
Abstract

Pharmaceutical care is a philosophy of the practice of pharmacy that has been accepted by many academic, professional, and regulatory bodies as a foundation for primary care by pharmacists in the health care system. 1,2 Despite widespread acknowledgement of the importance of pharmaceutical care — or centering the pharmacist's role on the patient, rather than the drug — pharmacists have been slow to adopt it. 3 Pharmacists may be more frequently engaged in passive pharmaceutical care activities, such as information-gathering and acting as a drug-information source, than in active interventions, such as patient counselling and drug monitoring, according to Schommer and Cable. 4 Also, it has been observed that many pharmacists still perform highly distributive functions, with very little commitment to pharmaceutical care responsibilities. 5,6
Traditional pharmacy design characteristics and administrative constraints may be reasons for the inertia in providing pharmaceutical care as part of routine pharmacy practice. 7,8 Many obstacles to the provision of pharmaceutical care have been discussed in the literature, including barriers in:
Infrastructure (physical layout, staffing levels, excessive workload, time constraints) Cognitive skills (lack of competence, inadequate training) Communication (lack of motivation, skills, or support) Compensation (economic incentives to provide pharmaceutical care) Logistics (lack of access to patient medical information and to other health care professionals) Motivation and training (unwillingness to take full advantage of technological developments)
7,9
–13
The objective of this study was to examine the design and workflow characteristics across a sample of Canadian community pharmacy practice sites that are engaged in pharmaceutical care.
Background
As the profession pursues patient-focused pharmaceutical care standards, it is important that pharmacists be able to assess the quality of the care they provide and recognize any barriers to comprehensive care. 14 Although several pharmaceutical care models and practice guidelines have been proposed and developed for community pharmacy settings, 2 minimal work has been done on evaluating the specific design features and workflow processes associated with the provision of pharmaceutical care.
Despite the challenges, many Canadian pharmacists have overcome barriers to the provision of pharmaceutical care, altering both the arrangement of pharmacy resources and the activities performed by the pharmacists. Pharmacists across Canada can learn from their colleagues' experiences and successes in these community pharmacy sites.
Results
Respondent summary:
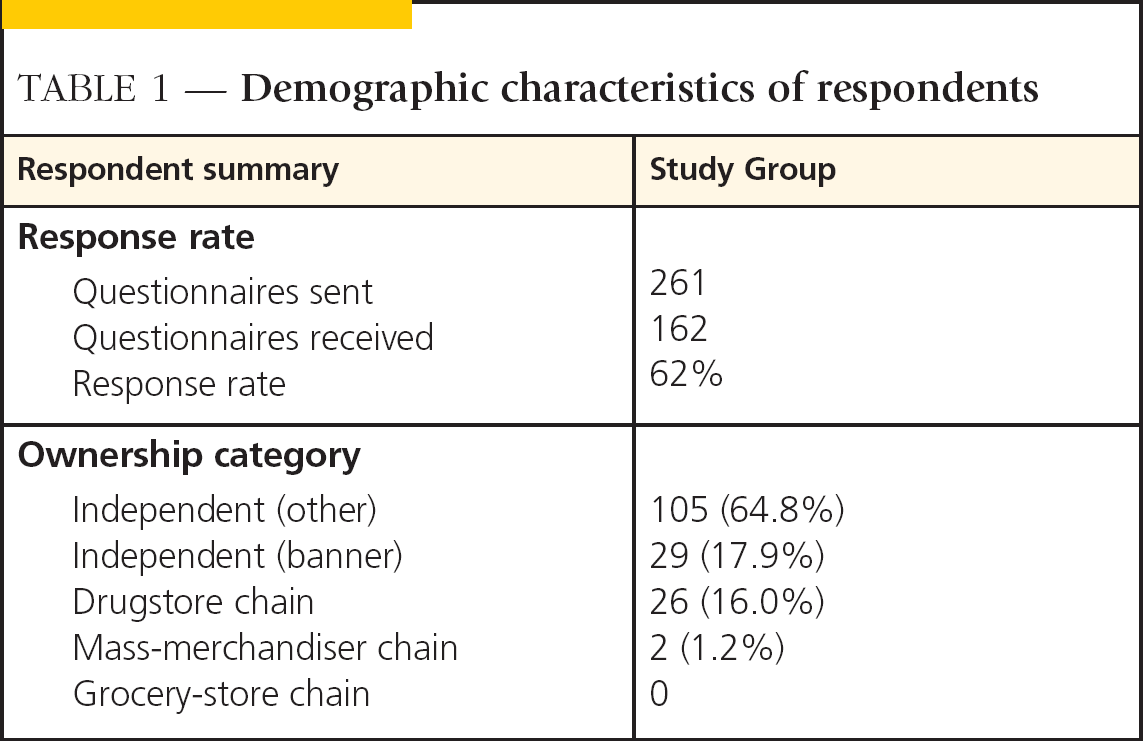
The response rate from 261 queries was 62%, with 162 usable responses (Table 1). A major proportion (about 83%) of the respondents were from independent pharmacies. Further, 72% of the pharmacies were from urban locations, and 28% were in a rural setting. Forty-four pharmacies were placed in the highest quartile subgroup, and 45 pharmacies were assigned to the lowest quartile subgroup.
