
Abstract
Objective:
To assess the effect of intensive vs conventional training on pharmacist-suggested implementation of cardiac risk reduction efforts in community practice.
Methods:
Sixty-one volunteer pharmacists from 40 pharmacies were randomized to 1 of 2 educational groups: intensive or conventional training in cardiac risk reduction. With training complete, pharmacists identified and approached patients at high risk for coronary artery disease (CAD) at their practice sites to participate in the program. After a patient interview, pharmacists documented the relevant CAD risk factors and medication history, and then faxed this information, along with risk reduction recommendations, to the primary care physician. Patients were then encouraged to book a medical appointment for further assessment and treatment, if warranted. Follow-up occurred at 4, 16, and 24 weeks to determine if any pharmacist-suggested risk reduction measures had been implemented. Pharmacists were reimbursed $30 per patient accrued.
Results:
A total of 217 patients were enrolled in the study, and of those, 216 had follow-up data available for analysis. No significant differences were observed between the groups with respect to mean number of patients enrolled per pharmacist (4.3 vs 2.7) and the proportion of pharmacists completing at least 1 patient (17/27 vs 14/34). Feedback from pharmacists on program delivery indicated no significant difference in satisfaction with the training provided. The recommendations forwarded by pharmacists of the intensive group (35.8%) received greater acceptance by physicians than those in the conventional group (23.8%).
Conclusion:
Although results are preliminary, intensive training for pharmacists was more likely to result in improvements in cardiovascular risk reduction therapy than when conventional training was used.
Pharmacists are considered an underutilized resource for patient care — especially in the area of appropriate use of medications. 1,2 Yet pharmacist participation in disease management programs has been shown to improve target conditions and to improve physician prescribing. 3 –8 There is strong evidence, for instance, of the value of pharmacist involvement in cardiovascular risk reduction efforts. 9 Still, treatment gaps continue to exist between clinical practice guidelines and actual practice. Collaboration across health disciplines could, perhaps, help close these gaps. 10,11
In their model of practice change for pharmacists, Holland and Nimmo describe the evolution of community pharmacy practice from primarily drug distribution to one that embraces the provision of drug information and consulting services. 16 In fact, the ideal practice model of pharmaceutical care is still a work in progress. Further improvements will require shifts in attitudes, as well as enhancements in knowledge and skill. Current practitioners possess tremendous experience and talents; however, extra training is usually provided before engagement in so-called expanded clinical programs.
The most effective way to provide extra training is unclear. 17 The focus of most trials to date has been the impact on patient care, rather than on the type of pharmacist training provided. 9 Research on changing physician practice behaviour suggests that multimodal or sequential interventions are more effective than traditional, lecture-based approaches. 18 –20 How best to educate patients (whether intensively or through more passive measures) has also received attention. 21
Although less common, education-based trials do exist in pharmacy circles. Researchers in the UK, for example, assessed the impact of disseminating evidence-based guidelines by mail (the control) vs educational outreach visits or attendance at continuing education sessions. 22 In that particular case, neither strategy proved effective in reaching the desired goal.
The purpose of this trial was to assess the effect of conventional versus intensive training on pharmacist-suggested implementation of risk reduction efforts for cardiac patients in the community. It was speculated that, because of the complex nature of adopting a new practice behaviour, intensive training would be more effective than conventional training (as seen during typical continuing education events) in preparing pharmacists to first identify patients at high risk for cardiovascular events, and then make therapeutic recommendations to physicians for optimizing care. (For more details on the Pharmacist Intervention in Risk Reduction study, please refer to the previous issue of this journal. 23 )
Methods
All practising pharmacists in the province of Saskatchewan were invited to participate through a mailing via the provincial regulatory authority. Volunteers were randomly assigned to conventional or intensive training. To prevent contamination among the study arms in pharmacies with multiple pharmacists participating, the same educational intervention was assigned to all pharmacists working at the same location.
