
Abstract
Background:
The Multistakeholder Framework of Rurality project was funded by Health Canada's Rural and Remote Health Innovations Initiative. The aim of this project was to develop a tool to assist rural communities with health human resource planning and to help governments and communities in recruiting and retaining health care providers in rural and remote communities.
Methods:
A national survey was sent to nurses, physicians, and pharmacists living in rural or remote communities to determine, among other factors, satisfaction with their personal and professional lives in those communities. One of the questions asked in the survey was “Do you plan to be in practice in the community in two years?”
Results:
Completed surveys were returned by 1019 pharmacists. Pharmacists who were married, had children living at home, were between the ages of 35 and 54 years, and had between 6 and 24 years in practice were more likely to say they would remain in the community. Communities where there were better working hours, better availability of coverage and backup, higher earning potential, and greater opportunities were more likely to retain pharmacists, as were communities where there were better opportunities for family members. Pharmacists were also more likely to state an intention to remain in communities where they had a sense of belonging and a sense of being appreciated. Multivariate predictors of pharmacists' intent to remain were children living at home, professional factors, and personal factors.
Conclusions/Implications:
Despite some study limitations, the results presented here could be used to help communities select pharmacists who are most likely to remain in practice in the communities for longer periods. Community attributes such as distance to large population centres cannot be changed, but attributes that contribute to personal and professional satisfaction could be altered.
Despite the current significant shortage of pharmacists in Canada and other English-speaking countries, the published literature discussing retention and recruitment issues for pharmacists is minimal compared with that for physicians and nurses. As in the other health professions, the distribution of vacancies in pharmacy is uneven, with more vacancies in Manitoba, British Columbia, Ontario, and Quebec, particularly in the rural areas of those provinces. 1 Rural areas appear to have more difficulty attracting and retaining pharmacists, but this observation has not been well documented or systematically analyzed.
Although strategies to improve recruitment of health professionals are often discussed when the issue of shortages arises, retention strategies may be of even greater importance. The presence of health professionals with longer tenures illustrates the desirability of the community to professionals considering positions in that community. As well, replacing health professionals is costly, in terms of both financial resources (because of severance, rehiring, and training) and human resources.
Research to date
Research on the retention of health professionals in rural areas has focused either on tracking the in- and out-migration of health professionals or on the reasons that health professionals leave or choose to remain in rural communities. Most of this research has been done in Australia and the United States, although a few Canadian studies have been published. A physician's satisfaction with and attachment to the rural community in which he or she works is a fairly consistent predictor of intent to remain in the community. 2 –5 Community attachment as a predictor of retention has not been as consistent in studies of nurses; Pan et al. 6 found that job satisfaction followed by satisfaction with the community predicted the likelihood of a nurse leaving his or her position in a rural community. Conversely, neither of these factors influenced the retention of public health nurses in British Columbia. 7
Another fairly consistent predictor of a physician continuing to work in a rural community was relief coverage 8 and on-call arrangements. 3,9 Professional autonomy did not appear to influence physicians' decisions to remain in a community 2 but may predict retention for nurses 7,10 and for physical therapists. 11 Professional isolation, including lack of opportunities for professional education and for relationships with other health professionals, was mentioned by physicians, nurses, and physical therapists working in rural or remote communities. 11 –13 With the exception of one survey of American nurses, 6 personal characteristics and distance of a community from urban centres were not or were only weakly associated with retention. 9,10,13
Predicting intention
In 2001, the Canadian Medical Association, the Canadian Nurses Association, and the Society of Rural Physicians of Canada received funding from the Rural and Remote Health Innovations Initiative of Health Canada to develop a health human resources tool called the “multistakeholder framework of rurality.” It was intended for use in human resource planning or to help recruit or retain health care providers for rural and remote communities. 14 As part of the process of creating this tool, an eight-page survey was developed and mailed to pharmacists, nurses, and physicians practising in rural and remote areas of Canada.
This paper reports a secondary analysis of the data collected from the survey. The aim of the secondary analysis was to determine how to predict rural pharmacists' intent to remain in practice in their communities.
KEY POINTS
Pharmacists who are more satisfied with both professional and personal aspects of living and working in a rural community are more likely to remain in practice in that community. Broad, integrated strategies are needed to ensure that pharmacists remain in their rural communities. Involving rural communities along with other stakeholders can be effective in both the recruitment and retention of health professionals.
