
Abstract
Background
Chronic limb-threatening ischemia (CLTI), a severe form of peripheral artery disease (PAD), results in significant morbidity and mortality. The Global Limb Anatomic Staging System (GLASS) is a new tool designed to predict outcomes in CLTI patients undergoing endovascular treatments, yet its relationship with short-term outcomes requires further investigation.
Objective
This study evaluates the correlation between GLASS staging and short-term outcomes in CLTI patients treated with endovascular procedures for infrainguinal lesions.
Methods
Prospective cohort of 160 CLTI patients who received endovascular treatment for infrainguinal lesions was analyzed. GLASS staging was assigned based on angiographic data, and short-term outcomes, including immediate technical failure (ITF), limb-based patency (LBP) at 1 year, and amputation-free survival (AFS) at 1 year, were measured.
Results
In the cohort of patients, a significant association was found between GLASS staging and short-term outcomes. Higher GLASS stages correlated with increased ITF rates, lower 1-year LBP rates, and reduced 1-year AFS rates. Specific GLASS parameters, such as femoropopliteal and infrapopliteal scores, independently predicted short-term outcomes.
Conclusion
This study indicates that GLASS staging is a useful prognostic tool for assessing short-term outcomes in CLTI patients undergoing endovascular treatment for infrainguinal lesions. Utilizing GLASS staging in clinical settings may enhance treatment planning and patient prognoses.
Keywords
Introduction
Chronic limb-threatening ischemia (CLTI) represents a special disease condition of an advanced stage of peripheral artery disease (PAD), characterized by significant morbidity, mortality, and substantial liability of limb loss. 1 In CLTI patients, open surgical or endovascular revascularization is the corner stone treatment to prevent limb loss. 2
The growing faith in the endovascular therapy (EVT) for treating patients with CLTI has raised the need to identify predictors of procedural outcomes. The Global Vascular Guidelines (GVG) have introduced the Global Limb Anatomic Staging System (GLASS), 3 an angiographic scoring system that offers a comprehensive evaluation of complex anatomical patterns of PAD, rather than focusing on locations and severity of individual arterial lesions or segments, as seen in other anatomical classification systems 4 GLASS takes into account the complexity of disease along the anticipated target arterial path (TAP) that provides in-line flow to the foot, by individually grading femoropopliteal (FP) and infrapopliteal (IP) arterial segments on a scale from 0 to 4 according to the length of the steno-occlusive disease. A consensus-based matrix merges these segmental grades into three overall GLASS stages (I–III), which correlates to technical complexity.
The purpose of GLASS is to improve the understanding of the expected immediate outcomes and durability of infrainguinal EVT of CLTI patients by correlating disease complexity to the anticipated technical success and 1-year limb-based patency (LBP). However, as a relatively new scoring system, GLASS has not yet been fully integrated into standard clinical practice, resulting in limited data on its accuracy and clinical utility Consequently, the aim of the present study is to assess the relationship between various GLASS stages and the short- and mid-term outcomes of EVT of CLTI patients with infrainguinal arterial lesions.
Patients and methods
Study population
This non-randomized prospective study was conducted at the Department of Vascular and Endovascular Surgery in a tertiary referral university hospital between October 2021 and September 2023. All patients provided informed written consent, and the study was reviewed and approved by the ethical committee of the faculty of medicine at Assiut university. (ethics approval reference/number 17101851).
The study included all consecutive CLTI patients (Rutherford classes 4–6) due to infrainguinal atherosclerotic disease who underwent EVT of FP steno-occlusive arterial lesions with or without IP interventions during the study period. The study excluded patients with aortoiliac or common femoral arterial disease, acute limb ischemia, previous infrainguinal revascularization procedures, non-atherosclerotic arterial disease (such as vasculitis, Buerger’s disease, and connective tissue disease), and patients with contraindication to contrast agents.
Patient evaluation
All patients underwent full history taking and clinical evaluation including ankle-brachial index (ABI) measurement. Preoperative multidetector computed tomography angiography (CTA) was performed on all patients to outline the anatomical characteristics of the arterial disease and to identify the preferred TAP for GLASS grading and staging. TAP is typically identified as the least diseased IP artery providing in-line flow from the origin of the superficial femoral artery (SFA) to the malleoli while considering angiosome-guided revascularization in patients with foot wounds when suitable TAP is available. GLASS modifier for inframalleolar (IM) disease was not used in this study. Severe arterial calcification of the TAP, defined as calcification of >50% of arterial circumference and/or presence of bulky plaques, increased GLASS grading by one point. Calcification was also assessed using the peripheral artery calcium scoring system (PACSS). 4 All patients adhered to the best medical therapy protocol, and received dual antiplatelet therapy before the procedure.
Procedure description
Ipsilateral access through the common femoral artery (CFA) was the typical access site. Contralateral femoral access was used in case of hostile groin, morbid obesity, or with ipsilateral CFA or proximal SFA arterial lesions. After sheath insertion, a bolus of 5000 IU of unfractionated heparin (UFH) was administered intra-arterially. Diagnostic angiogram was then performed to confirm the choice of TAP as well as FP and IP GLASS grading and staging.
Crossing of the lesion was done by using a combination of different guide wires and support catheters. Once the lesion was crossed, balloon angioplasty was done using an adequately sized balloon catheters, followed by a diagnostic angiogram to ensure patency of TAP from groin to foot. If attempts to reenter the distal true lumen via the antegrade approach were unsuccessful or if crossing was not achieved, a retrograde approach or reversed controlled antegrade retrograde tracking (CART) techniques were used. This approach was guided by either fluoroscopy or duplex ultrasound (DUS) according to the operator’s preference. Stenting was indicated when a residual stenosis ≥30% or flow-limiting dissection was encountered. Hemostasis was achieved by manual compression.