Demographic characteristics of respondents
Performance on Behavioral Pharmaceutical Care Scale:
The mean Behavioral Pharmaceutical Care Scale (BPCS) score of all respondents was 110 (range 39–171, SD 28.6). The 25th-percentile score was 93, and the 75th-percentile score was 130.2. A histogram displaying a normal distribution of the BPCS scores (as determined by a Lillefor's test for normality) is presented in Figure 1.
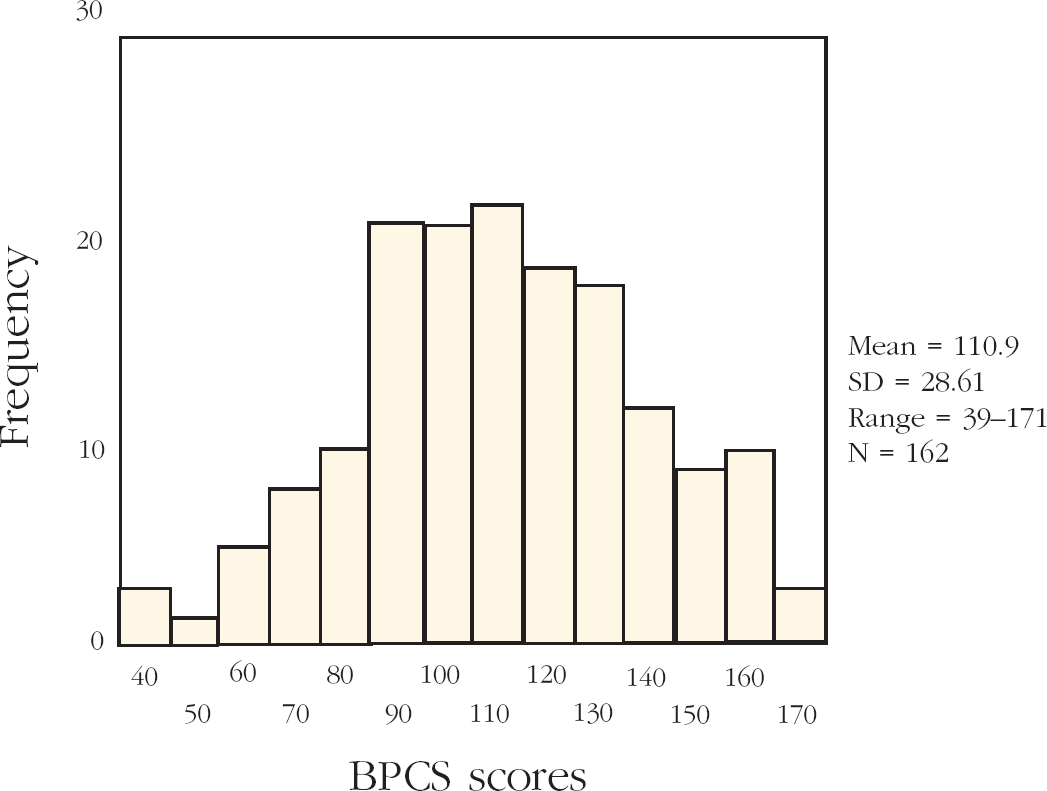
Behavioral Pharmaceutical Care Score distribution
Subgroup comparison:
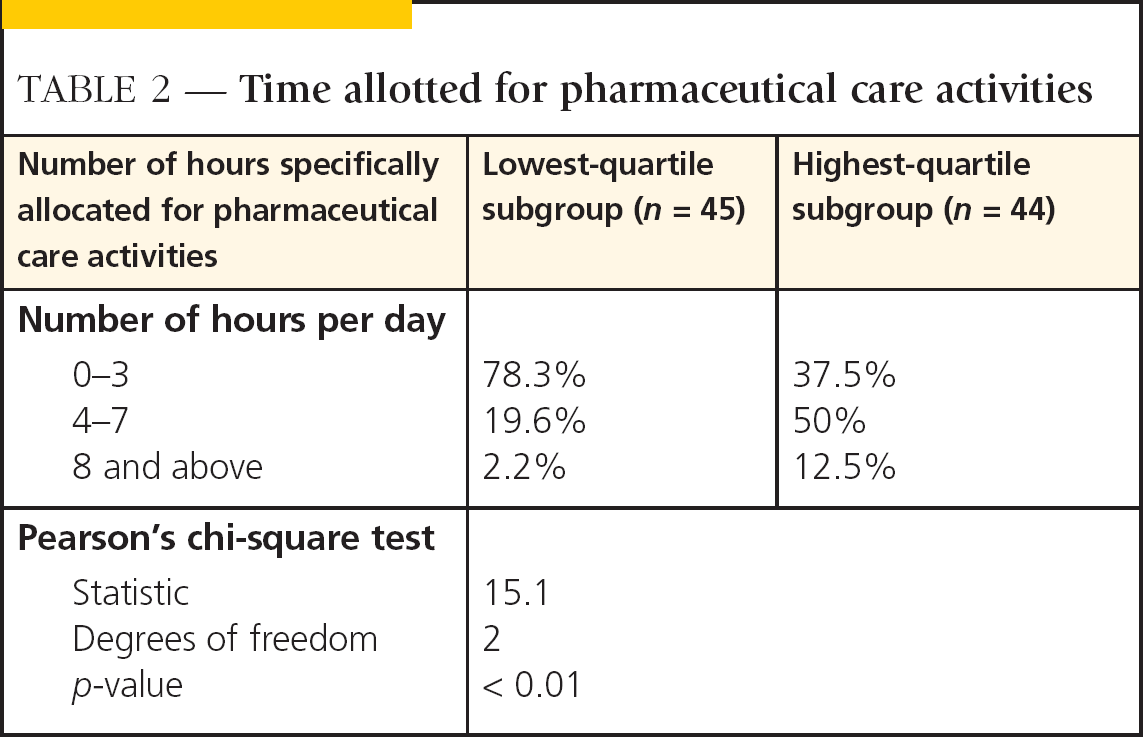
Regarding time allocation, a higher percentage of highest-quartile subgroup pharmacies reported allocation of more hours for pharmaceutical care activities than those in the lowest-quartile subgroup. In the highest-quartile subgroup, 50% of the pharmacies allocated four to seven hours per day, whereas only 19.6% of the lowest-quartile subgroup pharmacies allocated a similar number of hours for pharmaceutical care activities.
The highest-quartile subgroup reported a significantly higher allocation of hours per day specifically for pharmaceutical care activities than the lowest-quartile subgroup, as determined by Pearson's chi-square test (p < 0.01) (Table 2).
Time allotted for pharmaceutical care activities
METHODS
A data collection instrument, the Community Pharmacy Structural Elements Questionnaire (CPSEQ), was developed based on information obtained from a literature search of articles reporting structural changes in community pharmacy practices. In a pretest of 28 community pharmacy sites, the CPSEQ was found to have reliability and validity as an instrument for gathering information about the following categories of structural elements in community pharmacy:
Reorganization of pharmacists' and pharmacy technicians' duties Changes in physical layout Training for pharmacists and pharmacy technicians Financial compensation Modification of store policies and procedures Incorporation of technology
Respondents were assigned scores on the CPSEQ based on their reporting of recent structural changes; each change was given an equivalent score of one, and the scores were summed to determine a total score for the pharmacy.
