
Abstract
Background:
Community pharmacists have direct access to prescription refill information and regularly interact with their patients. Therefore, they are in a unique position to promote optimal medication use.
Objectives:
To describe how community pharmacists in Quebec, Canada, identify nonadherent patients, monitor medication use and promote optimal medication adherence.
Methods:
An invitation to complete a web-based survey was published online through different platforms, including a Facebook pharmacists’ group, an electronic newsletter, a pharmacy network forum and e-mail. The survey included questions on participant characteristics, methods used by pharmacists to identify nonadherent patients and monitor medication use and interventions they used to promote medication adherence.
Results:
In total, 342 community pharmacists completed the survey. The participants were mainly women (71.6%), staff pharmacists (56.7%) and aged 30 to 39 years (34.2%). The most common method to identify nonadherent patients was to check gaps between prescription refills (98.8%). The most common intervention to promote adherence was patient counselling (82.5%). The most common barriers to identifying nonadherent patients were lack of time (73.1%) and lack of prescription information (65.8%), whereas the most common barriers to intervening were anticipation of a negative reaction from their patients (91.2%) and lack of time (64%).
Conclusion:
Lack of time and lack of prescription information are frequent challenges encountered by community pharmacists regarding effective monitoring and management of patients with poor medication adherence. Pharmacists could benefit from electronic tools based on prescription refills that would provide quick and easily interpretable information on their patients’ medication adherence. Can Pharm J (Ott) 2020;153:xx-xx.
Knowledge Into Practice
Community pharmacists have direct access to information about prescription refills and frequently interact with patients and are thus in a unique position to promote optimal medication adherence.
Community pharmacists mainly identify nonadherent patients by checking the gaps between prescription refills and try to improve medication adherence by engaging in patient counselling.
The most common barriers to monitoring and managing nonadherent patients are lack of time, lack of prescription information and anticipation of negative reactions from their patients.
Further research is needed to investigate the development of an electronic tool in collaboration with community pharmacists that facilitates monitoring and managing their patients’ medication adherence.
Mise En Pratique Des Connaissances
Comme les pharmaciens communautaires ont un accès direct aux renseignements sur les renouvellements des prescriptions et qu’ils interagissent fréquemment avec les patients, ils sont les mieux placés pour promouvoir de manière optimale l’observance thérapeutique.
Les pharmaciens communautaires décèlent les cas de non-observance principalement en vérifiant les écarts entre les renouvellements des prescriptions et ils tentent d’améliorer l’observance thérapeutique en offrant des conseils à leurs patients.
Les obstacles les plus courants à la surveillance et à la prise en charge des cas de non-observance sont le manque de temps, le manque de renseignements sur les prescriptions et la crainte de réactions négatives de la part des patients.
Des recherches supplémentaires sont requises pour examiner le développement, en collaboration avec les pharmaciens communautaires, d’un outil électronique permettant de faciliter la surveillance et la prise en charge des cas de non-observance.
Introduction
Nonadherence to prescribed medications poses a significant barrier to the effectiveness of treatments for chronic diseases worldwide. Several studies have shown that patients being treated for chronic conditions adhere to their medications 50% of the time.1-3 Low adherence can result in inadequate disease control, reduced quality of life and increased utilization and cost of health care services.4-6 Accordingly, it is essential to improve the adherence of patients to their chronic therapeutic regimen.
Health care providers can positively influence their patients’ adherence by promoting optimal medication use. 7 Community pharmacists have direct access to information on prescription refills and frequently interact with their patients; therefore, they are among the best-positioned health care professionals to enhance their patients’ medication adherence.7,8
It is necessary that community pharmacists possess adequate tools and skills to easily and efficiently identify nonadherent patients, allowing them to intervene in a timely manner and encourage optimal medication use. 9 Several studies conducted in North America and Europe have reported that once community pharmacists have identified nonadherent patients from the pharmacy records of prescription refills, most will first intervene by discussing the issue with their patients.9-15 However, they face numerous challenges, including the lack of close monitoring, lack of accurate measures of patient adherence, the very busy pharmacy environment and limited patient interest.9,10,13,16-18 A study by Rickles et al. 9 showed that community pharmacists face difficulties with identifying, monitoring and intervening in cases of suspected nonadherence. Their results indicate a need for enhanced infrastructure (e.g., tools and staff) to facilitate regular monitoring of medication adherence and to promote interventions aimed at improving adherence.