Follow up
All patients were prescribed clopidogrel (75 mg/day) for at least 3 months postoperatively and aspirin (100 mg/day) for life. All patients underwent evaluation in the outpatient clinics every 3 months for 1 year after the procedure, including clinical examination, ABI measurement, assessment of wound healing, and DUS examination. Patients with worsening symptoms or decreased ABI were further investigated with DUS and/or CTA. Reintervention using repeat balloon angioplasty ± stenting was indicated for >50% recurrent stenosis or occlusion to achieve in-line flow with <30% residual stenosis.
Study endpoints and definitions
Immediate technical failure (ITF) was defined as the inability to cross the target lesion or failure to reestablish in-line flow through the designated TAP. LBP was defined as the absence of any of the following conditions: (1) occlusion or critical stenosis within the TAP on an imaging study, (2) reintervention impacting any part of the TAP, and/or (3) signs of hemodynamic compromise (>50% stenosis in the TAP or a decrease in the ABI of 0.15 or toe-brachial index of 0.10 accompanied by ongoing clinical symptoms of CLTI in the affected limb (e.g., rest pain, worsening, or persistent tissue loss). Major adverse limb events (MALE) included requirement of major amputation, open surgical revascularization, or thrombolysis of the treated limb.
Results
Patients’ characteristics and baseline data
Out of 350 chronic lower limb ischemia patients who underwent endovascular revascularization during the study period, 160 patients fulfilled the study criteria and were included for the present analysis. Causes and numbers of excluded patients showed in Figure 1. Causes and numbers of excluded patients. CLI, chronic lower limb ischemia; ER endovascular revascularization.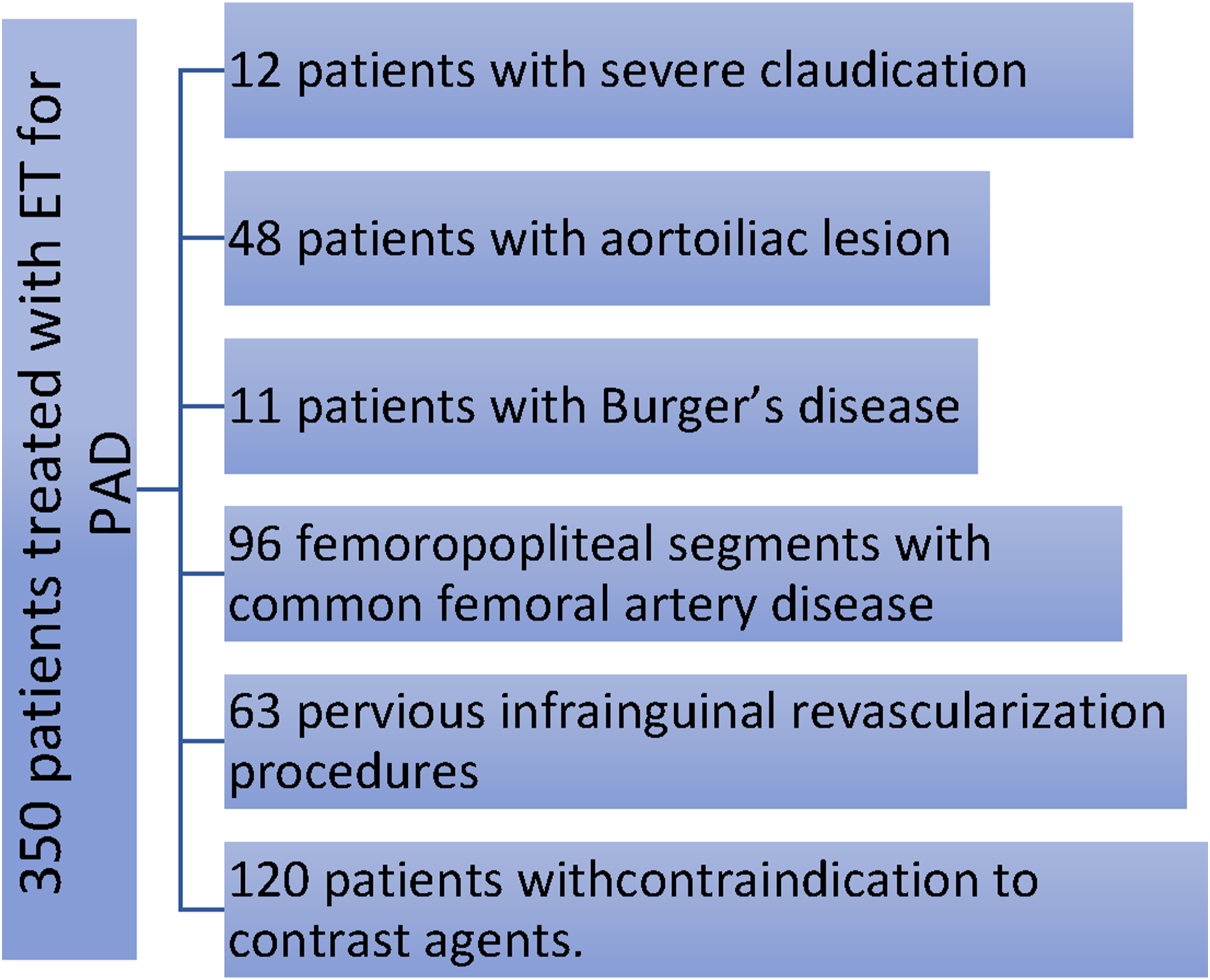
Patients’ characteristics comorbidities of the studied patients.
