
Abstract

Background
Proton pump inhibitors (PPIs) treat upper gastrointestinal conditions such as gastroesophageal reflux disease. They resolve symptoms in about 80% of patients, with erosions present after 4 to 8 weeks of treatment (and about 60% of patients without erosions). 1 Although the majority of patients with severe symptoms relapse if therapy is discontinued, patients with mild or moderate symptoms may not need continuous daily PPI therapy long term. 1 Prospective observational studies and cross-sectional studies suggest rates of inappropriate PPI use between 44% and 79%.2-5 Meta-analyses of cohort and case-control studies suggest PPIs may be associated with harms including Clostridium difficile infection, pneumonia and fractures,6-8 although some of these associations have been challenged. 9 Public drug programs in Canada spent $247 million on PPIs in 2012. 10
The decision to continue a PPI, use a lower dose, or stop and use on demand (only when symptoms come back) should be informed and made collaboratively between a patient and clinician (prescriber or pharmacist). Supervised dose reduction or stopping a medication that may no longer be needed is termed deprescribing.11,12 Our research group conducted a systematic review 13 and developed a PPI deprescribing guideline to assist clinicians in deprescribing PPIs where appropriate,13,14 and we have been exploring ways to implement these tools.
Patients may fear deprescribing and not understand when it can be considered. 15 Qualitative evidence suggests that patients accept PPIs as appropriate if their physician continues to prescribe them. 16 Even when a clinician feels deprescribing a PPI is appropriate, patients struggle to decide whether they wish to pursue deprescribing. 15 Thus, there is an opportunity to educate patients about this decision. Patients should feel confident in the decision they make and make a decision that is consistent with their values. 17 They should have sufficient knowledge of their options and of possible outcomes.17,18
Patient decision aids (PtDAs) outline the probability of benefit and harm associated with different treatment options and allow patients to identify what matters most to them. 19 They increase knowledge, help patients feel supported in their decision and achieve decisions congruent with values. 19 PtDAs can be delivered in consultation with a health care professional. Pharmacists are well positioned to implement consultation PtDAs, which can be delivered in a 10- to 15-minute visit. 20 A 2014 systematic review (n = 21 studies) suggests prescribers’ lack of access to resources (e.g., a pharmacist) and knowledge is a barrier to deprescribing. 21 Pharmacists can help to overcome these barriers and are therefore a key resource in engaging patients to discuss deprescribing.
We developed a consult PtDA to support patients in making the decision of whether to continue, stop and use on demand, or use a lower dose of PPI and will evaluate the effect of the PtDA when delivered by a pharmacist (http://deprescribing.org/resources/deprescribing-patient-decision-aids/). We also aim to show how pharmacists, as drug therapy experts, can act as key facilitators of the discussion surrounding deprescribing and the deprescribing process.
Methods/Design
Research questions
In patients ≥18 years of age who have used PPIs for >4 weeks with upper gastrointestinal symptom resolution and who have no indication to continue treatment, does a PtDA aimed at helping patients decide whether to continue a PPI or stop and use on demand/use a lower dose of their PPI: affect patient decision preference? improve patient knowledge surrounding the decision? affect patient expectations? affect decisional conflict? produce choices that are congruent with patient values?
When the PtDA is provided in consultation with a pharmacist, does shared decision-making take place (according to both the patient and clinician)?
Eight weeks after patients have received a consultation involving the PtDA, what is the effect on prescribing of PPIs?
In patients who have chosen to use a lower PPI dose or stop and use on demand, is there any difference in symptom control at 8 weeks compared with those who have continued taking their PPI?
Design of the study
This study will use a before/after design. This study design is recommended for pilot testing of PtDAs according to the International Patient Decision Aid Standards (IPDAS) and has been widely used to this end.18,22-24
Patients will have an appointment with a pharmacist to go through a PtDA to discuss the decision (probabilities of benefit and harm, individual values and preferences). Following the appointment, patients can follow up with their family physician should they wish to pursue deprescribing or can receive instructions from the pharmacist. While the pharmacist is conducting the study visit, implementing the decision aid is a collaborative effort. For example, prescribers have referred patients to the pharmacist to discuss their PPI, and pharmacists can discuss the eligibility of a particular patient with the prescriber in advance of an appointment.
The PtDA has been developed using a user-centred design approach, which included patient representatives as part of the development committee.25,26 The PtDA was drafted using an online tool (https://decisionaid.ohri.ca/eTraining/) and qualifying, certification and quality criteria set out by IPDAS. 27 It was revised in iterations based on feedback from our team.