To the best of our knowledge, no studies have described the practices of community pharmacists in Quebec, Canada, in terms of assessing and managing their patients’ medication adherence as a primary outcome. Thorough understanding of the current practices, including the barriers and challenges faced by pharmacists when assessing medication adherence, could help identify the unmet needs in clinical practice. Therefore, this study was designed to investigate how community pharmacists in Quebec identify nonadherent patients, monitor medication adherence and intervene to promote medication adherence.
Methods
Study design and setting
We conducted a cross-sectional study using an anonymous web-based survey addressed to community pharmacists in Quebec, Canada. The survey was created using Questback EFS Survey Software version 10.9. Invitations were sent using the following platforms: 1) La Dépêche, the electronic newsletter of the Quebec Order of Pharmacists (QOP) that reaches about 8000 pharmacists every month; 2) a Quebec practice-based research network of pharmacists (Réseau STAT) with 1150 members 19 ; and 3) a closed Facebook pharmacist group called Pharmaciens et pharmaciennes du Québec, which reaches around 5800 pharmacists. E-mails were also sent to about 2000 pharmacists acting as preceptors for the faculties of pharmacy in Quebec: Université de Montréal and Université Laval. The responses were collected in September and October 2017. This project was approved and the participants’ rights were protected by the ethical research review committees of Université de Montréal and Université Laval.
Participants and inclusion criteria
The target study population consisted of all community pharmacists practising in Quebec, estimated at approximately 6840. 20 The eligibility criteria to participate in the study were 1) being a member of the QOP; 2) having a license to practise in Quebec; 3) practising in a community pharmacy; and 4) having good French language skills because the survey was only available in French.
Survey questions
The web-based survey included 22 questions divided into 2 main sections: 1) the participants’ characteristics and 2) the pharmacists’ practices for assessing and managing medication nonadherence. The second section covered 2 topics: 1) monitoring of medication use, including the identification of nonadherent patients, and 2) interventions aimed at improving medication adherence.
In the first section, the participants were asked about their sociodemographic characteristics (sex and age group), number of years of practice in a community pharmacy, the year they obtained their licence to practise pharmacy in Quebec, current position (staff, substitute or owner) and whether they obtained accredited continuing education on medication adherence. Furthermore, they were asked about their region of pharmacy practice, the number of community pharmacies in which they currently work, the number of hours worked per week in a community pharmacy and average number of prescriptions filled per day. They were also asked to report the total number of hours of work by all pharmacists, per day, in their main pharmacy. This variable was used to estimate the workload for each working pharmacist in the pharmacy as the number of prescriptions filled per hour per pharmacist.
The second section of the survey started with a question on the importance the pharmacist gives to the measure of medication adherence on a scale of 1 to 10, where 1 = no importance given and 10 = high importance given. The following questions focused on the methods the pharmacists used to identify nonadherent patients, the average proportion of patients for whom they assess medication adherence and the barriers they encountered to identify nonadherent patients. The remainder of the survey comprised questions related to the interventions the pharmacists used to address medication nonadherence, the proportion of nonadherent patients for whom they generally intervene and the barriers encountered when intervening with nonadherent patients. The final question was related to the usefulness of a new electronic tool directly integrated in patients’ pharmacy records to effectively measure medication adherence on a scale of 1 to 10, where 1 = not useful and 10 = very useful.
Most of the questions were closed multiple-set answers or short-answer questions. For the closed questions, an “other” option was included to allow pharmacists to enter free-text answers if their preferred answer was not listed. The survey was pretested by 5 community pharmacists for content validity and to report any problems they experienced while completing the survey. We performed cognitive interviews with another 5 community pharmacists in which they were asked individually, in the presence of an interviewer, to respond to the survey by thinking out loud and to tell the interviewer what they thought about the questions as they completed the survey. 21 The aim of the cognitive interviews was to evaluate whether the pharmacists were correctly interpreting and understanding the questions. 21 The web-based survey was available in French because it is the most commonly used language in Quebec (used by 77.1% of the population). 22
Statistical analysis
The responses to the survey questions were extracted and coded in SPSS Statistics version 24 (SPSS, Inc., an IBM Company, Chicago, IL). Descriptive analyses were performed for each question by calculating the proportions, means and standard deviations as appropriate. Stratified analyses were performed to examine the association between pharmacist practices related to the identification of nonadherent patients and interventions to improve medication adherence, using the following pharmacist characteristics: the platform through which the pharmacist received the invitation to participate in the study, sex, age, number of years’ experience, current position (staff, substitute or owner), number of pharmacies in which the pharmacist works, number of hours worked per week, region of practice and daily pharmacist workload. The 3 most common answers were retained for the stratified analyses, specifically for the questions on methods used to identify nonadherent patients, interventions used for nonadherent patients and barriers to identifying and intervening in nonadherent patients. We used t tests or analysis of variance for continuous variables and χ2 tests for categorical variables. A p-value of <0.05 was set a priori as significant.
