
Abstract

Health care professionals in all sectors are in the midst of adapting to the complexities of our aging population. Comorbidities that emerge or deteriorate can lead to well-intentioned prescribing of increasing numbers of medications, adding further complexity and contributing to higher use of acute care services and mortality among older adults.1,2 Assessment of medication regimens can help reduce the use of inappropriate medications and improve patient outcomes.3 -5 The role of pharmacists conducting medication reviews has been recognized through remuneration programs across Canada. 6 In most practice settings, however, the potential demand for this service exceeds the available manpower resources and necessitates judicious consideration of which patients could derive the most benefit.
Pharmacists commonly use the number of medications, presence of “high-risk” medications and/or specific medical conditions to triage patients. Although these approaches often result in interventions to reduce polypharmacy and/or to optimize pharmacotherapies for particular disease states, they may miss patients who could benefit from a comprehensive medication review, including those for whom additional medications may improve health outcomes. 7 An additional criterion to signal the need for a medication review in older adults, which represents a more holistic approach, is frailty.
Although frailty is not a new concept, there is no universal agreement to a practical definition and assessment. 8 Typically, the definition of frailty encompasses an age-related decline in physiological reserve, beyond that expected from normal aging, that leads to heightened vulnerability to stressors, including changes in medications. 9 This vulnerability increases the potential for poor outcomes such as falls, delirium, worsening disability, admissions to hospital, need for a higher level of care and death. In addition, frailty can overlap with comorbidity and disability but is distinct from them.8,10
Frailty and medications
Owens et al.11,12 have highlighted the use of frailty to identify older adults for the purpose of optimizing pharmacotherapy to avoid decline in function. Recently, Cullinan et al. 13 found a correlation between a patient’s frailty index and prescribing of potentially inappropriate medication, as well as the likelihood of developing an adverse drug reaction.
Frailty can be modifiable and have some degree of reversibility; hence, medication optimization may reduce both frailty and subsequent undesirable outcomes.9,14-16 For example, cognitive impairment and low physical activity, which may be affected by medications, have been shown to be associated with increased frailty. 17 Moreover, just as frailty is an independent risk factor for adverse outcomes such as falls and delirium, so is polypharmacy.18,19 This complements the deprescribing literature, in which improved patient outcomes have been reported in multiple practice settings, following medication reductions.20 -22 Clear evidence that polypharmacy affects transitions among frailty states may be lacking, but it has been associated with increased risk of mortality.2,16
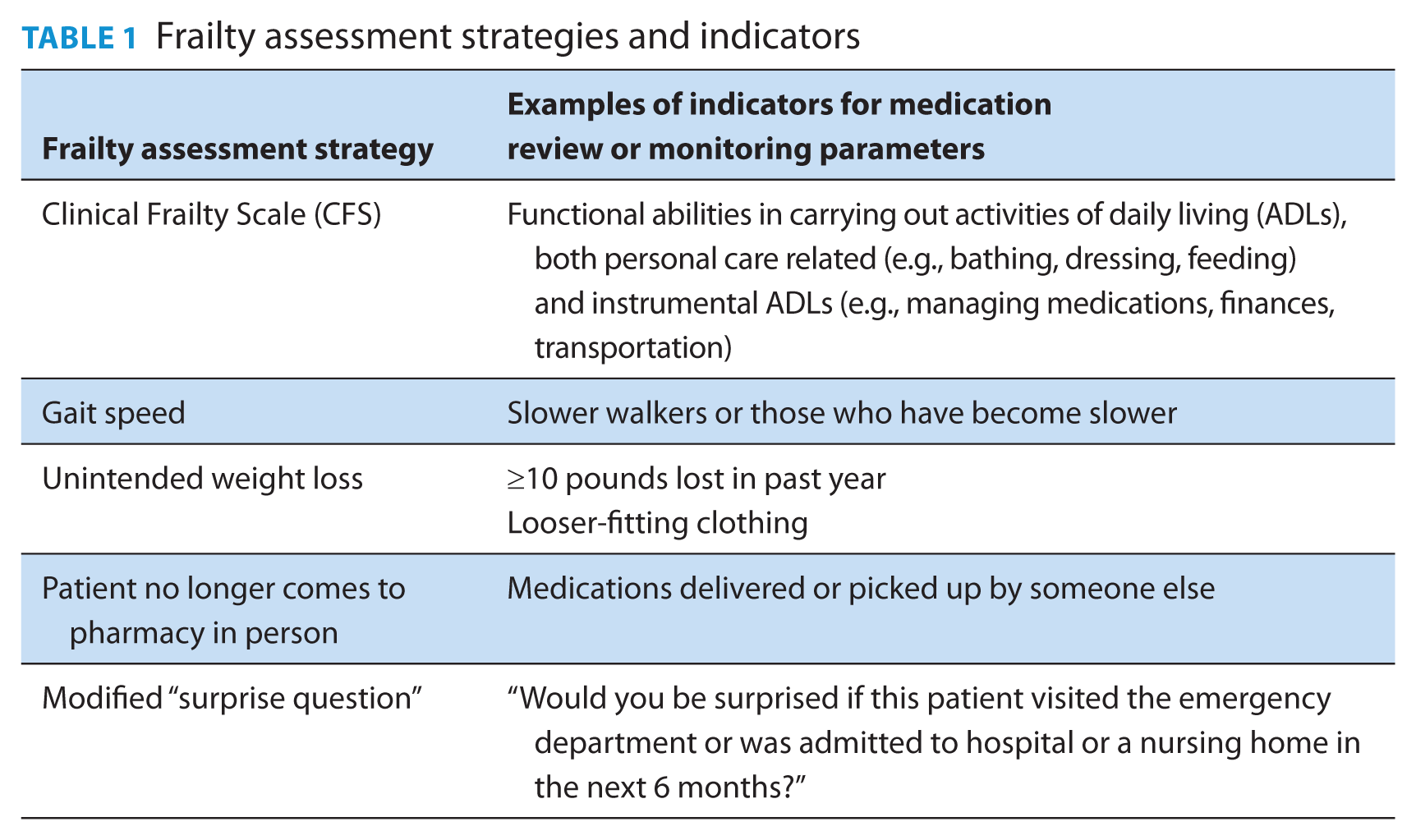
In order to successfully integrate the concept of frailty into pharmacy practice for the purpose of identifying patients who may benefit from a medication review, there is need for quick practical assessments. Some options are outlined in Table 1 and discussed below:
