
Abstract
Background:
The recent legalization of cannabis use in Canada requires pharmacists to be able to support their patients with accurate knowledge of its known risks and benefits. Certain populations, such as pregnant and breastfeeding women and their developing children, may be at higher risk than other populations.
Methods:
The authors independently searched the literature for clinical reports or reviews of the literature regarding the safety of cannabis use in pregnancy and breastfeeding using search terms such as cannabis, marijuana, pregnancy and breastfeeding.
Results:
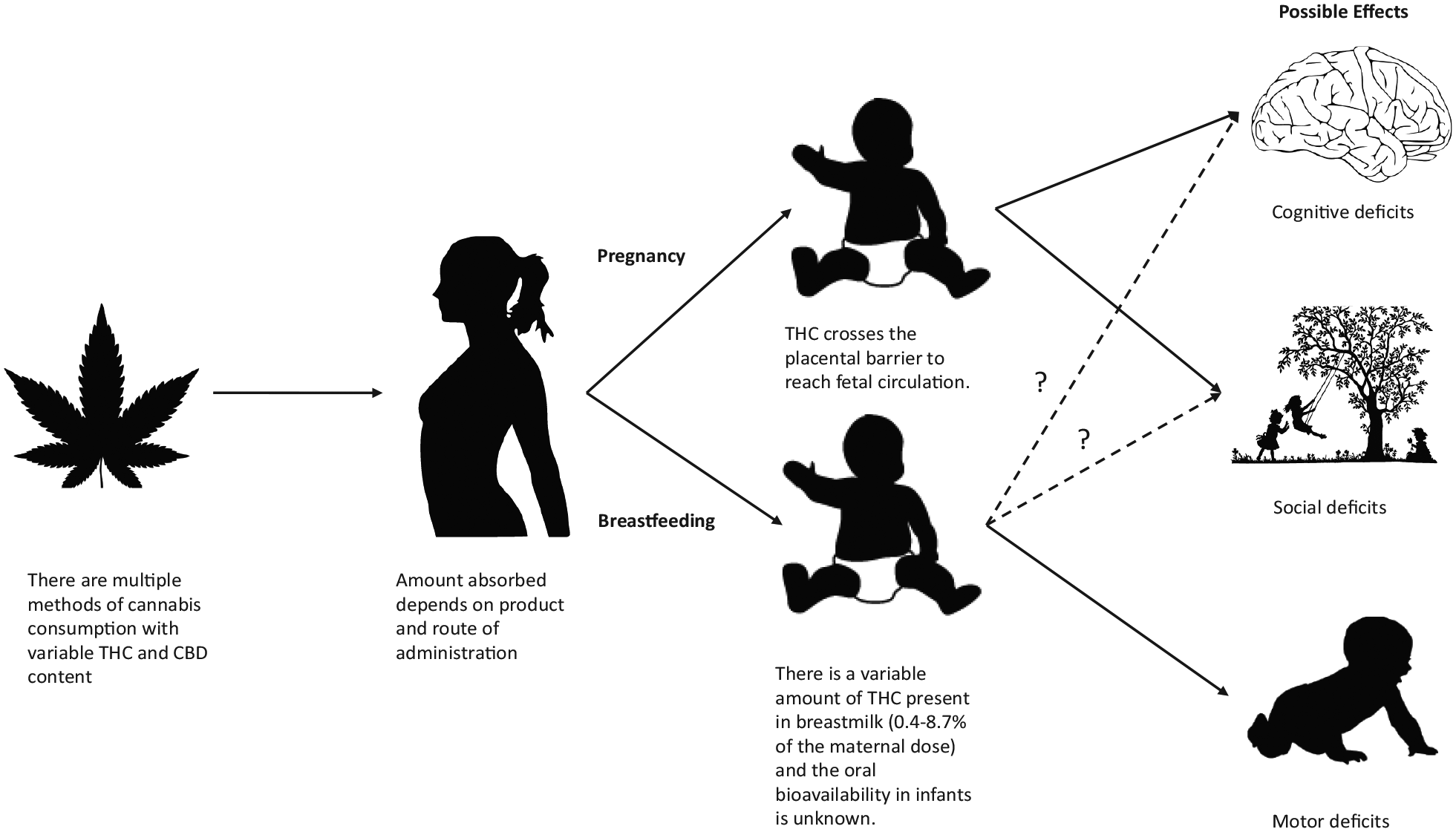
This review combines the relevant pharmacological, pharmacokinetic and clinical evidence for the effects of cannabis in this special patient population. The literature demonstrates that some of the constituents of cannabis can reach children in utero and through breastmilk. Given that Δ⁹-tetrahydrocannabinol can be present in breastmilk as quickly as 1 hour after consumption and last up to 6 days, it may not be possible to use cannabis and avoid infant exposure. There is evidence that this exposure may result in cognitive, social and motor defects. Some of these effects may be long term, lasting years. The pharmacist must be able to educate and screen patients regarding marijuana use in pregnancy and breastfeeding, with the ultimate aim of harm reduction.
