
Abstract

To the Editor:
Acute localized acute exanthematous pustulosis (ALEP) is a relatively rare and newly recognized condition, first described by Prange et al. in 2005. 1 It was identified in a patient who exhibited a facial rash that also fulfilled the diagnostic criteria for AGEP. Because of its clinical and histological similarities, ALEP is now regarded as a localized variant of AGEP, typically triggered by a hypersensitivity reaction to either conventional or herbal systemic drugs. In some cases, it has also been associated with contact mechanisms. We have read with great interest the recent case by Korbi et al., describing AGEP induced by jellyfish sting, and we herein report a case of ALEP induced by jellyfish. 2
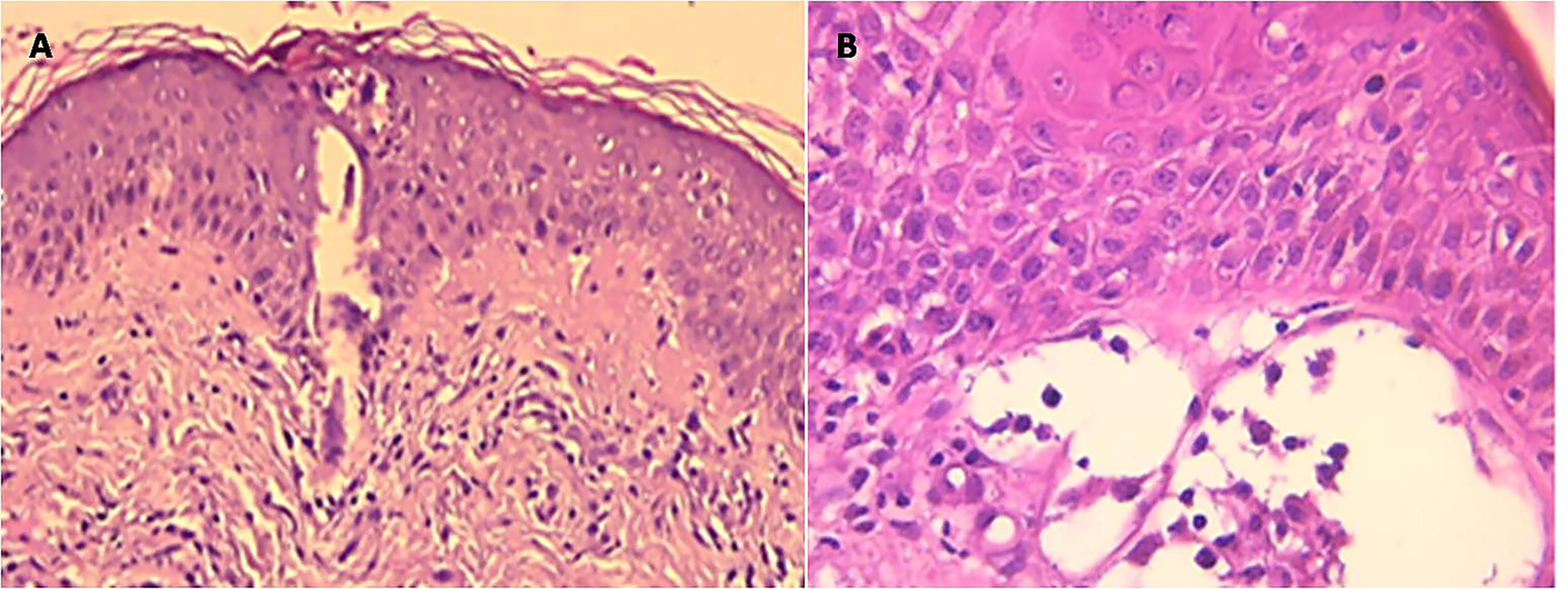
A 26-year-old woman, with no significant medical history, no known drug allergies, and no recent medication use, was stung on the neck by a jellyfish while swimming in the Mediterranean Sea. Within 48 hours, she developed sharply demarcated erythematous plaques on the lateral neck, extending to the mandibular and lower facial regions. These plaques were covered with numerous small, sterile, non-follicular pustules (Fig. 1). The eruption was mildly pruritic but painless, and there was no fever, mucosal involvement, or systemic symptoms. Routine laboratory investigations, including complete blood count and liver function tests, were normal. Bacterial cultures from pustular swabs yielded no growth. A skin biopsy revealed intraepidermal sterile pustules with a predominantly neutrophilic infiltrate (Fig. 2). Based on the clinical presentation, absence of systemic drug exposure, negative cultures, and histopathological features, the condition was classified as ALEP according to adapted EuroSCAR criteria.

Erythematous plaques covered with non-follicular pustules on the neck and face.
ALEP is increasingly recognized as a topographically restricted variant of acute generalized exanthematous pustulosis (AGEP), first delineated by Prange et al. in 2005. 1 While AGEP is typically drug-induced, ALEP remains rare, and non-drug-related triggers are only exceptionally reported. A few isolated cases have been attributed to arthropod bites, such as mosquitoes or spiders, suggesting that direct cutaneous insults may reproduce the immunopathological pathways observed in drug-induced pustuloses. 3
More recently, cnidarian stings have emerged as novel precipitants. Korbi et al. reported an AGEP triggered by Rhizostoma pulmo, whereas Ben Salah et al. described the first case of ALEP following a jellyfish sting.2,4 Our case further supports this emerging evidence and, to our knowledge, represents one of the very few histologically confirmed instances of ALEP induced by cnidarian venom. The strictly localized distribution, rapid and self-limited course, and biopsy-proven sterile intraepidermal pustules were highly consistent with this diagnosis.
From a pathophysiological standpoint, ALEP is thought to share the same mechanisms as AGEP, mediated by a type IVd hypersensitivity reaction. 5 Activated T cells release cytokines such as interleukin-8 and granulocyte-macrophage colony-stimulating factor, promoting massive neutrophilic recruitment and pustule formation. 5 In cnidarian stings, nematocyst-derived proteins and peptides exert a dual effect: direct cytotoxicity and immune activation, including mast cell degranulation, complement activation, and delayed T-cell-mediated responses.6,7 This combined mechanism provides a biologically plausible explanation for the development of ALEP in our patient.
Recently, a unifying concept has emerged proposing that AGEP and generalized pustular psoriasis represent 2 entities within a shared spectrum of “IL-36–driven pustulosis,” characterized by overlapping clinical, histological, and transcriptomic signatures. In this framework, ALEP may be considered the localized counterpart of AGEP within the same IL-36–mediated inflammatory continuum. Although molecular data are not yet available for ALEP, its identical histopathological pattern and acute, self-limited evolution strongly suggest that IL-36 signaling could also play a key pathogenic role in its development. 8
The differential diagnosis primarily includes infectious pustular eruptions. Distinguishing features of ALEP include the absence of systemic involvement, negative bacterial cultures, and rapid resolution under potent topical corticosteroids. Other differential considerations include impetigo, pustular psoriasis, and AGEP itself. In our case, the localized nature of the eruption, absence of systemic symptoms, and histopathological findings were decisive.
Management is straightforward. High-potency topical corticosteroids usually achieve rapid clearance within a few days. Recognizing ALEP in this setting is clinically relevant, as it prevents unnecessary systemic treatments, particularly antibiotics, and reassures both physicians and patients regarding the benign and self-limiting nature of the condition.