
Abstract
Objective
To compare endovascular kissing stent (KS) and aortobifemoral bypass (AFB) procedures in patients with bilateral common iliac artery occlusion.
Materials and Methods
This was a single-centre retrospective study. Subjects who underwent treatment for bilateral TASC II C and D common iliac artery occlusion between August 2013 and August 2021 with at least 3 years of follow-up were included in the study. The study group was divided into kissing stent (group A) and aortobifemoral bypass (group B) groups. The subjects’ demographic data (including age, sex, body mass index (BMI), smoking history, comorbid diseases and medications), TransAtlantic Inter-Society Consensus (TASC) II classifications and Rutherford classifications were noted. Preoperative diagnostic data included ankle–brachial index (ABI) measurements and computed tomography (CT) angiography assessments of the aorta and iliac–femoral axis. Intraoperative data (including operative times and complications) and hospital stay data were recorded. Patients were evaluated at the 1st, 3rd, 6th, 12th, 24th and 36th months after the procedure at outpatient visits. The primary patency, primary-assisted patency and secondary patency rates were calculated.
Results
This study included 120 cases. The mean age of the participants in the study group was 66.18 ± 4.63 years (range: 56–78). The BMI of group A was significantly greater than that of group B (23.13 ± 1.36 for group A and 21.51 ± 1.38 for group B, p = 0.001) (Table 1). The rate of TASC D classification in group B was significantly greater than that in group A (p = 0.001; p < 0.01). The operation time of group B was significantly greater than that of group A (mean of 56 min for group A and 210 min for group B, p = 0.001). Moreover, the hospital stay of group B was significantly longer than that of group A (mean of 1 day for group A and 7 days for group B, p = 0.001).
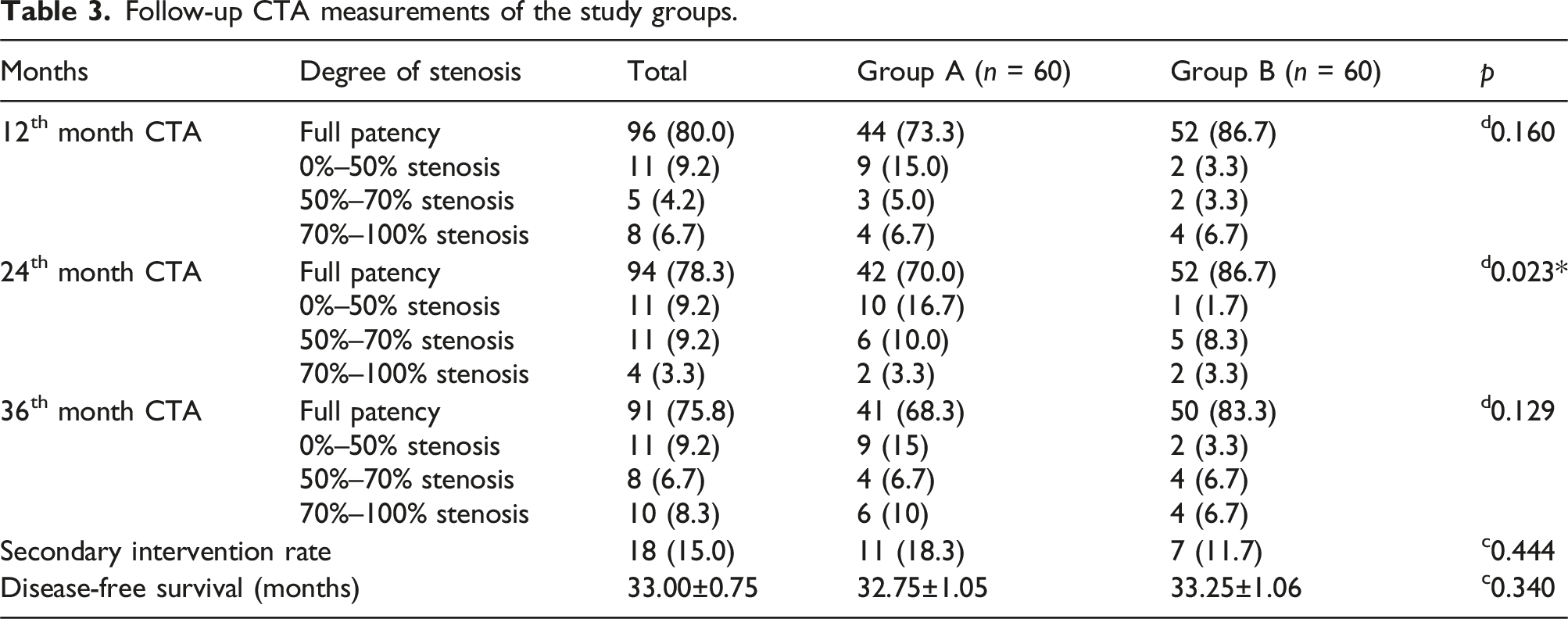
For the follow-up CT angiography measurements, a significant difference was observed between the groups at the 24th month of follow-up (p = 0.023; p < 0.05). The rate of full patency in patients in group B was significantly greater than that in group A (p = 0.027; p < 0.05). Additionally, the rate of 0%–50% stenosis in patients in group B was significantly lower than that in patients in group A (p = 0.023; p < 0.05). Other comparisons, such as those for CT angiography measurements, were not significant (p > 0.05 for all comparisons). Eleven (n = 11, 18.3%) out of sixty subjects in group A and seven (11.7%) out of sixty subjects in group B underwent secondary interventions (p = 0.444). The calculated primary patency, primary-assisted patency and secondary patency rates at 36 months were 68.3%, 21.7% and 10% for group A and 83.3%, 11% and 6.7% for group B, respectively.
Conclusion
The use of KS and AFB procedures in subjects with bilateral common iliac artery occlusion has comparable long-term patency rates.
