
Abstract

As Canadians await action on renewal of our much-debated health care system, learning from the successes of other countries has never seemed more timely. While the primary health care movement evolves in Canada we can examine best practices elsewhere to assist us in improving our own quality improvement mechanisms, as well as give us insight into how best to position the role of the pharmacist in our own health care system.
A delegation from Saskatchewan travelled to the United Kingdom (November 15 to 22, 2003) to learn about recent changes to the provision of primary health care within the National Health Service (NHS). Our delegation consisted of an assistant deputy minister of health and the executive director of primary health care from Saskatchewan Health; officers from the regulatory bodies for pharmacy, medicine, and nursing (including R.J.); a community pharmacist (G.S.); a primary care pharmacist (S.L.N.); two nurse practitioners; six family physicians; and the chair of Saskatchewan's Health Quality Council.
Our mandate was accomplished by intense observation of and dialogue with the staff in existing primary care practices and members of local health care cooperatives, and consultation with the National Primary Care Development Team and Primary Care Trusts.
The National Primary Care Development Team was established in 2000 to develop the capacity and capability of individuals and organizations to make improvements to patient care. They support and engage providers in programs which ensure rapid, systematic, and sustainable improvement in health care provision.
National Health System
The NHS has been developing services as a national agency for more than 60 years. Under the previous NHS structure, practices held funds for care of their rostered (registered) patients. Each practice received a monetary sum from the NHS to cover the medical needs of its patients. The practice then “purchased” services, such as radiology services, surgical procedures, and laboratory testing, on behalf of the patients, from other parts of the health care system.
The system failed if a patient or a practice reached the upper limit of available funding before the end of the year. At that point, required services would be deferred to the next budget year. Provision for emergency care was built into the system, but non-emergent or elective care was often associated with untimely delays that were deemed unacceptable by both patients and taxpayers.
In the early 1990s the system underwent a massive overhaul, which shifted the focus to preventive health care. National objectives were set (e.g., a patient should be able to see his or her own physician within 48 hours, 1 evidence-based prevention of coronary artery disease should be available 2 ), with the onus falling to primary care mechanisms to fulfill these expectations. The NHS established 18 Regional Health Authorities in the United Kingdom, with a total of 337 Primary Care Trusts (PCTs) operating under their auspices (Meera Kulkarni, National Primary Care Development Team, Manchester, UK; personal communication, November 21, 2003).
Each Regional Health Authority assumes the overall budget for all PCTs within its region, while each PCT is responsible for primary health care for the population it serves (about 100,000 people). It should be noted that, as in Canada, health budgets are broken down into “silos” of care, such as mental health, acute care, drugs, and primary care. However, the UK system is making strides in integrating these silos to achieve greater efficiencies in care delivery. It remains the goal of the NHS to further develop national objectives in the management of chronic disease states similar to those that have been established for coronary artery disease (Dr. Peter Godbehere, North Cambridgeshire, UK; personal communication, November 21, 2003).
Primary care practices
In the United Kingdom, primary health care is delivered by interdisciplinary practices. Patients are rostered to a particular practice and choose from among the different primary care providers within it. 2 Thus, a patient might choose to always see a nurse practitioner; alternatively, practice team members might collaborate on appropriate care for a given problem or need. Through patient rostering, primary care practices are held accountable to the patient for acceptable health outcomes and to the PCT for achieving NHS-established targets.
Integral to the model are the compensation scheme and the support provided to the practices. The practices are paid by a weighted capitation model, with financial incentives built into the contract for the achievement of quality-related outputs and outcomes. 3 The NHS sets the objectives or priorities, and the individual practices develop their own individualized plans for meeting those objectives. 2
The PCT to which the practice belongs (and the National Primary Care Development Team) support the practice in achieving the objectives. This support includes information technology, change modelling, linkage to other related services (e.g., addiction counselling services, home care nursing), collaboration among similar practices, and facilitation services to implement quality-focused change. It extends to dedicated time each week for learning and development when team members determine how they will measure an outcome, develop strategies for changing their practice to realize that outcome, and report back on their successes and failures.
