms (if any) were recorded, that is, claudication, tissue loss and rest pain. Patient and user satisfaction was recorded on a 5-point Likert scale ranging from one (very unsatisfied) to five (very satisfied). Primary outcomes were cuff ABPI and/or TBPI and BlueDop ABPI value. Secondary outcomes were patient and operator experience and preference.
Statistical methods
The Spearman Rank test was used to evaluate correlation, with ‘rs’ denoting the correlation coefficient (ranging −1 to +1). For this analysis, cuff-ABPI and TBPI values were truncated to have a maximum value of 1 since BlueDop gives a maximum value of 1 for ABPI. Bland-Altman analyses were used to evaluate agreement between different methods of measurement. Bland-Altman plots were produced to visually represent the data, and a regression line fitted to demonstrate any potential proportional bias (where the bias varies depending on the result (ABPI value)). The bias (the mean difference between the two methods values) was calculated along with 95% confidence intervals (CIs). The limits of agreement were defined as the bias +/−1.96 standard deviation values.
C-statistics were calculated to assess BlueDop ABPI’s accuracy in identifying patients with PAD (defined as cuff ABPI<0.8 or TBPI<0.7) and severe PAD (defined as cuff ABPI<0.5 or TBPI<0.3). A C-statistic of >0.9 was considered outstanding, 0.7 to 0.9 considered acceptable, 0.6 to 0.7 considered poor and 0.5 considered