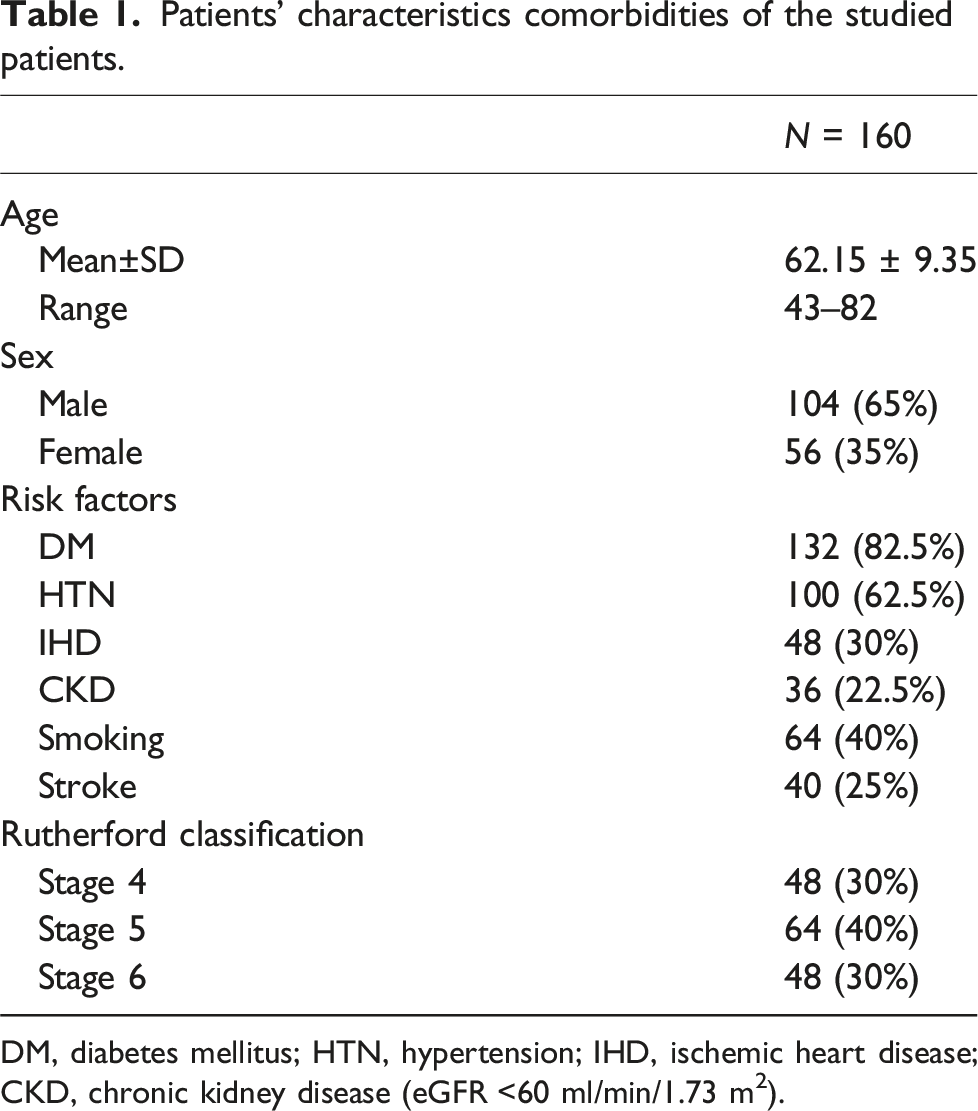
DM, diabetes mellitus; HTN, hypertension; IHD, ischemic heart disease; CKD, chronic kidney disease (eGFR <60 ml/min/1.73 m2).
Clinical and radiological evaluation
Regarding the main arterial lesion site, 84 (52.5%) patients were affected at the IP level, and 76 (47.5%) were affected at the SFA level. GLASS categorization of the FP grade showed that 24 (15%) patients were classified as grade 0, 48 (30%) as grade 1, 36 (22.5%) as grade 2, 36 (22.5%) as grade 3, and 16 (10%) as grade 4.
GLASS characteristics of the studied patients.
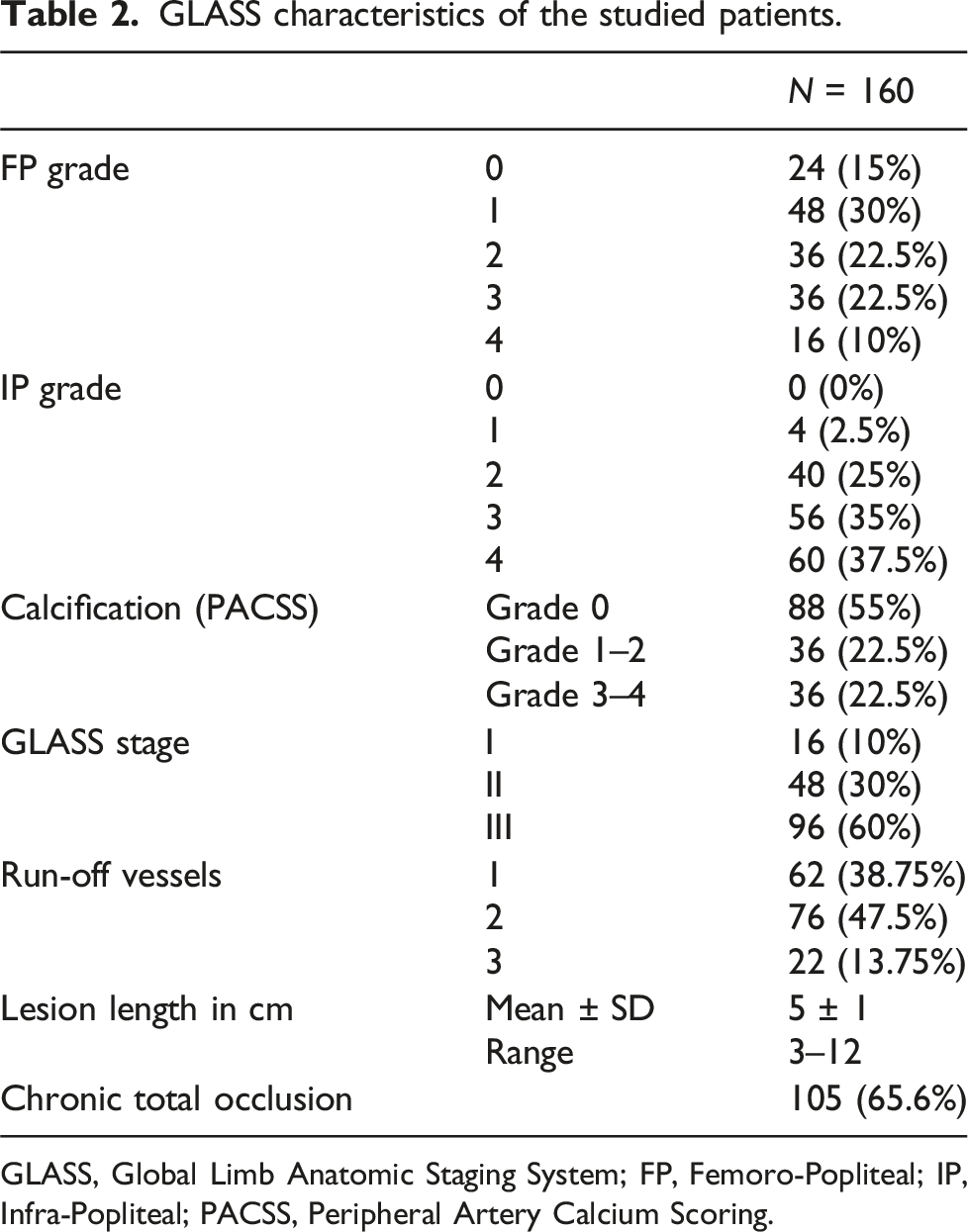
GLASS, Global Limb Anatomic Staging System; FP, Femoro-Popliteal; IP, Infra-Popliteal; PACSS, Peripheral Artery Calcium Scoring.