Results
Participant characteristics
A total of 342 community pharmacists completed the survey. A further 58 started but did not complete the survey and were thus excluded from the analyses. As presented in Table 1, most of the pharmacists received the invitation through e-mails sent to the Université de Montréal and Université Laval (59.6%). The participants were mainly women (71.6%), staff pharmacists (56.7%), aged 30 to 39 years (34.2%), had <10 years’ experience in community pharmacies (42.4%) and worked in pharmacies located in urban areas (65.2%).
Characteristics of the community pharmacists (n = 342)
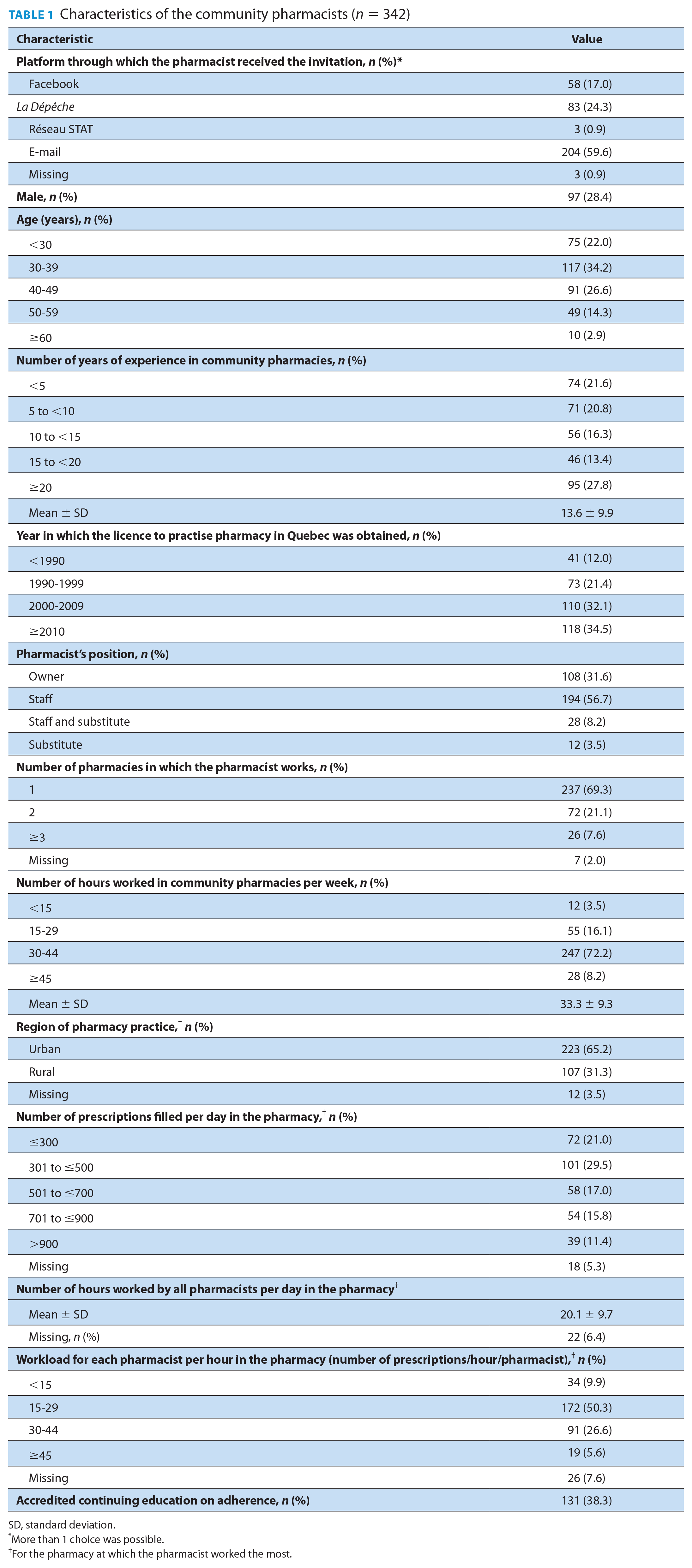
SD, standard deviation.
More than 1 choice was possible.
For the pharmacy at which the pharmacist worked the most.