Results
Completed surveys were returned by 1019 pharmacists (40%) representing all provinces and territories. Response rates varied by region and were lowest for pharmacists in New Brunswick and highest for those in the territories. The mean age (± standard deviation) of respondents was 47 ± 11 years, and 45% were female. The majority of the pharmacists (77%) were living in the rural or remote community in which they worked, and most (87%) were married. On average the respondents had worked in the community 15 ± 10 years, and 88% said they planned to be practising in the community in two years. The majority of the pharmacists were employed in community pharmacies (88%), while 10% worked in hospitals and 2% worked in both hospital and community pharmacies.
METHODS
The survey was mailed to a random sample of 2524 pharmacists living in rural and remote Canadian communities. Rural communities were defined as being outside a census metropolitan area or a census agglomeration.
The survey instrument was designed by the Steering Committee of the project, with input from a range of rural health care providers. Although the instrument was piloted before use, it has not been validated, nor has its reliability been assessed. The survey instrument comprised seven sections with questions in the following areas:
General (time in practice, community size and location) Satisfaction with rural practice Health care services in the community Health human resources in the community Collaborative and team models Telehealth Personal characteristics.
For the purposes of this secondary analysis, responses to only a subset of the survey questions were used. One of the questions asked in the survey was: “Do you plan to be in practice in the community in two years?” The following data, also collected in this survey, were used to determine how to predict a health professional's intent to remain in the community in which he or she was working at the time of the survey:
Respondents' demographic characteristics Community characteristics (size, distance from urban centres) Respondents' satisfaction with professional and personal aspects of working in the community.
A factor analysis was done to produce a smaller number of variables consisting of similar questions within each of the ten professional satisfaction and seven personal satisfaction questions. Three principal components were generated from questions related to professional satisfaction. These had eigenvalues of 4.400, 1.175, and 1.071, accounting for 66.49% of the variance in these ten questions. Variables in the above factors were combined to produce three new variables relating to levels of satisfaction with professional aspects of health professionals' work: availability (presence) of backup, coverage and consults, and time and money. For questions relating to personal satisfaction, two principal components were generated, with eigenvalues of 3.468 and 1.212, accounting for 66.85% of the variance in the seven questions. Variables in the above factors were combined to produce two new variables relating to levels of satisfaction with the personal aspects of health professionals' work: opportunities and community.
χ2-tests and independent t-tests were used, for categorical and interval or ratio variables, respectively, to test for differences between those who planned to stay and those who did not. Multivariate, hierarchical logistic regression analysis was then performed using only variables with p-values less than or equal to 0.15. The −2 log likelihood was used to check the incremental benefit (gain in prediction accuracy) of adding community factors to personal factors in the model.
Univariate predictors
The attributes of pharmacists who said they intended to remain were compared with those of pharmacists who said they did not intend to remain by means of independent t-tests (age) and χ2-tests (all other variables) (Table 1). Both marital status and the presence of children at home predicted respondents' intent to remain in practice in the same community. Most pharmacists who stated that they intended to remain had been in practice between 6 and 24 years (62%); only 34% of those who intended to leave had been practising for this duration. Twenty-one percent of those who had been practising for five years or less intended to leave, whereas only 7% of pharmacists in practice between 16 and 24 years and 19% of those in practice for 25 or more years intended to leave. The mean age of respondents intending to remain was lower, but the relation between age and intent to remain was curvilinear, with respondents older than 64 years least likely to remain in practice and those between 35 and 54 years most likely to remain.