Setting and participants
We set out to conduct the study at 2 Ottawa area primary care clinics, but because of low recruitment, we have expanded to recruit units at a continuing care hospital. Eligibility criteria are outlined in Table 1. Our study protocol has been approved by the Bruyère Research Institute and Ottawa Health Science Network Research Ethics Boards.
Eligibility criteria
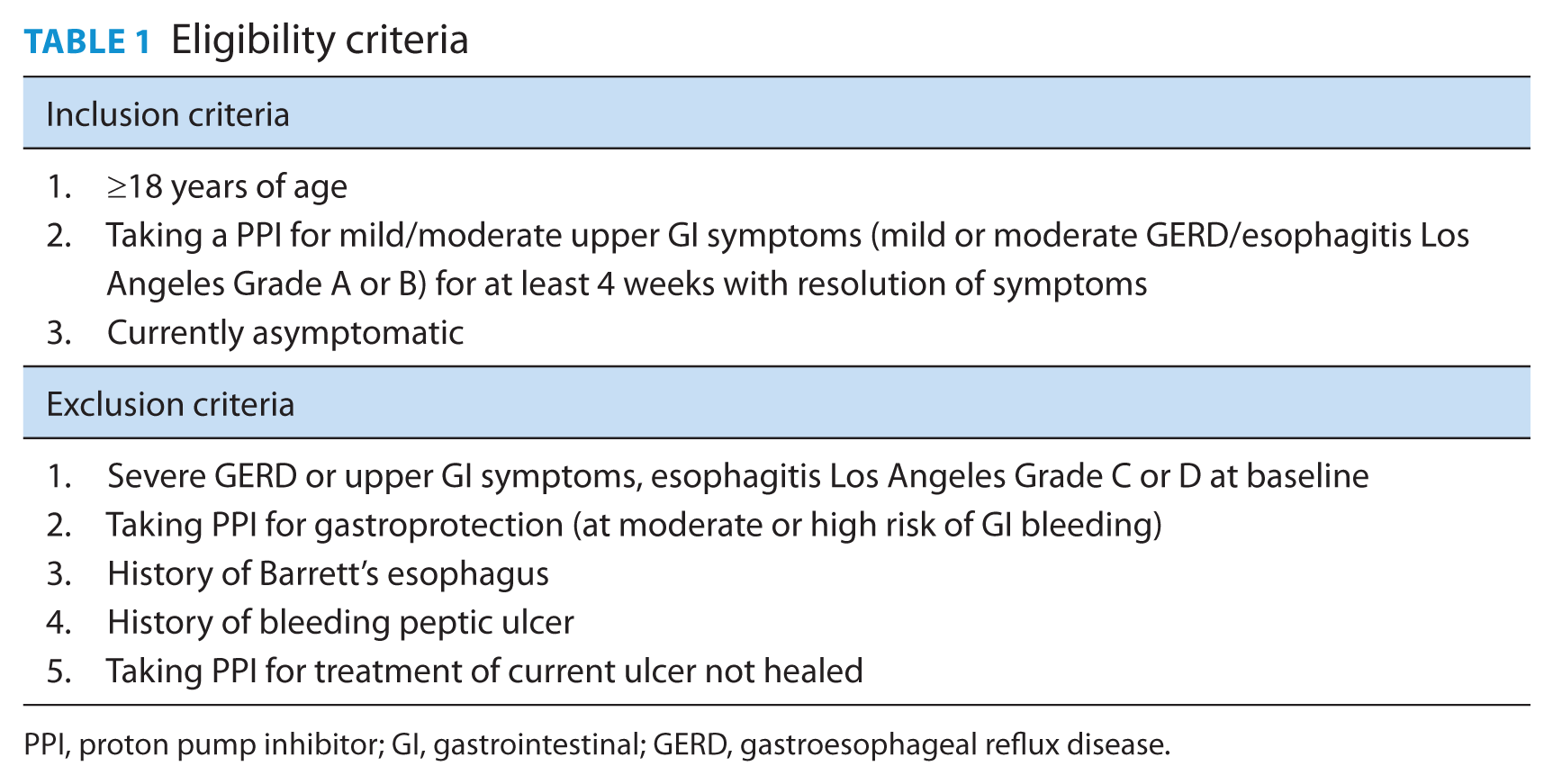
PPI, proton pump inhibitor; GI, gastrointestinal; GERD, gastroesophageal reflux disease.