Procedural data and early outcomes
Technical success was achieved in 136 (85%) patients, while the remaining 24 (15%) patients had ITF due to failure to enter occlusion (8/24, 33.3%), failure to cross occlusion (10/24, 41.67%), or failure to enter the lumen distal to the occlusion (6/24, 25%).
Stratifying ITF rates by the GLASS stage showed ITF rates of 20.83%, 2.5%, and 0% for GLASS stages 3, 2, and 1, respectively, and statistically insignificant (P value 0.171).
Complications.
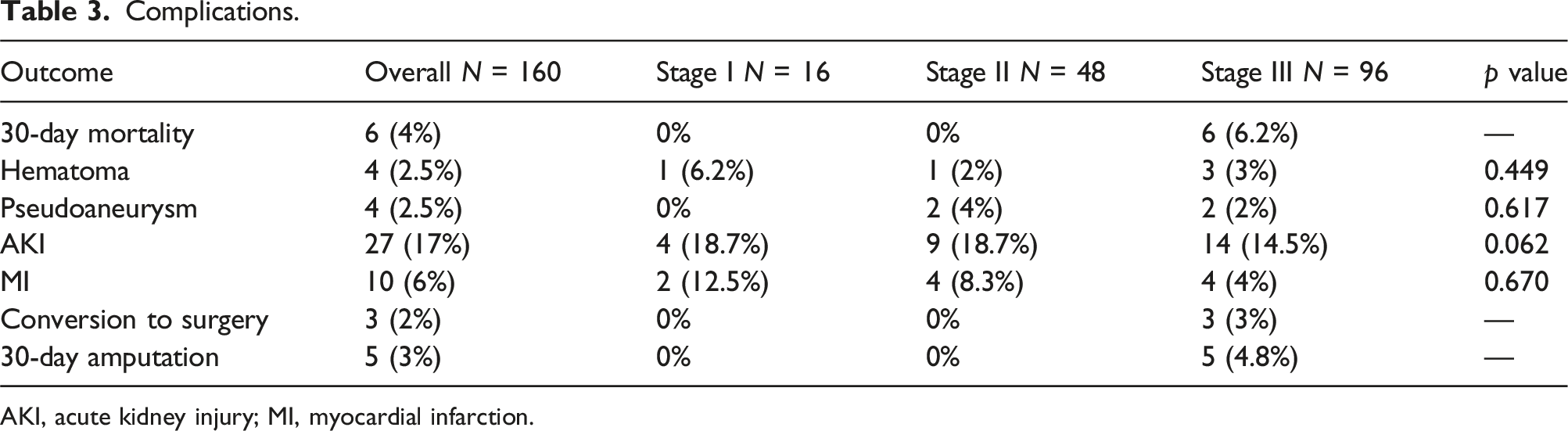
AKI, acute kidney injury; MI, myocardial infarction.