Behavioral Pharmaceutical Care Scale: Our data collection instrument also included the Behavioral Pharmaceutical Care Scale (BPCS) developed by Odedina and Segal. 15 It is a multi-item scale that measures pharmacists' efforts toward providing pharmaceutical care. The scale comprises 34 behavioural activities representing the following pharmaceutical care domains:
Direct patient care Referral/consultation Pharmaceutical care instrumental activities
When completing the BPCS, respondents are asked to reflect on their interaction with the five most recent patients who have presented with prescriptions to treat a chronic condition. The respondents then indicate how many of the five patients received the listed pharmaceutical care activities. Possible responses range from 0 (none of the patients) to 5 (all five patients) for each domain item. The theoretical total score on the BPCS, therefore, can vary from a low of 16 to a high of 180.
Selection of respondents
Study group participants were selected from community pharmacy practices across Canada. They were selected based on their affiliation with any one of six pre-identified pharmaceutical care models, or with the structured practice experiential teaching programs known to be in place in Canada at the time the survey was conducted:
Health Outcomes Pharmacies Structured Practical Experience Program (University of Toronto) Clinical Associate Program (University of Montreal) Asthma Self-Management Education Program (British Columbia) Geriatric Pharmaceutical Care Model (Manitoba) Pharmaceutical Care Research and Education Program (Alberta) Pharmaceutical Care Model (Dalhousie) In-Home Drug Evaluation Model (Saskatchewan)
2
A total of 301 community pharmacy practices in Canada were estimated to be affiliated with at least one of these pharmaceutical care models or programs.
Survey administration
Potential participants were contacted by telephone by a member of the research team and were invited to participate following a brief explanation of the study. The researchers assured participants of the confidentiality of their responses. A survey package, which included the CPSEQ, the BPCS, a cover letter, and a self-addressed postage-paid envelope, was then mailed to 261 potential respondents who consented to participate in the survey. The survey administration took place from August 27, 1999, to November 22, 1999.
Analysis
Using the distribution of total scores from the BPCS, the highest-quartile (HQ) subgroup (respondents above the 75th percentile) and lowest-quartile (LQ) subgroup (respondents below the 25th percentile) were determined. The HQ subgroup represented respondents with evidence of significant progress toward providing pharmaceutical care. The LQ subgroup represented respondents who, in the assessment of the researchers, could provide little validation of progress toward pharmaceutical care, despite their affiliation with a model or program.
Exploratory analysis was conducted to compare the design and workflow elements and the hours per day allocated for pharmaceutical care activities reported in the CPSEQ by the HQ and LQ subgroups.
Regarding structural elements, the frequencies of specific design or workflow elements reported were compared using Pearson's chi-square test. Structural elements that were reported in a significantly higher frequency by the highest-quartile subgroup were decreased pharmacist involvement in technical dispensing functions, use of audiovisual educational equipment, and the requirement for sit-down counselling for new prescriptions (all p < 0.01). Practice-site changes, such as increased pharmacist involvement in provision of professional services and a change in the dispensary software system, were also reported with high frequency by both subgroups, but were not statistically different (Table 3).
