
Abstract
Medication errors can occur at any stage in the medication use process (prescribing, transcribing, dispensing, administering, or monitoring) and in any setting (hospital, long-term care institution, or community). Few studies concerning dispensing errors in community pharmacies are available, but those that have been done indicate a risk of error similar to that in institutional health care settings.
In one observational study, researchers examined dispensing accuracy in a total of 50 pharmacies in six cities across the United States. 1 They found an error rate of about one per every 55 prescriptions filled. As such, it is likely that every pharmacist has made at least one dispensing error in his or her career. Many of these errors are picked up by the patient or another health care professional before the drug is administered, but even if the patient takes the drug, most such incidents do not lead to harm. Nonetheless, the errors signal vulnerabilities in the system and provide valuable learning opportunities for the prevention of similar mishaps that could result in harm. Simply “being more careful” is usually not a solution, as most of the causes of error are related to system factors. “Accidents” typically result from a sequence of events that tend to follow recurrent patterns, regardless of the personnel involved. All staff, even the most experienced and dedicated professionals, may be involved in preventable adverse events.
Sharing with others when errors and near-misses occur is a crucial step in learning and in improving the medication system. System improvement can be accomplished through a four-pronged approach 2 :
Analyzing individual errors at your practice site
Analyzing your aggregate medication error data
Analyzing “near-miss” events (errors that have the potential to reach the patient)
Learning from errors that have occurred in other organizations
Each prong provides valuable learning about weaknesses in the medication use system that collectively can lead to effective error reduction. This article focuses on the first prong — how to analyze individual errors at your practice site using the Canadian Root Cause Analysis (RCA) Framework. This framework was developed by the Canadian Patient Safety Institute, Saskatchewan Health, and the Institute for Safe Medication Practices (ISMP) Canada 3 to provide a standardized approach to the retrospective analysis of critical incidents and near-miss events in health care. RCA directs attention away from the actions of individuals toward the system-based causes of events.
Root cause analysis is intended to determine three things:
What happened
Why it happened
What can be done to reduce the likelihood of a recurrence
Here, we offer a hypothetical response to an incident that was reported to ISMP Canada as an example of how the RCA Framework might be used to analyze a medication incident in a community pharmacy.
The incident
A patient called the pharmacy where her long-term prescription for prednisone 5 mg had been refilled a couple of months before. She reported that she had been ill recently and had visited the emergency department of the local hospital. Medical staff in the emergency department determined that she had actually been taking prednisone 50 mg tablets and that this incorrect dose was the cause of her symptoms. The emergency physician had given her a decreasing dose schedule with instructions for follow-up with her own physician.
The hypothetical response
After apologizing to the patient and assuring her that the error would be fully investigated, the pharmacist should initiate an analysis of what happened and why. The RCA Framework recommends a team approach to reviewing an incident, which would include the following steps:
