
Abstract

PRECIS
This report illustrates allergic contact dermatitis (ACD) to clotrimazole in a patient with long-standing history of stasis dermatitis of the lower legs.
DISCUSSION
A 65-year-old male presented to our clinic with a 4-year history of stasis dermatitis of the lower legs. Past treatments included topical steroids (triamcinolone 0.1% cream/ointment, desonide 0.05% cream, hydrocortisone 2.5% cream/ointment), topical antifungals (clotrimazole 1% cream, ketoconazole 2% cream, miconazole 2% cream, nystatin powder), and one topical antibiotic (mupirocin 2% ointment). Two to three months prior to his patch testing, the patient’s dermatitis progressed with more intense erythema, scale, and weeping, raising concern for a possible superimposed contact allergy and prompting referral for patch testing (Fig. 1).

Severe deeply pink and scaly dermatitis of the right lower leg. Similar rash on left lower leg not pictured.
Patch testing was performed using the North American Contact Dermatitis Group standard series, as well as our clinic’s personal care product, preservative, and emulsifier series (SmartPractice, Phoenix, AZ; Chemotechnique, Vellinge, Sweden). Each of the patient’s previously used topical medications was additionally tested “as-is.”
Initial patches were applied to unaffected skin on the patient’s back using Finn Chambers (SmartPractice). They were removed after 48 hours. Both the 48-hour and day 5 readings demonstrated significant irritant reactions to the patient’s Lotrimin® AF clotrimazole cream (Fig. 2), prompting additional testing to our clinic’s antifungal series. The final (day 5) reading of this series was notable for a 3+ spreading reaction to the active ingredient in the patient’s home antifungal cream, clotrimazole 1% petrolatum (pet) (Fig. 3). He did not react to any of the commercially available inactive ingredients in this cream (benzyl alcohol, cetyl alcohol, stearyl alcohol, various sorbate derivatives); however, cetyl esters wax and octyldodecanol were not available for testing. In addition, the patient did not react to any of the other allergens on our antifungal series (nystatin 2% pet, ketoconazole 2% cream, tioconazole 1% pet, miconazole 1% alcohol, econazole 1% alcohol, selenium sulfide 2.5% lotion), as evidenced by sparing of the other disc spaces in Figure 3.
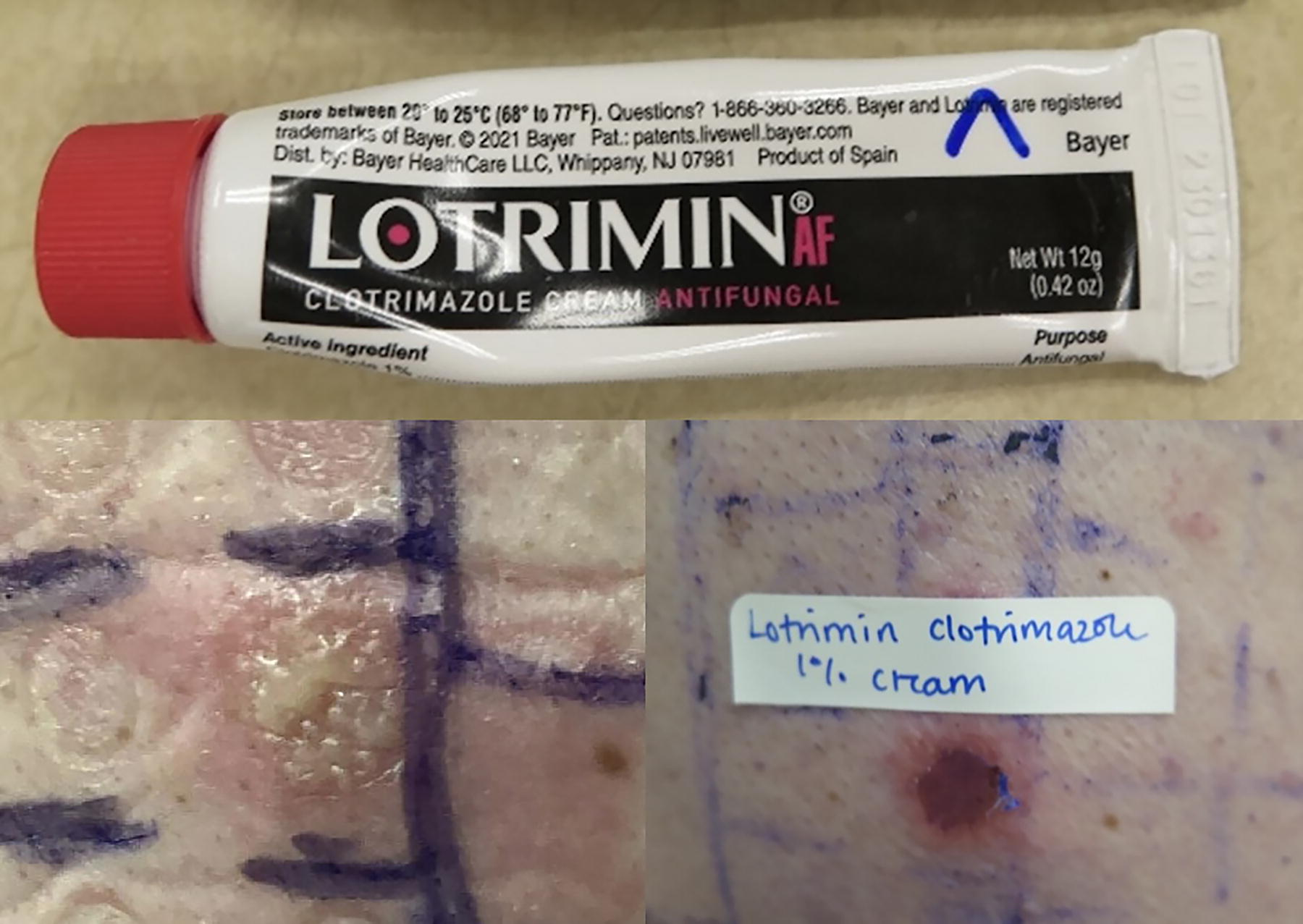
Irritant reactions to patient’s home product, Lotrimin® AF clotrimazole cream. Forty-eight-hour reading (left). Day 5 reading (right).