Introduction
The recent legalization of cannabis for recreational use in Canada is projected to result in approximately 6% of people who were not previous users trying cannabis products. 1 Marijuana is a broad term referring to the dried flowers, seeds, stems or leaves of the Cannabis sativa or Cannabis indica plants. Recreational cannabis is administered in many ways, including smoking, vaping, orally and by topical routes. 2 The effects of cannabis vary depending on patient factors (e.g., age, sex, mental and physical health, other medication and substance use), factors specific to the product ingested (e.g., potency, amount used) and the chronicity of use. Chronic use lacks a consistent definition but has been defined by researchers cited in this article as either 3 puffs per day or 7 uses per day.3,4
While cannabis contains more than 700 different chemical compounds, the components most commonly used for their pharmacological effect, known as cannabinoids, are Δ⁹-tetrahydrocannabinol (THC) and cannabidiol (CBD). 5 These compounds act by binding to cannabinoid receptors in the nervous system. THC is commonly associated with feelings of euphoria while CBD is considered to be more active medicinally, causing no obvious feelings of euphoria and impairment. 5 A wide array of cannabis products is available for purchase, and they are typically described by their THC and CBD content.
Knowledge Into Practice
Public perception of the safety of marijuana is evolving; with the ongoing normalization of the use of cannabis products, more pregnant and breastfeeding women may engage in recreational use of marijuana.
Given the pharmacokinetics of cannabis in nursing women, it is very unlikely for a patient to consume cannabis products and not have some appear in their breastmilk.
Pregnant and breastfeeding women should abstain or minimize their cannabis use as there is evidence that cannabis exposure during pregnancy and breastfeeding may result in cognitive, social and motor defects in children.
Where cannabis use is not avoided, the pharmacist should educate on potential short- and long-term effects of exposure to the infant.
Mise En Pratique Des Connaissances
La perception du public à l’égard de l’innocuité de la marijuana évolue; en raison de la normalisation en cours de l’utilisation des produits du cannabis, de plus en plus de femmes enceintes et qui allaitent peuvent s’adonner à l’utilisation récréative de la marijuana.
Compte tenu de la pharmacocinétique du cannabis chez les femmes qui allaitent, il est très improbable que le lait d’une patiente qui consomme des produits du cannabis ne contienne pas de cannabis.
Les femmes enceintes et qui allaitent devraient s’abstenir de consommer du cannabis ou réduire leur consommation, car il existe des données probantes démontrant que l’exposition au cannabis pendant la grossesse ou l’allaitement peut entraîner des déficiences cognitives, sociales et motrices chez l’enfant.
Lorsque l’utilisation du cannabis se poursuit, le pharmacien devrait présenter les effets à court et à long terme de l’exposition pour l’enfant.