no better than chance. Corresponding sensitivity, specificity, positive and negative predictive values (PPV and NPV) were also calculated. These are represented at the ‘optimal threshold’ which was determined using the ‘Youden method’ which aims to identify the threshold which maximises both sensitivity and specificity and is commonly used to report the performance of a prediction model.
Subgroup analyses included evaluating BlueDop’s accuracy to predict PAD and severe PAD when these were defined according to cuff ABPI alone and cuff TBPI alone.
A mean satisfaction score (MSS) was calculated for each method using the value of satisfaction according to the Likert scale from 1 (very unsatisfied) to 5 (very satisfied) (see supplemental material 2). The mean difference was compared using the paired t test.
Results
Documented reason for inability to record result.

Correlation of BlueDop with cuff-ABPI or TBPI
BlueDop ABPI was moderately correlated with cuff-ABPI (rs = 0.42, p = .001) and weakly correlated with TBPI (rs = 0.22, p = .04).
Figure 2 demonstrates a Bland-Altman plot comparing BlueDop and cuff-ABPI values. The plot’s regression line demonstrates potential proportional bias (the difference between the two methods increases as the mean of their values increase). The bias was 0.062 (95%CI = 0.006 to 0.119). The limits of agreement were −0.358 to 0.482. This estimates that in 95% of cases, the difference between BlueDop and cuff-ABPI ranges from −0.358 and 0.428. Bland-Altman plot comparing BlueDop and cuff-ABPI values. Downward sloping values in the top right of figure two represent cases where cuff-ABPI values were truncated to = 1.