Univariate analysis of pharmacist attributes
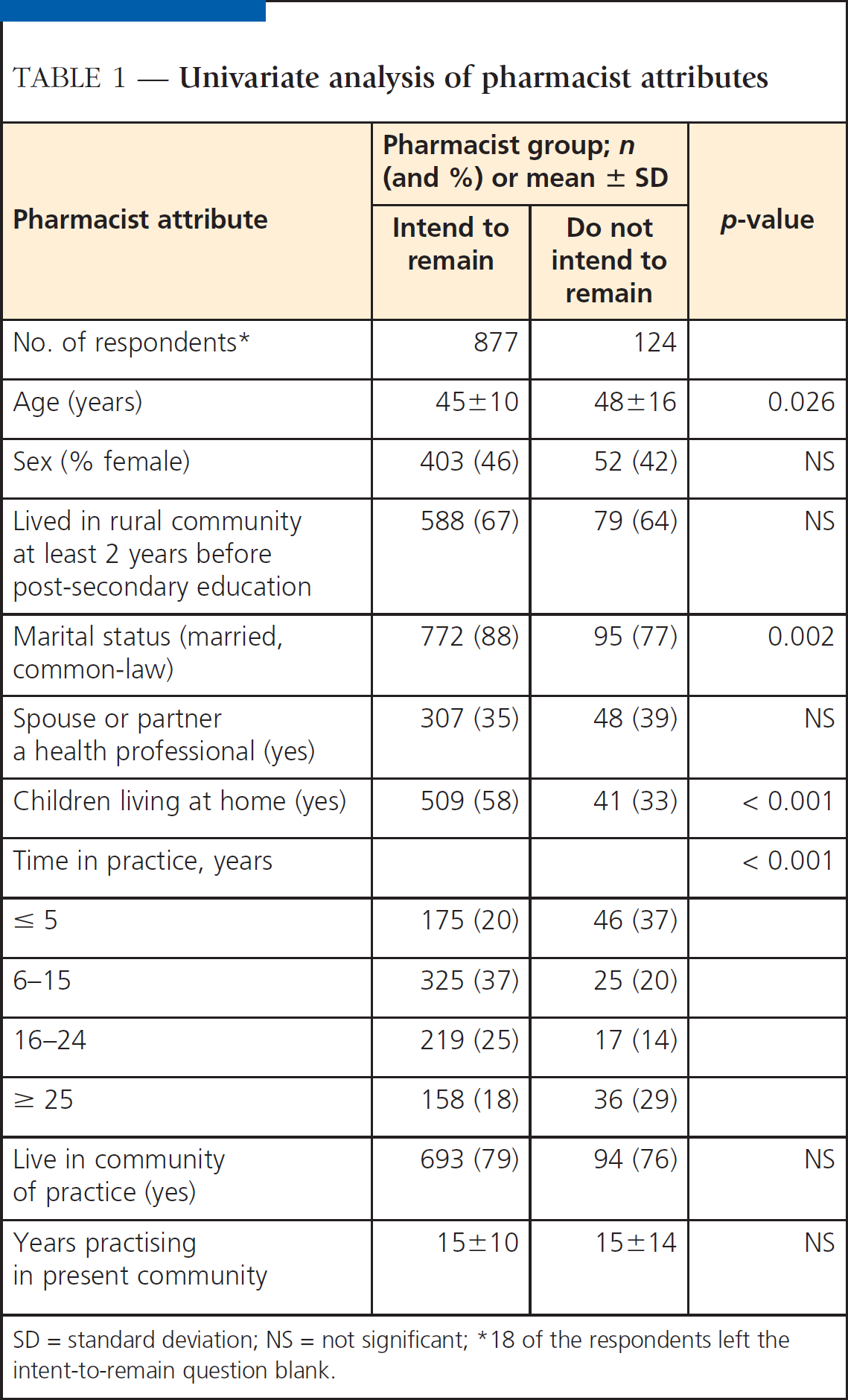
SD = standard deviation; NS = not significant;
18 of the respondents left the intent-to-remain question blank.
Independent t-tests were used to compare community attributes and satisfaction with various aspects of practice and the community for pharmacists who said they intended to remain and those who did not (Table 2). Although neither the size of the community nor the size of the catchment area predicted intent to remain, distance to a larger population centre did. The greater the distance, the lower the proportion of pharmacists who said they still intended to be in practice in that community in two years. Higher levels of satisfaction with all of the professional and personal factors (with the exception of availability of backup) predicted the intent to remain.
