
Abstract
Objectives
Pelvic congestion syndrome (PCS), often underdiagnosed, is a cause of chronic pelvic pain in women and is frequently associated with pelvic varicose veins. Endovascular embolization is an established treatment, traditionally performed via femoral or jugular access. However, these approaches may carry higher risks of complications. This study aimed to evaluate the safety, feasibility, and clinical outcomes of using basilic vein percutaneous access for pelvic vein embolization in patients with PCS.
Methods
A retrospective cohort study was conducted on 292 women of reproductive age with symptomatic PCS who underwent pelvic varicose vein embolization using percutaneous access via the distal third of the right basilic vein. The study spanned from 2018 to 2023 and was carried out at two hospitals in Bogotá, Colombia. Inclusion criteria comprised chronic pelvic postcoital pain and Doppler-confirmed pelvic varicosities with reflux diameters >6 mm. Data collected included demographics, CEAP and Symptoms-Varices-Pathophysiology classifications, intraoperative details (access approach, duration, coil usage, complications), and postoperative outcomes (symptom resolution, complications, reintervention, ICU/hospital stay, and mortality). Follow-up evaluations were conducted at 15 days, 3 months, and 6 months post-procedure. Descriptive statistics were used for analysis. A detailed description of the surgical technique used for basilic vein access and embolization was included.
Results
All 292 procedures were successfully performed using basilic vein access with no access-related complications such as bleeding, thrombosis, or hematoma. The average surgical duration was 41.1 min (SD = 4.1), and a mean of 2.6 coils (SD = 0.7) was used per case. The left gonadal vein was embolized in all patients, with additional embolization of the right gonadal (68.8%) and hypogastric veins (6.8%) when indicated. Only one patient (0.3%) experienced a coil migration resulting in pulmonary embolism, requiring reintervention and a short ICU stay. No mortalities were reported. Symptom resolution was achieved in 278 patients (95.2%), indicating high procedural effectiveness.
Conclusions
Basilic vein access is a feasible and safe alternative for pelvic vein embolization in patients with PCS. This approach demonstrated excellent technical success, a low complication rate, and high symptom resolution, with the added benefits of shorter procedure time and reduced coil usage compared to traditional access routes. These findings suggest potential procedural and resource efficiency advantages. However, due to the study’s retrospective nature and lack of comparative controls, prospective studies are necessary to further assess the long-term efficacy and cost-effectiveness of basilic access in comparison to femoral and jugular approaches. Establishing standardized guidelines for vascular access in PCS treatment could enhance outcomes and procedural safety.
Keywords
Introduction
Pelvic varicose veins represent dilations within the pelvic venous network stemming from venous dysfunction, obstruction, and reflux, predominantly encircling the uterus and its adjacent structures within the female reproductive system. 1 This condition typically manifests in multiparous women or primiparous women with vaginal delivery and prolonged labor process. 2 Furthermore, factors such as inferior vena cava thrombosis, endometriosis, adhesions, Nutcracker syndrome, and May–Thurner syndrome may contribute to their pathogenesis. 3 The concomitant presence of ovarian and pelvic varicose veins alongside related symptoms, such as non-cyclical chronic pelvic pain persisting for over 6 months, dysmenorrhea, dysuria, or dyspareunia, is recognized as pelvic congestion syndrome (PCS).1,4
While often underdiagnosed, approximately 30% of women aged 18 to 50 experiencing chronic pelvic pain are ultimately diagnosed with PCS.1,4 Timely identification of PCS is imperative given its association with symptomatic recurrences, imposing substantial economic strain on individuals and healthcare systems, while also detrimentally affecting patients’ quality of life.1,5
PCS is typically diagnosed either directly through physical examination of the vulvar or perivulvar regions or indirectly through a symptomatic history consistent with its diagnosis. However, it is now recognized that varicose veins can be effectively visualized using imaging modalities such as catheter venography or transvaginal/transperineal Doppler ultrasound. 2 Conversely, while various treatment modalities exist for PCS, ranging from conservative to surgical approaches, percutaneous catheter embolization of ovarian and/or pelvic veins has emerged as a primary therapeutic intervention. This procedure boasts a success rate of approximately 96%, with sustained symptom relief achieved in 70–90% of cases. 6
The primary approach for performing transcatheter embolization of pelvic varicose veins typically involves utilizing either an internal jugular vein or a femoral vein approach. However, these methods are associated with increased complications related to vascular access, a higher risk of bleeding, and elevated levels of pain for the patient. 7 The aim of this study was to showcase the safety and efficacy of utilizing basilic vein percutaneous access for endovascular embolization of pelvic varicose veins.
