
Abstract
Background
The management of Common Femoral Artery (CFA) stenocclusive disease presents unique challenges, with debates persisting regarding the optimal treatment strategy between Open Common Femoral Endarterectomy (CFE) and Endovascular Therapy (EVT). This study aimed to compare the efficacy of CFE versus EVT, as well as simple versus advanced EVT (aEVT), using a Bayesian hierarchical framework.
Methods
A systematic review was conducted according to PRISMA guidelines by querying PubMed, ScienceDirect, Scopus, and the Cochrane Library for articles published through June 2024. The study included randomized controlled trials and retrospective observational studies with a minimum of 40 patients per cohort. Data were synthesized using a Bayesian random-intercept logistic model to estimate pooled Odds Ratios (OR) for primary patency, freedom from reintervention, and limb salvage.
Results
The analysis included 10 comparative studies encompassing 1452 patients. Open CFE demonstrated superior outcomes compared to EVT, with a significantly reduced odds of patency loss (OR 0.480; 95% CrI: 0.367–0.626) and lower reintervention rates (OR 0.534; 95% CrI: 0.391–0.718). Limb salvage rates also favored CFE (OR 0.548; 95% CrI: 0.402–0.737). In subgroup analyses, advanced EVT (involving atherectomy) improved primary patency compared to simple EVT (OR 0.520; 95% CrI: 0.306–0.883) but did not statistically significantly reduce the need for reintervention (OR 0.910; 95% CrI: 0.427–1.894).
Conclusion
Open CFE remains the gold standard for CFA stenocclusive disease, offering superior long-term durability and limb salvage compared to endovascular interventions. While advanced endovascular techniques improve patency rates compared to simple balloon angioplasty, they fail to significantly reduce reintervention rates, likely due to the biomechanical stress of the femoral region. EVT should be considered a pragmatic option reserved primarily for high-surgical-risk patients.
Keywords
Introduction
Peripheral artery disease (PAD) is a major global health concern, with atherosclerotic involvement leading to stenosis and occlusions that can compromise limb perfusion and function 1 . The common femoral artery (CFA), in particular, plays a critical role in lower extremity blood supply and is frequently afflicted by atherosclerotic lesions due to its anatomical location and exposure to mechanical stress 2 . The management of CFA stenocclusive disease poses unique challenges: while open common femoral endarterectomy (CFE) is recognized for its long‐term durability with reported 5‐year primary patency rates exceeding 90%3,4 its invasiveness is associated with higher perioperative morbidity, including wound complications and extended recovery 5 . Conversely, endovascular therapy (EVT) offers a less invasive alternative with shorter hospital stays; however, EVT is often linked with increased rates of restenosis and the need for reintervention, particularly due to the biomechanical stresses imposed on stents and balloons in the groin region6–8.
Prior systematic reviews and meta‐analyses have yielded mixed results due to heterogeneity in study design, patient populations, and evolving device technology5,6. Recent randomized trials7,8 and observational studies9–11 have provided further insight, yet debates remain regarding the optimal treatment strategy. In addition, the emergence of “advanced” endovascular techniques combining atherectomy with adjunctive stenting or drug‐coated balloon therapy has further complicated the therapeutic landscape12–14. The current clinical guidelines of the European Society of Cardiology (ESC) 3 and the National Institute for Health and Care Excellence (NICE) 4 continue to emphasize individualized treatment decisions based on disease severity, anatomical complexity, and patient comorbidities 15 .
The advent of Bayesian hierarchical meta‐analysis has provided a robust framework for synthesizing heterogeneous data while appropriately accounting for between‐study variability 16 . By incorporating prior distributions and utilizing Markov chain Monte Carlo (MCMC) sampling, Bayesian methods offer a flexible approach to estimate pooled effect sizes and assess model adequacy through predictive checks and information criteria (e.g., WAIC) 17 . In this study, we integrate data from 10 comparative studies and implement a Bayesian random‐intercept logistic model to compare open CFE with EVT, as well as to compare EVT versus advanced EVT (aEVT), across three critical clinical endpoints: primary patency, freedom from reintervention, and limb salvage. Moreover, we conduct a sub‐analysis contrasting simple (balloon ± drug‐coated) and advanced endovascular approaches.
We further report the outcomes from our new analysis pipeline implemented in R using packages such as rjags, bridgesampling, and runjags which provides detailed diagnostic outputs (e.g., trace plots, Gelman–Rubin statistics, and effective sample sizes) and sensitivity analyses. Our aim is to generate robust, reproducible estimates that inform evidence‐based clinical decision‐making in the management of CFA stenocclusive disease.
Methods
Study selection and data extraction
Literature search and study eligibility
We conducted this meta‐analysis in accordance with the Preferred Reporting Items for Systematic Reviews and Meta‐Analyses (PRISMA) guidelines. Four electronic databases PubMed, ScienceDirect, Scopus, and the Cochrane Library were queried through June 2024. Search terms included “common femoral artery,” “endarterectomy,” “atherectomy,” “balloon angioplasty,” “drug‐coated balloon,” “stent,” “limb salvage,” “primary patency,” and “reintervention,” combined using Boolean operators (e.g., (common femoral) AND (endarterectomy OR atherectomy OR stent OR balloon)). The initial search retrieved 1143 articles (75 in PubMed, 74 in ScienceDirect, 910 in Scopus, and 84 in the Cochrane Library). After de‐duplication, 1025 unique records were retained for abstract/title screening.
Two reviewers independently (N.G. and T.P.) evaluated abstracts and titles. We excluded non‐English conference abstracts, studies lacking relevant comparative data, cohorts with fewer than 20 patients per study arm, and investigations focused on non‐CFA sites. This screening yielded 129 full‐text articles, from which an additional set of exclusions was applied, ultimately leaving 10 eligible studies. Inclusion criteria were as follows: (1) Population: Adult patients (≥18 years) with CFA stenocclusive disease necessitating revascularization. (2) Comparative Design: Each study compared either (a) open endarterectomy versus any endovascular (EV) approach, or (b) simple versus advanced endovascular interventions. (3) Outcomes: Binomial event data (events/sample) for at least one of the following endpoints: primary patency, freedom from reintervention, or limb salvage. (4) Minimum Sample Size: At least 40 patients. (5) Study Type: Randomized controlled trials or retrospective/observational investigations.
A PRISMA flow diagram (S.1) details the selection process, from initial identification to final inclusion.
Study registration
This systematic review and meta-analysis were prospectively registered with PROSPERO registration number CRD42025649928. The protocol is publicly available through the PROSPERO database, ensuring transparency and reproducibility of the study methodology.
Data extraction and study characteristics
Baseline characteristics, demographics, and lesion classifications of the included studies.