Practices related to medication adherence
Pharmacists gave an average score of 9 of 10 for the importance they place on assessing medication adherence in their practice (Table 2). They reported assessing medication adherence for 75.7% of their patients during their pharmacy visits. The most common methods used to identify nonadherent patients included checking gaps between prescription refills (98.8%), identifying prescriptions that were never filled (75.7%) and directly discussing medication use with patients (67%). In this study, unfilled prescriptions included written prescriptions brought by the patient to the pharmacy or prescriptions sent to the pharmacy electronically (i.e., via fax or electronic medical records) that were never filled by the patient. Pharmacists reported that barriers to identifying nonadherent patients included lack of time (73.1%), lack of information on the medication prescriptions (e.g., prescriptions that were never brought to pharmacy or medication discontinuation) (65.8%) and anticipation of a negative reaction from the patient (46.2%).
Community pharmacists’ practices related to identifying and managing medication adherence (n = 342)
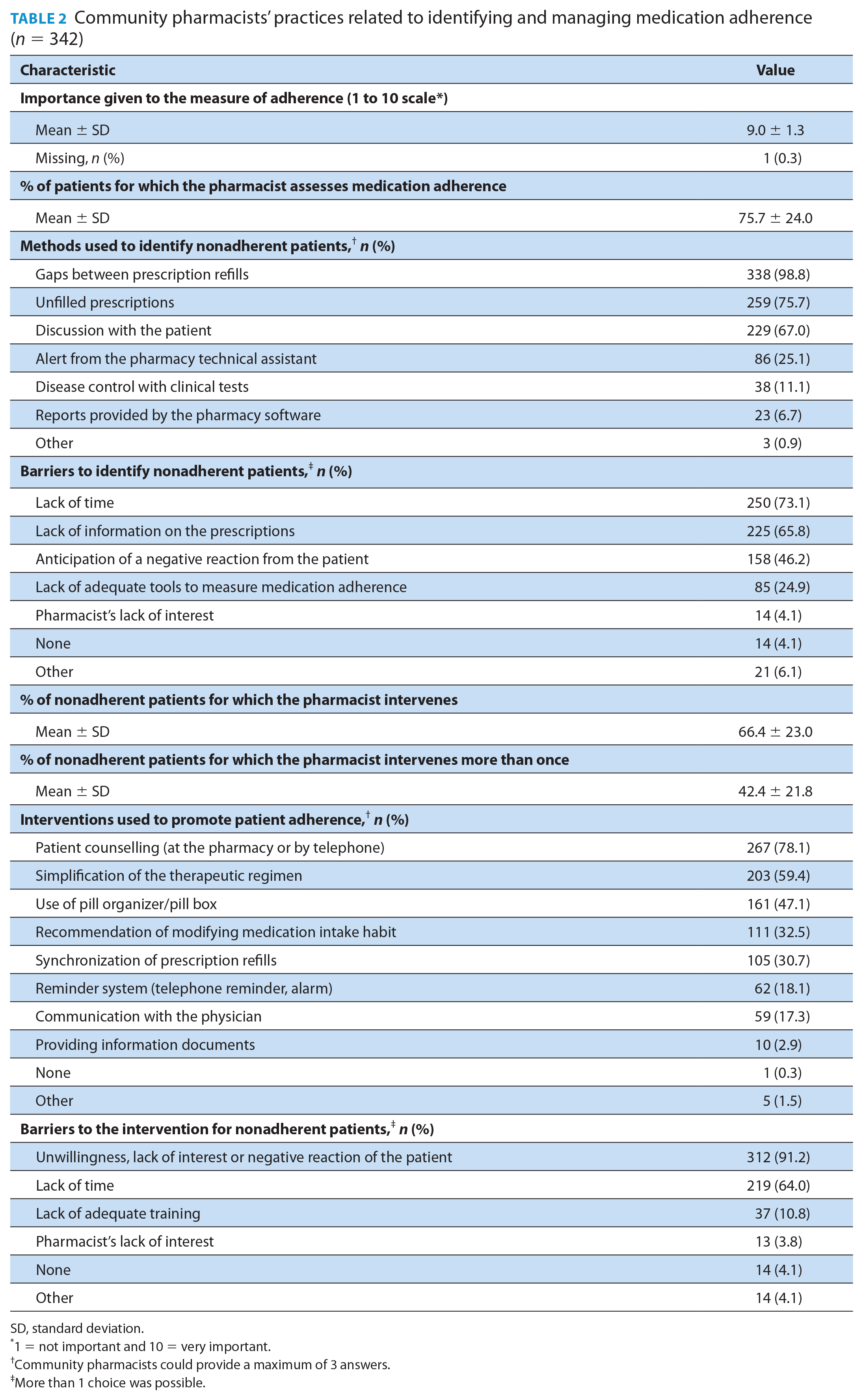
SD, standard deviation.