Primary care teams ensure that every patient achieves risk-reduction targets
PLAN, DO, STUDY, ACT
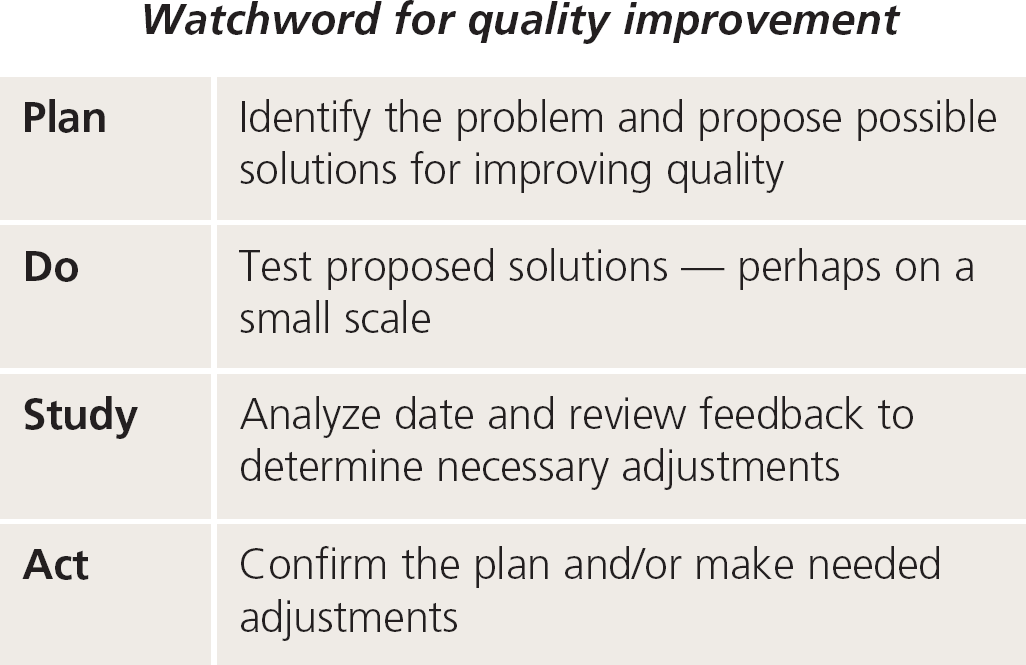
This four-step process for continual improvement is widely cited in National Health Service materials, and has been adapted by many North Americans involved in quality control.
For further information: www.modern.nhs.uk/serviceim-provement/1338/4668/5970/Doncaster%20Boards.pdf
Teams use the PDSA model (plan, do, study, act) to study the impact of a change, and quickly incorporate, amend, or abandon the strategy. 2 Their motto is “pursuing perfection.” As an example, our study group observed practices that repeated the PDSA approach (see box below) until every patient within their rostered populations had achieved the NHS risk reduction targets for coronary artery disease. The PCTs and the National Primary Care Development Team never attempt to define a “one-size-fits-all” initiative, nor do they try to impose the same change model across all practices. 2 Instead, they work with those innovative practices/practitioners who are interested and internally motivated to solve a practice-related problem.
Capturing best practices
When a practice develops a solution to a common problem, the team members are recognized by being asked to become “the experts” for that particular problem. Through the Primary Care Collaboratives, other practices that want to solve a similar problem benefit from the previous experience; however, they are allowed to adapt the solution to fit their own circumstances.
This fostering of innovation and ground-level approach to the provision of care lends itself well to the diverse populations within a PCT. For example, programs for indigent people in the PCT will differ significantly from those within more affluent areas, in that programs in impoverished areas must be linked with non–health-care intersectoral partners (i.e., social services, justice, education).
Clearly, this is a system in which all disciplines practice to the full extent of their expertise and capabilities. Territorialism, restriction to traditional job descriptions, and maintenance of the status quo were not observed in the practices we visited. In most cases, without formal introductions we could not distinguish among the different care providers until they described their roles. In addition, patients play an integral role in helping to define initial health care policy directions, as well as providing feedback.
Embracing quality
Most remarkable to us is the organizational culture associated with the care delivery model. Primary health care was patient-centred and outcome-focused, and the quality improvement is embraced by everyone, from the receptionists and the practitioners, through the leaders and managers, to the health policy-makers.
While continuous quality improvement is common-place in the institutional setting within Canadian health care, it is not followed systematically in the primary care setting. In contrast, the primary care practices we visited in the United Kingdom illustrated uptake of evidence-based guidelines, improvement in patient satisfaction, implementation of community preventive health initiatives, and implementation of the NHS goal of a maximum 48-hour wait for patients to see their physician. These goals were achieved through bottom-up approaches to which the practices are truly committed, rather than through top-down enforced changes. 2
Comparing UK, Canada
In reflecting on our study tour, we realize that Canadians have much to be proud of in our own health care system, but also that there is much to learn from the successes of others. In general, the role of the pharmacist in the health care system is more advanced in Canada, whereas integration of the pharmacist as a member of the primary care team is more advanced in the United Kingdom.