Evolving perception of risk
The public perception of the safety of marijuana has changed significantly over time, and this has been reflected in the prevalence of marijuana use. In 2015, approximately 10% of Canadian adults and 25% of Canadian youth ages 15 to 24 reported consuming marijuana during the previous year. 6 In the 2017 Canadian Cannabis Survey, the majority of respondents also believed that marijuana use had no effect on their work or studies, marriage, physical mobility or physical health and had positive effects on mental health and quality of life. In addition, 60% of respondents who used marijuana for medical purposes indicated that either it had no effect on their ability to drive or that “it depends.” 6
Survey data from the United States estimate that 5% to 35% of pregnant and breastfeeding women are using marijuana.7,8 Ten percent of these women indicated that they would have used marijuana more during pregnancy if it had been legal. 7 Marijuana use does tend to drop off as pregnancy progresses, similar to the trend seen with opioid use in pregnant women.9,10 One study showed that the percentage of pregnant women who believed smoking marijuana posed “no risk” increased from 3.5% to 16.5% over a 7-year study. 11 Pregnant women may also be receiving advice to consume marijuana for nausea associated with pregnancy, as reported by a study in Colorado. Sixty-nine percent of dispensaries and 83% of those with a medical license to dispense recommended marijuana for nausea in pregnancy. 12 Eighty-five percent of lactation professionals recommended breastfeeding while using marijuana in 1 US survey. 13
There is an ongoing normalization of the use of cannabis products. This normalization contributes to pregnant women receiving advice from friends and dispensaries to use marijuana in the first trimester to treat nausea. This societal shift underscores the responsibility for pharmacists to be knowledgeable about the known effects of marijuana in pregnancy and breastfeeding and to be prepared to counsel patients on how to minimize risks both known and unknown (Figure 1).
Concerns about cannabis in pregnancy and breastfeeding
Cannabis in pregnancy and breastfeeding
THC, a small highly lipophilic molecule, is known to cross the placental barrier into fetal circulation and accumulate with repeated exposure. 14 There have also been a number of studies demonstrating that THC and CBD may be detectable in human milk up to 6 days after use and that THC accumulates in breastmilk with chronic, heavy exposure.3,4 It is also known that THC is rapidly distributed to and stored in the brain and fat tissues and has an estimated half-life of 4.1 days in chronic cannabis users. 15 The potential for cannabinoids to adversely affect developing fetal and infant brains led the Society of Obstetricians and Gynecologists of Canada and the Motherisk program, formerly run through SickKids, to recommend that all pregnant and breastfeeding women abstain from marijuana use.16,17 The Canadian Pediatric Society has not published a statement on the use of marijuana in pregnancy and breastfeeding, but the American Association of Pediatrics has spoken out on the issue and recommended education and abstinence from cannabis products during pregnancy and breastfeeding. 18
Pregnancy
The literature on maternal use of marijuana in pregnancy has shown mixed results on children’s development. The literature initially supported negative outcomes in the immediate postnatal period, such as low birth weight, increased risk of neonatal intensive care unit admission, preterm birth and behavioural outcomes such as increased startling and tremors.19-22 More recently, a large meta-analysis was published, including 31 observational studies of varying quality, that demonstrated that the association between marijuana and negative outcomes in infants became insignificant when other substance use was controlled for, such as alcohol and nicotine. 23 The association persisted, however, in women who reported heavy use.23,24 There is also evidence to suggest that the concurrent smoking of nicotine and marijuana results in a greater risk of negative outcomes in the infant than use of either alone.25,26
Despite the lack of strong evidence of negative outcomes in the short term, there is substantial evidence of long-term harm from prenatal marijuana exposure. Three prospective cohorts have reported on the effects of perinatal marijuana exposure.9,25,27 Although results by age were mixed, all 3 consistently found associations between prenatal exposure to marijuana (especially in the first trimester) and persistent behavioural and cognitive deficits later in childhood (Table 1).