Conventional training comprised a 2-hour evening lecture on cardiac patient management, considered typical of continuing education programs for pharmacists. In addition to the therapeutic content, there was a 45-minute presentation on study procedures. Intensive training consisted of a 6-hour workshop, in addition to therapeutics and study procedures, that included a presentation on patient counselling techniques, interactive case-based sessions with standardized patients, and e-group support. All pharmacists received a study binder that contained handouts of the presentations made to their respective groups, the study protocol, study forms, review articles, consensus statements, patient education tools, and letters of support from prominent local physicians.
With training in place, patients at a high risk for cardiovascular events (as indicated by the Canadian Working Group on Dyslipidemias 24 ) were identified by the study pharmacists and approached for entry into the study (i.e., the risk reduction program). The main method for this was through in-pharmacy patient profiles. The inclusion criteria included patients who had a known history of acute myocardial infarction, angina, revascularization procedure, those with a greater than 6-month history of cerebrovascular disease (stroke or transient ischemic attacks), peripheral vascular disease, as well as those with diabetes who were over age 30 with one or more other cardiovascular risk factors. Patients were excluded from the study if they were involved in a risk reduction study or if they did not provide consent to participate.
After an interview, pharmacists completed a physician referral form for each patient. The form contained information on cardiovascular risk factors as obtained from the patient, a medication history, and most importantly, recommendations to the physician for maximizing cardiovascular risk reduction therapies. This was faxed to their physician. Patients were subsequently asked to book appointments with that same physician for further assessment.
Key points
Pharmacist involvement in cardiovascular risk reduction efforts, as well as other disease management programs, has been shown to improve target conditions. Intensive training for pharmacists was more likely than conventional training to result in improvements in cardiovascular risk reduction therapy.
Points clés
Il a été démontré que la participation des pharmaciens à des initiatives visant à réduire les risques cardiovasculaires et à d'autres programmes de gestion des maladies contribuait à améliorer l'état des patients atteints des maladies en question.
Pour les pharmaciens, une formation intensive était plus susceptible de contribuer à une amélioration des traitements visant à réduire les risques de maladies cardiovasculaires qu'une formation traditionnelle.
Pharmacists conducted follow-up with each patient at 4, 16, and 24 weeks following the interview to determine whether there had been any introduction of a new risk reduction medication or dosage enhancement of an existing medication arising from the referral. Pharmacists were remunerated $15 for every patient enrolled and a further $15 per patient upon completed follow-up.
The primary endpoint was an institution or enhancement of any risk reduction effort between educational groups, including institution and/or enhancement of:
Antiplatelet therapy Any ACE inhibitor Lipid-lowering therapy Antihypertensive therapy Pharmacologic glucose control therapy Smoking cessation program Pharmacologic therapy for weight reduction
Study pharmacists verified achievement of any of the above by faxing a copy of the prescription or pharmacy patient profile to the Pharmacist Intervention in Risk Reduction (PIRR) study office.
Secondary endpoints included the number of patients who were enrolled per pharmacist, pharmacist satisfaction with the education provided, and self-reported pharmacist confidence with applicable practice skills. For the latter 2 outcomes, researchers developed measures, given that measurement tools were unavailable. Pharmacists were considered to have dropped out of the study if they informed the investigating team of their intent to no longer participate or if they failed to recruit any patients.
The sample size was calculated based on the assumption that conventional training would result in achieving the primary endpoint in 30% of the patients enrolled, as guided by the SCRIP trial. 6 To detect a significant difference between the groups (an endpoint achievement rate of 40% by the intensive group) with a 2-sided alpha of 0.05 and 80% power, 376 patients would be required in each arm of the study.
This study was approved on ethical grounds by the University and Health Region ethics committees.
Results
A total of 61 pharmacists from 40 pharmacies volunteered to participate in the study. Of these, 27 were randomized into the intensive training group and 34 into the conventional group. The pharmacists, 65.5% of whom were women, had varying levels of practice experience. The majority practised in larger urban centres and had no previous experience with conducting practice-based research. Approximately one-half were employed by large chain, franchise, and grocery locations, and the remainder worked at independent or clinic pharmacies. The groups did not differ significantly with respect to demographic variables. 23
While the pharmacists provided education to at-risk patients, they also received education during the 2 training sessions. In fact, satisfaction with the education provided was high. Both groups of pharmacists reported mean satisfaction scores of 3.5 on a scale of 1 (highly dissatisfied) to 4 (highly satisfied). Confidence in practice skill scores was also similar between the groups, with the intensive group having a mean confidence in practice skill score of 3.2 and 3.0 for the conventional group on a scale from 1 (not confident) to 4 (extremely confident) (p > 0.05). Table 1 provides the scores on individual skills polled.