Materials and methods
A retrospective-cohort based population study was conducted, including patients who underwent endovascular embolization for pelvic varicose veins with percutaneous access on the distal third of the right basilic vein, at two medical centers in Bogotá, Colombia: Hospital Simón Bolívar and Clínica Colombia between 2018 and 2023.
The inclusion criteria for patient selection were women of reproductive age with symptomatic PCS, characterized by chronic pelvic postcoital pain and varicose veins in the lower limbs with a pelvic distribution. Additionally, the embolization must have been performed via the basilic vein access, with other access routes (cephalic, jugular, femoral) being excluded. In all cases, basilic vein access was attempted as the first-line approach. No patients were excluded due to failed basilic access, as all procedures in this series were successfully performed via this route. The diagnosis was confirmed by transvaginal pelvic Doppler ultrasound, identifying pelvic varicose veins with a diameter greater than 6 mm and evidence of reflux.
The current study collected demographic data including age, gender, race, and body mass index (BMI) for all patients. Two classification systems were utilized to assess the severity of pelvic varicose veins. The Symptoms-Varices-Pathophysiology (SVP) classification considers symptoms, varicose vein location, and pathophysiology (anatomy, hemodynamics, and etiology) to stage varicose vein disease, while the CEAP classification utilizes clinical, etiologic, anatomic, and physiologic factors to describe the visible signs of venous disease.
Intraoperative variables analyzed were venous procedural approach via basilic vein, surgery duration, hemorrhagic events, and the number of coils used. Signs of vascular access complications (bleeding, thrombosis, and hematoma) were recorded as well. Postoperative outcomes evaluated were successful embolization of the targeted refluxing pelvic veins (left gonadal, right gonadal, or hypogastric), congestive symptom resolution, the need of reintervention, complications such as pulmonary embolism due to coil migration, length of hospital stay, length of stay in intensive care unit (ICU), and mortality at 6 months.
The postoperative follow-up comprised clinical outpatient evaluations at 15 days, 3 months, and 6 months, to evaluate the procedural effectiveness. Patients experiencing persistent symptoms underwent additional investigations as required, including transvaginal Doppler examinations, to ensure a thorough assessment of the long-term efficacy and safety profile of endovascular embolization in this patient group. The evaluation of procedural effectiveness was based on symptom resolution.