Cannabis impact on infant outcomes: Evidence from human studies
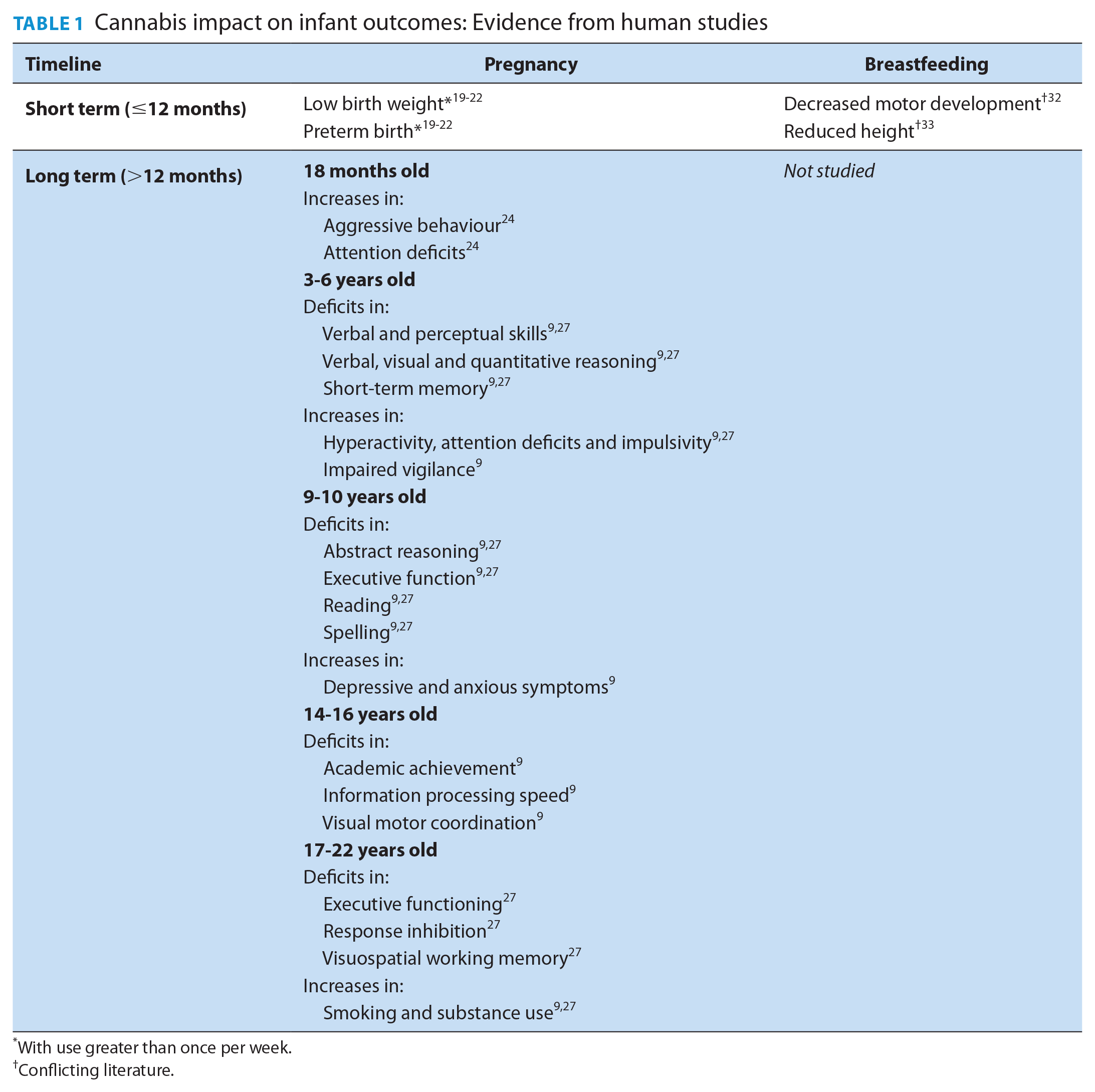
With use greater than once per week.
Conflicting literature.
Breastfeeding
The effects of marijuana exposure through breastmilk on children are less well studied. In fact, the majority of studies to date have focused primarily on quantifying the amount of cannabinoids found in breastmilk following exposure and not long-term health outcomes of infants who have been exposed. The lipophilicity of cannabinoids and their distribution into the fat of breastmilk and fatty tissues, including the developing brain, make cannabis use a particular concern in breastfeeding.