Analysis
We will use the SURE test to measure decisional conflict/confidence. 28 We will also measure patient knowledge and realistic expectations before and after using the PtDA (Appendix 1 available at cph.sagepub.com/supplemental). We will analyze these continuous outcomes with paired t tests (5% significance level). Patients will be asked to indicate which option they prefer (continue PPI, stop and use on demand/use a lower dose, or unsure) before and after the consultation, and we will analyze this outcome using McNemar’s test (5% significance level). The congruence between patients’ choice and values will be evaluated using multivariable logistic regression. 29 Both the patient and pharmacist will rate the perception that shared decision-making took place using the control preferences scale,30-32 and the agreement between patient and pharmacist ratings will be measured. After 8 weeks, the proportion of patients continuing on PPIs at their pre-PtDA dose will be measured. Symptoms will also be assessed at 8 weeks in all patients. 33 Our sample size is based on the paired difference in the proportion of patients preferring to continue on their PPI before the PtDA consult compared with after. 34 To detect a difference in paired proportions of 15% (80% power, alpha of 5%), we need a sample size of 54.
Discussion
Our research group developed 3 deprescribing guidelines, the first of which focuses on PPIs. We also implemented our deprescribing guideline into primary care practices 35 in a previous phase of our research. This PtDA is a tool to further facilitate implementation of these guidelines and involve patients in the decision-making process. We recognize the importance of patient values surrounding the decision to continue or stop a medication; thus, we want to empower patients to make an informed decision.
A 2014 systematic review (n = 21 studies) suggests that barriers to prescribers discussing deprescribing include lack of prescriber time during appointments, competing priorities, access to key resources (e.g., a pharmacist) and lack of a stimulus to review medications. 21 This project seeks to overcome those barriers by having a pharmacist use his or her knowledge and expertise to become a champion of appropriate PPI use and to have dedicated 10- to 15-minute appointments to address this issue.
The 2014 systematic review described above also noted challenges in confirming the indication or rationale for a drug being started, as well as uncertainty about whether a patient was eligible for deprescribing. 21 This problem has also been described by other researchers. For example, an Australian study to reduce inappropriate PPI use could not verify the indication for 15 out of 57 patients. 3 We have encountered similar difficulties in recruiting patients so far, where it has been time-consuming to identify eligible patients and there is uncertainty about whether a patient is eligible to consider the option of having a PPI deprescribed. Thus, while inappropriate PPI prescribing appears to be common, actually attempting interventions to reduce PPI use in practice is challenging.
Our study is limited by a before/after design and a small sample size. However, it will provide valuable information about whether the PtDA is helpful and impactful in clinical practice. This study will lay the foundation for a larger randomized controlled trial to more thoroughly investigate whether our PtDA influences decisions surrounding PPI treatment and actual PPI prescribing rates. Widespread utilization of our PtDA could reduce rates of inappropriate PPI use and thus the incidence of rare harms and unnecessary health care expenditures.
Footnotes
Acknowledgements
The authors would like to acknowledge Dr. Dawn Stacey for her suggestions surrounding study design and analysis.
Author Contributions:
All authors conceived the study and its design. W. Thompson prepared the draft manuscript and received critical feedback from B. Farrell, V. Welch, P. Tugwell and L. M. Bjerre. All authors approved the final version of the manuscript for submission.
Declaration of Conflicting Interests:
All authors have completed the ICMJE uniform disclosure form at ![]() and declare no support from any organization for the submitted work. W. Thompson reports an MSc stipend from the Government of Ontario; L. M. Bjerre reports personal fees and nonfinancial support from Department of Family Medicine, University of Ottawa, nonfinancial support from Bruyère Research Institute, grants from the Canadian Institutes for Health Research, grants from the Ministry of Health and Long-Term Care of Ontario, outside the submitted work; no other relationships or activities that could appear to have influenced the submitted work.
and declare no support from any organization for the submitted work. W. Thompson reports an MSc stipend from the Government of Ontario; L. M. Bjerre reports personal fees and nonfinancial support from Department of Family Medicine, University of Ottawa, nonfinancial support from Bruyère Research Institute, grants from the Canadian Institutes for Health Research, grants from the Ministry of Health and Long-Term Care of Ontario, outside the submitted work; no other relationships or activities that could appear to have influenced the submitted work.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.