All data were placed in Microsoft Excel for Mac and analyzed using descriptive statistics. Percentages were calculated for all nominal variables included in the study.
Surgical technique
The procedure was performed with the patient in a supine position and the left arm abducted to 90° and externally rotated to optimize basilic vein alignment. Local anesthesia with 1% lidocaine was administered, and ultrasound guidance (7.5–10 MHz linear probe) was used to identify and cannulate the basilic vein in the medial antecubital fossa using a 21-gauge micropuncture needle. Following confirmation of intraluminal placement, a 0.018-inch wire was exchanged for a 5-Fr hydrophilic radial sheath (optionally 6-Fr for larger devices), through which 2–3 mL of heparinized saline was injected to prevent thrombus formation (Figure 1) Basilic vein approach for endovascular embolization of pelvic varices: step-by-step overview. (a). Venographic exclusion of May–Thurner syndrome. (b). Evaluation of pelvic varices originating from hypogastric veins. (c) Venographic exclusion of Nutcracker syndrome. (d). Venographic evaluation of the left gonadal vein. (e). Embolization of the left gonadal vein—initial coil placement. (f). Completion embolization of the left gonadal vein. (g). Evaluation of the right gonadal vein. (h). Embolization of the right gonadal vein—initial coil deployment. (i). Completion embolization of the right gonadal vein.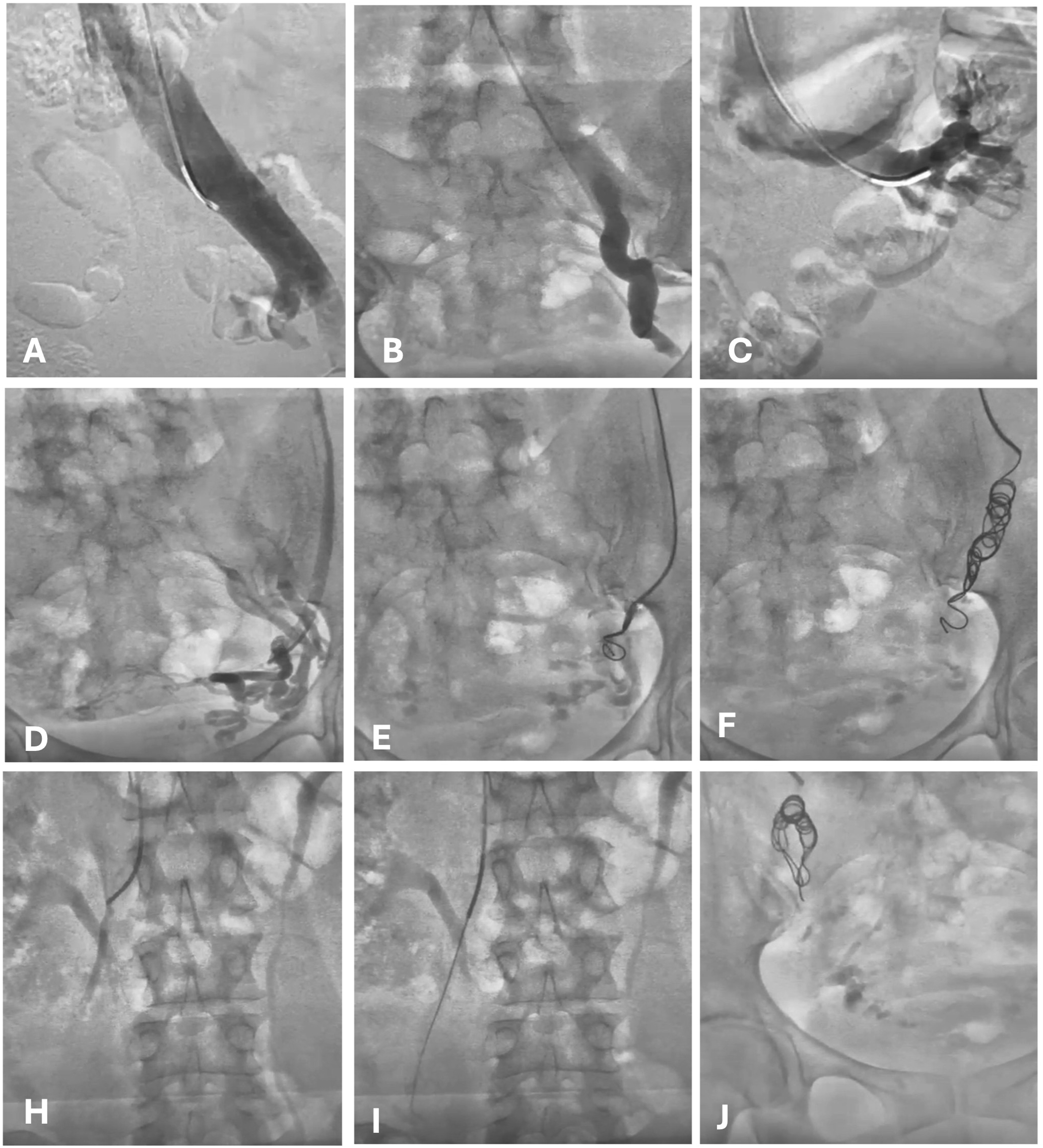
A 0.035-inch hydrophilic guidewire was then advanced through the basilic, brachial, axillary, and subclavian veins, crossing the cavoatrial junction and reaching the infrarenal inferior vena cava (IVC) under continuous fluoroscopic guidance. To facilitate guidewire passage in tortuous anatomy, gentle torquing and breath-hold maneuvers were employed. A 5-Fr multipurpose (MPA-1) catheter was advanced over the wire and positioned in the infrarenal IVC, where a cavogram was performed using iodinated contrast to assess patency and collateral flow.
Subsequently, selective phlebography was performed through the left common iliac vein and internal iliac veins to evaluate for pelvic varicosities and rule out May–Thurner syndrome. The catheter was then directed into the left renal vein for contrast injection to exclude Nutcracker syndrome. Pressure measurements across the renocaval segment were performed selectively in patients with suggestive findings.