1 = not important and 10 = very important.
Community pharmacists could provide a maximum of 3 answers.
More than 1 choice was possible.
Pharmacists reported that they intervened in order to improve medication adherence for 66.4% of nonadherent patients on average. The interventions most frequently used included patient counselling (78.1%), simplification of the therapeutic regimen (59.4%) and suggesting the use of a pill organizer or pill box (47.1%). The barriers to interventions included negative patient attitudes (91.2%), lack of time (64%) and lack of adequate training (10.8%). Pharmacists responded favourably regarding the usefulness of a new electronic tool to measure medication adherence (mean of 6.8 out of 10; data not shown).
Stratified analyses
Several pharmacist characteristics were significantly associated with the identification of nonadherent patients (Table 3) or interventions to improve medication adherence (Table 4). The complete stratified analyses are provided in Appendices 1 and 2 (available at www.cpjournal.ca).
Community pharmacists’ characteristics associated with identification of nonadherent patients
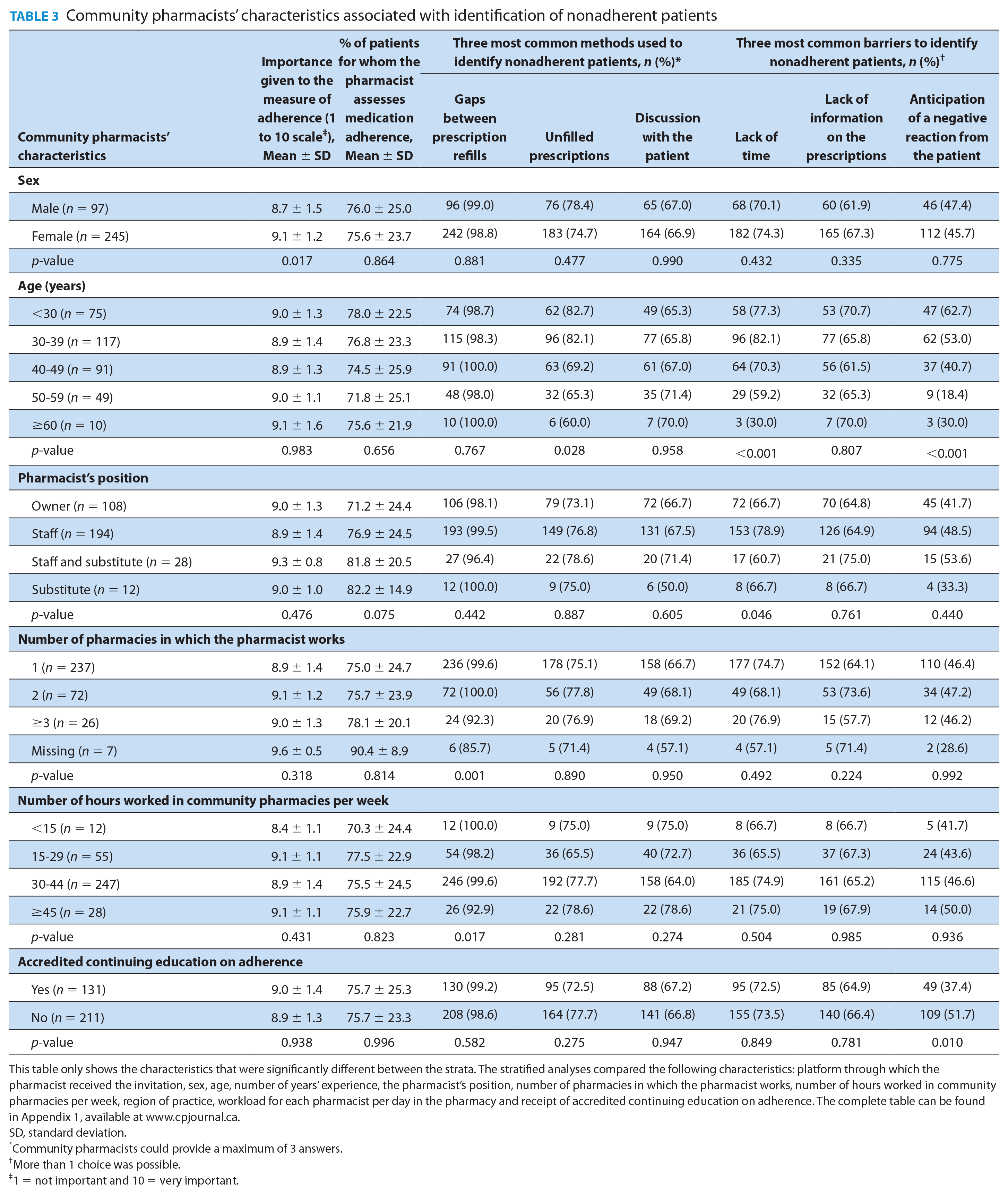
This table only shows the characteristics that were significantly different between the strata. The stratified analyses compared the following characteristics: platform through which the pharmacist received the invitation, sex, age, number of years’ experience, the pharmacist’s position, number of pharmacies in which the pharmacist works, number of hours worked in community pharmacies per week, region of practice, workload for each pharmacist per day in the pharmacy and receipt of accredited continuing education on adherence. The complete table can be found in Appendix 1, available at www.cpjournal.ca.