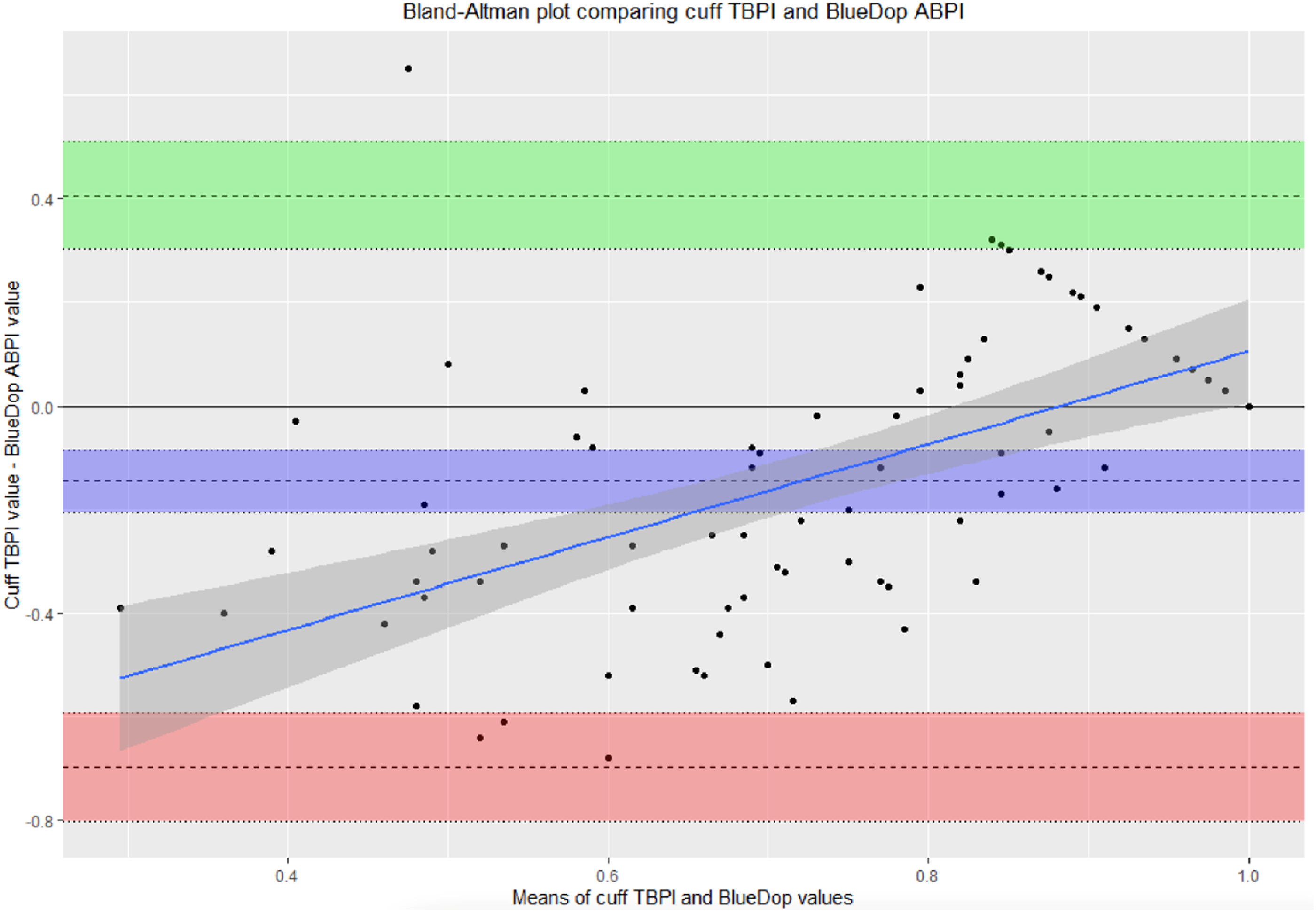
Figure 3 demonstrates a Bland-Altman plot comparing BlueDop and TBPI values. The regression line demonstrates potential proportional bias (increasing as the mean values increase). The bias was −0.145 (95%CI = −0.206 to −0.084). The limits of agreement were −0.697 to 0.303. This estimates that in 95% of cases, the difference between BlueDop and TBPI ranges from −0.697 and 0.303. Bland-Altman plot comparing BlueDop and TBPI values. Downward sloping values in the top right of figure two represent cases where cuff-TBPI values were truncated to = 1.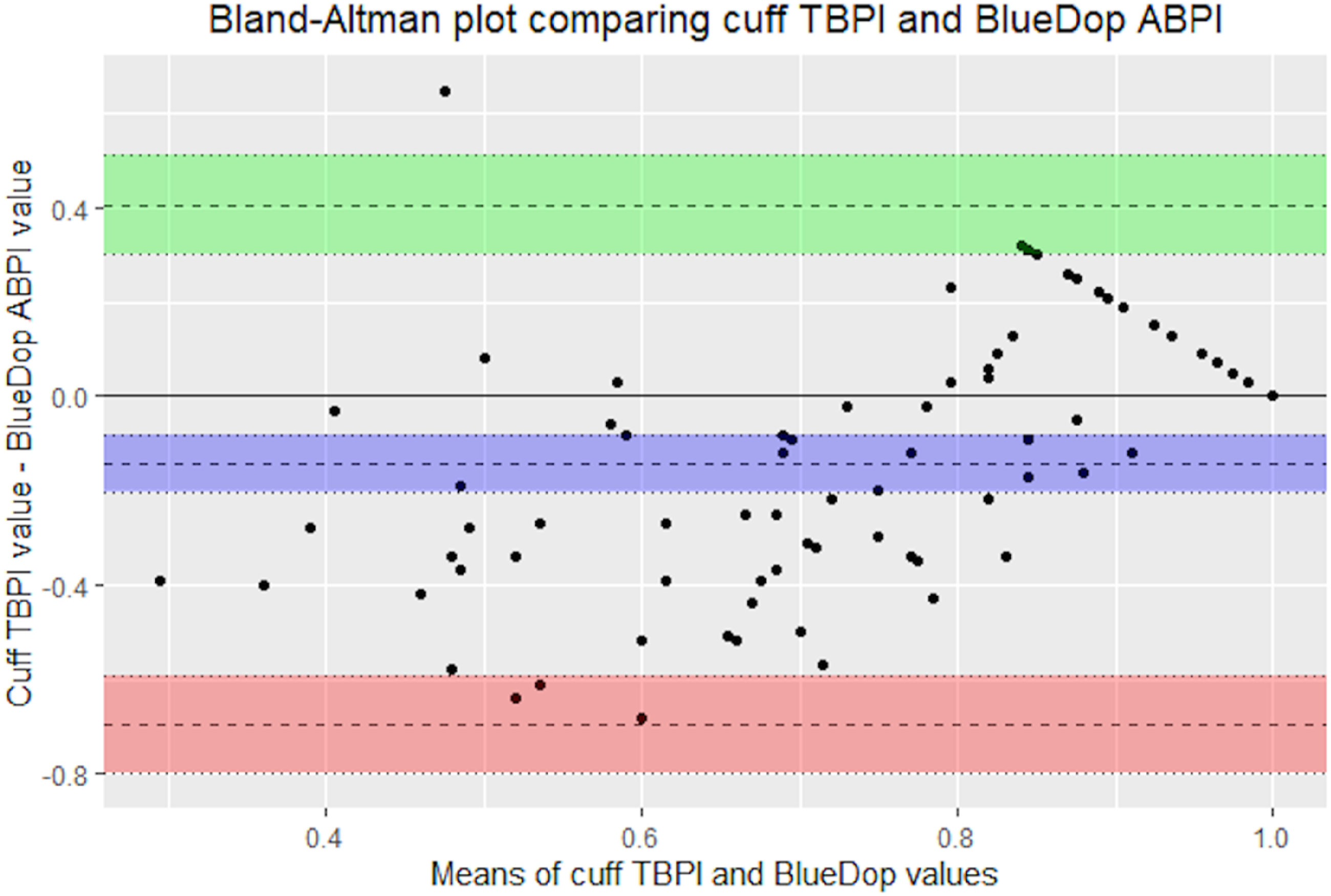
Ability of BlueDop to predict PAD and severe PAD
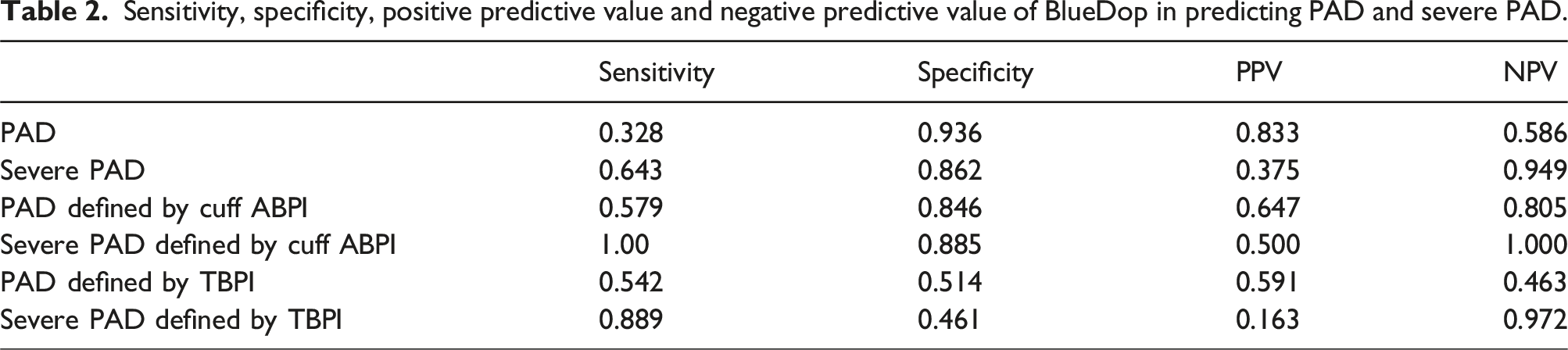
BlueDop had C-statistics of 0.600 and 0.748 in predicting PAD and severe PAD, respectively (Figure 4). Table 2 demonstrates the sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) of BlueDop in predicting PAD and severe PAD and when defined by cuff-ABPI and TBPI alone. C-statistics were better (0.713 and 0.942, respectively) when PAD/severe PAD was defined according to cuff-ABPI only and were less good (0.421 and 0.659, respectively) when PAD/severe PAD was defined by TBPI only. Corresponding predictive values