Pharmacist confidence in practice skills *
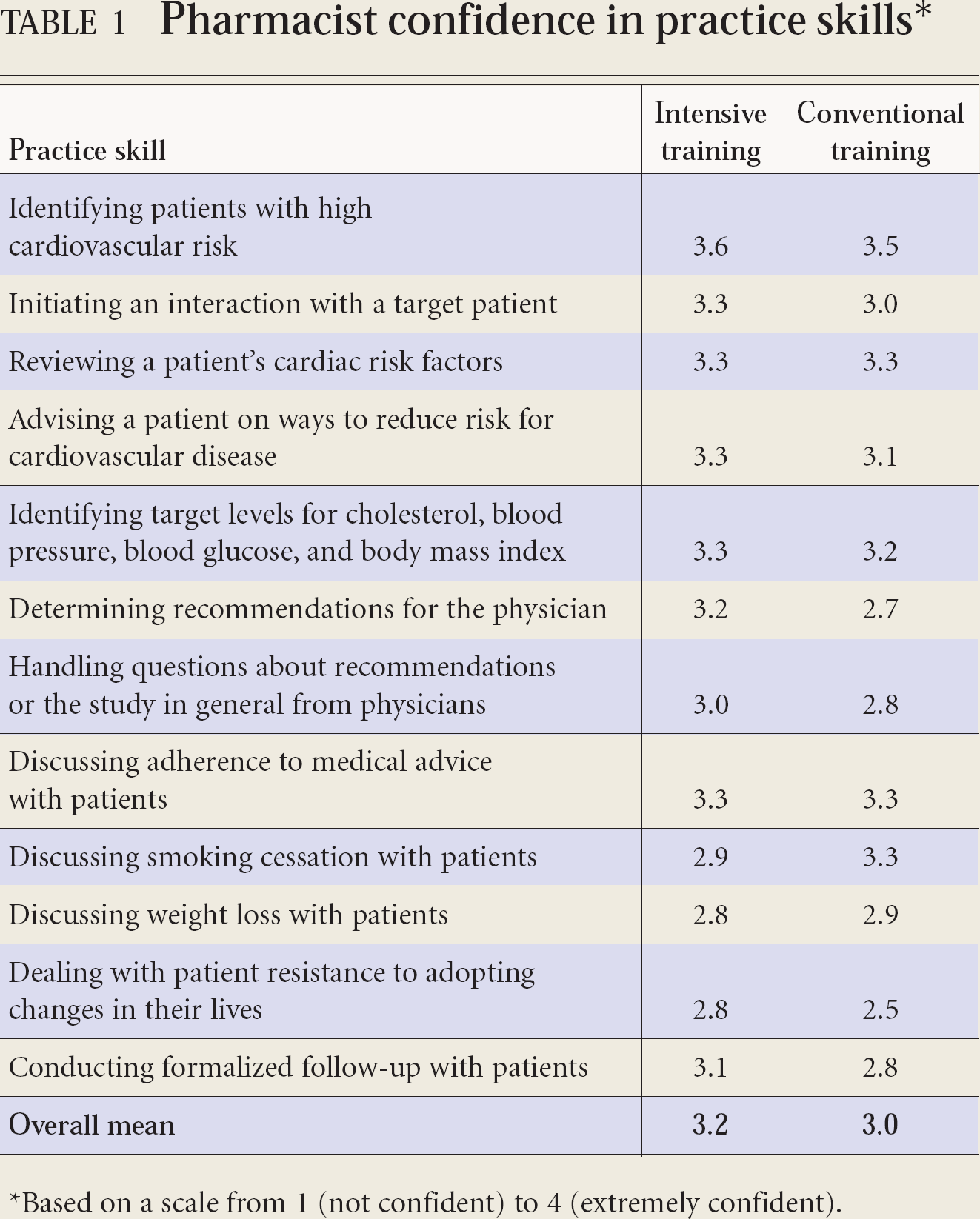
Based on a scale from 1 (not confident) to 4 (extremely confident).