Final antifungal series reactions read on day 5, notable for a 3+ spreading reaction to clotrimazole 1% petrolatum and sparing of other disc spaces.
Although as-is testing with the patient’s home antifungal cream resulted in an irritant reaction, testing with purified clotrimazole revealed true contact allergy, as demonstrated by the erythema, edema, and vesiculation in Figure 3. Clotrimazole belongs to the imidazole class of antifungal medications. It is commonly incorporated into topical preparations used to treat tinea and candida infections of the skin. 1 Because this medication is available over the counter (OTC), it is widely accessible to consumers and is often used as initial self-treatment for skin rash prior to formal dermatologic evaluation.
Our patient had self-started Lotrimin AF clotrimazole cream in the preceding months prior to the worsening of his stasis dermatitis. He was never prescribed or instructed to use this medication, which emphasizes the importance of thoroughly investigating all prior topical medication use during patch testing evaluation rather than relying on the electronic medical record alone.
ACD to clotrimazole is rare, with most reported cases involving the genital area.2B3 -5 Some reports have noted cross-reactivity between clotrimazole and other imidazoles, including miconazole, itraconazole, and croconazole.2,3 However, in our case, as well as cases published by Pullen 4 and Kalb, 5 reactions were significant for contact allergy to clotrimazole only, permitting the use of other imidazoles if patients have tested negative to them.
ZEBRA
ACD to clotrimazole exists; inquiring, inspecting, and testing to OTC and prescription topical medications, in both their commercial/purified forms, is of utmost importance.