Univariate analysis of pharmacist attributes
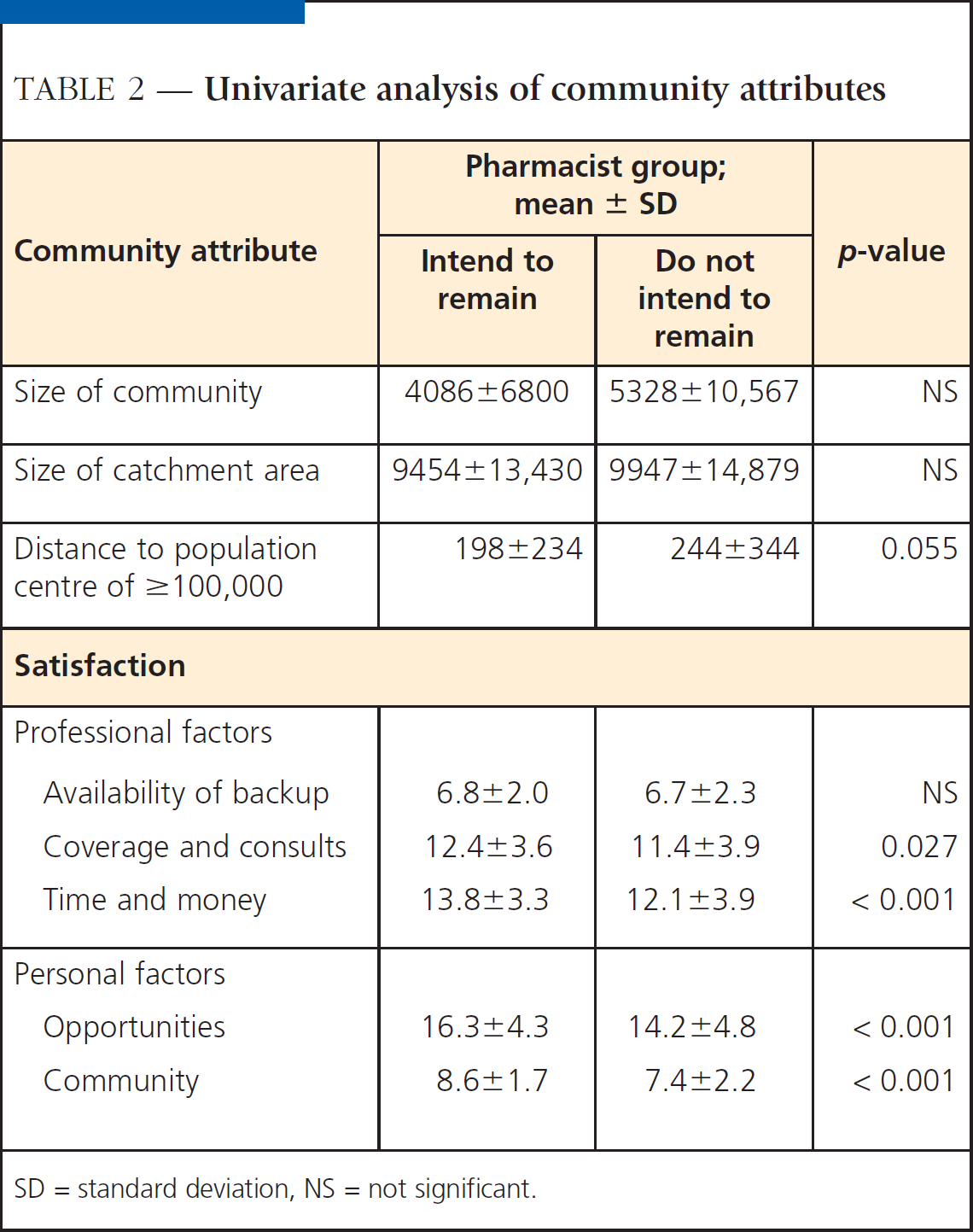
SD = standard deviation, NS = not significant.
Multivariate predictors
Measures of satisfaction may relate to overall satisfaction and may be highly correlated with one another, which could lead to problems of multicollinearity when multivariate analysis is performed. Factor analysis with a varimax rotation should produce orthogonal factors and avoid this problem, but bivariate (Pearson) correlations were calculated anyway, to ensure that there were no correlation coefficients higher than 0.7 between the measures of satisfaction. All variables measuring satisfaction were significantly and moderately correlated, but the highest correlation coefficient was 0.570; therefore, all of these variables were entered simultaneously into the analysis (Table 3).