Pharmacists returned to their respective pharmacies and began to search for potential patients. Patient accrual occurred over 24 months (December 2001 to December 2003), with 217 patients eventually enrolled in the study. There was at least 1 follow-up for 216 patients, with 198 having complete 24-week follow-up data. If no data were available for the 24-week follow-up, the last available patient profile information was carried forward for analysis in an intent-to-treat fashion. The patients were 57.4% male, with a mean age of 64.5 years.
The intensive training group enrolled an average of 4.3 patients per pharmacist, which did not differ significantly from the conventionally trained group's average of 2.7 patients per pharmacist (p > 0.05). A higher pharmacist dropout occurred in the conventionally trained group; 20 out of 34 pharmacists failed to complete any patient interventions, whereas only 10 pharmacists failed to complete patients from the intensive group.
Table 2 outlines the recommendations made by the study pharmacists. There were no significant differences between groups as to the number or type of recommendations, with the exception of smoking cessation programs. Pharmacists in the conventional group were twice as likely to recommend smoking cessation than those who were in the intensive group (18.6 vs 7.6%).
Pharmacist recommendations forwarded to physicians
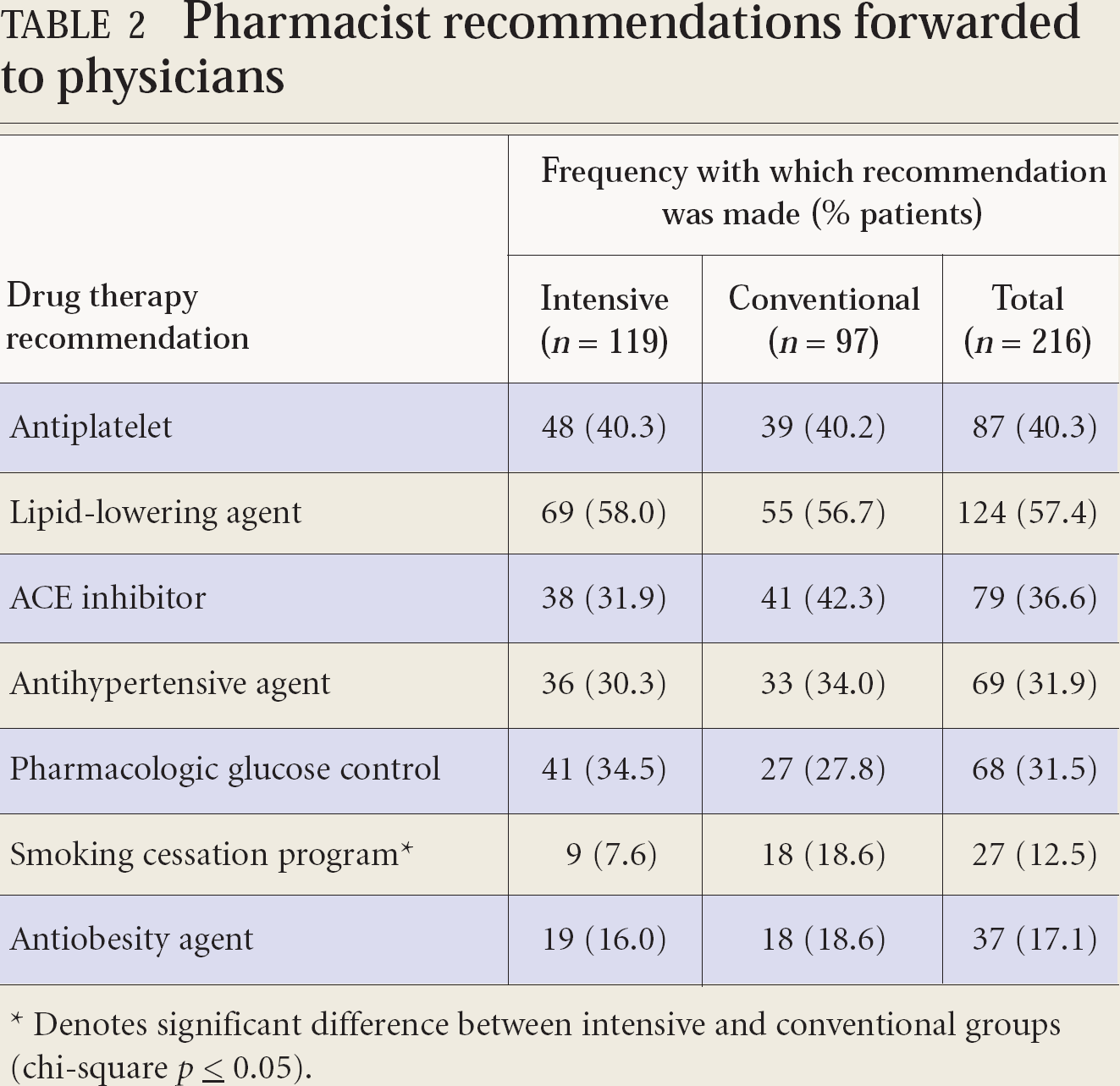
Denotes significant difference between intensive and conventional groups (chi-square p ≤ 0.05).
Table 3 reports the outcomes of the pharmacist recommendations. The intervention acceptance rate was 35.8% in the intensive group and 23.8% in the conventional group, which differed significantly (p ≤ 0.05).
Physician acceptance rate of pharmacist recommendations
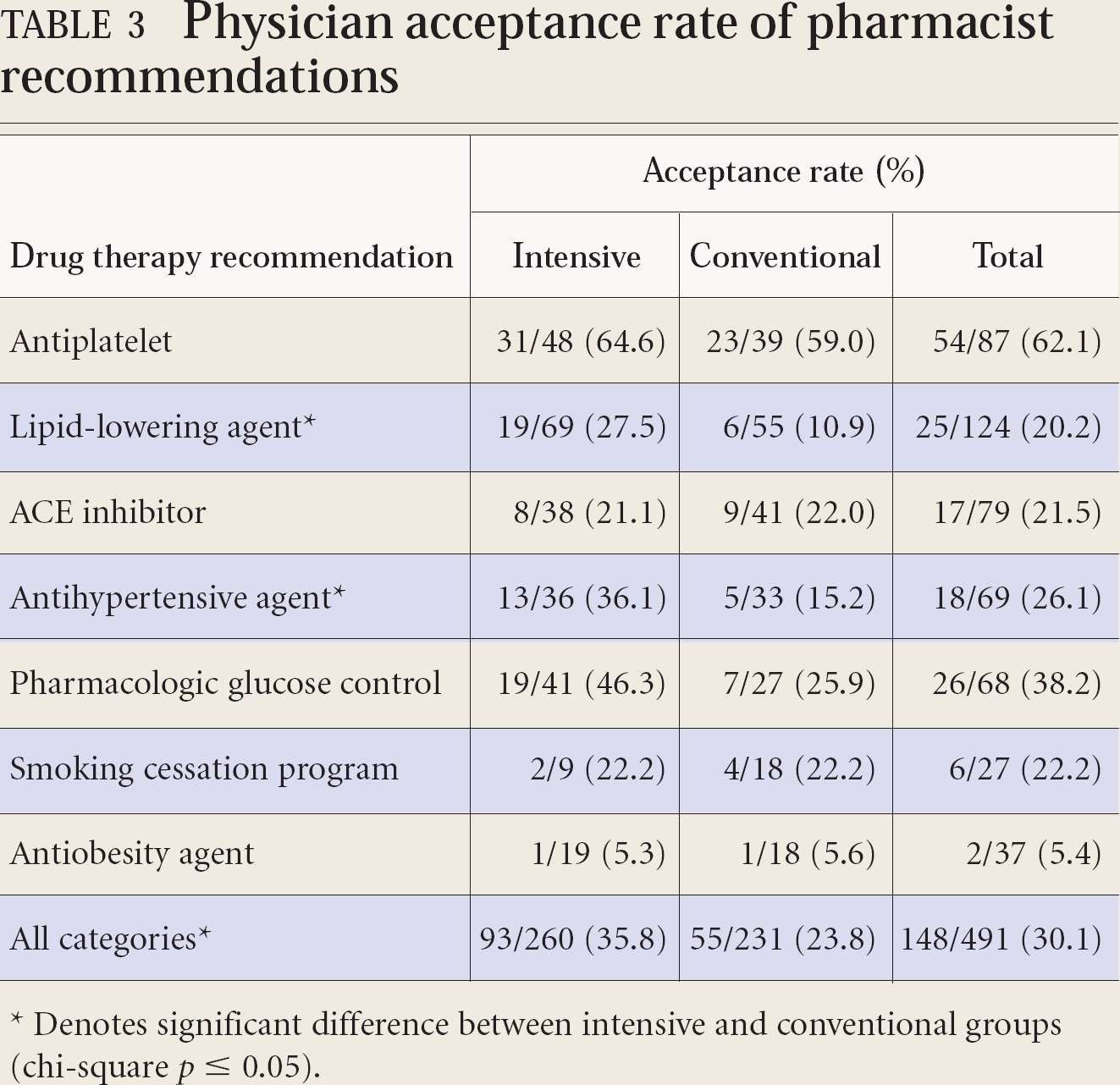
Denotes significant difference between intensive and conventional groups (chi-square p ≤ 0.05).
Table 4 depicts the percentage of patients on drug therapy for each educational group, as well as the change seen for both groups from the time of baseline to finishing the study.
Percentage of patient drug utilization at baseline and study exit for each educational group
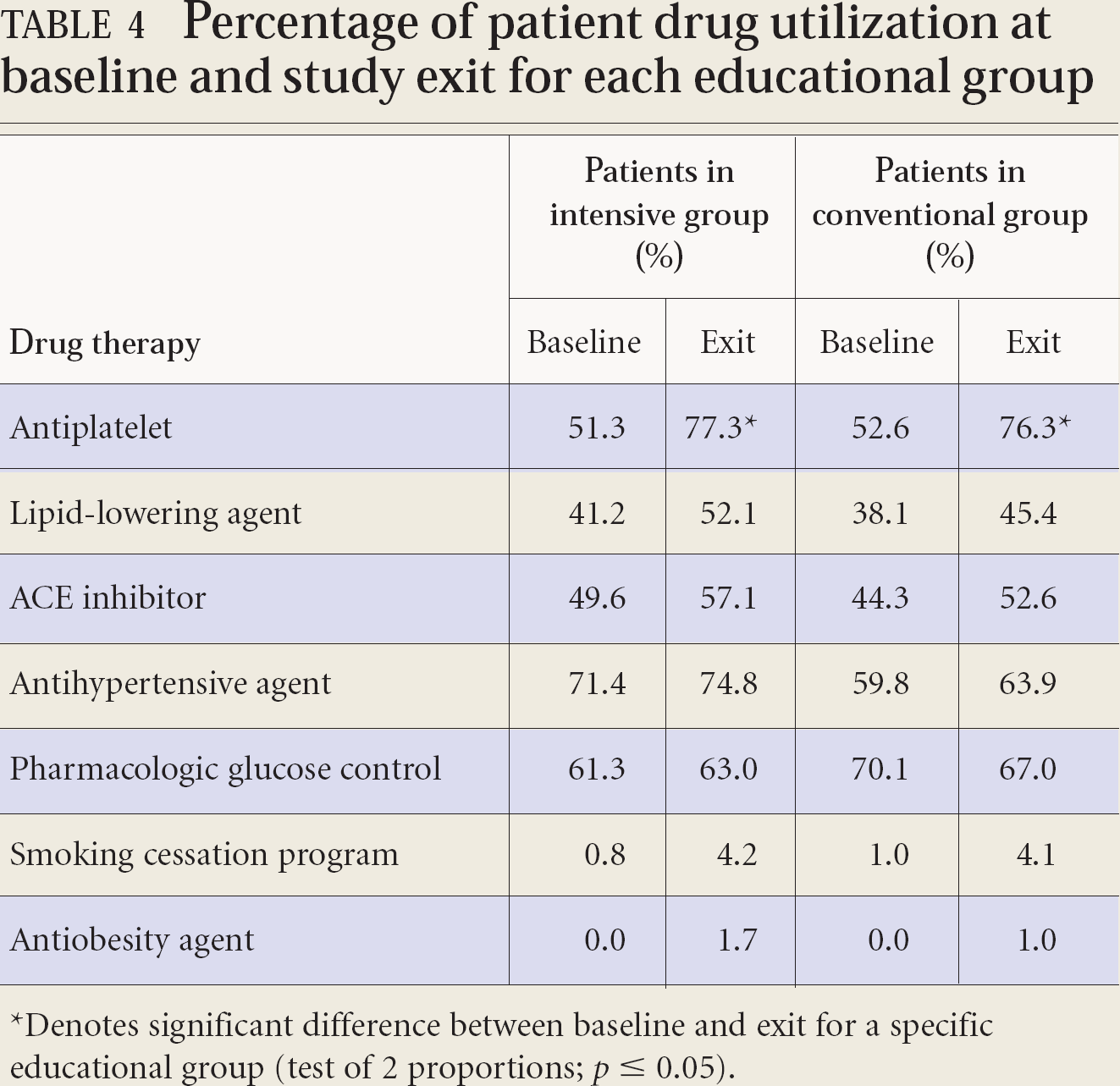
Denotes significant difference between baseline and exit for a specific educational group (test of 2 proportions; p ≤ 0.05).
Discussion
From the clinical pharmacy movement on through to pharmaceutical care, pharmacists have been asked to adapt to change by undertaking new professional activities. Researchers have attempted to assess the propensity for pharmacists to adopt such changes. 25 –30 These reports provide conclusions that change is never quick enough or taken to the appropriate extent.