SD, standard deviation.
Community pharmacists could provide a maximum of 3 answers.
More than 1 choice was possible.
1 = not important and 10 = very important.
Community pharmacists’ characteristics associated with interventions aimed at increasing medication adherence
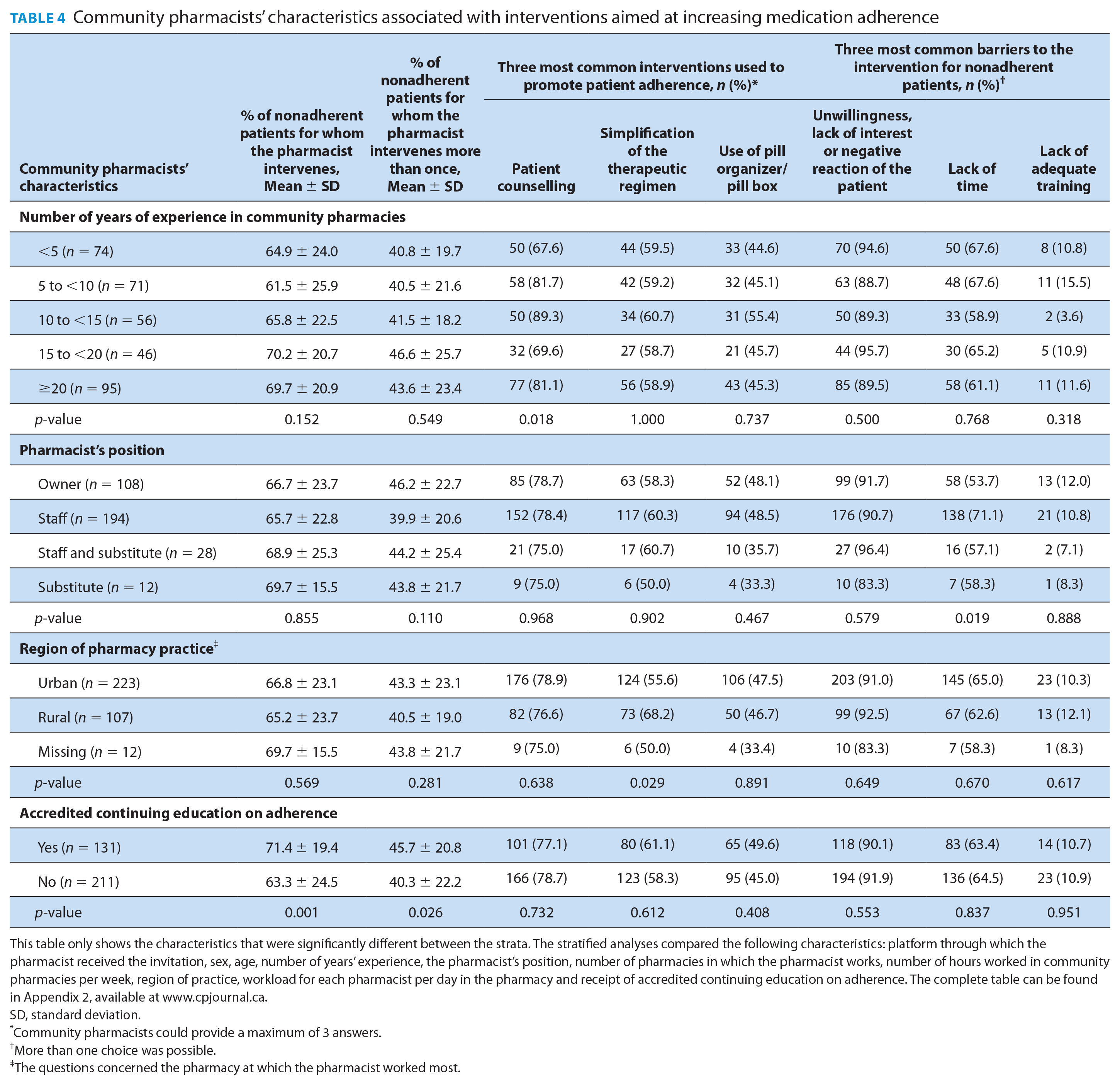
This table only shows the characteristics that were significantly different between the strata. The stratified analyses compared the following characteristics: platform through which the pharmacist received the invitation, sex, age, number of years’ experience, the pharmacist’s position, number of pharmacies in which the pharmacist works, number of hours worked in community pharmacies per week, region of practice, workload for each pharmacist per day in the pharmacy and receipt of accredited continuing education on adherence. The complete table can be found in Appendix 2, available at www.cpjournal.ca.