Bilateral gonadal vein phlebography was conducted to assess for venous reflux, dilation (>5 mm), and the presence of cross-pelvic collaterals. When venous incompetence was identified, selective embolization was performed using detachable platinum coils (e.g., Interlock or Concerto), typically sized 20–30% larger than the target vein diameter to ensure secure occlusion. In patients with complex collateral networks or large-diameter veins, embolization was supplemented with foam sclerotherapy (3% sodium tetradecyl sulfate mixed with air) using a sandwich technique (distal coil, sclerosant, then proximal coil) to enhance occlusion durability and reduce recanalization risk.
Final phlebography confirmed complete occlusion of refluxing veins and absence of significant residual flow. The catheter and sheath were removed, and hemostasis was achieved through manual compression. A compression bandage was applied for 24 h to minimize hematoma formation. In patients with difficult anatomy or anticoagulation, closure devices were selectively employed. Throughout the procedure, adjunctive measures such as intra-sheath vasodilators (e.g., nitroglycerin or verapamil) were used to counteract venous spasm, and microcatheters were employed when selective cannulation of small or tortuous gonadal veins was required.
Results
Demographic characteristics of included patients.
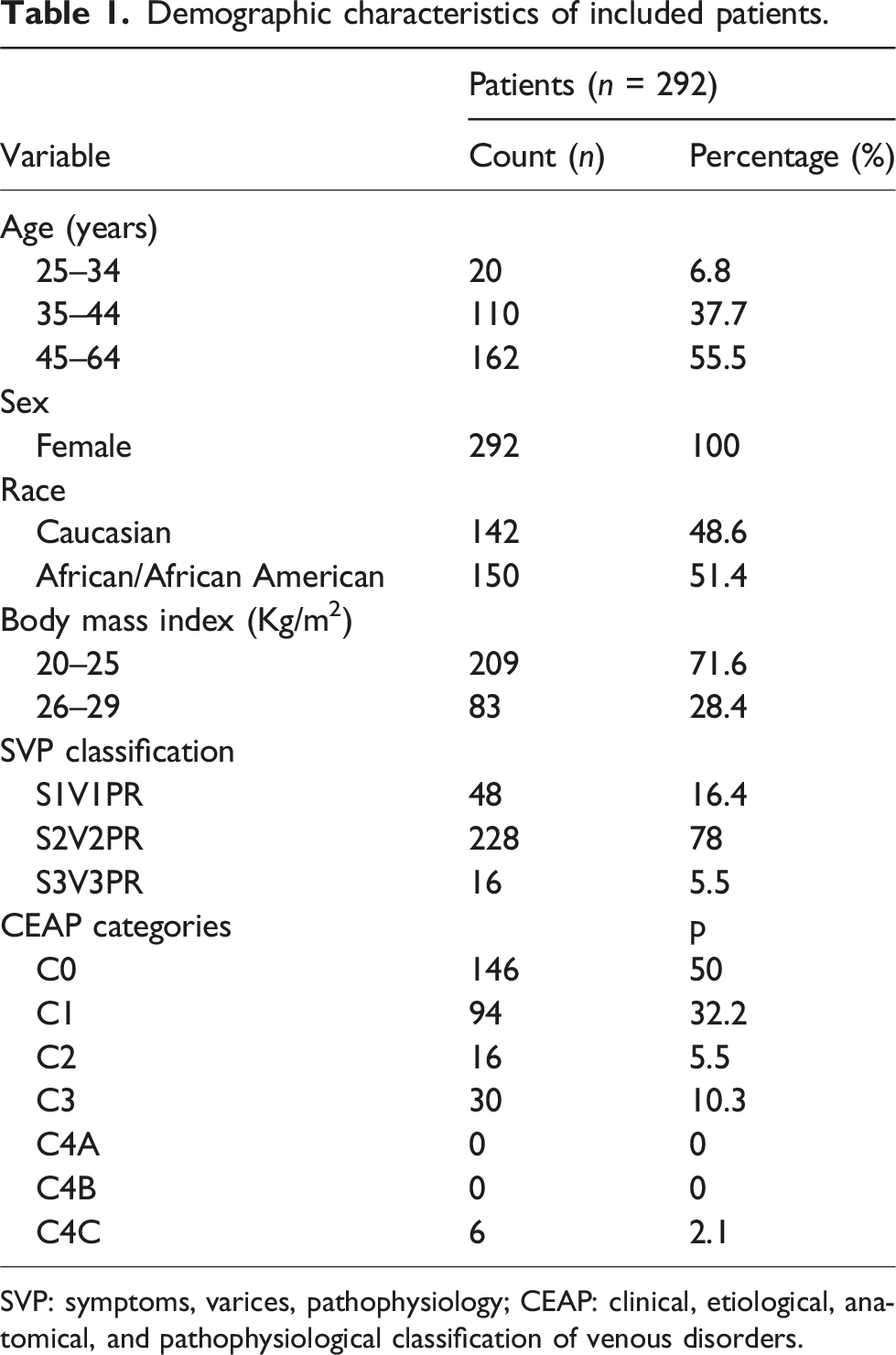
SVP: symptoms, varices, pathophysiology; CEAP: clinical, etiological, anatomical, and pathophysiological classification of venous disorders.