were also worse. Receiver operating characteristic (ROC) curve demonstrating C statistics of BlueDop in predicting PAD and severe PAD. Sensitivity, specificity, positive predictive value and negative predictive value of BlueDop in predicting PAD and severe PAD.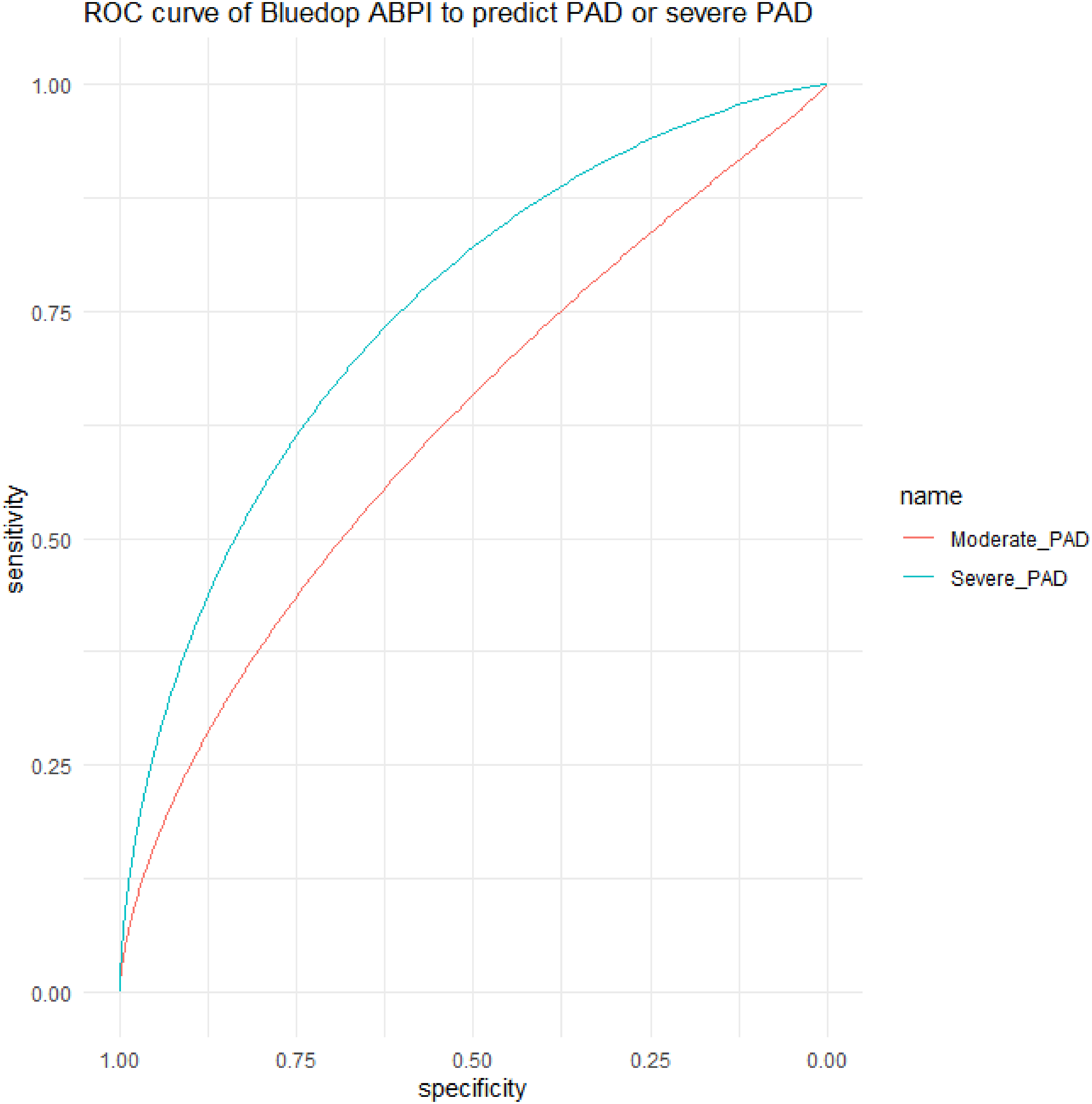
Satisfaction with BlueDop
Patients were more satisfied with BlueDop (MSS = 4.33) compared to ABPI (MSS = 2.89; mean difference = 0.544, p < .001), and when compared to TBPI (MSS = 3.82, mean difference = 0.579, p < .001).
Operator satisfaction was equivalent between BlueDop (MSS = 4.29) and ABPI (MSS = 2.83, mean difference = 0.250, p = .137) and TBPI (MSS = 1.94, mean difference = 0.300, p = .104).
Discussion
In this prospective observational study of 176 limbs, correlation of absolute values of BlueDop was moderate with cuff-ABPI and was weak with TBPI. BlueDop was poor at predicting PAD/severe PAD (defined using a combination of cuff-ABPI and TBPI or TBPI alone), but when PAD/severe PAD were defined with cuff-ABPI alone, BlueDop’s predictive abilities to diagnose PAD/severe PAD was poor-acceptable. Overall, patients reported greater satisfaction with BlueDop compared to ABPI and TBPI. Operator satisfaction with BlueDop compared to ABPI and TBPI was equivocal.