First-order correlations between independent variables
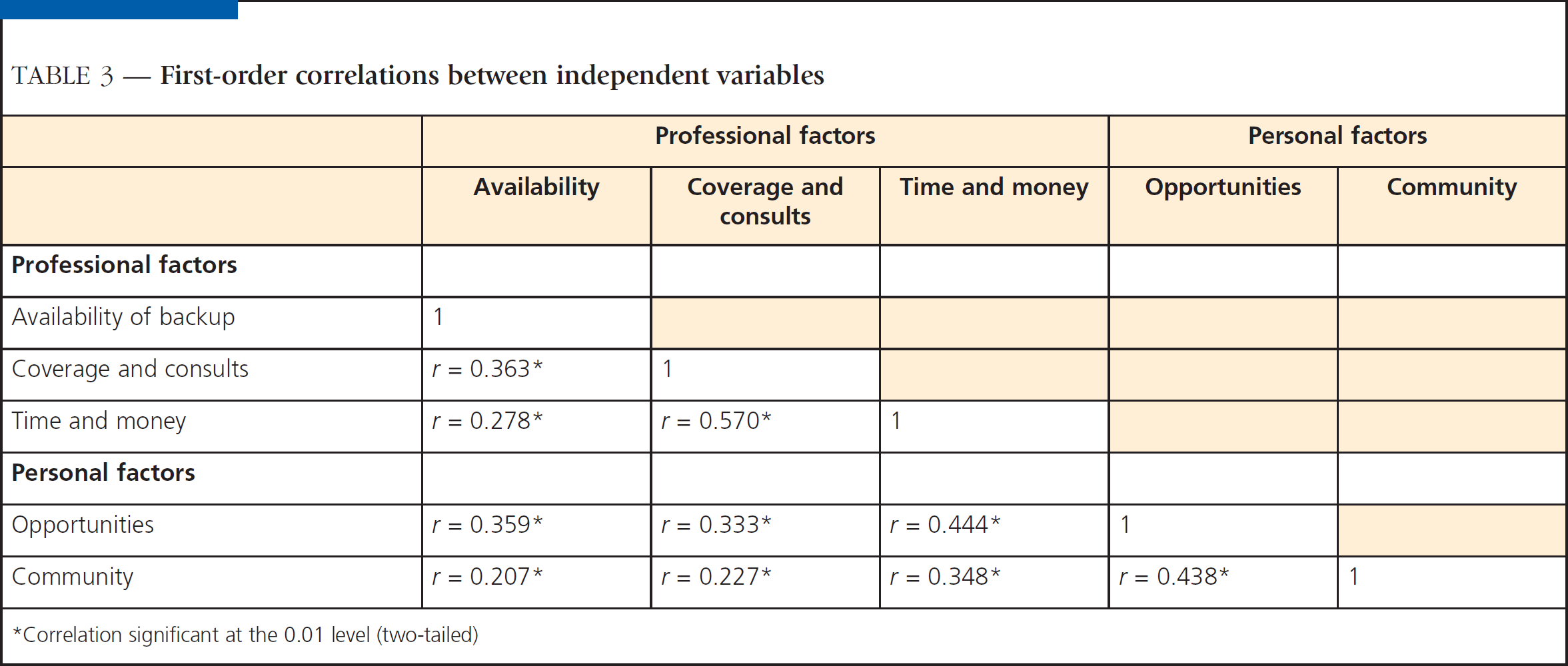
Correlation significant at the 0.01 level (two-tailed)
Logistic regression analysis was performed in a hierarchical fashion, with pharmacist attributes entered in the first step and community attributes in the second step. Variables from the univariate analyses were included if p < 0.15. Factor scores (n = 5) were used instead of the 17 individual personal and professional factors. As a result of missing data for some respondents (n = 425), only 594 (58%) of the responding pharmacists were included in the multivariate analysis. Pharmacist attributes that significantly predicted intent to remain in practice in the community for the next two years were older age and time in practice (Table 4). The addition of community factors to the model significantly improved its fit (χ2 = 39.69, df = 6, p < 0.001), although the only area of professional satisfaction that remained significant in multivariate analysis was time and money and the only area of personal satisfaction that remained a significant predictor was the personal factor related to community. The time and money factor included hours of work, opportunities for professional development, opportunities for career advancement, and earning potential. The community factor included a sense of belonging to community and a sense of being appreciated by community.