Introduction
Aortoiliac occlusive disease (AIOD) is an advanced type of peripheral artery disease, and the treatment for this disease is more complex and debated compared to other treatments for artery disease. 1 The exact prevalence of AIOD is unknown, but it is thought that 3%–10% of the population is affected by AIOD, with its prevalence increasing with age.2,3
The conventional treatment for AIOD is aortobifemoral bypass (AFB), which is a well-established and reported procedure. AFB bypass provides long-term satisfactory results; however, it has the potential to increase morbidity and mortality. Endovascular treatment has been favoured in recent years and demonstrates comparable outcomes with AFB. 4 Endovascular treatment demonstrates low morbidity and mortality and was initially offered for high-risk patients. 5 Indications for its use have expanded over time; however, long-term patency may still be questionable.6–8 For AFB, the 5- and 10-year patency rates have been reported to be between 80% and 95% and between 74% and 86%, respectively. 2
The 2007 TASC consensus stated that endovascular treatment should be an option only in high-risk cases with respect to open surgery. The consensus also acknowledged that TASC D lesions should be primarily treated with open surgery and that endovascular treatment should not be used as a primary treatment. However, the 2017 ESC/EVS guidelines highlighted the notion that endovascular treatment may be considered for TASC D and C lesions if it is performed by an experienced team and if endovascular treatment does not compromise the later treatment options. 9
Endovascular treatment involves different techniques, including stenting techniques. With the development of stent technology, kissing stents have begun to be used for more complex lesions. The kissing stent technique has been used to simultaneously describe the bilateral iliac stents. In 1991, Palmaz et al. were the first authors to report the use of kissing stents in seven subjects.10,11 The technique gained more attention after 2010. 3 A previous review including 1390 subjects from 21 studies indicated favourable midterm results, as the 1-, 2- and 5-year primary patency rates were reported to be 89.3%, 78.6% and 69.0%, respectively. 3 However, a comparison of techniques in balanced groups is needed to determine the better option for treating AIOD. 12
The present study compared the use of AFP and endovascular kissing stents in patients with bilateral common iliac artery occlusion and reported the 3-year patency rates.
Materials and methods
This was a single-centre retrospective study. The study was performed at the Department of Cardiovascular Surgery of Bakirkoy Dr. Sadi Konuk Training and Research Hospital. Ethical approval for the study was obtained from the same hospitals’ ethical review board.
Subjects who underwent treatment for bilateral TASC II C and D common iliac artery occlusion between August 2013 and August 2021 with at least 3 years of follow-up and patients in whom we used an 8 mm graft or an 8 mm stent in the iliac artery were included in the study. Subjects with TASC II A and B lesions, those who underwent single-sided treatment, those who had aneurysms and dissections associated with the abdominal aorta and iliac artery, those who underwent bilateral common iliac artery stenting without kissing formation, those with previous abdominal aorta/iliac surgeries, those who had a history of endovascular treatment, those with active malignancies and those who were lost to follow-up were excluded from the study.
The study group was divided into kissing stent (group A) and ABF (group B) groups. The subjects’ demographic data (including age, sex, body mass index (BMI), smoking history, comorbid diseases and medications), TransAtlantic Inter-Society Consensus (TASC) II classifications and Rutherford classifications were noted. The preoperative diagnostic data included ankle–brachial index (ABI) measurements and computed tomography (CT) angiography assessments of the aorta and iliac–femoral axis.
The indications for surgery included critical limb ischaemia (CLI) or severe lifestyle-limiting intermittent claudication despite conservative treatment. Intraoperative data, early postoperative data (including data on operative times and complications) and hospital stay data were also recorded.
Procedures
All of the procedures were performed by the endovascular intervention team of the Department of Cardiovascular Surgery of Bakirkoy Dr. Sadi Konuk Training and Research Hospital.
Kissing stent procedure
Subjects who underwent stent placement were administered a 300 mg clopidogrel loading dose immediately before the procedure. Under local anaesthesia, a sheath was placed into both femoral arteries via the Seldinger technique. 70–100 IU/kg IV heparin was then administered. Contrast material was subsequently administered, and arteriography was performed. Occlusion was observed in both of the main iliac arteries. The lesions were crossed via a guide wire, and support catheter simultaneous kissing stent implantation was performed in both of the main iliac arteries via a balloon expandable stent. Complete patency was evaluated via control arteriography. The sheaths were removed, and the procedure was terminated.
Special considerations
A bare metal stent (BMS) was applied to all of the stent subjects. Covered stents were used in two subjects due to iliac rupture (Advanta V12, Atrium Maquet Getinge Group, Hudson, NH, USA). In cases in which more than one stent was required in the same iliac segment, stents were placed with an overlap of at least 10 mm.
Aortobifemoral bypass procedure
The procedure was performed under general anaesthesia. The right and left common femoral artery (CFA), superficial femoral artery (SFA) and proximal femoral artery (PFA) were explored with bilateral femoral incisions and turned separately with tapes. Afterwards, subumbilical and supraumbilical median incisions were made, laparotomy was performed to open the retroperitoneum and the abdominal aorta was explored at the infrarenal level. Tunnels were created in both femoral incisions and in the retroperitoneal area. The right and left legs of a 16 × 8 mm Dacron Y graft (JOTEC®FlowNitBioseal®Knitted Polyester Vascular Graft) were pulled through this tunnel into both femoral regions. After 1 mL of IV heparin was administered, clamps were placed in the abdominal aorta, and aortotomy was performed. Proximal anastomosis of the graft was completed. Clamps were subsequently placed in the left and right CFA, SFA and PFA, and arteriotomy was performed in both CFAs. Distal anastomoses of the graft were completed in both CFAs. After the clamps were removed, pulses were detected in the bilateral SFA and PFA. Bleeding control was then performed, and the retroperitoneum was closed over the graft. A silicone drain was placed in the abdomen, and haemovac drains were placed in both femoral regions. The layers were subsequently closed in the anatomical plane. The procedure was completed without any complications being observed.
Postprocedure care
Subjects who underwent ABF were administered heparin (1 mg/kg/h IV infusion under ACT control) on the first postoperative day. All of the subjects received flurbiprofen 100 mg twice per day for 10 days after the procedure. A proton pump inhibitor (lansoprazole 30 mg) was also provided to subjects with gastric problems. Acetylsalicylic acid (ASA) 100 mg and clopidogrel 75 mg per day dual therapy were provided for 1 year after the procedure to all of the study subjects. In both groups, statin therapy was started, and LDL levels below 100 mg/dl were targeted for therapy.