SD, standard deviation.
Community pharmacists could provide a maximum of 3 answers.
More than one choice was possible.
The questions concerned the pharmacy at which the pharmacist worked most.
Table 3 shows that, compared with men, women gave greater importance to the assessment of adherence in their clinical practice (9.1 ± 1.2 vs 8.7 ± 1.5, p = 0.017). We also found that a smaller proportion of pharmacists reported that they checked gaps between prescription refills when they worked in 3 or more community pharmacies and worked >45 hours per week (p = 0.001 and p = 0.017, respectively). We also found that a smaller proportion of younger community pharmacists reported that they checked unfilled prescriptions (p = 0.028). There was a large difference of approximately 22% between the youngest (<30 years) and the oldest (≥60 years) age groups. Additionally, younger pharmacists (p ≤ 0.001) and staff pharmacists (p = 0.046) were more likely to perceive the lack of time as a barrier. We also observed that younger pharmacists were more likely to anticipate a negative reaction from the patient compared with older pharmacists (p ≤ 0.001), with 62.7% of those aged <30 years reporting this barrier compared with 18.4% aged 50 to <60 and 30% aged ≥60 years. Similarly, those who did not receive any continuing education on medication adherence were more likely to perceive the same barrier than those who did (p = 0.010), with a difference of almost 15% between these 2 groups.
As presented in Table 4, pharmacists who received accredited continuing education on medication adherence were more likely to intervene to increase medication adherence as compared with those who did not (p = 0.001). Those with 10 to 15 years’ experience in community pharmacies were more likely to report patient counselling as an intervention (p = 0.018) than pharmacists with less or more experience. Finally, a higher proportion of staff pharmacists (71.1%) reported that lack of time was a barrier to them intervening to improve their patients’ medication adherence as compared with owner pharmacists (53.7%; p = 0.019).
Discussion
This study explored the practices of community pharmacists for assessing and managing medication nonadherence, as well as the characteristics associated with these outcomes. Pharmacists who participated in our survey reported that they assess medication adherence for 76% of their patients and intervened to improve nonadherence for 66% of their nonadherent patients.
Our findings contrast with the naturalistic observational study conducted in the United States by Rickles et al. 9 in 2016, in which 26% to 30% of patients reported that their pharmacist intervened by asking why they had not collected their medications, after they deliberately switched between 2 pharmacies, creating artificial gaps between prescription refills. Differences in perceptions between pharmacists (as in our study) and patients (as in Rickles et al. 9 ) might explain the disparity in results. Rickles et al. 9 also found that 61% to 73% of patients reported that their pharmacist provided solutions only after mentioning skipping doses. Although this finding is similar to what the community pharmacists in our study reported, the patients in that study had to be proactive for their pharmacist to intervene. This might indicate that, overall, the pharmacists in our study tended to intervene more often or they possibly overestimated the proportion of nonadherent patients for whom they intervene.