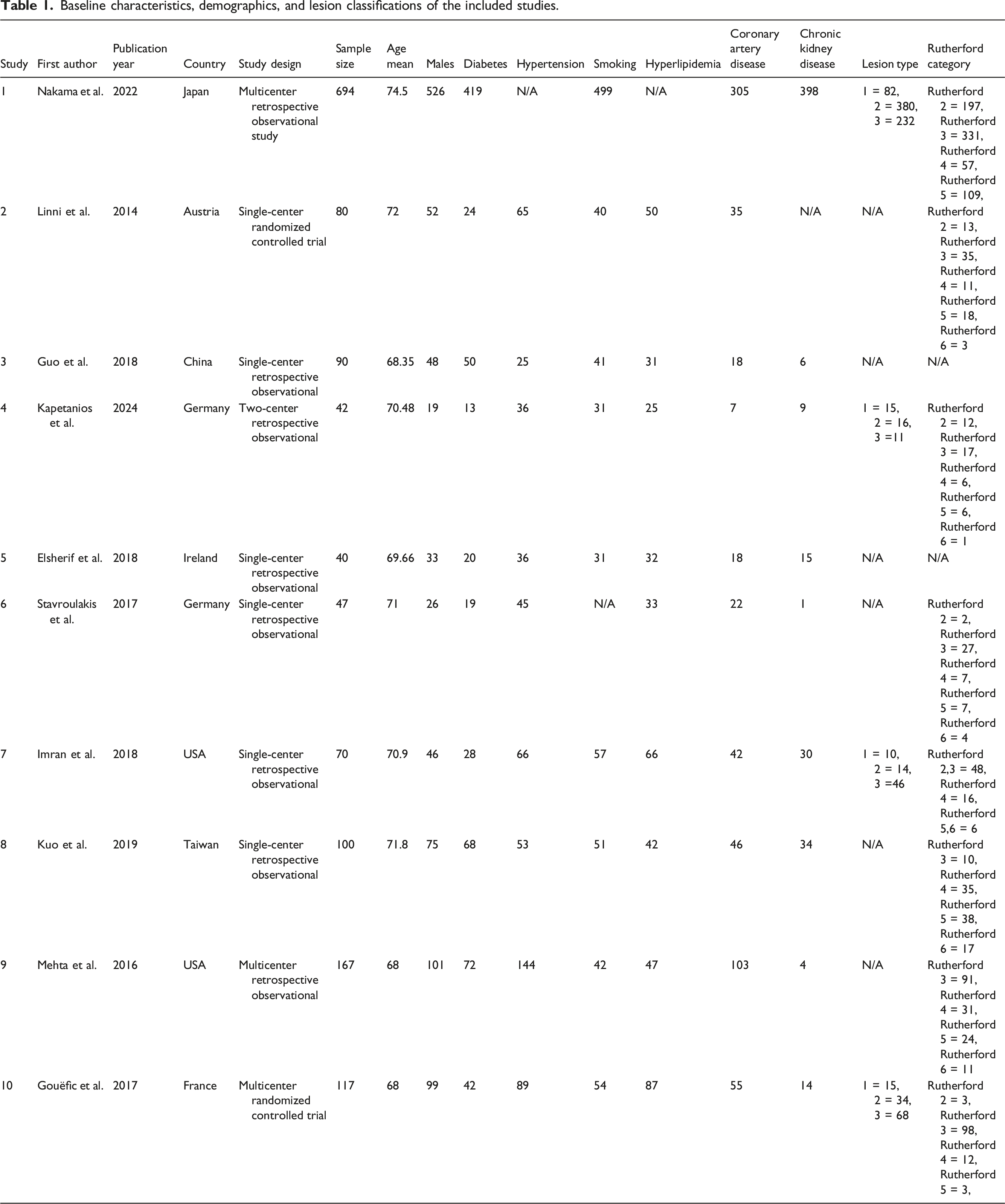
We classified open CFE arms as those explicitly labeled “endarterectomy” without mention of “atherectomy.” Interventions mentioning balloon angioplasty, stenting, or atherectomy were deemed endovascular (EV). For the sub‐analysis, we distinguished “advanced” EV arms (directional/orbital atherectomy ± stent/balloon) from “simple” EV arms (balloon ± drug‐coated balloon [DCB]) based on the text descriptions.
Outcome definitions
We compiled binomial event data (number of events and total participants) for three key outcomes: (1) Primary Patency: Maintained patency of the treated artery, typically defined as ≤50% restenosis or no occlusion by duplex ultrasound or angiography at ∼12–48 months of follow‐up. (2) Freedom from Reintervention: The proportion of patients who did not undergo any further endovascular or surgical procedure on the target lesion during the study period. (3) Limb Salvage: The absence of major (above‐ankle) amputation throughout follow‐up.
Bayesian hierarchical model specification
For each outcome, we assumed that the observed number of events yiyi followed a binomial distribution:

Random intercepts for each study were modeled as • β∼N(0,0.52)β∼N(0,0.52) • μα∼N(0,0.12)μα∼N(0,0.12) • σα∼Uniform(0,5)σα∼Uniform(0,5)
For the subgroup analysis comparing simple versus advanced endovascular therapies, the same model was employed with the treatment indicator defined by the presence of atherectomy in the intervention description.
Model implementation and diagnostics
The model was implemented using the rjags package in R (version 4.4.2). Two parallel MCMC chains were run for 20,000 iterations each, discarding the initial 6000 iterations as burn-in and applying a thinning factor of 4 to mitigate autocorrelation. Convergence was assessed using trace plots, Gelman–Rubin diagnostic statistics (target R^≈1.00 R^≈1.00), and effective sample size (ESS) calculations. Posterior summaries (median, standard deviation, and 95% credible intervals) were calculated for all parameters; the posterior samples for ββ were exponentiated to yield odds ratios (ORs).