Follow-up
Subjects were evaluated at the 1st, 3rd, 6th, 12th, 24th and 36th months after the procedure at outpatient visits. For each follow-up clinical examination, the Rutherford classification, ABI measurement and CT angiography assessment of the aorta and iliac–femoral axis were noted. All of the subjects were administered dual antiplatelet therapy (aspirin–clopidogrel) and statin therapy for the first year. In subjects who did not exhibit stenosis after 1 year, clopidogrel was discontinued, and ASA was continued alone. Subjects with ischaemia findings during these visits were evaluated with BTA without delay for the first year. Surgical thrombectomy was performed for subjects in the ABF group with 70%–100% stenosis on the BTA; additionally, PTA was performed again for subjects in the kissing stent group, and these subjects were continuously monitored with dual antiplatelet therapy. The same procedure was administered to patients who again exhibited 70%–100% stenosis during their follow-up. In addition, in patients with 0%–50% or 50%–70% stenosis on BTA, maximum medical treatment (involving aspirin, clopidogrel, cilostazol, pentoxifylline and statin administration) was applied in addition to the continuation of dual antiplatelet therapy.
The primary patency (a patent stent or graft that did not exhibit any degree of stenosis), primary-assisted patency (a patent stent or graft that exhibited stenosis between 0% and 70% and that did not require any reintervention under medical treatment) and secondary patency (a stent or graft that exhibited stenosis greater than 70% and that required surgical or endovascular reintervention) were calculated.
Statistical analysis
During the evaluation of the findings that were obtained in this study, the SPSS 27 program was used for statistical analysis. The quantitative variables are presented as the mean, standard deviation, median, 25%–75% (Q1–Q3), minimum and maximum values, and qualitative variables are presented with descriptive statistical methods such as frequencies and percentages. The Shapiro–Wilk test and box plot graphs were used to evaluate the conformity of the data to a normal distribution.
The Student’s t test was used for quantitative two-group evaluations demonstrating a normal distribution; conversely, the Mann–Whitney U test was used for evaluations of variables that were not normally distributed in the two groups. The chi-square test, Fisher’s exact test and Fisher’s–Freeman–Halton test were used to compare the qualitative data. Kaplan–Meier survival analysis was used in survival analyses for the secondary intervention, and the log rank test was used in evaluations according to the groups. The results were evaluated at the 95% confidence interval, with a significance level of p < 0.05.
Results
The study included 120 patients, 94.2% (n = 113) of whom were male and 5.8% (n = 7) of whom were female. The ages of the patients who were included in the study ranged from 56 to 78 years, and the average age was 66.18 ± 4.63 years.
Baseline characteristics of the study groups.
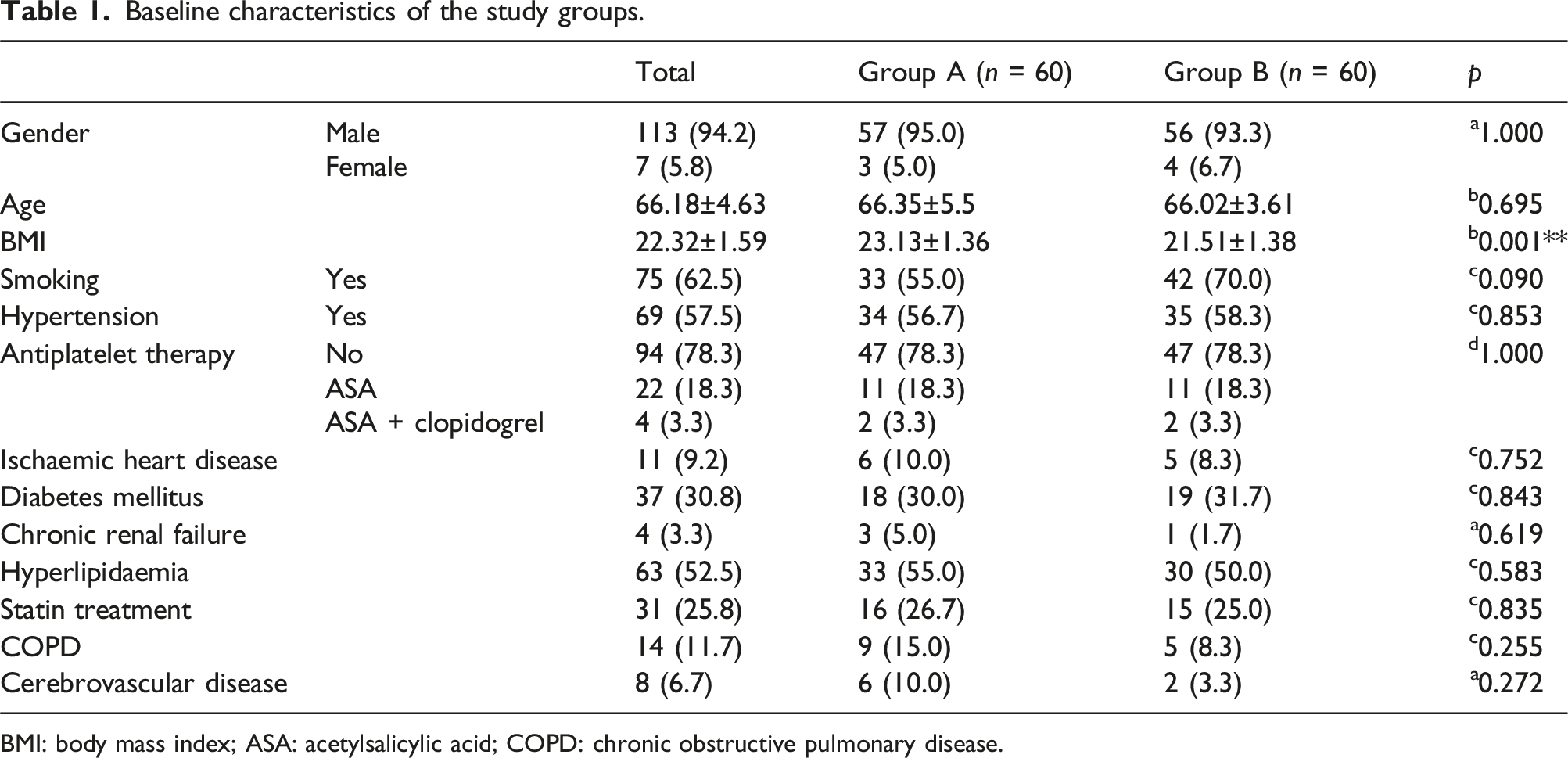
BMI: body mass index; ASA: acetylsalicylic acid; COPD: chronic obstructive pulmonary disease.