Key elements in the lowest-and highest-quartile subgroups
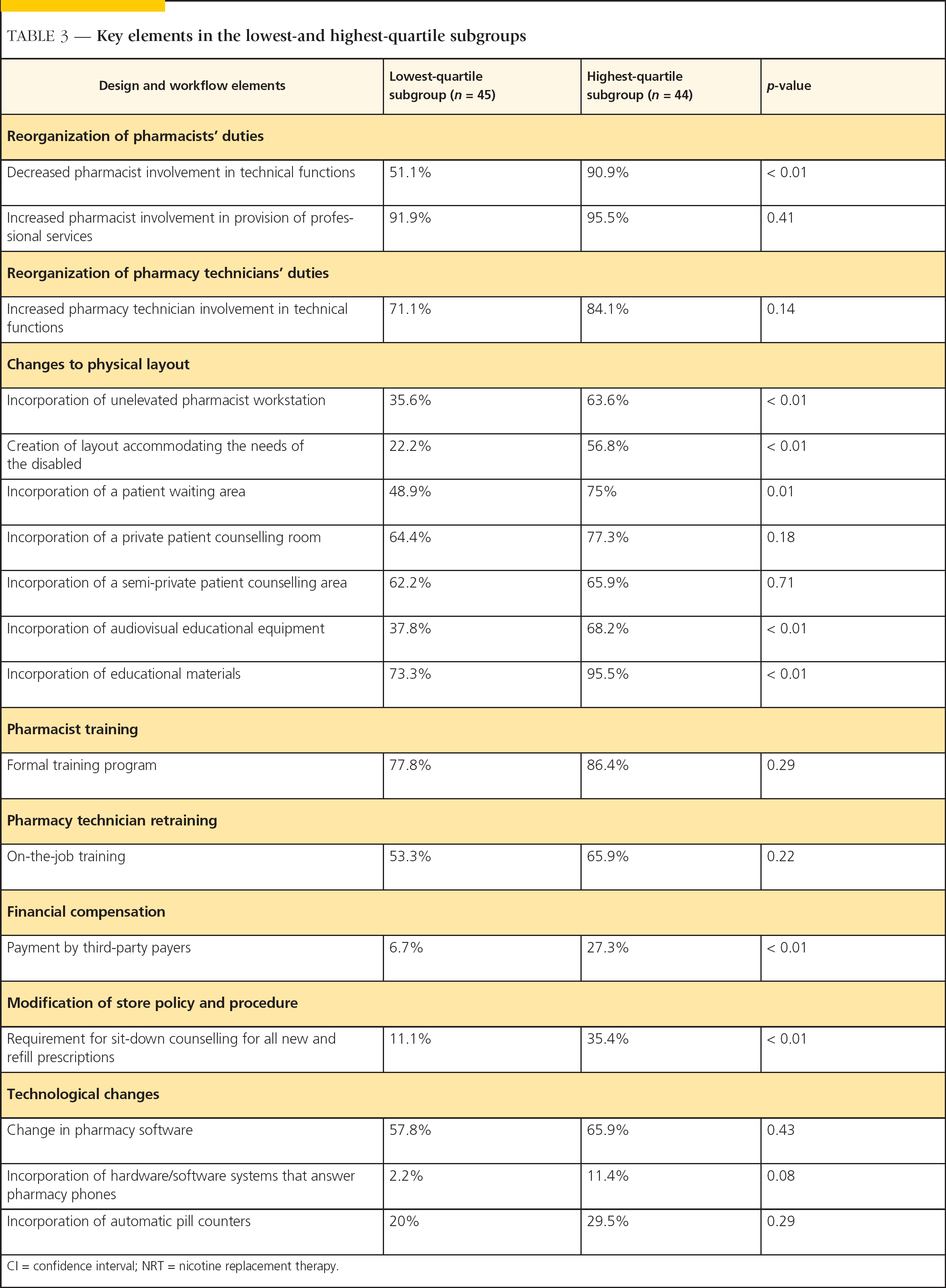
CI = confidence interval; NRT = nicotine replacement therapy.
Discussion
Many practice leaders demonstrated significant progress toward the provision of pharmaceutical care (based on the Behavioral Pharmaceutical Care Scale). The unexpected finding of some very low BPCS scores suggests that, despite a stated affiliation with a defined pharmaceutical practice model, there were respondents who could demonstrate little evidence of positive patient care efforts as measured by the BPCS.
KEY POINTS
Since its introduction in 1990, “pharmaceutical care” has become a key conceptual framework for developing community and hospital pharmacists' roles. Pharmaceutical care is patient-centered rather than product-centered. Pharmaceutical care is an important precursor to pharmacist involvement in primary health care. Despite widespread support of the concept by professional leaders, individual pharmacists have been slow to adopt it. Barriers include an actual lack of expertise to make drug therapy decisions. Structural changes in community pharmacies are necessary to implement the pharmaceutical care model.