Model adequacy was evaluated via posterior predictive checks. We generated replicated datasets from the median posterior parameter estimates and compared the mean event rates in the observed and replicated data. In addition, the widely applicable information criterion (WAIC) was computed for each model to facilitate model comparison and penalize overfitting. Sensitivity analyses were performed by altering the prior distributions (e.g., using β∼N(0,12)β∼N(0,12) instead of N (0,0.52)N(0,0.52)).
Analysis pipeline
We developed a custom R function, BayesCFAStudy, to streamline the entire analysis process. This function loads the primary patency, freedom from reintervention, and limb salvage datasets; constructs subgroup data frames using text-mining techniques to distinguish between interventions (based on keywords “endarterectomy” and “atherectomy”); and runs the Bayesian models via rjags. The pipeline outputs detailed diagnostic plots including trace plots, autocorrelation plots, and forest plots of the baseline odds (exponentiated random intercepts) and computes WAIC values for each model. Additional functions perform sensitivity analyses and posterior predictive checks.
Risk-of-bias assessment
Risk of bias was evaluated separately for randomized and observational studies. For randomized controlled trials, we applied the revised Cochrane risk‐of‐bias tool (RoB 2). Domain‐level judgments were used to derive an overall risk‐of‐bias rating for each trial. Detailed RoB 2 assessments for each randomized study are provided in (Supplemental Table S2).
For observational studies, quality was appraised using the Newcastle–Ottawa Scale (NOS), which examines selection, comparability, and outcome ascertainment. Studies were awarded stars based on predefined criteria, with higher scores indicating a lower risk of bias. Full NOS ratings and justifications for each observational study are available in (Supplemental Table S3).