Operative and postoperative characteristics of study groups.
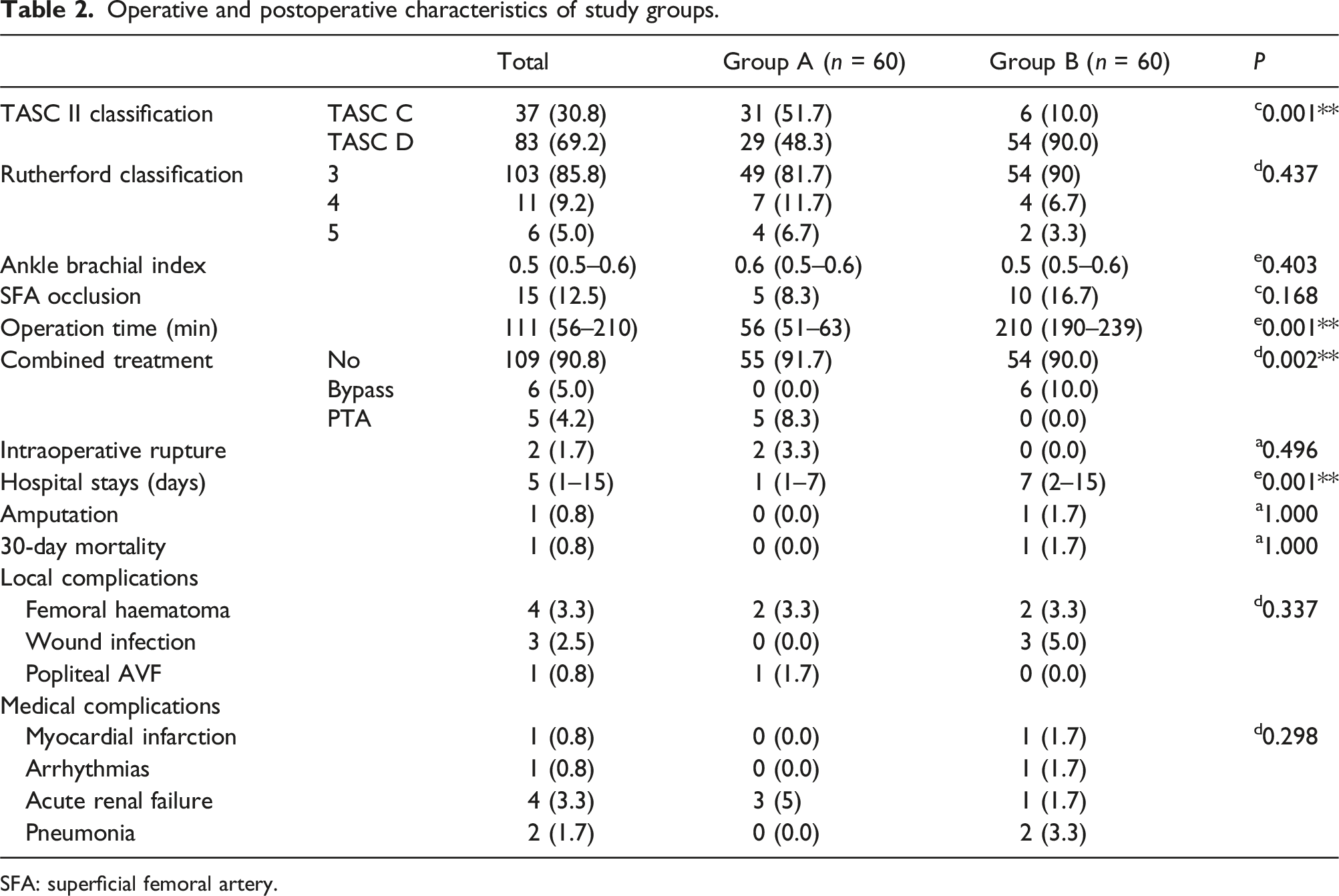
SFA: superficial femoral artery.
In group A, the right and left stent lengths (mm) were 61.12 ± 16.76 mm and 53.48 ± 18.36 mm, respectively. Additionally, the rates of vascular access for the femoral and popliteal arteries were 91.7% (n = 55) and 8.3% (n = 5), respectively. Five (8.3%) out of sixty subjects in group A and six (10%) out of sixty subjects in group B required combined treatment (percutaneous transluminal angioplasty for group A and bypass for group B). In two (3.3%) subjects in group A, an intraoperative rupture occurred.
The groups did not significantly differ in terms of local or medical complications. Additionally, the groups did not significantly differ in terms of amputation rates or 30-day mortality rates (p > 0.05 for all comparisons). The hospital stay of group B was significantly longer than that of group A (1 day (range: 1–7 days) for group A and 7 days (range: 2–15 days) for group B, p = 0.001).
Follow-up CTA measurements of the study groups.