One early pharmacokinetic study measured the amount of THC in the breastmilk of 2 women who were smoking marijuana. They found that the infants received approximately 0.8% of the maternal dose of marijuana, but in the heavy user (smoked in pipe 7 times per day), the milk to plasma ratio was 8:1. 4 This makes THC stand out when compared to most other drugs that transfer into human breastmilk, as these typically have a milk to plasma ratio of 1 or less, meaning the drugs are excreted into breastmilk but do not concentrate there. 28 It is evident that depending on the chronicity of the mother’s cannabis use, breastmilk can have up to 8 times the THC concentration of the mother’s plasma. The concentration of THC in breastmilk is variable, but a mean of 2.5% (range 0.4% to 8.7%) of the maternal dose has been reported with cannabinoids (THC and its active metabolite, 11-OH-THC, and CBD) detectable in breastmilk as early as 1 to 4 hours after use and for up to 6 days after use through various routes of administration, including inhaled, ingested and topical.3,29
The controversy surrounding cannabis use during lactation stems from 4 main concerns:
Concerns also exist in situations where the infant is not exposed to THC through breastmilk, but 1 or both parents consume cannabis products while caring for the child. Second-hand smoke is harmful for children and can result in illness. Being under the influence of THC while parenting can cause parents to miss hunger cues, not pay sufficient attention to their child’s development and be unable to keep their children safe. The effects of cannabis products can last for several hours, potentially impairing a parent’s ability to adapt quickly to changing situations. 5 This is particularly important given the prevalent perception that marijuana has no impact on physical mobility or alertness. 6
Future research
Studies assessing prenatal exposure, birth outcomes and infant development were likely too small to find associations with rare outcomes, did not quantify marijuana use or used self-reporting when determining quantity used. When women who use marijuana during pregnancy also use other substances such as alcohol and nicotine, the effects of these agents can be difficult to distinguish. 37 In addition, the potency of THC in marijuana today is much greater than it was in the 1980s and 1990s when much of the data on this topic were published. 38
Further research is required in several areas, including the pharmacokinetics of THC and other components of marijuana in breastmilk and in breastfeeding infants, the effects of varying THC/CBD doses on outcomes in pregnancy and breastfeeding and the effect of the timing of exposure and chronicity of parental cannabis use on the type and severity of potential deficits in child development. The recent legalization of cannabis products for recreational use in Canada may encourage and allow for the research required to answer these important questions.
Pharmacists’ role and practice implications
The role of the pharmacist is to screen and educate with the aim of harm reduction, that is, reducing the negative consequences associated with drug use. 39 Public perception of the safety of marijuana is evolving, and with the ongoing normalization of the use of cannabis products, more pregnant and breastfeeding women may engage in recreational use of marijuana.
Pregnant or breastfeeding women, or women who are seeking to become pregnant, should be asked about substance use as part of their regular care and counselled on the potential risks to their baby from exposure to THC or CBD in utero or through breastmilk. A practice tool (Appendix 1, available online at www.cpjournal.ca) highlights the considerations for the use of cannabis products in pregnant or breastfeeding women. Pharmacists should work with patients to assess their comprehension of this information and to make recommendations or referrals regarding harm reduction. ■
Supplemental Material
893395_App_1_online_supp – Supplemental material for Cannabis use in pregnancy and breastfeeding: The pharmacist’s role
Supplemental material, 893395_App_1_online_supp for Cannabis use in pregnancy and breastfeeding: The pharmacist’s role by Erin Davis, Tiffany Lee, John T. Weber and Shawn Bugden in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Author Contributions:
SB initiated the project. ED wrote the manuscript drafts. All authors (ED, TL, JTW, SB) contributed to research, developed the project concept and manuscript and reviewed the final draft.
Financial Acknowledgements:
None.
Conflict of Interest:
None of the authors have any conflicts to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.