Results
Study characteristics
A total of 10 studies, representing 1452 patients, met the inclusion criteria. The studies were conducted in diverse regions including Japan, Austria, China, Germany, the USA, Ireland, Taiwan, and France. Key characteristics of these studies, including study design, sample size, mean age, and details of the interventions (open CFE vs EVT and endovascular subtypes) are summarized in Table 1.7,8,11,18–24.
Primary patency
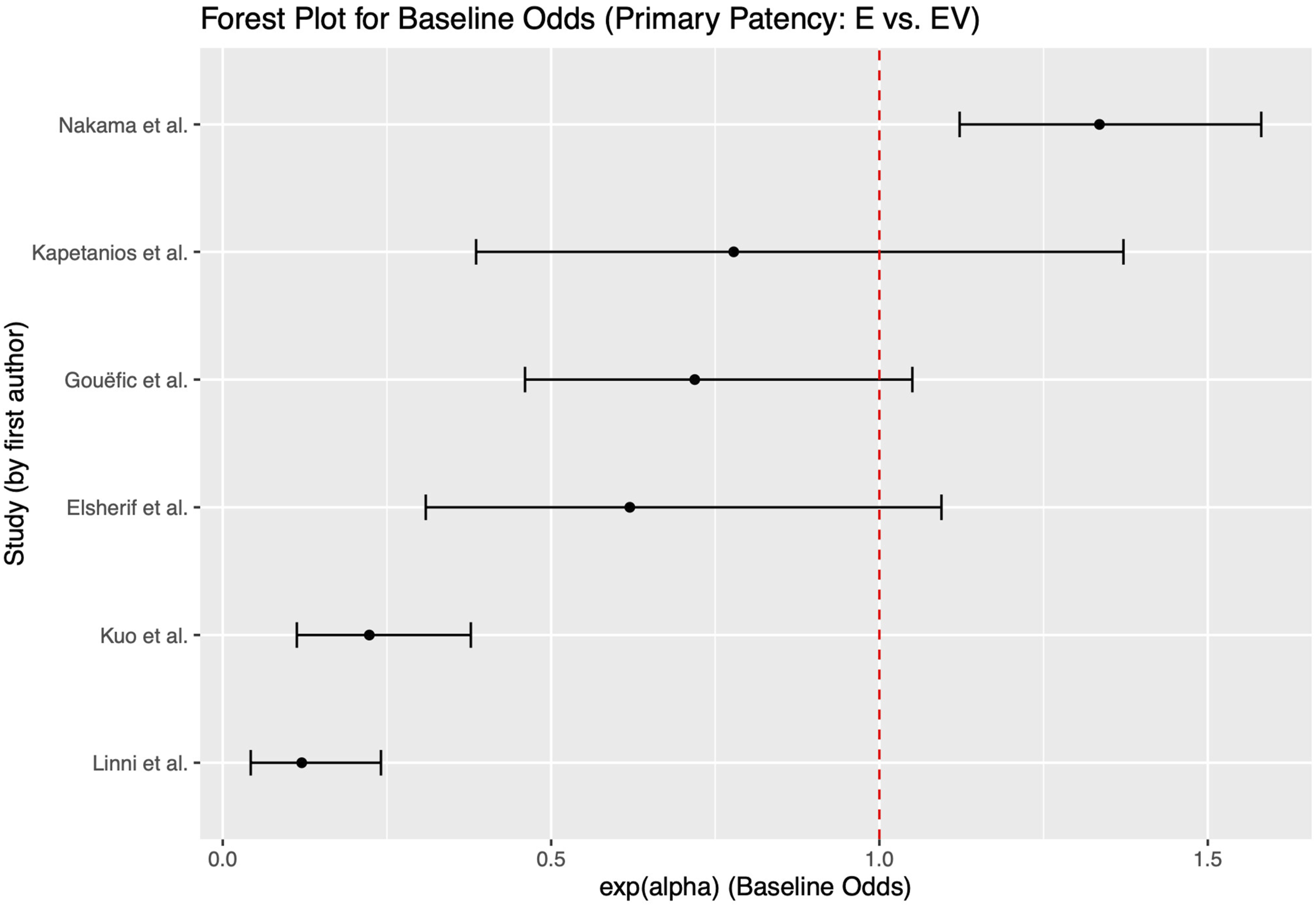
Data for primary patency were available from six studies comparing open CFE with EVT. The Bayesian model converged successfully (all Gelman–Rubin R^R^ values were ∼1.00), and the effective sample sizes were robust (all exceeding 6000). The posterior median for the treatment effect (ββ) was estimated to be −0.734 (95% CrI: −1.002 to −0.468). Exponentiating this estimate produced an OR of 0.480 (95% CrI: 0.367–0.626), which implies that open CFE reduces the odds of patency loss by approximately 52% compared with EVT7,8,18,20,23,24 (Figures 1 and 2). Bayesian diagnostic plots (trace plot, posterior density, and autocorrelation) for the primary patency analysis (endarterectomy vs endovascular therapy) Forest plot for baseline odds for primary patency (endarterectomy vs endovascular therapy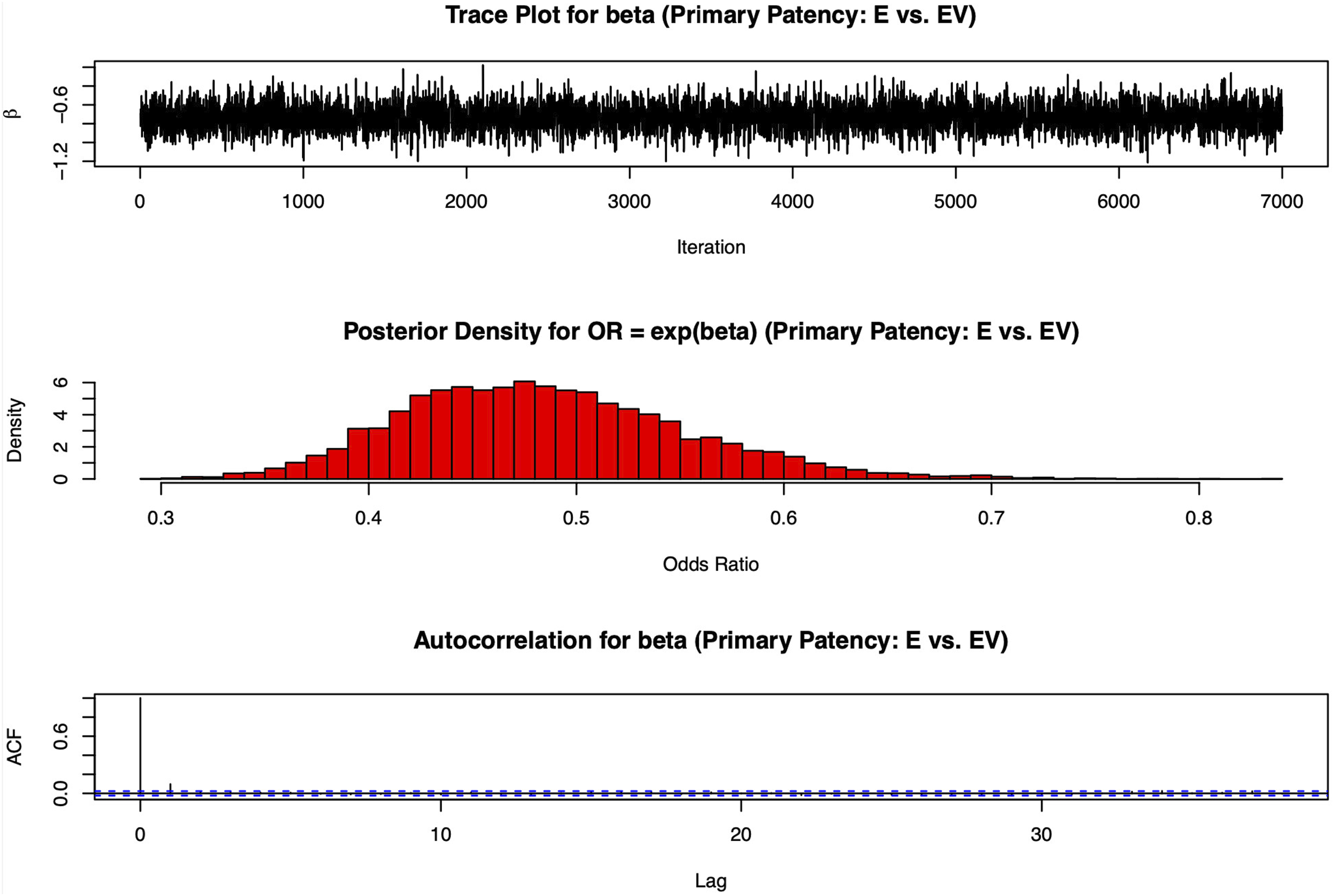
Freedom from reintervention
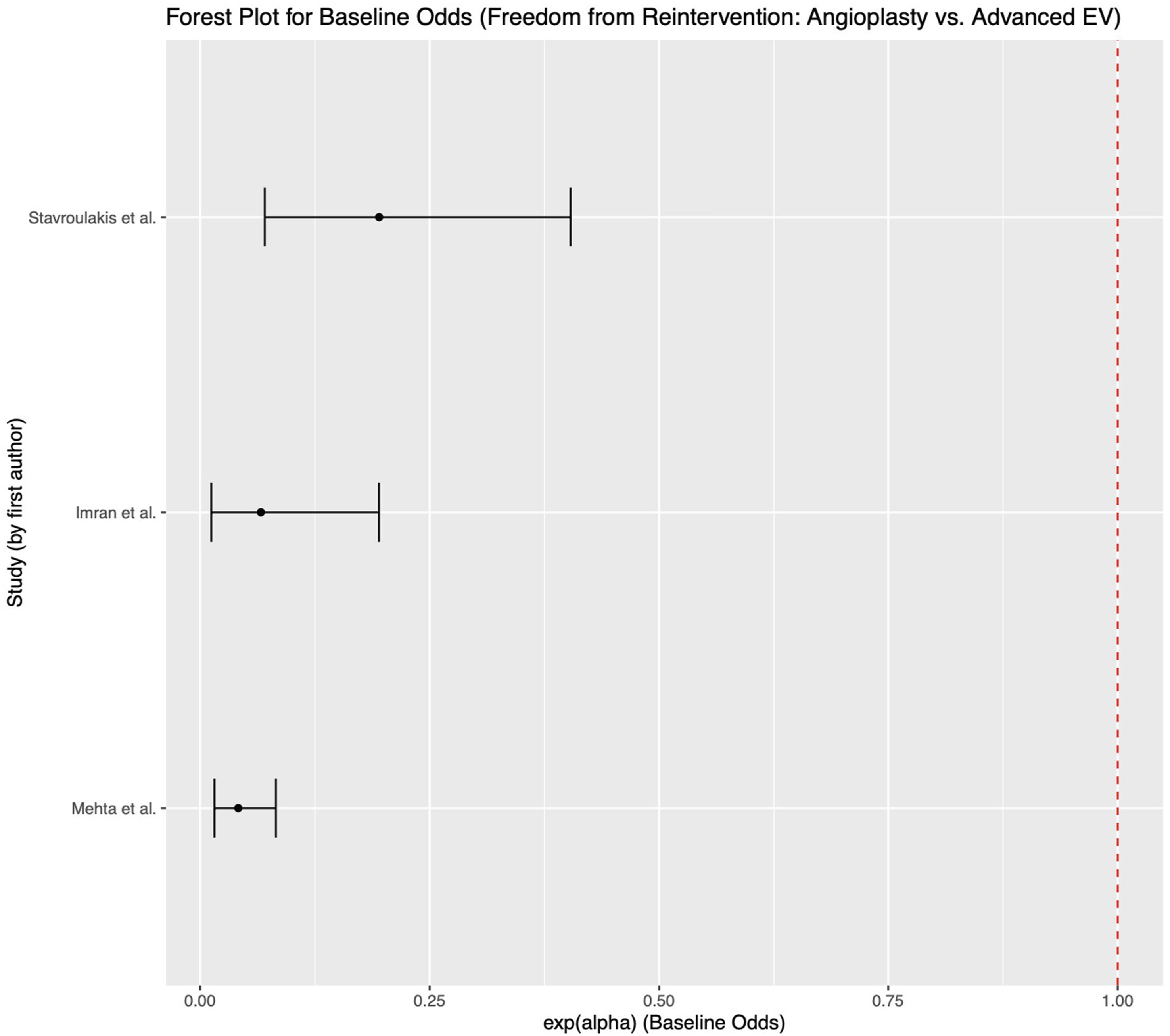
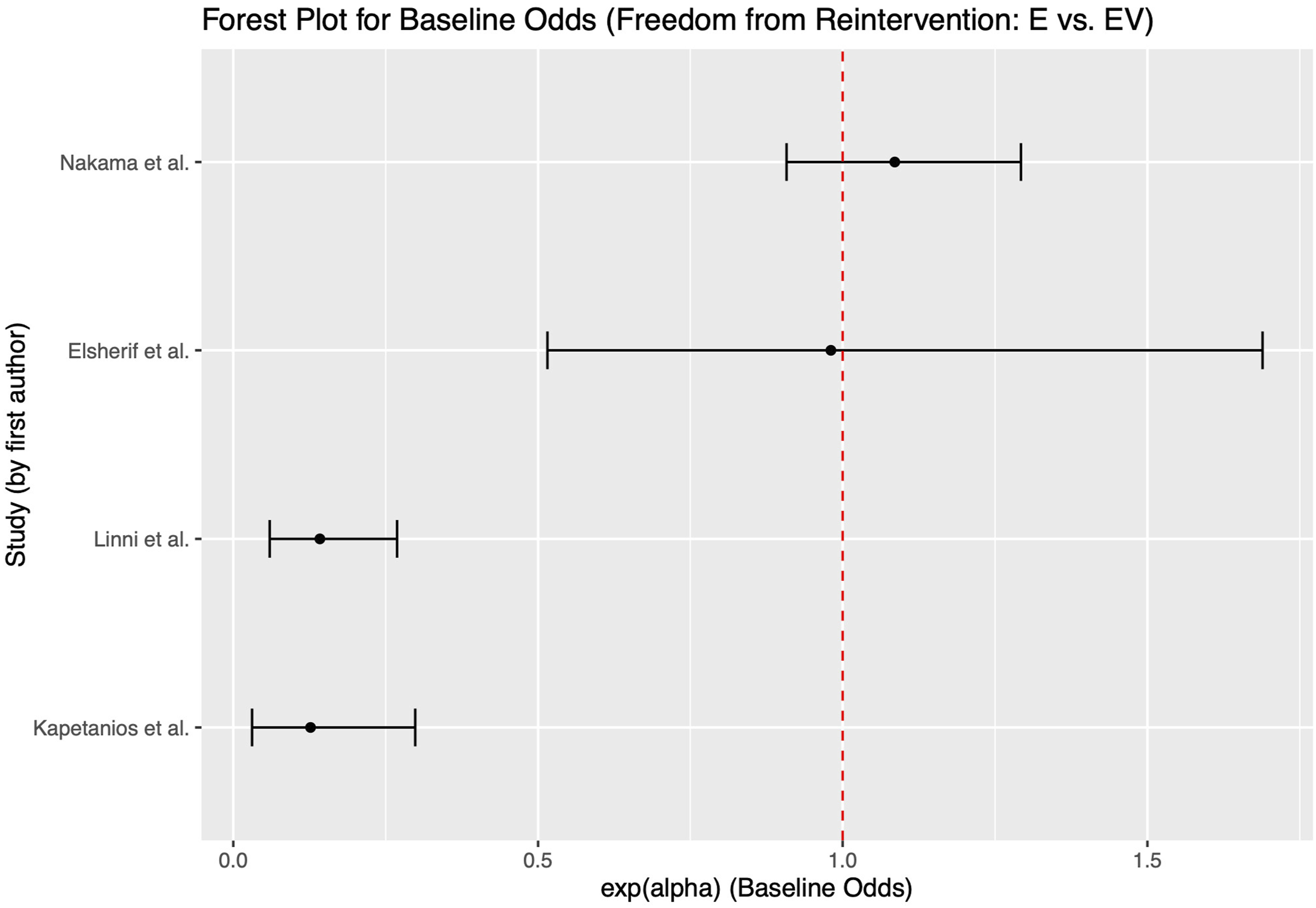
For freedom from reintervention, data were pooled from four studies. The posterior median ββ was −0.627 (95% CrI: −0.938 to −0.331), corresponding to an OR of 0.534 (95% CrI: 0.391–0.718)7,20,23,24 .These findings indicate that patients undergoing open CFE are less likely to require repeat interventions compared to those treated with EVT (Figures 3 and 5). Bayesian diagnostic plots (trace plot, posterior density, and autocorrelation) for the freedom from reintervention analysis (endarterectomy vs endovascular therapy) Forest plot for baseline odds for freedom from reintervention (angioplasty vs advanced endovascular therapy)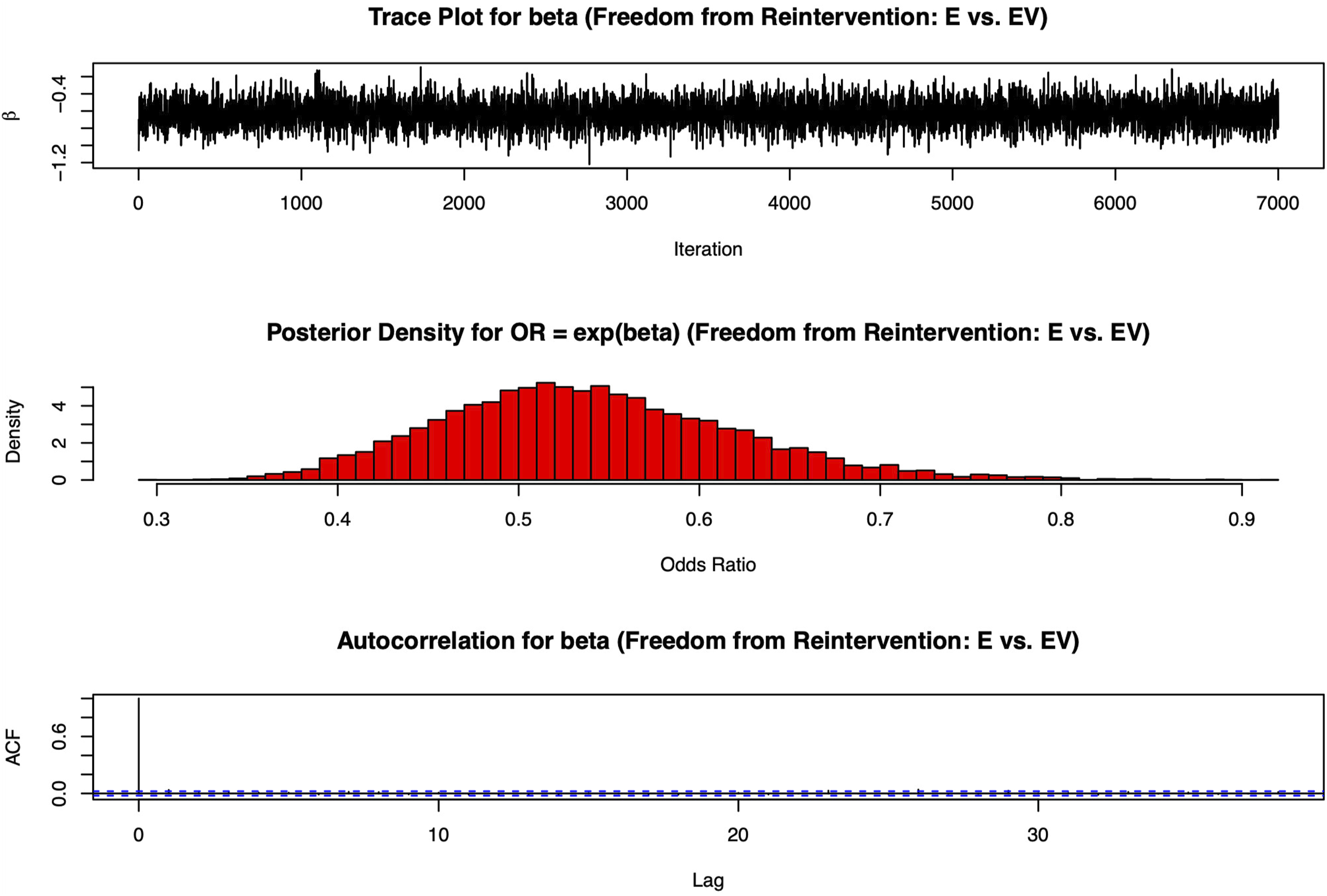