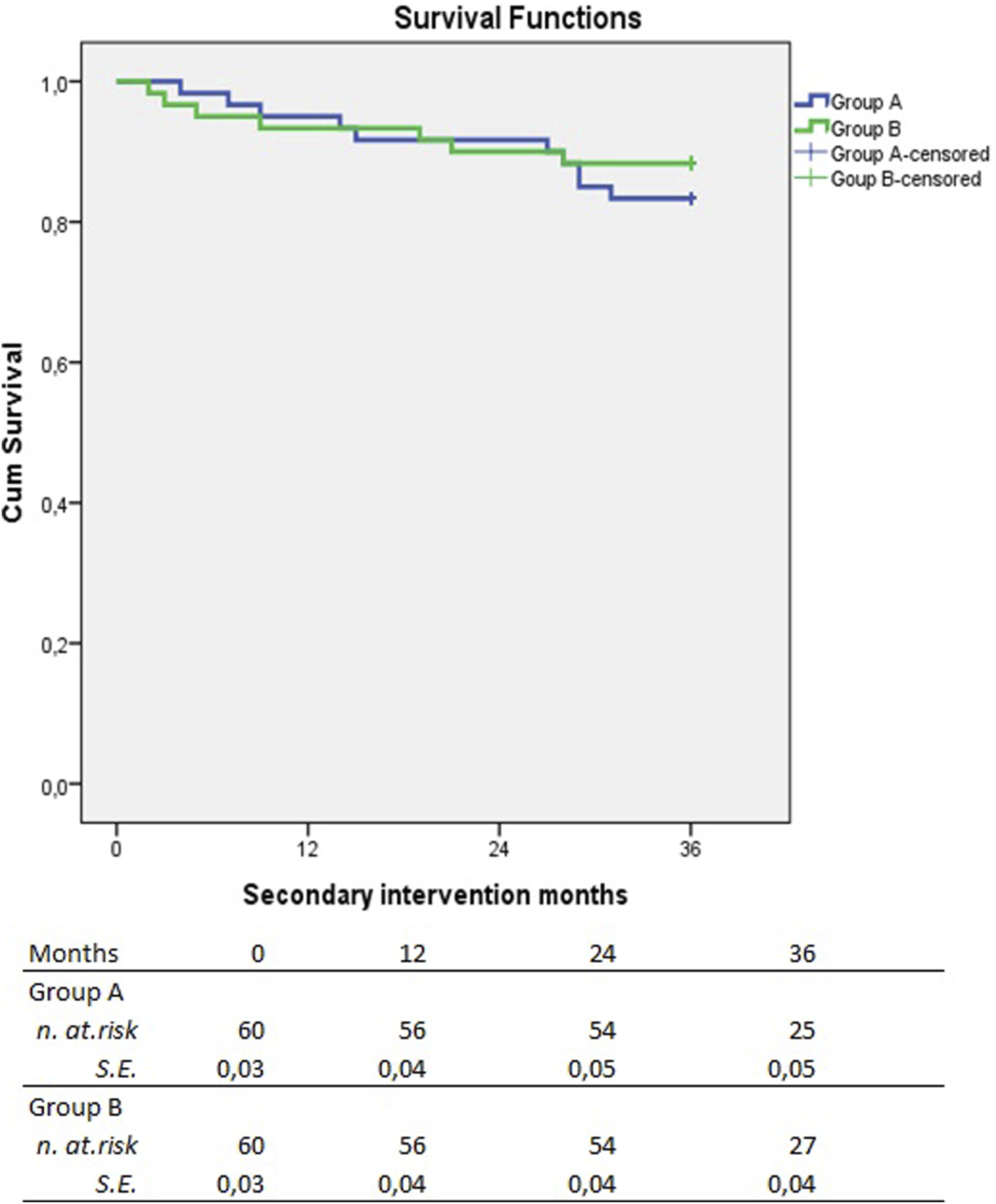
A total of 120 cases were followed up for 36 months; the follow-up results demonstrated that 102 of the cases required a single intervention (85.0%), whereas 18 required a second intervention. The mean disease-free survival time was 33.00 ± 0.75 months (Figure 1). Survival curves according to secondary intervention are presented in Figure 2. Disease-free survival of total study group. Survival curves of groups according to secondary intervention.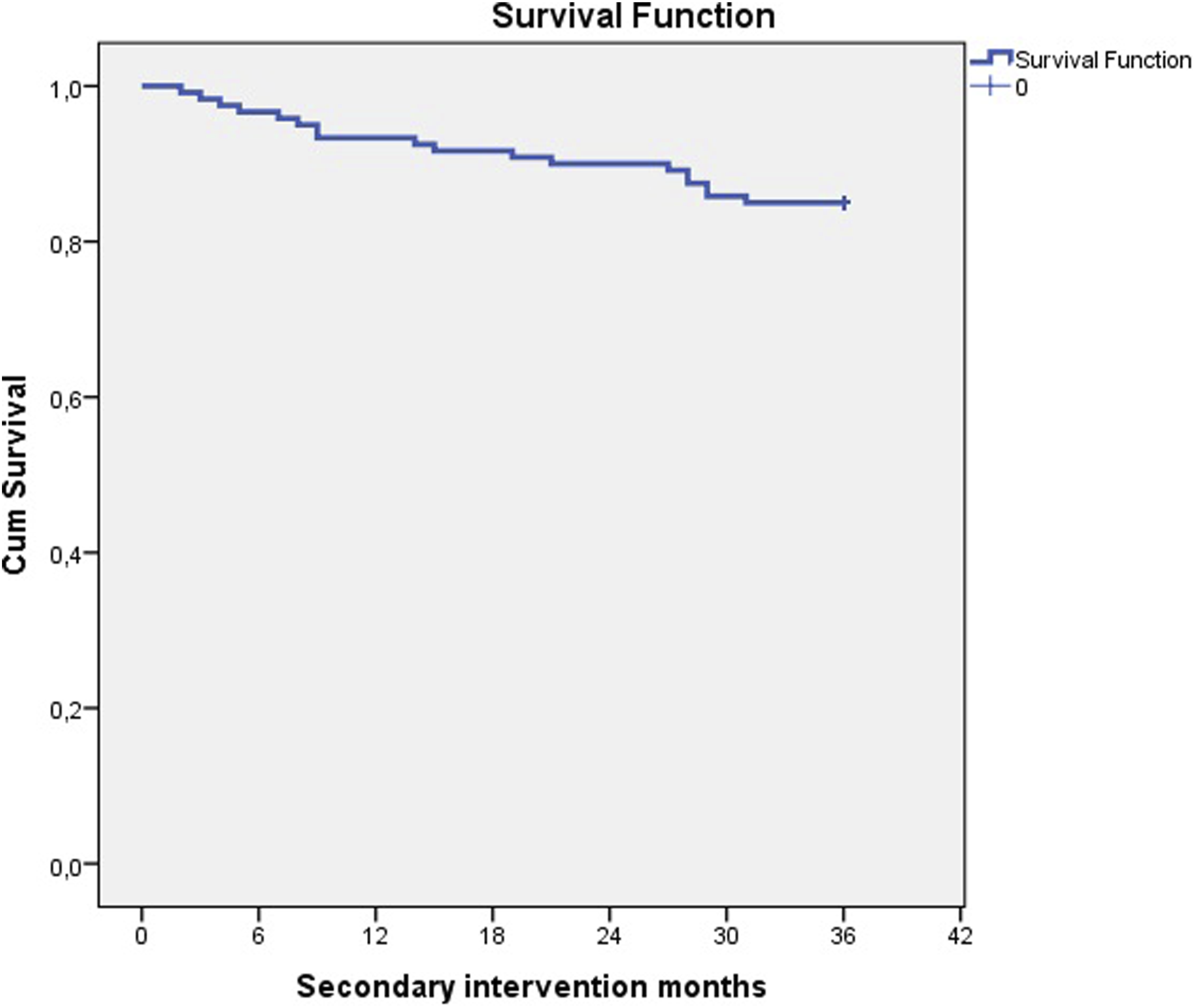