Mid-term outcomes
Regarding LBP, our analysis based on GLASS stages revealed distinct patterns. In GLASS 1, LBP was preserved in 50% of cases. For GLASS 2, LBP was preserved in 45.83% of cases. In contrast, GLASS 3 demonstrated a lower preservation rate, with LBP preserved in 27.08% of cases. LBP is shown in Figure 2. Kaplan–Meier curve for LBP regarding GLASS.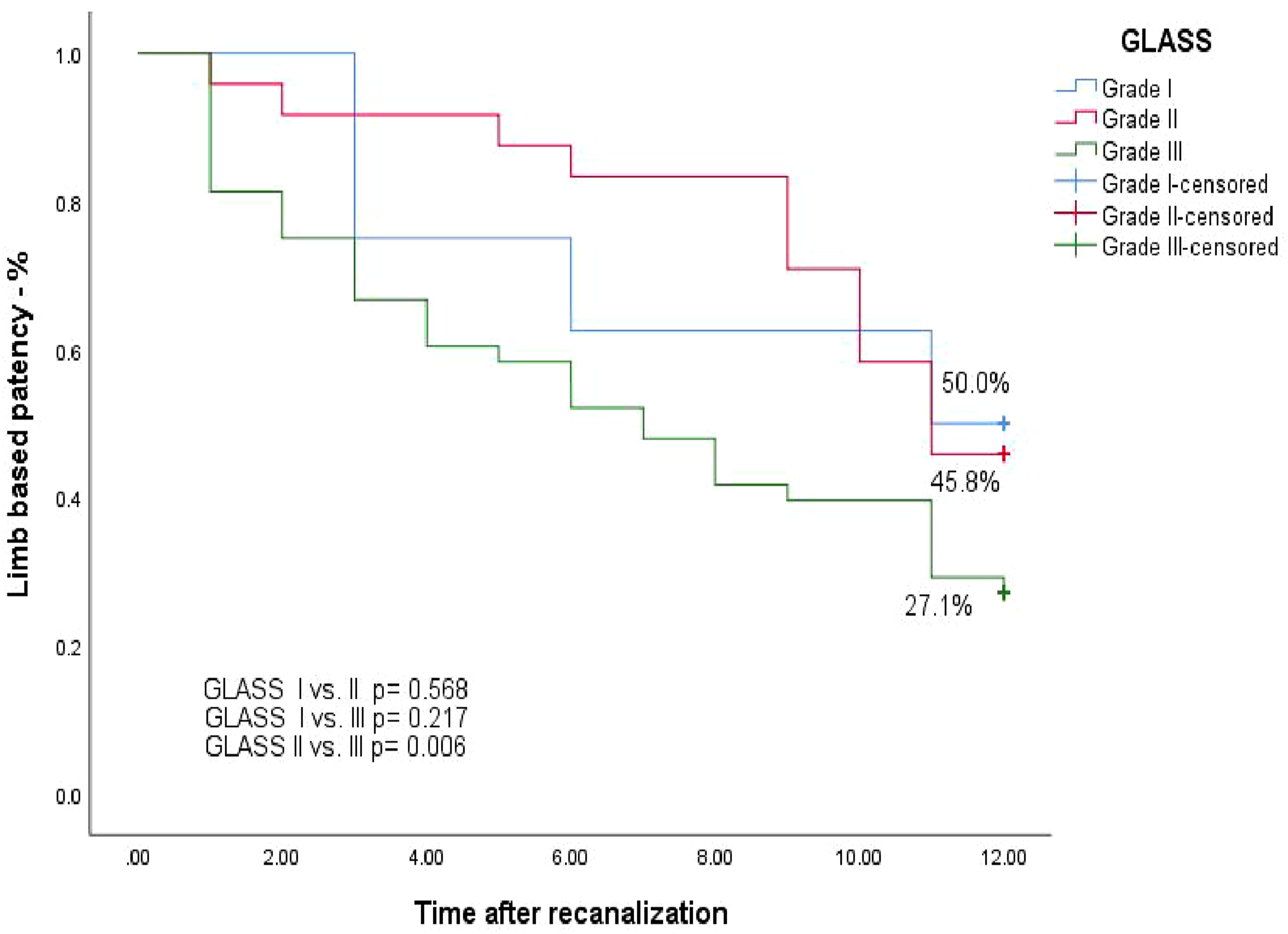
In terms of amputation rates, our analysis based on the GLASS revealed distinct patterns. GLASS 3 exhibited the highest amputation rate, constituting approximately 58.33% of cases. GLASS 2 demonstrated a lower amputation rate, representing around 29.17% of cases. In contrast, GLASS 1 exhibited the lowest amputation