Perioperative outcomes of patients who underwent pelvic varicose veins embolization using basilic vein access.
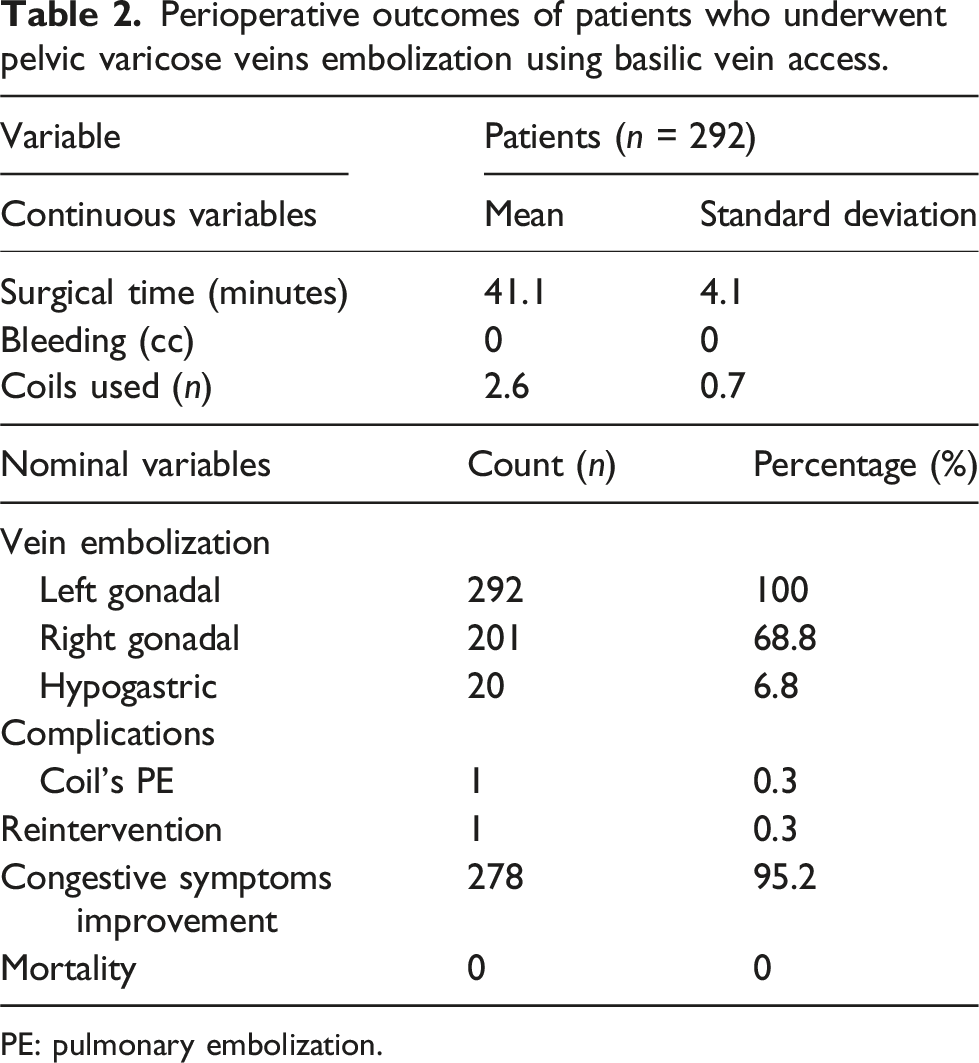
PE: pulmonary embolization.