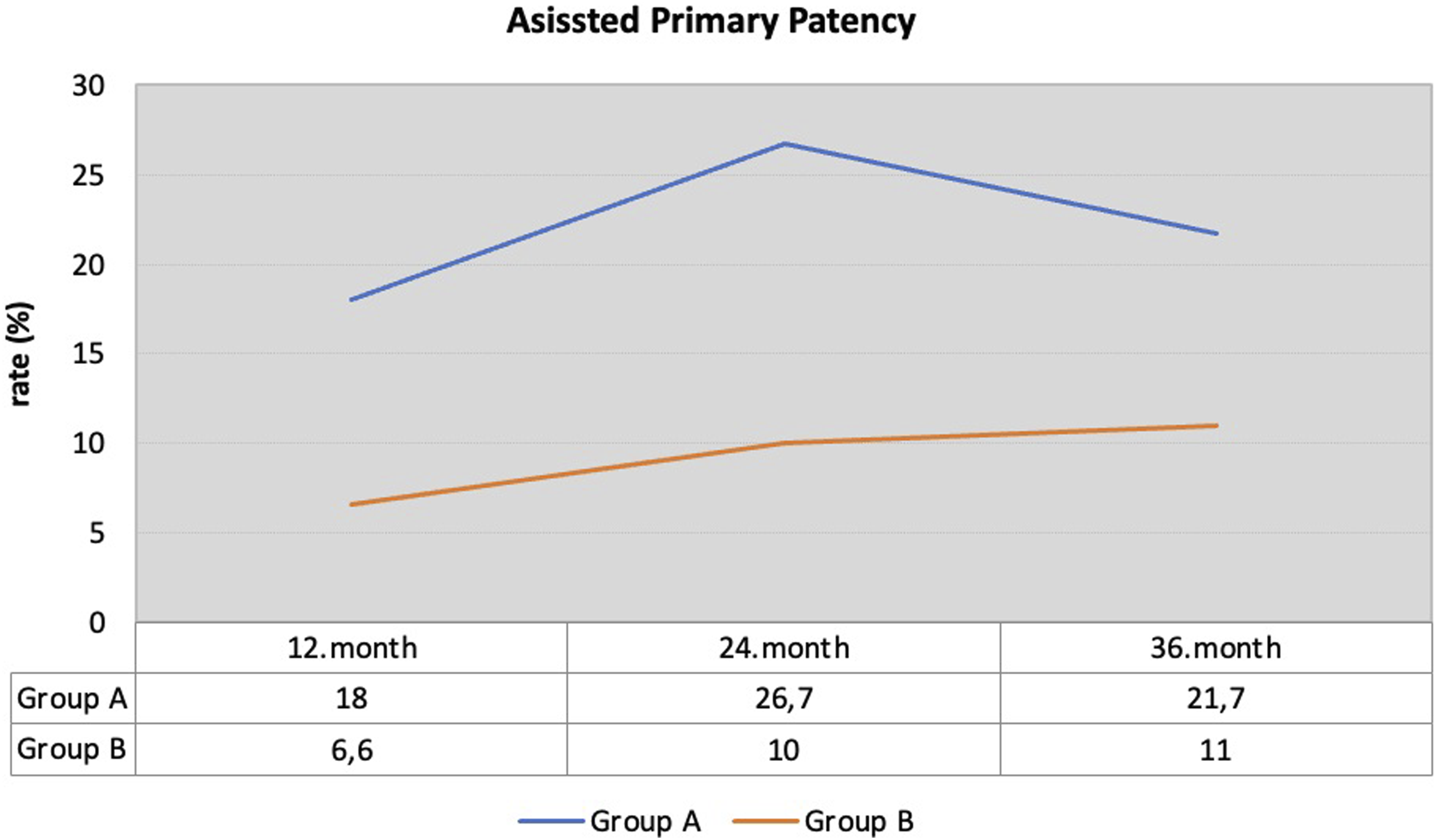
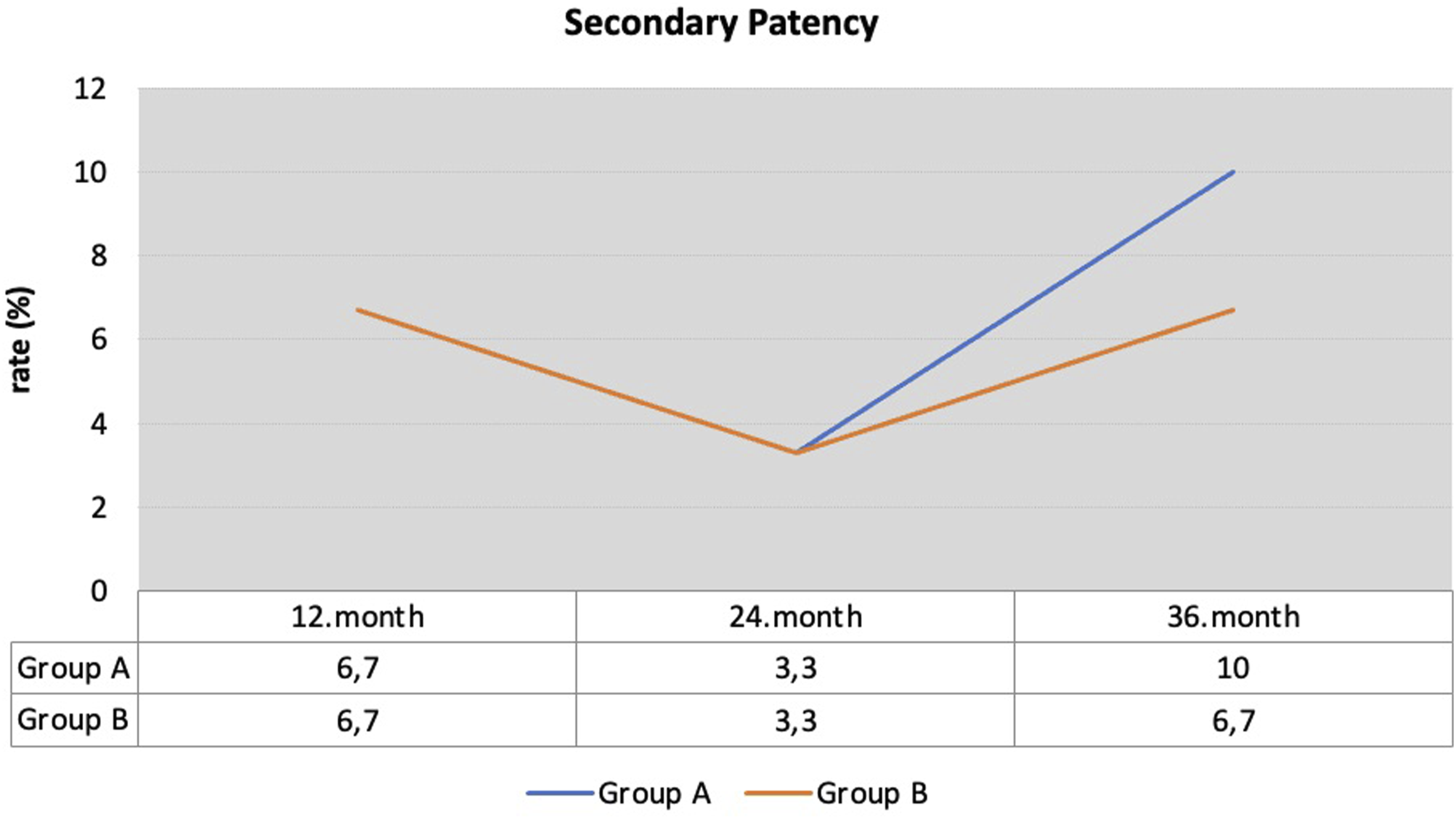
The calculated primary patency, assisted primary patency and secondary patency rates at 36 months were 68.3%, 21.7% and 10%, respectively, for group A and 83.3%, 11% and 6.7%, respectively, for group B (Figures 3–5). Primary patency at 12, 24 and 36 months follow-up. Assisted primary patency at 12, 24 and 36 months follow-up. Secondary patency at 12, 24 and 36 months follow-up.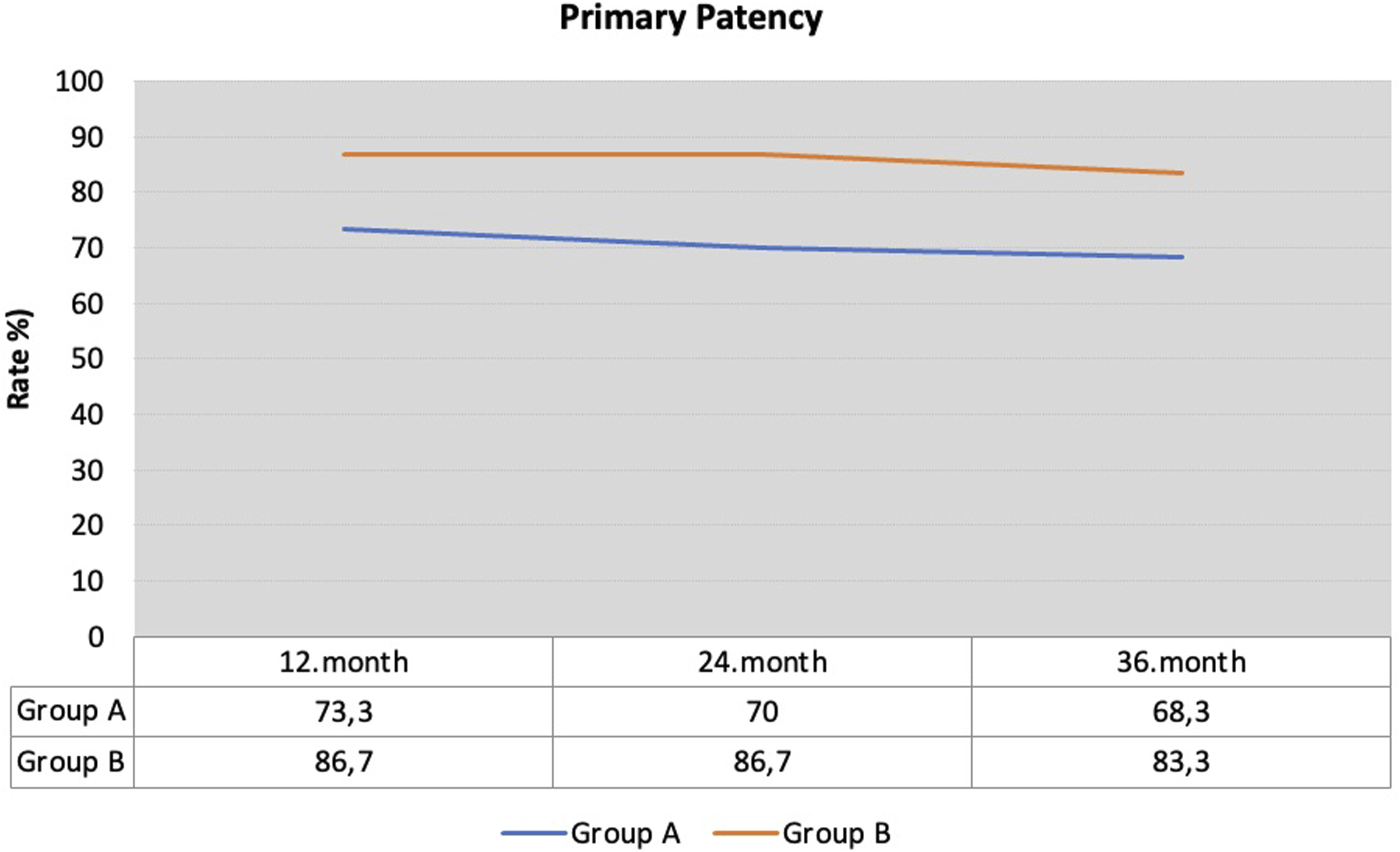
Discussion
Our study revealed that the KS procedure had comparable outcomes to AFB in terms of complications and long-term patency rates in 120 subjects who had TASC C and D lesions and similar baseline characteristics. The 36-month follow-up indicated that the patency rates were lower at the 24th month for KS; however, the 12- and 36-month patency rates were not significantly different between KS and AFB.