rate, accounting for approximately 25% of cases. AFS was demonstrated in Figure 3. Kaplan–Meier curve for Amputation-free survival (AFS) regarding GLASS.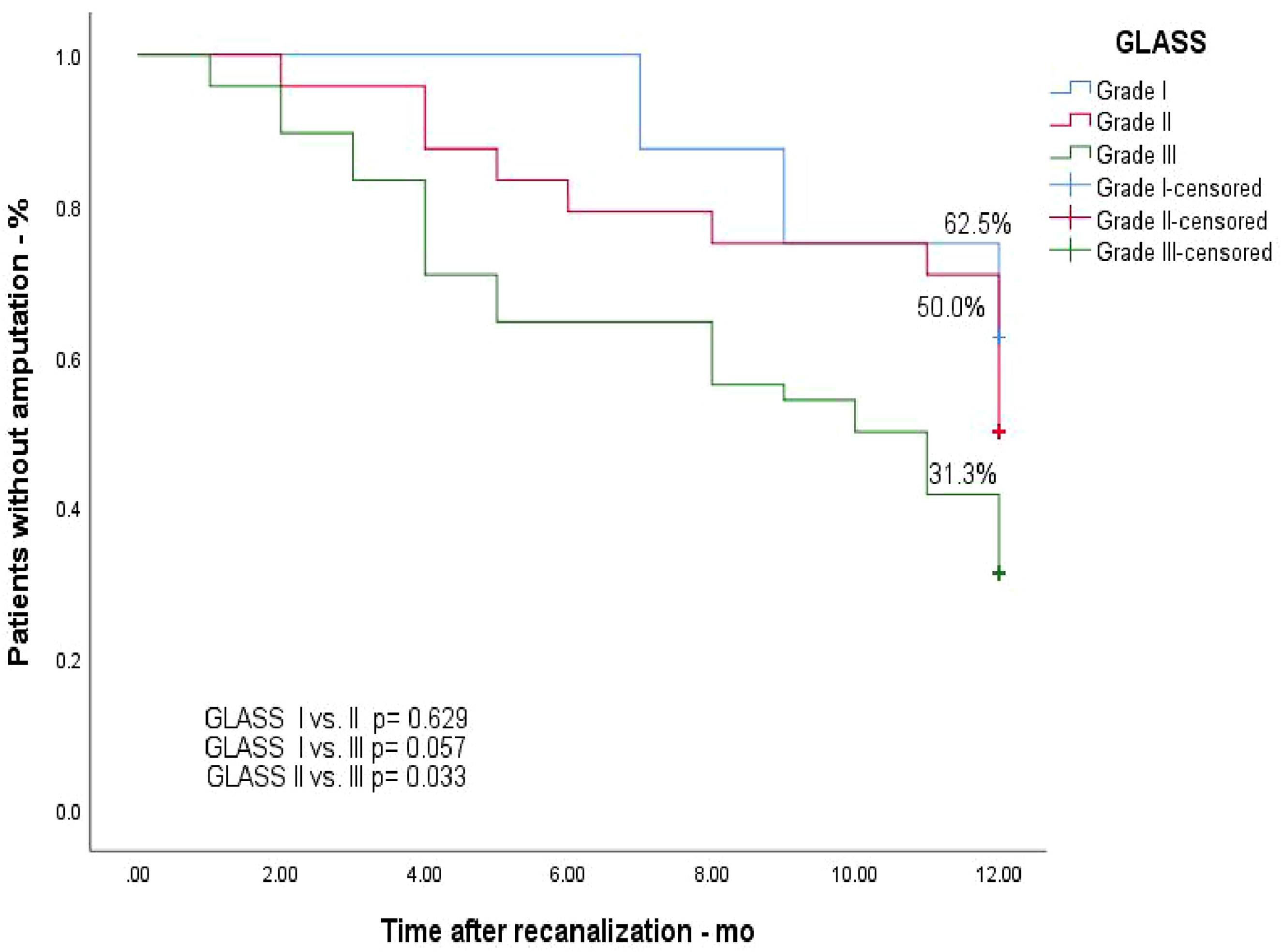
In terms of mortality rates, our analysis based on the GLASS revealed distinct patterns. GLASS 3 exhibited the highest mortality rate, constituting approximately 41.67% of cases. GLASS 2 demonstrated a lower mortality rate, representing around 16.67% of cases. In contrast, GLASS 1 exhibited the lowest mortality rate, accounting for approximately 12.5% of cases. Figure 4 shows MALE-free survival (MALE-FS) regarding GLASS. Kaplan–Meier curve for OS regarding GLASS.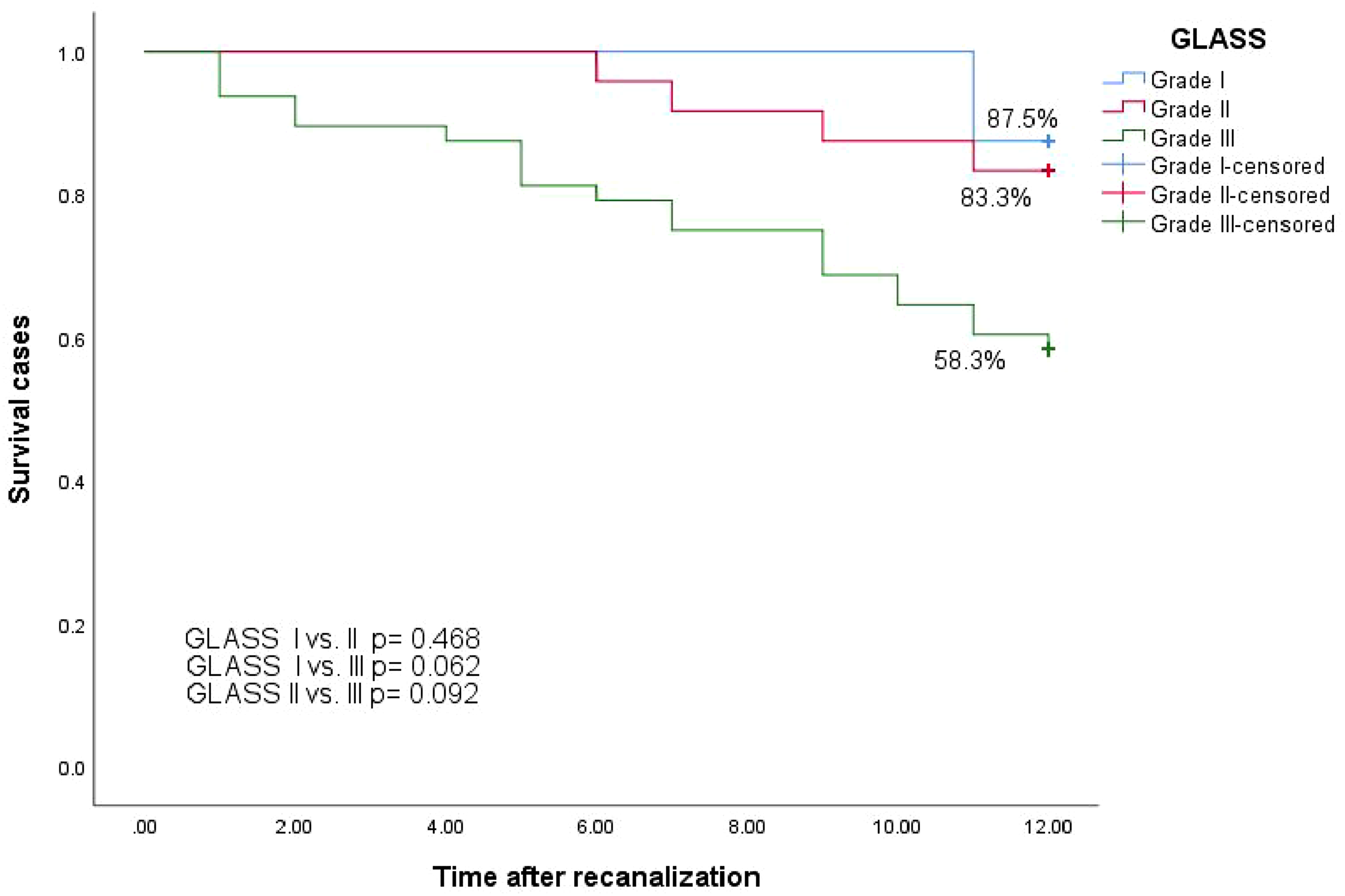
Predictors of loss of LBP and AFS.