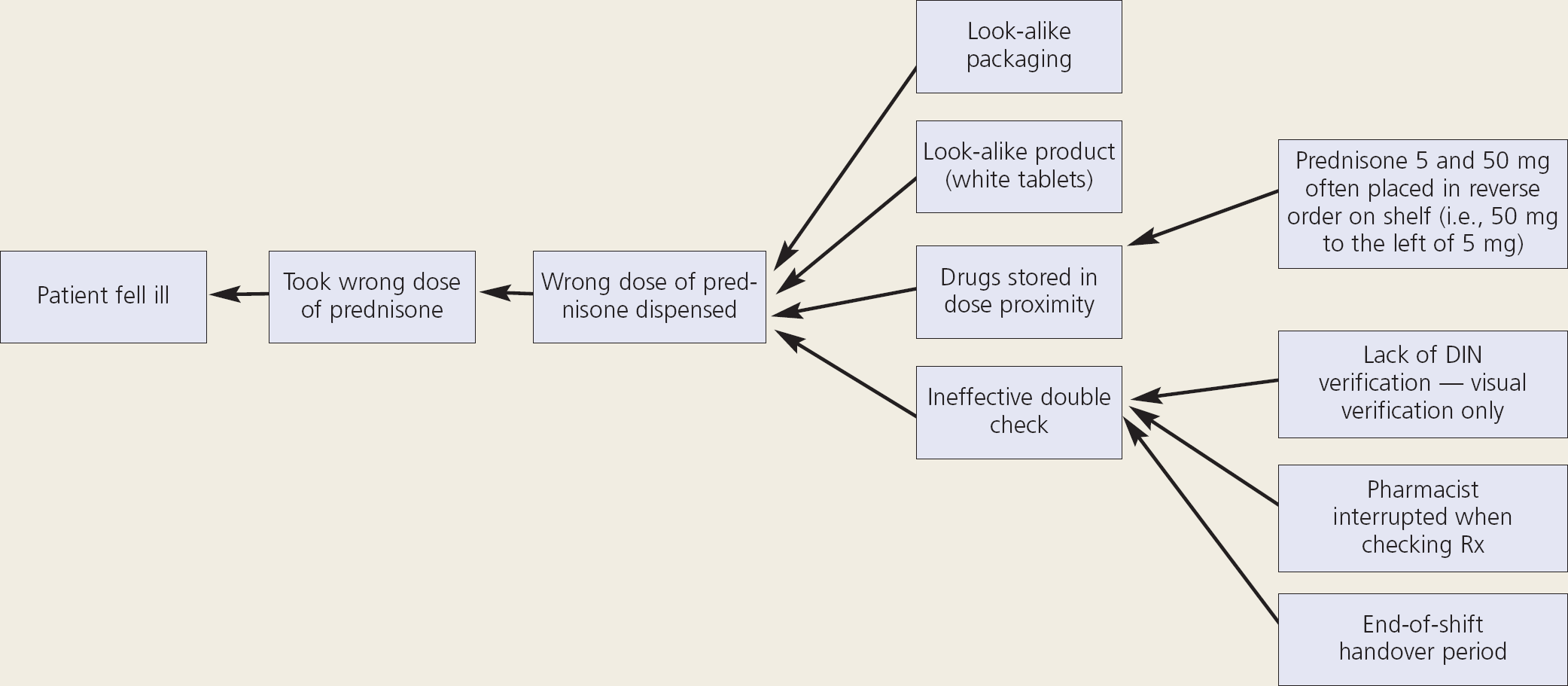
Cause-and-effect diagram of prednisone error
Review the documentation (i.e., the written prescription and the computer entry).
Review the physical environment where the error occurred, including the dispensary work space and medication storage areas.
Review product labelling and packaging.
Interview the dispensing pharmacist(s) and pharmacy technician(s) to determine the sequence of events and anything else that might have been happening at the time.
The information gathered is then used to create a flow chart or narrative timeline. Once the team has a good understanding of the sequence of events, a cause-and-effect diagram will assist in identifying the factors that contributed to the incident. The team begins the diagramming process by identifying the adverse outcome experienced by the patient and then asks a series of “caused by” and “why” questions to determine the action that preceded each event in the sequence. A hypothetical cause-and-effect diagram for the prednisone error is shown in Figure 1.
A number of contributing factors will usually be identified through the diagramming process. The next step is to determine which of these contributing factors, if corrected, would have prevented the error. These crucial factors are the “root causes.” In the prednisone incident, the following root causes might be identified:
Look-alike packaging
Look-alike product
Storage in close proximity
Lack of verification of drug identification number (DIN)
The root causes are then framed into “causal statements,” which form the basis for developing actions. The following causal statements might apply in this case:
The look-alike packaging of prednisone 5 mg and 50 mg increased the likelihood that the incorrect strength of medication would be dispensed.
The similar appearance of the prednisone 5 mg and 50 mg tablets decreased the likelihood that a dispensing error would be detected.
The storage of prednisone 5 mg and 50 mg tablets in close proximity increased the likelihood that the incorrect strength would be selected and dispensed in error.
The lack of a standardized process for verification of DIN when dispensing and checking prescriptions reduced the likelihood that a dispensing error would be detected.
Strategies can then be developed to reduce the likelihood of a recurrence of this or a similar incident. The following actions might be appropriate in this case:
Store look-alike products in separate locations in the dispensary.
Purchase prednisone 5 mg and 50 mg tablets from different manufacturers to improve label differentiation.
Use auxiliary warning labels to alert staff to high-potency products.
Develop a standard process for verifying the DIN during dispensing, a process that should include documentation by both the technician filling the prescription and the pharmacist checking the prescription.
Conclusions
A thorough RCA often reveals underlying system deficiencies that are not immediately obvious, as well as issues that have become so familiar to dispensary staff that they are no longer recognized as posing risks. RCA does not assign blame; rather, it is an outcome-directed process emphasizing specific, high-leverage actions that take into account the need to integrate safeguards into system design and the need to consider human capabilities and limitations.
The RCA Framework is a tool for analyzing errors that will help pharmacists and support staff gain an understanding of the underlying conditions that set the stage for errors. The framework provides a structure for both error analysis and development of actions for system improvement. Sharing the results of RCAs within your own organization and with the pharmacy community at large provides important learning for all.