Time:
The exploratory analysis revealed that in the reorganization of pharmacists' duties, decreased pharmacist involvement in technical dispensing functions was reported with a higher frequency by the highest-quartile subgroup than the lowest-quartile subgroup (p < 0.01). This is an important change associated with the provision of pharmaceutical care, since pharmacists must free up time to focus on patients' medication-related problems.
Physical layout:
The presence of an unelevated pharmacist workstation, the design of a patient waiting area, the use of audiovisual educational equipment, and the incorporation of patient-education materials were all reported more frequently by the highest-quartile subgroup (p < 0.01).
Since the design of a separate counselling area was a precondition of participation or enrolment in many of the pharmaceutical care models or programs, both subgroups were expected to score high with respect to this requirement. These design features are seen to be beneficial in facilitating patient contact, increasing privacy for confidential conversations, enhancing the patient counselling environment, and adding resources that complement and reinforce patient counselling. The benefits of these changes to the physical layout of the pharmacy in overcoming barriers such as workspace, resources, and time to enhance the provision of pharmaceutical care, have also been widely discussed in the literature. 7,11,14,16,17
Both subgroups were expected to score high in the pharmacists' training category, as this was also a mandatory requirement of several of the pharmaceutical care models and programs. Pharmacists and pharmacy technicians may require additional training to overcome identified barriers (see box).
In the modification of a pharmacy's policy and procedures category, the requirement for sit-down counselling for all prescriptions was reported with higher frequency in the highest-quartile subgroup. This procedural change may help ensure that comprehensive care is provided, including monitoring, continuity of care, and follow-up.
This subgroup consisted of progressive community pharmacy practices and provided more evidence indicative of progress toward the provision of pharmaceutical care than the lowest-quartile subgroup. The results of the exploratory analysis revealed that the highest-quartile subgroup pharmacies allocated more hours per day specifically for pharmaceutical care activities. These community pharmacy practices also made design and workflow changes to facilitate their pharmaceutical care practice objectives.
Limitations of study
Self-reporting bias:
The information for this study was gathered through a survey using instruments (the CPSEQ and the BPCS scales) that required self-reporting by pharmacists. Therefore, there was opportunity for respondents to modify or falsify answers in order to appear better at providing pharmaceutical care (i.e., social-desirability bias). To help control for this behaviour, respondents were assured of total anonymity, as well as of the confidentiality of their responses.
Barriers to pharmaceutical care
Weak communication skills Inability to select appropriate patient educational tools Inability to recognize situations in which specific knowledge is necessary Inability to select and apply scientific technical and clinical information in a timely and appropriate manner Lack of expertise to make drug therapy decisions
No time implications:
The survey asked respondents to simply indicate the changes that had been made in the pharmacy to implement a pharmaceutical care practice. No supplemental information was requested to determine the timing of any structural changes or to assess whether or not the changes were part of a deliberate pharmaceutical care strategy. Future research that uses a longitudinal design would permit study of the timing effect on selected variables and the pharmacist's motivation to make changes.
Conclusion
Building a successful pharmaceutical care practice is not a simple task. Established community pharmacy sites in Canada with successful pharmaceutical care practices are still few in number. This remains uncharted territory without proven models from which pharmacists can plan design and workflow changes. Affiliation with a pharmaceutical care model or program such as those followed in this study could be a useful strategy for facilitating practice change.
This study characterizes the efforts that have been made by some innovative Canadian community pharmacy practices to provide pharmaceutical care. This preliminary listing of design and workflow elements may be a useful resource for assisting community pharmacists to translate the philosophy of pharmaceutical care into daily practice. Further, the findings reported here are intended to generate guidance for the development of future research studies to provide stronger evidence about pharmacy structural changes that support the provision of pharmaceutical care in the community pharmacy.
Footnotes
Acknowledgements:
We would like to express our gratitude to Apotex Inc. for its generous research grant, which funded this study. We also express our sincere appreciation and thanks to Dr. Timothy-John Grainger-Rousseau, who initiated this study, for his most significant and valuable input throughout the research project.