Canadian pharmacists take a more proactive role in establishing their place in the primary health care system than do UK pharmacists. There are many examples of best practices in Canada where pharmacists provide risk assessment or management for chronic disease, 6 –9 disease-based education programs, 6 –8,10 and pharmacotherapy assessment and monitoring within community pharmacies. 11 Primary care studies of pharmacist-directed initiatives to close the gap between clinical practice guidelines and current practice have been conducted in community pharmacies. 9,11 Some practices have tried to physically connect pharmacists and prescribers in collocated practices. 12 –16
Finally, academic detailing by pharmacists is also a well-developed part of Saskatchewan's primary health care environment, with the RxFiles program being expanded to more communities within the province; similar programs are in place in Alberta, British Columbia, and Nova Scotia.
PHARMACISTS AS SALARIED CONSULTANTS
We observed two major roles for pharmacists in the NHS: traditional community pharmacy practice and a salaried or contracted advisory or consultancy role for the PCTs. 4,5
Community pharmacists
Community pharmacist practice activities are similar to those in Canada — dispensing prescriptions, self-medication assessments and consultation, and health promotion. Pharmacists still receive remuneration on a per-prescription basis; however, alternative reimbursement is used in a few situations, such as nonprescription nicotine replacement products, smoking cessation counselling and monitoring, risk assessment with point-of-care testing, disease-state education (e.g., asthma), and methadone maintenance programs. PCT-employed or contracted pharmacists included academic detailing (educational outreach), management of formularies and prescribing guidelines, interdisciplinary communication, patient advocacy, research coordination, and planning in their work.
Salaried consultant pharmacists
In Glasgow we encountered a community pharmacist who had been hired by the PCT on a per diem basis to act as a liaison between the PCT, the primary care practices, and community pharmacists. We visited one of his projects in a highly deprived area to observe a newly renovated pharmacy (for which the PCT had provided 25% of the funds) designed to enhance the delivery of PCT programming such as methadone maintenance therapy. The pharmacy was well equipped with a counselling room for patients to meet with social service workers, a patient Internet station, and a small examination room where itinerant care providers could meet patients.
Academic detailing
Each primary care trust employs a number of pharmacists as outreach educators for academic detailing to prescribers. The pharmacists receive quarterly prescriber-specific data for use in educating prescribers about their prescribing habits, including comparisons with PCT and national averages. Physicians receive data on the monetary value of the medications they have prescribed and a breakdown of prescriptions according to therapeutic category, and variance from local and national norms.
Audit data on drug-use variances are not seen as punitive
In addition to the audited data, verbal education accompanied by written materials is provided on a specific theme. We met with several physicians to discuss this service. We learned that the pharmacists were highly regarded by the physicians, and the prescribers found the audit data most helpful in their practices. Indeed, the audited data has no punitive connotations — two physicians willingly showed us their own data.
A significant issue for Canadian pharmacists is the lack of sustainable funding. While it is often possible to obtain grants for pilot projects or studies whose results support the value of pharmacists within our system, there is at best a significant time lag between the reported results of a pilot and its expanded implementation, and at worst discontinuation of the work because of lack of compensation. Pharmacists must improve efforts to disseminate information about their work and to lobby government and third-party payers so as to obtain the types of remuneration schemes (i.e., sessional fees, fee-for-service, salary) that they feel are appropriate.
For more information about the study tour, contact the Saskatchewan Health Quality Council (
Lessons learned
Ensuring that we will be involved as team members as the primary health care movement takes hold requires that we position ourselves and market the important role of the pharmacist. In the United Kingdom, each community values its pharmacists because of the well-established therapeutic relationships they share, with excellent access to pharmacists.
The communities' involvement in the planning and delivery of services means that they recognize the important role of pharmacists in their health care, and ensures that pharmacists are welcomed as members of the primary care team. An optimized role rather than expanded scope of practice for pharmacists is actively sought and respected. The leaders within the profession seem to understand specific practice issues, while practitioners seem to understand the vision and goals of the leadership. This mutual trust results in a system that balances current business realities with the aspirations of the profession and the needs of the Primary Care Trusts. It was no coincidence that the NHS selected the term “Trust” in naming these organizations.