Discussion
Previous studies have identified left femoral venous access as a commonly used approach for pelvic varicose vein embolization and venography. 1 In our study, basilic vein access proved to be a feasible and effective alternative for pelvic vein embolization in patients with pelvic congestion syndrome (PCS). Although the literature lacks direct comparisons between different vascular access routes, our experience suggests that the basilic approach may offer practical advantages in certain clinical settings.
We found that basilic vein access was associated with favorable intraoperative outcomes, including shorter procedure times and reduced coil usage. While these findings are encouraging, it is important to note that they are based on observational data, and no randomized or comparative studies have been published to date that directly evaluate procedure time, resource use, or cost across vascular access techniques. Nonetheless, these findings highlight the viability of basilic vein access with a low incidence of complications and the potential for performing phlebocavography as needed.
Compared to the internal jugular approach, which is often considered simple and direct, our data and findings from previous studies suggest that it may carry a higher risk of complications. In a retrospective cohort of 156 patients, jugular access was associated with an 8.9% complication rate, including contrast extravasation (1.9%), abdominal pain (1.3%), access site pain (0.6%), pudendal vein thrombosis (0.6%), and allergic reactions to contrast (1.3%). Additionally, 18.9% of patients reported increased pelvic pain in the post-procedural period, and 20% required reintervention due to symptom recurrence. 8
Similarly, femoral access, while technically successful in 100% of cases in one study, often required the use of additional materials (67.3%) and was associated with a 35.3% rate of persistent pain at 3-month follow-up. 9 In our series, basilic vein access was associated with a higher rate of symptom resolution, with 90.5% of patients experiencing significant improvement in pelvic pain and congestion.
A particularly notable finding in our study was the reduction in the number of coils used during embolization. Compared to an average of six coils reported in studies using femoral and jugular access,1,10 basilic vein access required an average of only 2.6 coils per procedure—a 57% reduction—without an increase in procedure-related complications. Although this difference may primarily reflect operator preference and technique rather than the access site itself, it suggests a potential for improved resource efficiency that warrants further investigation.
Given the well-documented predominance of left ovarian vein involvement in PCS,11–14 the basilic approach also offers direct anatomical access to the affected venous territory. In our cohort, successful embolization was achieved in all patients. While no clear consensus exists regarding the necessity of embolizing the right ovarian or iliac veins in all cases, our findings support the feasibility of using basilic vein access to effectively treat the primary site of venous reflux in PCS.
This study has several limitations, foremost its retrospective nature and the absence of a control group. As a result, we were unable to control for potential confounders or compare outcomes across different access routes in a standardized manner. The relatively short follow-up period also limits the assessment of long-term efficacy and delayed complications. Furthermore, the lack of objective symptom scoring precludes definitive conclusions about the magnitude of symptom improvement. Despite these limitations, our study adds valuable data to the limited literature on alternative venous access routes for PCS treatment and highlights basilic vein access as a feasible and potentially advantageous technique that merits further prospective evaluation.
Conclusion
This study demonstrates the feasibility and safety of basilic vein access for endovascular embolization of pelvic varicose veins in patients with pelvic congestion syndrome (PCS). Our findings suggest that this approach may offer advantages over more commonly used access routes, such as the internal jugular vein, including a lower incidence of complications, reduced need for hospitalization, and high rates of symptom improvement. While we did observe shorter procedure times and reduced coil usage in our cohort, these findings must be interpreted cautiously, as there are currently no prospective studies directly comparing different vascular access techniques for PCS embolization.
The results of this study support the consideration of basilic vein access as a viable and potentially preferable route for pelvic vein embolization. It appears to provide a safe and patient-friendly alternative that may improve procedural efficiency and outcomes. However, further prospective, comparative studies are warranted to validate these observations and to establish standardized protocols regarding the optimal vascular access route for this intervention. In addition, our findings highlight important gaps in the current literature. There is a need for well-designed studies comparing vascular access options in terms of technical success, procedural time, resource utilization, cost, complication rates, and long-term outcomes. Establishing evidence-based guidelines for access route selection could significantly enhance the standardization and effectiveness of PCS management through embolization.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
This retrospective study adhered to rigorous ethical standards, including strict measures to protect patient confidentiality and data privacy. The Ethics Committee reviewed the study and determined that the minimal risk posed to participants justified its approval without additional evaluation.