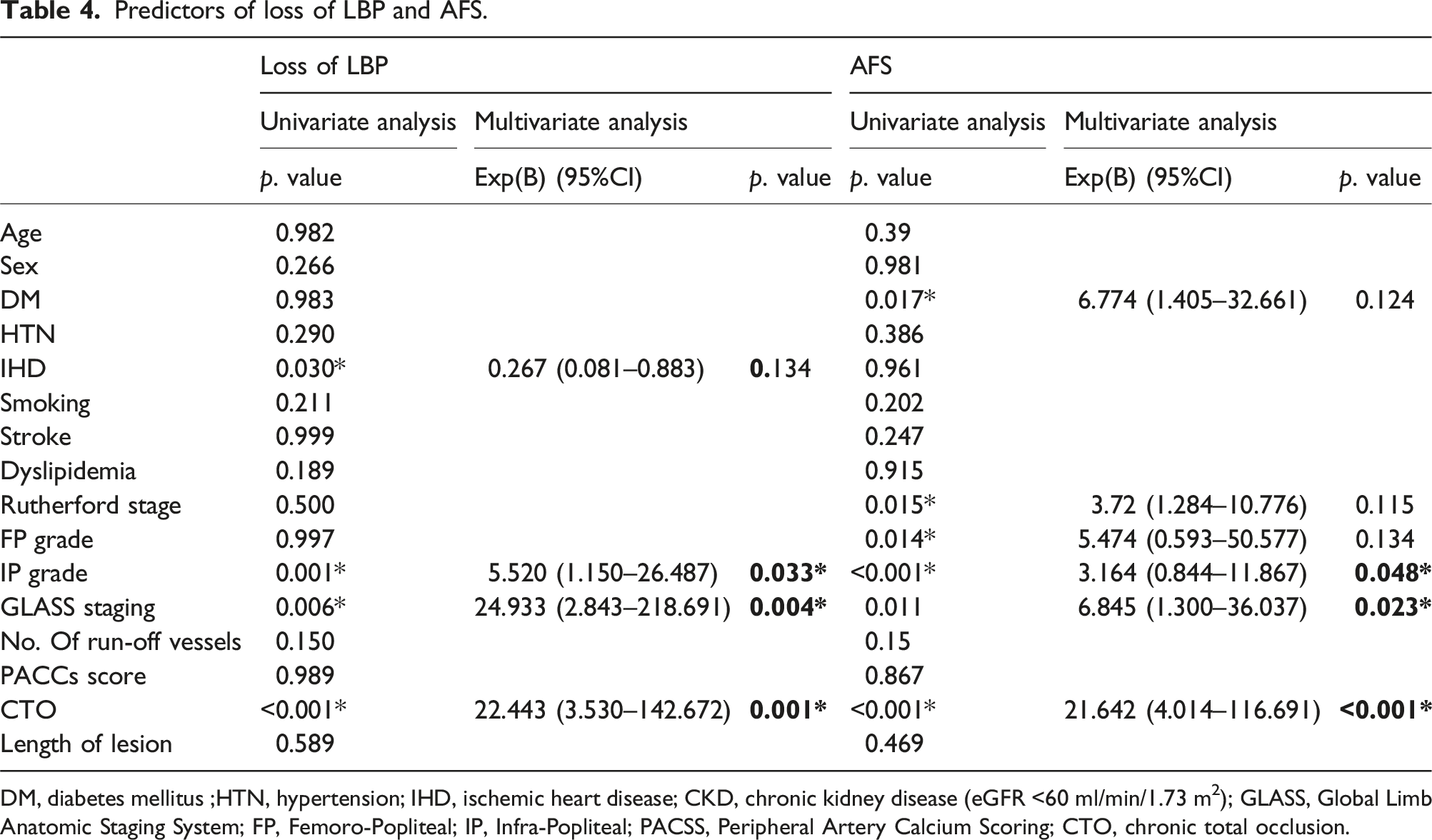
DM, diabetes mellitus ;HTN, hypertension; IHD, ischemic heart disease; CKD, chronic kidney disease (eGFR <60 ml/min/1.73 m2); GLASS, Global Limb Anatomic Staging System; FP, Femoro-Popliteal; IP, Infra-Popliteal; PACSS, Peripheral Artery Calcium Scoring; CTO, chronic total occlusion.
Discussion
The primary objective of our study was to evaluate the value of GLASS classification as a predictor for short- and mid-term outcomes following endovascular revascularization in patients diagnosed with CLTI. In the current study, GLASS stage emerged as a significant predictor of survival-related and limb-specific outcomes of EVT procedures for infrainguinal CLTI. GLASS 3 anatomy was related to both ITF and loss of LBP after EVT, with a higher incidence of major amputation and major adverse limb events (MALE). These findings underscore the importance of GLASS classification in clinical decision-making for CLTI patients eligible for revascularization. In other words, it raises the question about the eligibility of EVT for the management of CLTI patients with GLASS stage III anatomy.