Pharmacists working within teams are one example of an adaptation for improved patient care. In spite of much prodding, practice change is a difficult endeavour at the best of times. Pharmacists exist within health care systems that may or may not be conducive to such pursuits. Having the time, the motivation, the staffing, and the skills required to be successful are other factors obviously in play.
The PIRR program was created to improve cardiac patient care in Saskatchewan through community pharmacists who worked in conjunction with primacy care physicians. The goal of the educational interventions was to induce a practice change — adopting a new cardiovascular risk assessment service — in participating pharmacists. We did not reach our patient recruitment goal of 376 patients per group; thus, interpretation of the results is somewhat difficult since, in essence, the study was underpowered. That said, statistical significance was still found. What this potentially means is that the effect size estimate was greater (less conservative) than anticipated during sample size determination, resulting in fewer patients being needed. According to the results, the higher proportion of patients who had their risk reduction therapies enhanced in the intensive group provides some evidence that intensive training better equipped community pharmacists to identify and assess high-risk patients than those pharmacists who were trained via a traditional didactic presentation.
It was conceivable that more intensively trained pharmacists might forward stronger arguments to physicians for drug therapy modifications. One might therefore expect to see higher intervention acceptance rates for the intensive group. Indeed, this was the case, with significant differences seen for lipid-lowering and antihypertensive agents, as well as overall in all categories. No acceptance rate, however, ascended beyond 65%, and this may reflect physician priorities for care. Physician confidence in the skill level of pharmacists may also have been a factor. 31
If the intensive educational arm was in fact superior at motivating pharmacists to take on this new practice behaviour, the patients enrolled per pharmacist should have been higher and, one would suspect, the pharmacist dropout rate lower, than the conventionally trained group. We saw trends to support the hypothesis, but the 2 groups did not differ statistically to a great extent on these 2 measures. Again, this could be due to insufficient patient numbers.