Limb salvage
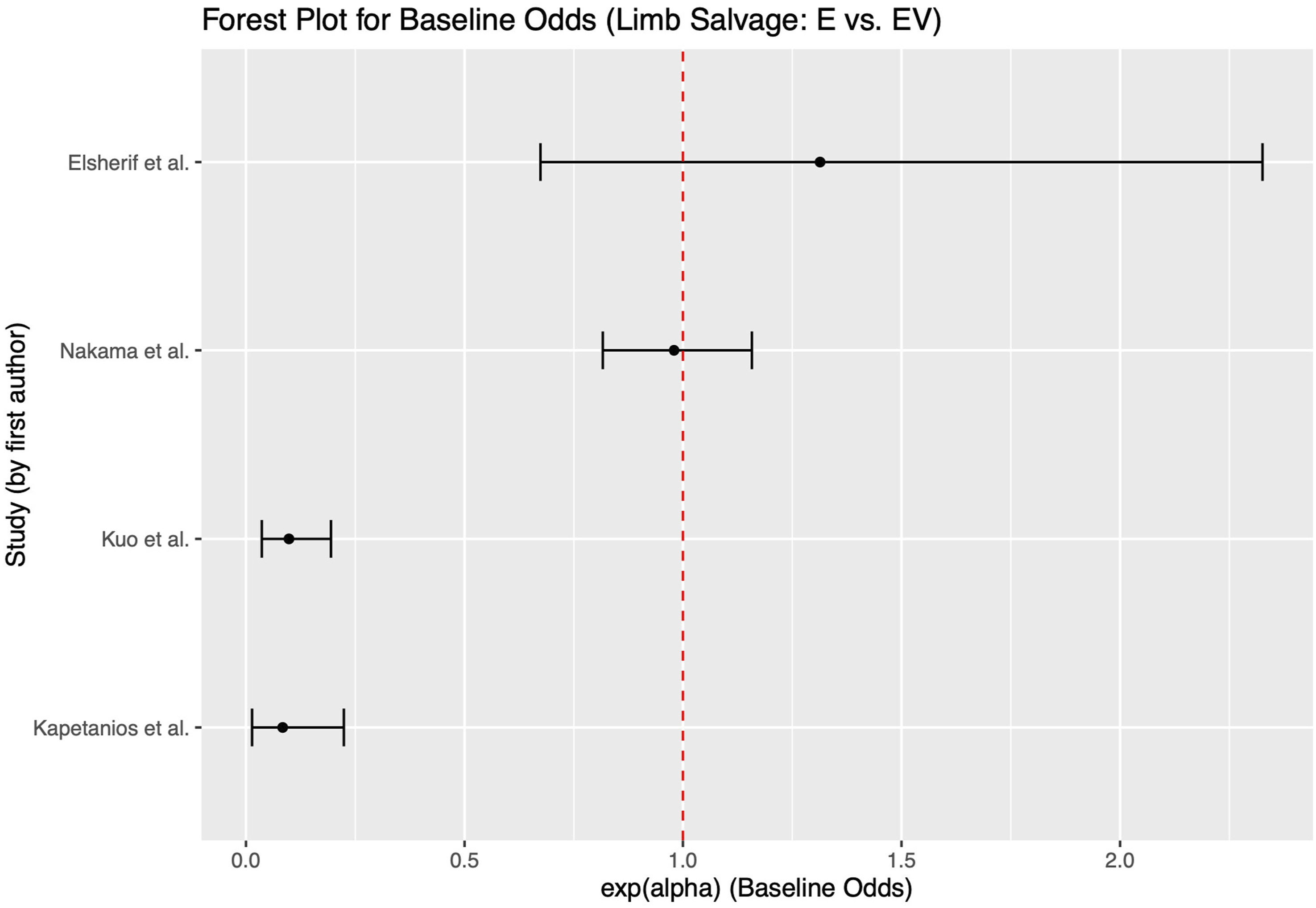
Seven studies contributed to the limb salvage outcome analysis. The overall posterior median ββ was −0.602 (95% CrI: −0.912 to −0.306), translating to an OR of 0.548 (95% CrI: 0.402–0.737)8,20,23,24. This suggests that open CFE provides a 45% reduction in the odds of major amputation relative to EVT. Although seven studies reported limb salvage outcomes, three of them either had zero events in both treatment arms or provided insufficient detail for inclusion in the pooled analysis (Figures 4 and 6). Bayesian diagnostic plots (trace plot, posterior density, and autocorrelation) for the limb salvage analysis (endarterectomy vs endovascular therapy Forest plot for baseline odds for limb salvage (endarterectomy vs endovascular therapy)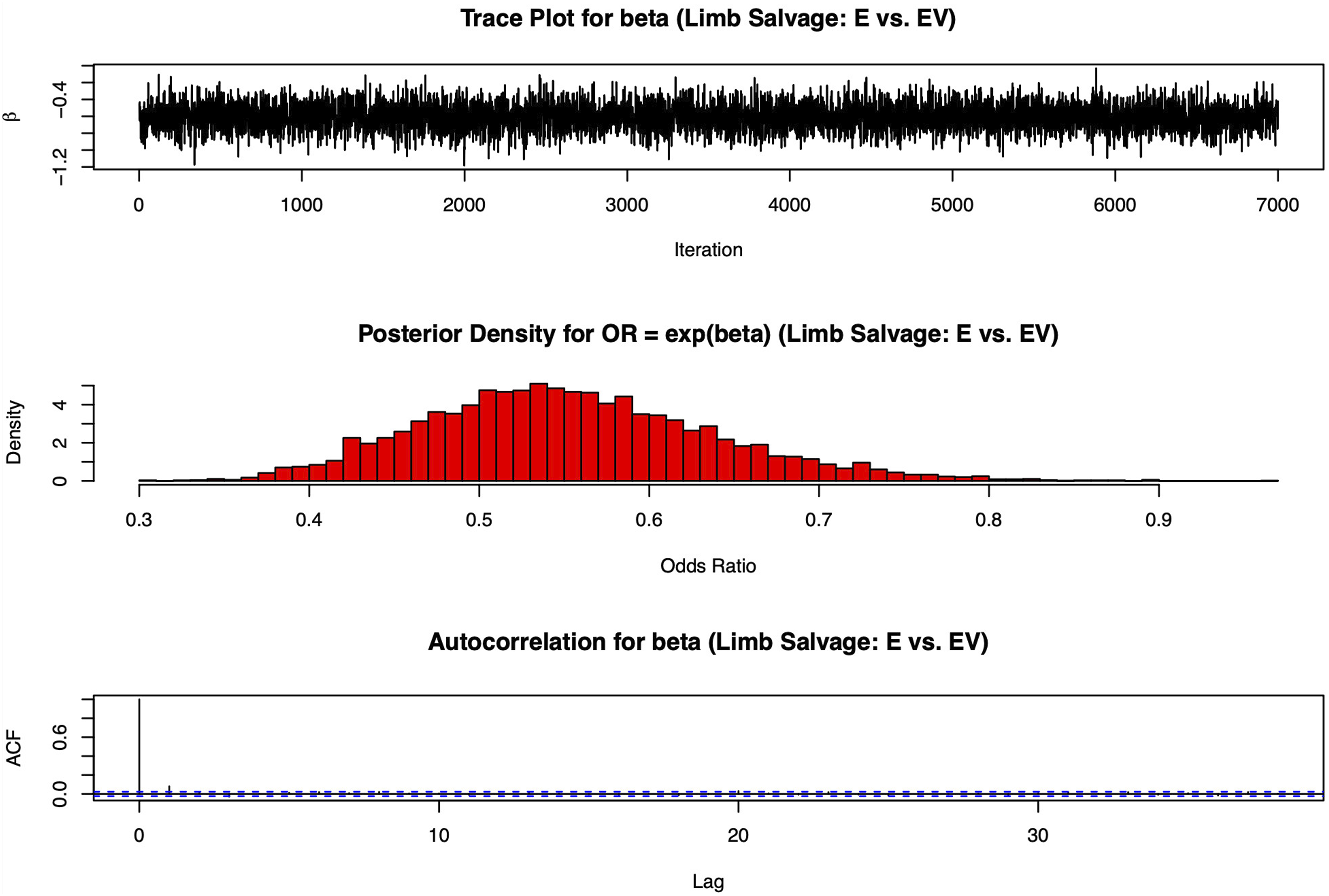
Subgroup analysis: Simple versus advanced endovascular techniques
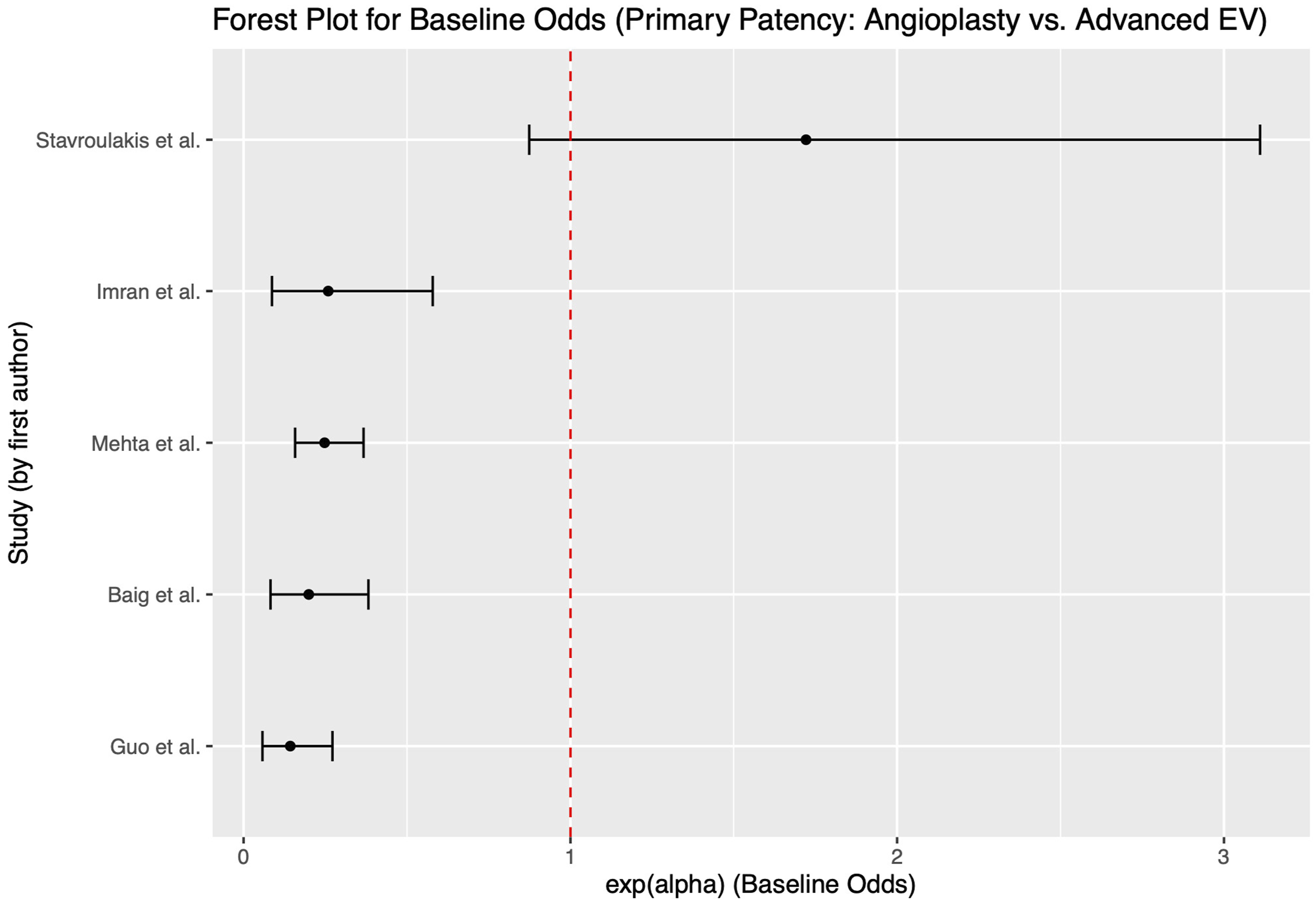
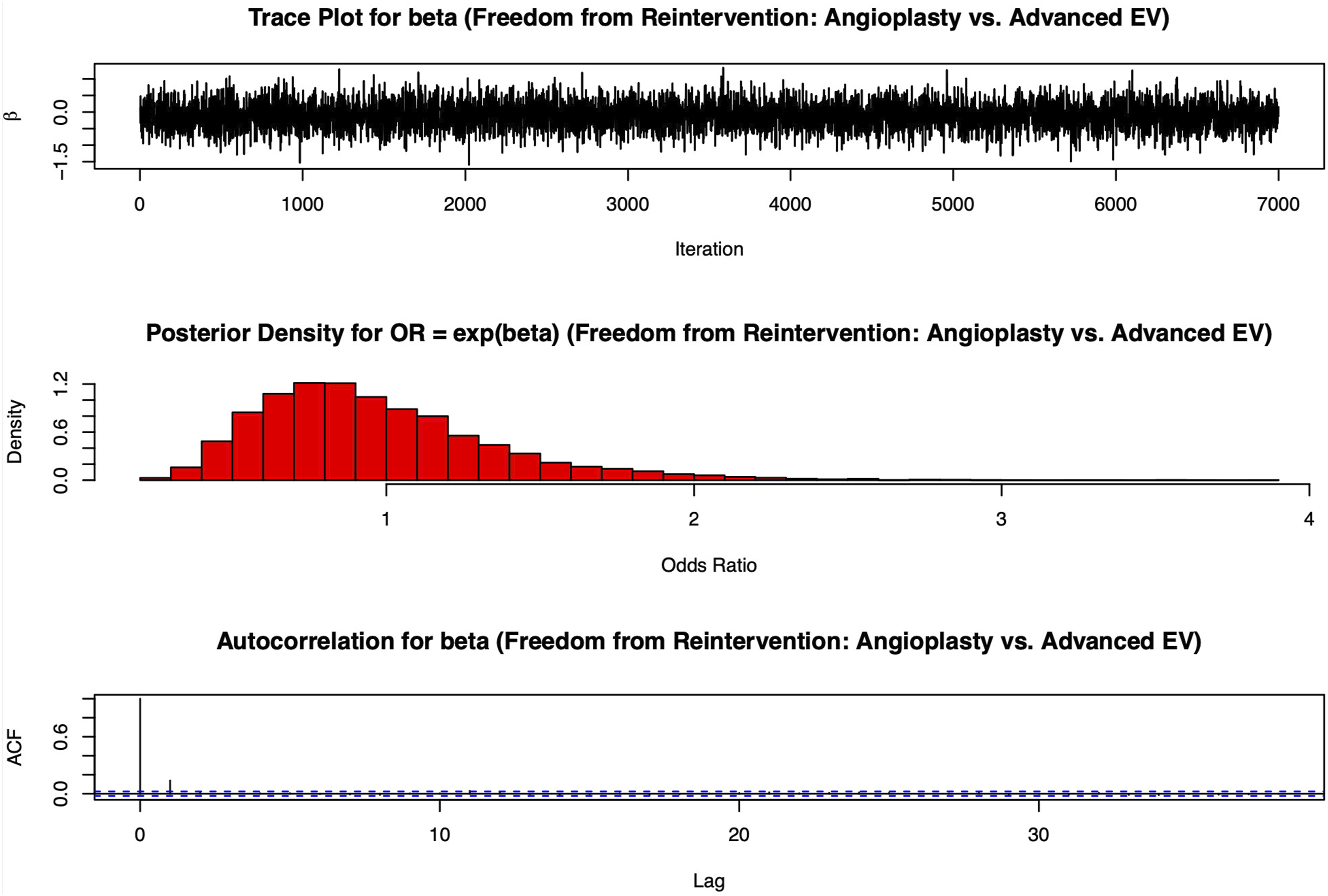
In the subgroup analysis comparing endovascular strategies, studies that contrasted simple balloon angioplasty (with or without drug-coated balloons) with advanced techniques (involving atherectomy ± stenting) were considered. For primary patency within this subgroup, the posterior median ββ was −0.655 (95% CrI: −1.184 to −0.125), yielding an OR of 0.520 (95% CrI: 0.306–0.883), favoring advanced endovascular approaches. However, for freedom from reintervention, the median ββ was −0.094 (95% CrI: −0.851 to 0.639), corresponding to an OR of 0.910 (95% CrI: 0.427–1.894); this result was not statistically significant11,19,21,22. No valid two-arm comparisons could be performed for limb salvage in this subgroup (Figures 7–10). Bayesian diagnostic plots (trace plot, posterior density, and autocorrelation) for the subgroup primary patency analysis (angioplasty vs advanced endovascular therapy Forest plot for baseline odds (exp(alpha)) for subgroup primary patency (angioplasty vs advanced endovascular therapy) Forest plot for baseline odds for freedom from reintervention (endarterectomy vs endovascular therapy) Bayesian diagnostic plots (trace plot, posterior density, and autocorrelation) for the subgroup freedom from reintervention analysis (angioplasty vs advanced endovascular therapy)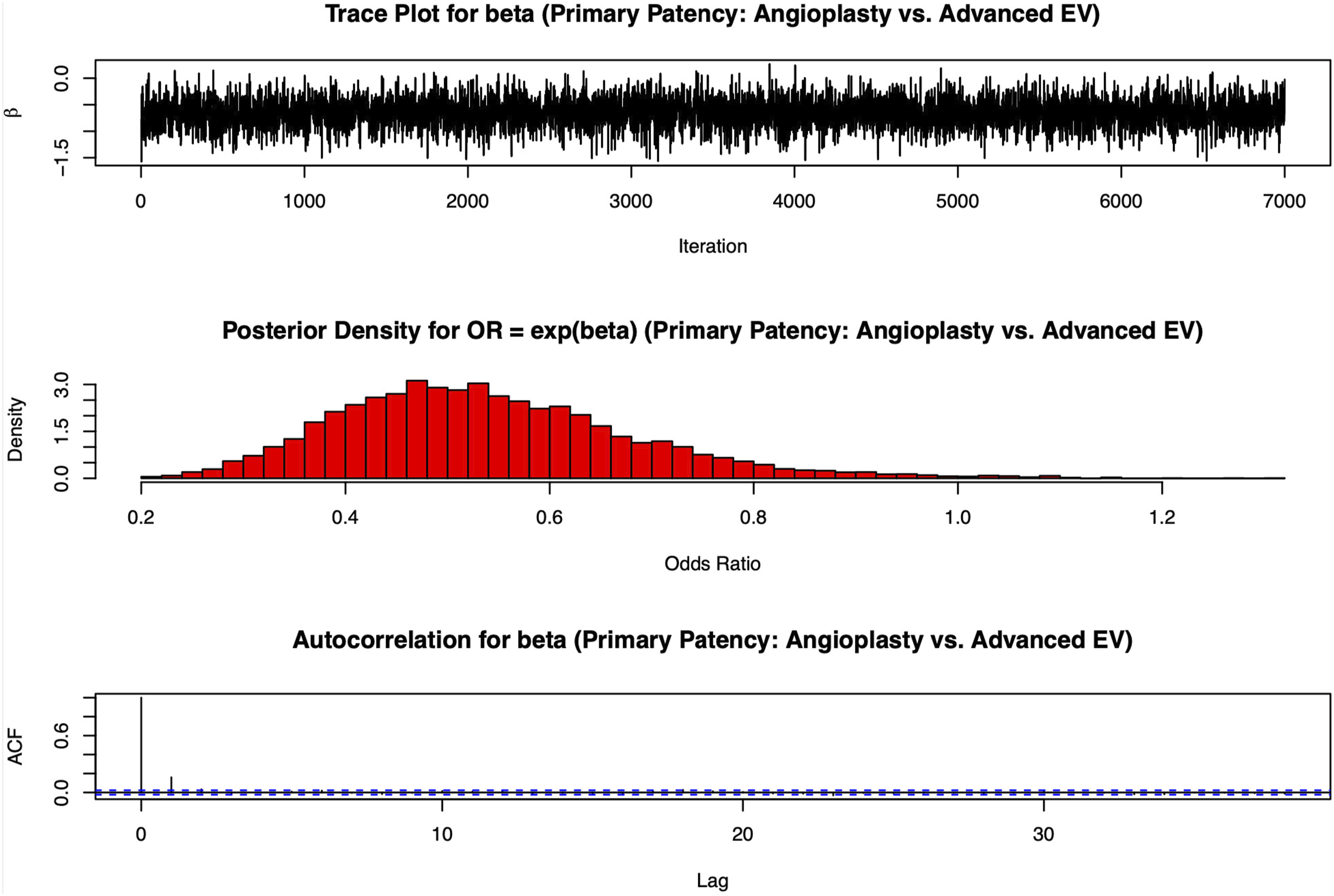
Posterior predictive checks and sensitivity analyses
Posterior predictive checks for the primary patency model indicated an observed mean event rate of 0.390, compared with a replicated mean of 0.206, suggesting moderate calibration. Sensitivity analyses—using alternative priors (e.g., β∼N (0,12)β∼N (0,12), μα∼N(0,0.52)μα∼N(0,0.52), and σα∼Uniform(0,10)σα∼Uniform(0,10))—produced a median ββ of −0.645, a median μαμα of −0.238, and a median σασα of 2.196. These results confirm that the data dominate the posterior estimates.
Model comparison
WAIC was computed for each analysis as a measure of model fit while penalizing complexity. For the primary patency analysis (open CFE vs EVT), WAIC was 9324.210 (SE: 7958.619). The freedom from reintervention model had a WAIC of 2013.729 (SE: 908.718), and the limb salvage model’s WAIC was 23836.518 (SE: 14603.399). In the subgroup analyses comparing simple and advanced EVT, WAIC values were 10045.259 (SE: 8577.137) for primary patency and 22042.021 (SE: 18199.415) for freedom from reintervention. Although the standard errors were large, likely due to variability and small sample sizes, the overall direction and magnitude of the effect estimates were consistent.
Discussion