Whilst ABPI and TBPI are considered the gold standard for screening and diagnosis of PAD, both are flawed. 14 There are some data available to support individual non-invasive tests in the diagnosis of PAD; however, there is no perfect method. 14 A normal ABPI cannot reliably exclude PAD, however, false positive rates are generally low and therefore it can aid in screening. 14 Alternatively, a normal TBPI makes a diagnosis of PAD less likely. 14 Variable diagnostic reliability and a lack of standardised normal values for TBPI could explain the weaker correlation between TBPI and BlueDop in this study. 5 An additional test that could be considered for future comparison is pulse volume recording (PVR). BlueDop and PVR have similarities in utilising waveform analysis to estimate perfusion, 15 whereas PVR measures the waveform response to inflation of a cuff. It is not routinely measured in the Aneurin Bevan University Health Board, therefore was not chosen for comparison in this study. As there is no perfect non-invasive screening test for PAD, there is no perfect comparison for BlueDop. This could explain the correlation findings in this study compared to Korszadeh et al, who document an accuracy of 92%, sensitivity of 95% and specificity of 90% when compared to Duplex sonography. 12 Moreover, all tests are operator dependent which can lead to variation in results. The sensitivity, specificity, NPV and PPV reported in this study vary in part due to our method of producing these values to optimise both sensitivity and specificity which is susceptible to change due to changes in the ROC curves’ shapes.