Changing behaviour within any health care profession is a daunting and complex task. 32 –36 The Holland-Nimmo model of practice change proposes that 3 elements must be considered when adopting a new behaviour: 1) the practice environment, 2) practitioner motivation, and 3) education. 37 First, the practice environment must support the new activity. The pharmacists, for example, in the present study needed to have time away from dispensing duties and to have access to a reasonably private counselling area to conduct patient interviews. To help attenuate financial issues, we hoped that the small payment seen here would offset some barriers within the practice environment. 23 The current project was not designed, however, to assess the impact of professional reimbursement on pharmacist behaviour. 38,39
A second requirement for change is that practitioners must be motivated to take on the new role. On entry into this study, both groups of pharmacists were likely equally motivated, because they were among the approximately 1% of the province's pharmacists who responded to the call for volunteers. It was therefore assumed that motivation was high for all participants. It was also assumed that those who did volunteer had the necessary resources or staffing in place to allow some degree of success in this endeavour. However, there were dropouts, so a number of participants may have become overwhelmed when they became aware of the full extent of what was being asked. There was less pharmacist dropout within the intensive training group (37.0% vs 58.8%), suggesting that those with such training may have had more confidence and competence when entering their first patient.
The third and most easily manipulated requirement for fostering practice change is education. Nevertheless, all 3 elements must be addressed, and all the advanced training available to a pharmacist may not change practice realities once returning home. Our limited ability to impact 2 of those 3 elements may explain the lower-than-anticipated patient recruitment observed during the study period, yet differences did show up between educational groups. This bodes well for practice. A similar comparison involving physicians in Halifax found greater gains in knowledge and program satisfaction with problem-based learning than that seen with a lecture-based format. 38 Fjortoft and Schwartz, however, found that a lipid and hypertension educational program for pharmacists, with a combination of self-study and 3 interactive workshops, improved pharmacist skill, but not actual practice behaviours. 41
To determine the success of any given program, comparison to some form of standard is required. It was difficult to ascertain what would constitute a control group for the study reported here. It was believed that the therapeutic content given to both groups was of high quality, delivered by a cardiovascular care expert. Thus, the conventional group perhaps does not represent a true placebo control of “usual care.” That said, comparisons are still possible between the groups, and in this situation, intensive training fared better than the alternative. We suspect that use of proxy patients during the interactive cases played a significant role in better preparing pharmacists to make interventions. An e-group was set up for the intensive group as a forum for continued motivation, discussing challenging cases, and to share recruiting strategies or practice tips, but it was used rarely and eventually abandoned. Feedback from physicians was not systematically obtained, but anecdotal reports were mostly positive.
Aside from suboptimal statistical power, the study was limited by a failure to obtain both pre- and post-training assessments of pharmacist confidence in practice skills, satisfaction, change in pharmacist knowledge, and the ability of the educational interventions to meet the needs of the volunteers. It was also a shortcoming to omit addressing the reasons pharmacists were unable to enter patients or provide follow-up to completion. This may have been due to new dynamics at the pharmacy level, but may reflect the quality of the educational activities.
Other limitations included the difficulties inherent in conducting educational trials, such as lack of blinding 42 and the difficulty (if not impossibility) in maintaining group integrity with respect to training received. Participants of either group, for example, may have taken further action toward enhancing their skills in this area. Of note, non-PIRR pharmacies ran several other heart health clinics during the course of this study.
A comparison of the training costs would have been useful data to consider for designing future programs aimed at promoting the uptake of expanded services by pharmacists.
Conclusion
The goal of this endeavour was to enable pharmacists, in conjunction with primary care physicians, to improve upon the care of at-risk cardiovascular patients. Such patients represent a group that will experience significant morbidity and mortality and are in dire need of specific risk reduction measures. Unfortunately, many barriers still exist in the pharmacy practice environment, and overcoming them continues to be a slow and arduous process. The efforts presented here focused on one main component for changing practice — training.
We compared training that might be given during a typical evening continuing education event against an intensive day-long event with interactive cases. Although costs were not taken into consideration, the extra effort appeared to pay off. Intensive training for pharmacists was more likely to result in improvements in cardiovascular risk reduction therapy than when conventional training was used.
Footnotes
Funding for the PIRR study was provided by educational grants from Aventis Pharma Canada Inc., the Canadian Foundation for Pharmacy, and the Pharmacy EduLab Program (University of Saskatchewan).
Acknowledgements:
The authors would like to thank Dr. Michelle Diment for her contributions in developing the study protocol and educational events.