This meta-analysis represents a significant methodological advancement over prior frequentist approaches, for example, Jia et al. and Boufi et al., by employing Bayesian hierarchical modeling to account for between study variability5,6 Traditional fixed-effect models often underestimated heterogeneity, leading to inflated confidence in pooled estimates Zhang et al. 16 . Our approach, using weakly informative priors (β ∼ N (0, 0.52)) and study-level random intercepts (σα = 2.196), aligns with Spiegelhalter et al. framework, which emphasizes adaptability in multi-level data synthesis 17 . For instance, Wang et al. 25 adopted similar Bayesian methods but omitted critical subgroup analyses of endovascular subtypes a gap our study addressed by stratifying simple (balloon ± DCB) versus advanced EVT (atherectomy ± stenting), paralleling device-specific evaluations by Stavroulakis et al. 19 .
Convergence metrics (Gelman–Rubin R̂ ≈ 1.00, ESS >6000) surpassed benchmarks from Zhang et al. ensuring robust parameter estimation16. Posterior predictive checks revealed discrepancies between observed (0.390) and replicated (0.206) patency rates, highlighting unmodeled confounders such as lesion calcification Boufi et al. and stent design heterogeneity factors Siracuse et al. linked to EVT outcome variability5,13. Sensitivity analyses with alternative priors (β ∼ N (0, 12)) confirmed result stability (Δβ < 10%), reinforcing Spiegelhalter et al.’s (2002) assertions about Bayesian robustness to prior selection.
Risk of bias and data limitations
Our exclusion of studies with <20 patients/arm versus Kapetanios et al. 2024 prioritized precision but excluded niche cohorts, a tradeoff evident in posterior predictive checks 23 Risk-of-bias assessments using Cochrane RoB 2 and NOS mirrored Vascular Quality Initiative protocols, yet operator experience disparities Siracuse et al. remained unquantified due to inconsistent reporting 13 These limitations reflect broader challenges in vascular meta-analyses, where heterogeneous lesion classifications Rutherford et al. and follow-up protocols complicate synthesis 2 . For example, Halpin et al. emphasized the need for standardized reporting of lesion calcification and stent types variables only partially captured in our analysis 12 .