The Clinical Frailty Scale (CFS)23,24 is a 1-page tool that describes 9 stages of function from very fit to terminally ill, with scores of 5 (mildly frail) to 8 (very severely frail) indicating decline that correlates with the potential for increasingly poor outcomes8,9 (Appendix 1, available in the online version of the article). Through discussion with a patient or caregiver about a patient’s ability to carry out activities of daily living (ADLs), a pharmacist can quickly score a patient’s level of frailty.
The CFS is commonly used by multidisciplinary teams to guide the setting of patient goals that in turn guide the development and adjustment of therapeutic plans. With changes in frailty levels, patient goals can fluctuate depending on the occurrence of new stressors and patient response. An event that leads to increased frailty may lead patients to request a dramatic change in their goals of care, which can subsequently affect their overall treatment plan. Therefore, ongoing monitoring is required to determine how these changes need to affect a medication regimen.
Slow gait speed, defined as taking more than 10 seconds to walk 10 feet (~0.3 m/s), is a frailty criterion that has shown to be predictive of chronic disability and long-term nursing home stay, as well as being associated with injurious falls. 17 Other authors have reported that average gait speed varied from ~0.6 m/s in those deemed frail to ~1.0 m/s in those considered “prefrail” and ~1.1 m/s in “not frail” individuals. 25 Walking speed was also shown by Odden et al. 26 to affect the association between blood pressure and mortality. Despite the variability in gait speed definitions and implications, pharmacists can make observations about patients’ mobility and changes in mobility to signal possible decline in frailty.
Unintended weight loss is another indicator of frailty and has been associated with chronic disability, long-term nursing home stay and death. 17 Availability of an accurate, accessible weigh scale in a community pharmacy could assist with identification and monitoring of weight loss.
Increased level of frailty is a common reason that an older client/patient is no longer able to visit his or her community pharmacy. In these cases, a home-based medication review may be warranted.
Another assessment that could be relevant to this topic is a modified version of “the surprise question.” Most commonly used in palliative care, experienced health care practitioners use their clinical judgement to respond to “Would you be surprised if this patient died in the next year?” to guide when to initiate discussions with patients and families regarding whether it is time to change to a palliative rather than curative approach. 27 In the context of older adults and medications, the clinician can consider the patient’s risk of hospitalization, emergency room visit or nursing home admission in the next 6 to 12 months.
Frailty assessment strategies and indicators
While there may be no perfect strategy to identify those who could benefit from a pharmacist-performed medication review, using frailty as a criterion may be a way to more holistically and practically do so. Frailty can also be used as a referral criterion that can be easily communicated to others (health care professionals and the public). Any of the above options can be used to not only identify those with advancing frailty but also to monitor the impact of medication changes. The bigger challenge will be to demonstrate improved outcomes (reduced emergency department visits or hospital and nursing home admissions) to this approach.
Footnotes
Author Contributions:
L. Blain wrote the initial draft of the article. L. Blain and P. Flanagan reviewed and revised the article. Both authors approved the final version of the article.
Declaration of Conflicting Interests:
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding:
The authors received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.