Many endovascular treatment options exist; however, a standard technique could not be previously described. Open AFB is regarded as being the gold standard for treating advanced AIOD. This technique provides good long-term patency with good functional outcomes. In previous TASC investigations, AFB was mainly offered for TASC C and D lesions, and TASC A and B lesions were treated with endovascular options. 10 Endovascular interventions have been offered for many years and have begun to be used for TASC C and D lesions, with comparable outcomes being observed. 13
Indes et al. 8 reviewed studies published between 1989 and 2010 and reported the results of 57 studies (29 studies on open bypass and 27 studies on endovascular treatment) for the treatment of AIOD. They concluded that open surgery increased the length of stay, risk of complications and 30-day mortality. In the present study, 30-day mortality and overall complications were not affected by the selected technique; however, AFB increased the length of hospital stay. In the same previously mentioned meta-analysis, open surgery resulted in better primary and secondary patency rates at 1, 3 and 5 years than did endovascular intervention. Salem et al. previously reported a meta-analysis that compared standard endovascular treatments (SEVs), including KS, CERAB (covered endovascular reconstruction of the aortic bifurcation) and open surgery (OS). 10 The meta-analysis included 66 studies that reported the results of 9319 subjects. The 1-, 3- and 5-year primary patency rates of SEV and OS were reported to be 90%, 78% and 71%, respectively, for SEV and 96%, 93% and 89%, respectively, for OS. Moreover, the 1-, 3- and 5-year secondary patency rates of the SEV and OS were reported to be 96%, 93% and 88%, respectively, for the SEV and 97%, 97% and 95%, respectively, for the OS. In our study, although the 24-month follow-up resulted in better patency rates for ABF, the calculated primary patency, assisted primary patency and secondary patency rates at 36 months were 68.3%, 21.7% and 10%, respectively, for group A and 83.3%, 11% and 6.7%, respectively, for group B. The patency rates at 36 months were not significantly different between the groups. Notably, our definitions of assisted primary patency and secondary patency are different from those of the abovementioned studies.
Bjorses et al. reported the results of 173 subjects who were treated with KS. 14 Subjects with TASC A-D scores were included in the study. The reported primary patency, assisted primary patency and secondary patency rates at 36 months were 83%, 90% and 95%, respectively. The authors noted that patency rates were not affected by the TASC classification of the subjects. In a meta-analysis, GrootJebbing et al. from twenty-one studies presented 1390 patients. In this meta-analysis, 48.4% of the lesions were TASC-D lesions. Although long-term results could not be reported, the incidence rates at 1, 2 and 5 years were reported as 89.3%, 78.6% and 69.0%, respectively. 3
Our study investigated the results of the compared techniques only for TASC C and D lesions. This may have affected the patency rates that were observed in our study. This advanced stage of AIOD exhibits specific treatment challenges. 15 Subjects with TASC C and D lesions tend to exhibit more calcific and long lesions. In addition, these patients have the potential to demonstrate comorbid diseases, which may complicate the performance of open surgery. In our study, subjects with TASC D lesions were treated with open surgery at a significantly higher rate, and subjects with TASC C lesions were treated with KS at a significantly higher rate. This scenario may lead to an unbalanced group.
In comparative studies, different results have been reported. Lee et al. reported 46 subjects treated for AIOD (24 subjects treated with KS and 22 subjects treated with open surgical bypass). The results indicated that KS is more advantageous than open surgical bypass in terms of operation time, hospital stay and patency rates. 1 The 5-year primary, assisted primary and secondary patency were reported as 95.8%, 95.8% and 100.0%, respectively (compared with rates of 77.3%, 77.3% and 95.5% for open surgical bypass, respectively).
Dorigo et al. reported 210 subjects treated for AIOD (128 subjects treated with KS and 82 subjects treated with AFB). With a mean 38-month follow-up, the authors reported similar early and late results for both techniques. 4 In a more recent report, Colacchio et al. demonstrated that KS patients had a higher readmission rate in the first 36 months. The time to readmission for AFB was lower; however, the statistical analysis of readmission rates revealed that the readmission interval did not reach a statistically significant level. 16 Colacchio et al. also compared the costs of open aortobifemoral bypass and kissing stenting and reported similar costs between the techniques. 6
This study presents single-centre data with a retrospective design. The cost analysis related to the device cost and hospital stay, among other factors, could not be performed and presented. The choice between the kissing stent and aortobifemoral bypass was made according to the surgical team’s preference. Other endovascular treatments, such as CERAB, were not investigated and compared in the present study.
Conclusion
Endovascular KS and AFB procedures in subjects with bilateral common iliac artery occlusion have comparable long-term patency rates.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.