Results of multivariate, hierarchical logistic regression
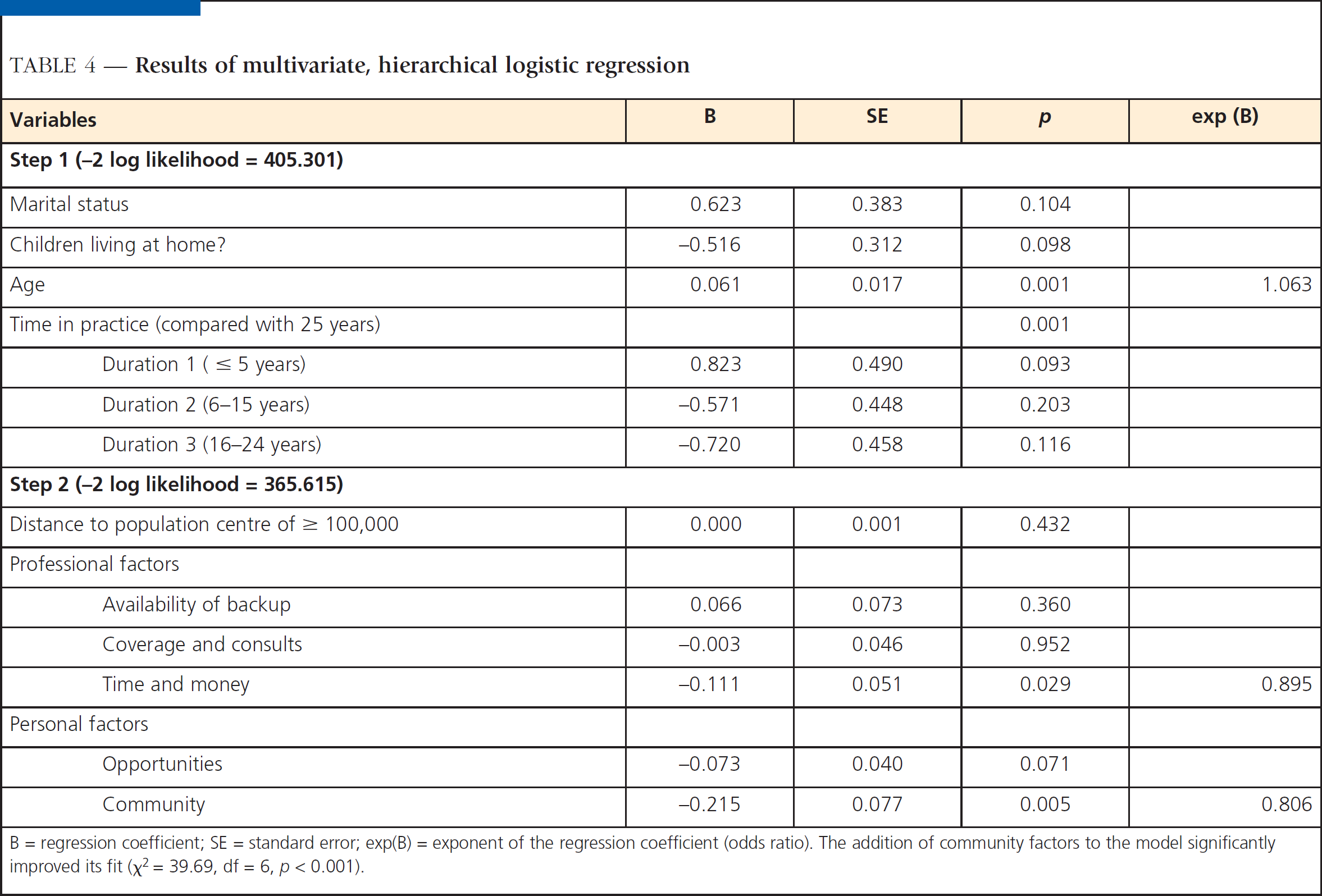
B = regression coefficient; SE = standard error; exp(B) = exponent of the regression coefficient (odds ratio). The addition of community factors to the model significantly improved its fit (χ2 = 39.69, df = 6, p < 0.001).
Discussion
Although younger age, being married, and the presence of children at home were associated with rural pharmacists' intention to remain practising in the community, only age remained significant when these predictors were considered simultaneously in a univariate analysis. These differences were not explained by differences in the subgroup in which the multivariate analysis was done. The presence of children was significantly related to a respondent's age and to marital status, which likely explains why only age remained significant in the multivariate analysis.
In this study, sex was not associated with the intent to remain, whereas in a survey of 541 pharmacists in four American states the turnover rate for female pharmacists was significantly higher than that for male pharmacists (average annual rate of 15% vs 10%, respectively). 15 Other retention factors varied by physician age and sex in the study by Humphreys et al., 9 but age and sex in and of themselves did not predict retention.