A greater patient satisfaction with BlueDop compared to ABPI and TBPI was demonstrated in this study. This is understandable and aligns in part to qualitative research that highlighted that patients with PAD and CLTI can have poor experience of cuff-ABPI due to factors such as tissue loss and pain. 8 A method of evaluating limb perfusion that is viewed more favourably by patients could positively influence patient compliance with screening. Operator satisfaction of BlueDop compared to ABPI/TBPI was equivocal, however, the cohort of operators in this study are frequently using ABPI/TBPI in the vascular and podiatry clinic. Overall, operators find all methods acceptable.
A strength of this study is the prospective design. Furthermore, inclusivity in terms of patients with a variety of underlying pathologies, such as diabetes, reflects real work practice making this study clinically relevant. In addition, comparison of BlueDop to ABPI and TBPI makes this study applicable to current practice.
Limitations of this study include lack of blinding, and potential reporting bias as patients submitted responses directly to the operator, potentially impacting subjective outcomes. Patients who did not have both ABPI/TBPI and BlueDop could not be included in comparative analysis. The factors preventing assessment with ABPI and TBPI included wounds or lack of digits meaning a significant proportion of patients presenting to such services were excluded, limiting the applicability of the results. The sample size for this study was not determined by a power calculation. To the best of our knowledge, there are no publicly available data comparing BlueDop to ABPI or TBPI that would inform such calculations. We cannot determine BlueDop’s usefulness in comparison with other tests, such as Duplex sonography, CT or MR angiography, or the gold standard: digital subtraction angiography, which are accepted to have far greater sensitivity and specificity than ABPI or TBPI. Further comparison of BlueDop with these imaging modalities in addition to clinical outcomes would provide valuable information on its efficacy. Whilst operator satisfaction with BlueDop in this study was equivalent to other methods, we must acknowledge that they were all well versed in assessing limb perfusion with cuff-ABPI and TBPI; therefore, we cannot assert that non-specialist users would report the same.
BlueDop’s ability to better predict more severe PAD suggests that it could be best placed in the vascular clinic for initial assessment of patients with suspected CLTI, or perhaps in the podiatry clinic which frequently assesses patients with high risk lower limbs. It would need to achieve reasonable sensitivity in predicting patients with severe PAD as the corresponding specificity was low which is a limitation since the number of false positives will be relatively high. Ultimately, further evidence demonstrating a correlation of BlueDop with mild to moderate PAD would be required in order to support introduction into a non-specialist setting. Features of CLTI, such as significant rest pain and tissue loss, might also make the cuffless feature even more appealing compared to cuff-ABPI or TBPI for this patient group.
Supplemental Material
Supplemental Material - Can BlueDop be used as an alternative for diagnosing peripheral arterial disease? A prospective comparison of traditional ABPI and TBPI with BlueDop
Supplemental Material for Can BlueDop be used as an alternative for diagnosing peripheral arterial disease? A prospective comparison of traditional ABPI and TBPI with BlueDop by Lucy Fligelstone, Brenig Llwyd Gwilym, Melissa Blow, Julie Lee, Annie Clothier, Kristian Glover, Tracey Hutchings and David C Bosanquet in Vascular
Footnotes
Present address: Sunshine Coast University Hospital, 6 Doherty Street, Birtinya, QLD 4575
Author’s note
This work has been presented at the Vascular Societies’ Annual Scientific Meeting in Brighton (2022) and Dublin (2023).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Mr David Bosanquet has received funding from All Wales Diabetes Implementation Group (AWDIG) and the Royal College of England (Pump Priming Grant) to purchase the BlueDop equipment. Neither he nor any other member of the team have received any funding from BlueDop Medical at any point.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.