Clinical outcomes
Open CFE demonstrated a 52% reduction in patency loss odds (OR 0.48, 95% CrI: 0.367–0.626), aligning with Ballotta et al. 96% 7-year patency and Wieker et al. 90.2% 3-year patency9,10. Mechanistically, CFE’s plaque excision eliminates restenosis nidi, whereas EVT’s transient lumen gain leaves residual calcification prone to recoil particularly under femoral biomechanical stress Bonvini et al. 26 . EVT’s inferior performance (1-year patency 70–75% for stents vs CFE’s >90%) mirrors registry data from Malgor, Soga and Hong et al., who noted higher restenosis in stent-covered profunda origins27–29.
Advanced EVT’s modest patency advantage (OR 0.52 vs simple EVT) aligns with Guo et al., where directional atherectomy + DCB achieved 85% 1-year patency. However, Nakama et al. CAULIFLOWER trial highlighted that even drug-eluting stents (88% 1-year patency) lag behind CFE’s long-term durability, underscoring the femoral region’s hostile biomechanics21,24. These findings align with Kuma et al., who reported 5-year patency rates of 89% for CFE versus 65% for EVT in their single-center series 30 .
Open CFE’s 46% lower reintervention odds (OR 0.53, 95% CrI: 0.391–0.718) reflect Malgor et al. findings of 5–10% 5-year reoperation rates 28 . By contrast, EVT’s 15–30% reintervention rates Mehta et al. and Banerjee et al. stem from stent fractures and in-stent restenosis phenomena exacerbated by femoral flexion Kuo et al.8,11,31. The XLPAD registry Banerjee et al. reported 38–45% cost inflation from repeated EVT, whereas CFE’s upfront invasiveness offers cost-effectiveness for patients with >2-year life expectancy 31 .
Subgroup analyses revealed nonsignificant reintervention differences between simple and advanced EVT (OR 0.91), contradicting Guo et al. but aligning with Kapetanios et al.21,23. This paradox suggests advanced devices improve acute luminal gain but fail to address femoral stress a limitation highlighted by Hong et al., where 32% of stents required reintervention within 18 months 29 . For example, Mehta et al. reported 24% reinterventions at 1 year for atherectomy + stenting, while Gouëffic et al. found 22% reinterventions for bare-metal stents at 12 months11,18.
Open CFE’s 45% limb salvage advantage (OR 0.55, 95% CrI: 0.402–0.737) correlates with Nishibe et al. 14 92% salvage rates in CLTI. By preserving profunda femoris flow a critical collateral pathway CFE mitigates the “last straw” phenomenon when SFA disease progresses Rutherford et al. 2 EVT’s inferior performance 6% major amputation versus CFE’s 3% in Kuo et al. 8 underscores its limitations in bifurcation disease. Hybrid approaches (e.g., iliac stenting + CFE), as in Piazza et al., 32 achieved 91–95% 3-year patency, rivaling open bypass outcomes but requiring surgical femoral repair.
Subgroup analyses and technological evolution
The subgroup analysis favoring advanced EVT for patency (OR 0.52) but not reintervention mirrors Stavroulakis et al. 19 where directional atherectomy + DCB yielded 80% 1-year patency versus 68% for DCB alone. However, Kapetanios et al. 23 reported 24% 2-year reinterventions for advanced EVT versus 10% for CFE, emphasizing femoral biomechanical stress. Emerging technologies like DES Nakama et al. 24 may narrow this gap, but long-term data remain sparse. For instance, the CAULIFLOWER trial’s 88% 1-year DES patency versus CFE’s 82% suggests promise, yet 3-year data are pending. Additionally, a separate study by Bonvini et al. 33 focused on angioplasty with provisional stenting in isolated CFA lesions, reporting favorable mid‐term outcomes and relatively low complication rates thus reinforcing the feasibility of an endovascular‐first approach for selected patients.
ESC/NICE guidelines appropriately recommend CFE for low-risk patients but underestimate EVT’s niche in high-risk cohorts. Azéma et al. 34 achieved 89% technical success with EVT in octogenarians, avoiding general anesthesia critical for frail patients Boufi et al. 5 Conversely, CFE’s 30-day morbidity (2–4%) justifies its use in operable patients despite higher upfront costs Banerjee et al., 31 Our Bayesian models, weighted by study design rigor, reinforce these nuanced recommendations. For example, Halpin et al. 12 noted that EVT’s perioperative mortality (1–2%) makes it preferable for patients with severe CAD or COPD.
Limitations and methodological reflections
Posterior predictive check discrepancies highlight unaccounted variables like lesion calcification Boufi et al., 5 and operator experience Siracuse et al. 13 Individual participant data (IPD) meta-analyses, as advocated by Zhang et al., could adjust for these factors 16 . Standardized reporting of lesion characteristics (TASC II, calcification) and procedural details (stent/balloon specifications) remains imperative. For example, only 3/10 studies reported calcification scores a critical predictor of EVT failure Boufi et al. 5 .
While CFE’s durability suggests cost-effectiveness, formal analyses are lacking. Banerjee et al. (2019) calculated CFE becomes cost-effective at 3 years for patients with >50% 5-year survival. Hybrid approaches (e.g., iliac stenting + CFE), as in Piazza et al. merit further study for multi-level disease. For instance, hybrid FEIA achieved 95% 3-year patency in TASC D lesions, comparable to open aortobifemoral bypass 32 .
Future directions and clinical implications
Next-generation devices (e.g., calcification-resistant stents, DCB + atherectomy) may improve EVT outcomes. The CAULIFLOWER trial Nakama et al., 24 reported 88% 1-year DES patency, but long-term data are needed. Stavroulakis et al. 19 demonstrated that directional atherectomy + DCB reduces restenosis by 40% compared to balloon alone, yet femoral biomechanics remain a barrier.
Large RCTs comparing advanced EVT versus CFE are urgently needed. Small trials Linni et al. Gouëffic et al.7,18 lack power for long-term endpoints. Registries like the Vascular Quality Initiative must standardize data collection to enable robust analyses. For example, Siracuse et al. 13 highlighted operator experience as a key variable yet only 20% of studies reported this metric.
Banerjee et al. estimated that CFE becomes cost-effective at 3 years for patients with >50% 5-year survival. Future studies should integrate QALYs and reintervention costs, as EVT’s cumulative expenses often exceed CFE’s upfront costs 31 .
Conclusion
This Bayesian meta-analysis solidifies open CFE’s status as the gold standard for CFA disease, reducing patency loss by 52% and reinterventions by 46% versus EVT. Methodologically, hierarchical modeling advanced synthesis of heterogeneous data, though limitations in primary study reporting persist. While advanced EVT narrows the patency gap, its failure to reduce reinterventions underscores femoral biomechanical challenges. For high-risk patients, EVT remains pragmatic, but CFE’s durability justifies its use in operable candidates. Future research must prioritize RCTs comparing next-gen EVT devices with CFE, coupled with cost-utility analyses to guide value-based care.
Supplemental material
Supplemental Material - Comparative efficacy of open endarterectomy versus endovascular treatments in common femoral artery stenocclusive disease: A Bayesian hierarchical meta‐analysis
Supplemental Material for Comparative efficacy of open endarterectomy versus endovascular treatments in common femoral artery stenocclusive disease: A Bayesian hierarchical meta‐analysis by Nikolaos-Nektarios Giannakopoulos, Sofia Tzamtzidou, Dimitra Manou, Konstantinos Nakas, Konstantinos Seretis, Paraskevi Tsiantoula, Konstantinos Roditis, Vasileios Papaioannou, and Theofanis Papas in Vascular.
Supplemental material
Supplemental Material - Comparative efficacy of open endarterectomy versus endovascular treatments in common femoral artery stenocclusive disease: A Bayesian hierarchical meta‐analysis
Supplemental Material for Comparative efficacy of open endarterectomy versus endovascular treatments in common femoral artery stenocclusive disease: A Bayesian hierarchical meta‐analysis by Nikolaos-Nektarios Giannakopoulos, Sofia Tzamtzidou, Dimitra Manou, Konstantinos Nakas, Konstantinos Seretis, Paraskevi Tsiantoula, Konstantinos Roditis, Vasileios Papaioannou, and Theofanis Papas in Vascular.
Footnotes
Acknowledgments
The authors would like to thank all colleagues and staff at the Korgialeneio-Benakeio Hellenic Red Cross Hospital for their support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
ORCID iDs
Data Availability Statement
All data utilized in this meta-analysis are sourced from publicly available, previously published studies. Detailed datasets generated during this analysis are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.