In the current study, both shorter (< 5 years) and longer duration in practice were associated with the intention to leave, probably because of retirement in the latter situation. In Mott's survey of US pharmacists, 15 50% of job turnovers occurred before the pharmacists had worked three years for a particular employer. Since it appears that pharmacists in both their middle years of practice and middle age are more likely to remain and since job performance usually improves with experience, it appears that communities and employers searching for new pharmacists should target older, more experienced pharmacists rather than following the common practice of attempting to hire new graduates.
After a pharmacist's personal attributes were taken into account, community characteristics and the pharmacist's satisfaction with both professional and personal aspects of living and working in a rural community were significantly associated with his or her intention to remain in practice in that community. This finding is consistent with those of most studies of retention among rural physicians 2,3,8 and nurses. 6,13
Although the size of the community in which pharmacists were working and its distance from a larger urban centre did not predict intent to remain in a univariate analysis, the community's distance from a population centre larger than 100,000 was related to intent to remain when other variables were taken into account. Distance from a city was only weakly (although significantly) correlated with cultural opportunities and educational opportunities for children (r = 0.133 and 0.171, respectively). (This is similar to Australian findings, where proximity to larger urban areas was the least important factor in retention of rural physicians, although other retention factors, including distance to urban centres, did vary by geographic location. 9 )
Satisfaction with all of the professional and personal factors was higher among pharmacists who said they still planned to be practising in their rural community two years from the time they completed the survey. In Mott's survey, 15 the four leading reasons that pharmacists gave for leaving their jobs were:
Relocation (desire for a new location) Salary Stress level Desire for change.
Pharmacists in the present survey were asked not about their potential reasons for leaving but rather about levels of satisfaction with both their professional and personal lives in that community. Those who were more satisfied with their earning potential were significantly more likely to say they would remain.
Influences on the decision to remain in practice in a rural community are multifactorial, and both personal and community attributes play a role in a health professional's decision to remain in a rural community.
Limitations
There were a number of limitations to this analysis. First is the problem of nonresponse bias, given that only 40% of pharmacists in the targeted sample completed and returned the survey. This return rate was similar to the rate of return in Mott's survey (34.5%). 15 Respondents who did not return the survey and those submitting an incomplete survey may differ systematically in some way that might bias the results of these analyses and limit their generalizability.
The use of respondents' plans to remain as a proxy for actual retention may be problematic. A stronger study design (which would also take longer and be more expensive) would be a longitudinal one, with actual retention as the outcome measure. Conversely, the study by Pathman et al. 16 of the predictive accuracy of physicians' stated plans to remain in a rural community supports the approach used here; in that study, respondents' predictions corresponded well with actual retention over a five to six year period.
Finally, the use of satisfaction with various professional and personal aspects of the community may be a poor measure of actual community attributes. It is possible that people who are less “content” as a personality trait express lower levels of satisfaction and are less likely to remain in any position for long periods of time.
There is a need for more research on recruitment and retention issues for pharmacists in both rural and urban settings. The Canadian Pharmacists Association completed a situational analysis with Human Resources Development Canada in 2000 and is now the secretariat for a committee of pharmacy organizations and associations that is negotiating a $2.6 million pharmacy occupational sectoral study with Health Canada's Health Human Resource Strategy Division (HHRSD). This study will look at the roles of pharmacists and pharmacy technicians in health care reform and will help to forecast the system's needs and provide strategies for dealing with the shortage in the short and long terms.
Useful links
For more on CPhA's pharmacy occupational sector study, see Canadian Pharmacists Association at www.pharmacists.ca/content/about_cpha/whats_happening/cpha_in_action/demand_pharmsrves.cfm.
See also “Development of a Multistakeholder Framework/Index of Rurality,” www.pharmacists.ca/content/about-cpha/whats_happening/cpha_in_action/pdf/RuralityFrameworkFinalReportE.pdf.
Implications
The shortage of pharmacists in rural and remote communities threatens the quality and availability of health care in these communities. Research on this issue as it relates to pharmacists is non-existent. As many or more resources must be dedicated to retaining pharmacists in rural communities as are dedicated to recruiting them.
Despite the limitations of this analysis, the results could be used to help communities select professionals who are most likely to remain in practice in the communities for longer periods. Broad, integrated strategies are needed to ensure that pharmacists and other health professionals choose to remain in their rural communities. The role of the local rural community may be even more important in retention than it is in recruitment. Obviously, community attributes such as distance to large population centres cannot be changed, but attributes that contribute to personal and professional satisfaction can be altered. Involving rural communities along with other stakeholders has been effective in both the recruitment and the retention of health professionals. 17