While it is widely agreed that nearly all CLTI patients are candidate for revascularization in addition to optimal medical therapy, the ongoing debate about the most effective method for revascularization is continued. Specifically, the discussion revolves around whether a bypass graft—ideally using a vein from the patient’s leg (vein bypass)—is preferable, or if the best approach is through endovascular treatment, which typically involves balloon angioplasty with or without stenting and BASIL-1-reported that rate of a composite endpoint, which includes major adverse limb events or death from any cause, was significantly lower in the vein bypass group compared to the best endovascular treatment group. 5
The BASIL-2 trial reporting that CLTI patients who requiring an infrapopliteal revascularization procedure, either alone or in addition to more proximal infra-inguinal procedure to restore limb perfusion, a vein bypass-first revascularization strategy was linked to a higher risk of major amputation. Or death from any cause compared with a best endovascular treatment first revascularization strategy.5,6 These conflicting results come from that the severity and anatomical distribution of atherosclerosis influences treatment options and outcomes in chronic limb-threatening ischemia. Approximately three-quarters of participants in the BASIL-1 trial underwent a vein or prosthetic bypass, or plain balloon angioplasty, for disease affecting the femoropopliteal segment, which includes the arteries between the hip and knee. This difference in result obliged the researchers to do subgroup analysis to formulate the best treatment option for specific subgroups of patients this analysis is still deficient and needs to be evaluated by further studies. The previously available angiographic scoring systems like TASC and Bollinger did not predict clinical limb-based and patient-based outcomes. The anatomical complexity of the disease is a key factor influencing treatment choices and clinical outcomes. For all these aforementioned causes GLASS classification was developed. The core principles of the GLASS involve restoring in-line flow to the ankle and foot as the anatomical objective of revascularization in CLTI, defining TAP and LBP. 7
GLASS classification shift from a lesion-focused perspective to a limb-based evaluation enhances the clinical relevance of our findings and contributes to a more nuanced approach in managing this challenging condition. 8 The 2020 Global Vascular Guidelines seek to enhance structured decision-making in CLTI by offering a framework for evidence-based revascularization (EBR). 9
The implementation of GLASS has enabled a more efficient evaluation of complex disease patterns. A greater number of cases exhibited a combination of FP and IP grades, prompting strategic direction of endovascular Interventions to address multilevel disease. Additionally, the impact of below-the-knee run-off on outcomes following isolated FP revascularization has emphasized the necessity of a comprehensive scoring system, as achieved in GLASS.10,11 In our study, technical success was obtained in 85% of patients. 24 patients (15%) experienced ITF, including 4 patients (8.3%) in GLASS II, 20 patients (20.8%) in GLASS III. These results match with results published in Buntins, Vangelis et al., 12 The rates of immediate technical failure (ITF) for GLASS stages II, and III stand at, 7.39% and 21.07%, respectively. Notably, Kodama et al. recently documented an ITF rate of 28% for endovascular intervention (EVI) conducted on limbs with GLASS III anatomy, drawing from data originating from the BASIL (Bypass vs. Angioplasty in Severe Ischemia of the Leg) trial. This finding is consistent with the Global Vascular Guidelines, which indicate ITF rates of less than 10% for GLASS I, less than 20% for GLASS II, and more than 20% for GLASS III. 10 In our study, all patients were followed up for 12 months with a mean period of (9.8 ± 3.2) months. We observed a strong association between loss of LBP and the higher the GLASS stage. In our results LBP was 50% for GLASS I, 45.8% for GLASS II and 27.1% for GLASS III at 12 months.
These findings align with predictions outlined in the Global Guideline document, indicating that GLASS 3 disease is associated with higher ITF rates and lower LBP outcomes. This consistency strengthens the validity of our results and highlights the robust predictive capacity of GLASS staging in assessing short-term outcomes after endovascular revascularization for patients with CLTI.
Kodama et al. 13 reported that GLASS III anatomy was significantly associated with worse limb salvage outcomes (p = 0.035) in patients treated with endovascular intervention (EVI) in the BASIL-1 trial. Our Kaplan–Meier curve for limb salvage shows strong association between major amputation and Increasing GLASS stage that limb salvage was 75% for GLASS I, 70.8% for GLASS II and 41.7% for GLASS III. Rate of amputation in between different GLASS Stages (GLASS I, II vs GLASS III) was statistically insignificant and that may be due to small sample size. 12 The GLASS system addresses the gap between femoropopliteal and infrapopliteal disease classifications by assigning limb “stages” based on an algorithm that evaluates the disease burden in both segments. This study demonstrates that the GLASS multilevel combined staging system can be utilized in two key ways: first, to assess preoperatively which limbs are likely to respond well to endovascular treatment, and second, to evaluate postoperatively which limbs are at higher risk for restenosis and may require future interventions. 9
El Khoury Rim et al. study found a significant association of increasing GLASS stage and worse OS with rate of survival at 12 months were 85% and 62% for GLASS (I–II) and GLASS III, respectively, and this aligns with our results that show 87.5%, 83.3% and 58.3% for GLASS I, GLASS II, and GLASS III, respectively. 7 In the study conducted by Hata et al., it was noted that neither the GLASS femoropopliteal (FP) score nor the GLASS infrapopliteal (IP) score significantly predicted wound healing following the endovascular intervention. However, the extent of infrapopliteal calcification emerged as a significant predictor.7,14
Complex lesions, such as chronic total occlusion (CTO), are too hard to manage like conventional lesions. CTOs account for 40% of EVT for PAD, even femoropopliteal (FP) artery CTOs challenging.14,15
CTO tend to have a lower technical success rate, more intervention time, and more radiation exposure and contrast. In patients performing EVT for the FP segment, patients with GLASS stage III were associated with significantly worse AFS, and MALE-FS compared to GLASS stages I and II. 16
The relationship between anatomical patency post-intervention and subsequent clinical outcomes appears to be influenced by various factors, it was found that predictors for lost LBP were severe infrapopliteal stage with p value was 0.033 and severe GLASS stage (p value = 0.004), and finally CTO (p value = 0.001) while the predictors of major amputation were the severe IP grade with (p value = 0.048), GLASS stage (p value = 0.0023), and lastly CTO with (p value <0.001). In light of the aforementioned evidence, EVT is not considered the treatment of choice in GLASS III anatomy especially with high IP or long CTO grade and surgery must be evaluated as an alternative for the management of those people.
This study has certain limitations, as it is a single-center investigation with a relatively small cohort and a follow-up period of only 12 months. Additionally the lack of subgroup analysis of the FP domain and IP domain due to small numbers which may bias the results and lack of long-term outcomes and its correlation to the GLASS stage. Also the lack of evaluation of wound healing, GLASS inframalleolar modifier, which is strongly associated with major amputation ignored in our study. Finally, surgery did not evaluate as availed alternative to EVT which may have better result in these subsets of patients.
Conclusion
GLASS stages correlate with key factors such as Amputation-Free Survival, Overall Survival, limb-based patency, and the incidence of amputation and mortality rates. The findings emphasize the utility of GLASS staging in risk stratification and decision-making for endovascular interventions.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.