In our study, 99% of the pharmacists responded that they mainly identify nonadherent patients by checking gaps between prescription refills in their patients’ records. This concurs with another study conducted in the United States in which the number of days that patients who failed to refill their prescriptions were late was the only information in the pharmacy’s computer system that helped pharmacists to adequately monitor medication adherence in daily practice. 23 In addition to this method, the pharmacists in our study reported that they reviewed unfilled prescriptions and discussed medication use with their patients. However, reviewing unfilled prescriptions in patient records was less favoured by older pharmacists. Some studies have reported that older adults are less comfortable with information technologies,24,25 and this might explain why those aged >50 years favour discussing medication adherence with patients more than checking unfilled prescriptions in pharmacy records. Older pharmacists might also be more skilled at engaging in discussions with patients, considering their many years of experience. In fact, a smaller proportion of older pharmacists reported that they anticipated negative reactions from their patients as compared with those younger.
Our study also suggests that the most common interventions used by pharmacists to improve adherence included patient counselling (at the pharmacy or by telephone), simplification of the therapeutic regimen and suggesting the use of a pill organizer or pill box. Pharmacists with <5 years’ experience in a community pharmacy less frequently reported that they engaged in discussions with their patients as compared with those with more experience. Patient counselling, simplification of the therapeutic regimen and the use of pill organizers are often used in community pharmacies and were shown to improve adherence in several studies.26-31
Lack of time, lack of prescription information and anticipation of a negative reaction from patients were common barriers to monitoring and managing nonadherent patients. The barriers identified in our study are similar to those found in previous studies.13,16-18,23,32-35 However, we found that younger pharmacists were more likely to report lack of time and anticipation of a negative reaction from patients as barriers than were older ones, which may be due to their lack of experience, while staff pharmacists were more likely to report lack of time as a barrier as compared with owners.
Our study also showed that pharmacists who received accredited continuing education on adherence were less likely to report that they anticipated a negative reaction from their patients when assessing medication adherence. They also reported more frequent use of proactive interventions aimed at addressing nonadherence issues. In light of these results, we hypothesize that accredited continuing education on adherence has a positive impact on the initiation of discussions with nonadherent patients and greater pharmacist skill with performing interventions aimed at improving adherence.
Our findings should be considered in light of some limitations. Because study participation was voluntary, the survey might have attracted pharmacists who may have a greater interest in the monitoring and management of medication adherence in daily practice. We also hypothesize that these pharmacists were more proactive in supporting patient medication adherence compared with the general population. In addition, they might have subconsciously altered survey responses towards a more positive view of their practice. Thus, our findings may overestimate the degree to which community pharmacists identify nonadherent patients or their involvement in interventions aimed at promoting adherence in clinical practice. As described above, pharmacists reported a surprisingly high proportion of patients for whom they assess medication adherence and intervene (76% and 66%, respectively) compared with Rickles et al. 9 Furthermore, because we recruited participants through different online platforms, such as Facebook and an electronic newsletter, it may have been more difficult to reach older pharmacists who may spend less time on the Internet compared with their younger colleagues. 25 In addition, the survey respondents represented only 5% of community pharmacists in Quebec, and because of this low proportion, we might have missed some associations between pharmacist characteristics and their monitoring and management of medication adherence. Nevertheless, we reached community pharmacists across the province and therefore collated the perspectives of pharmacists from several regions of Quebec.
In conclusion, we observed that, in daily practice, community pharmacists identify patients who do not adhere to medications for chronic conditions mainly by checking the gaps between prescription refills. Pharmacists reported that they generally engage in patient counselling in order to improve medication adherence. They also reported many barriers to monitoring and managing nonadherent patients, including lack of time, lack of prescription information and anticipation of a negative reaction from the patient. These findings suggest that improvements are needed to facilitate the timely identification of patients with adherence issues, improve the exchange of relevant information between prescribers and pharmacists and improve pharmacists’ communication and behaviour change technique skills regarding medication adherence. For example, a tool embedded in the patient’s pharmacy record that provides quick and precise information on the patient’s level of adherence along with information on when treatments are stopped, as well as cues and prompts on ways to engage with discussions when nonadherence is detected, could support community pharmacists in their responsibilities to promote optimal medication use. ■
Supplemental Material
902494_Blais_Appendix_1 – Supplemental material for Monitoring and managing medication adherence in community pharmacies in Quebec, Canada
Supplemental material, 902494_Blais_Appendix_1 for Monitoring and managing medication adherence in community pharmacies in Quebec, Canada by Rébecca Fénélon-Dimanche, Line Guénette, Alia Yousif, Geneviève Lalonde, Marie-France Beauchesne, Johanne Collin and Lucie Blais in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Supplemental Material
902494_Blais_Appendix_2 – Supplemental material for Monitoring and managing medication adherence in community pharmacies in Quebec, Canada
Supplemental material, 902494_Blais_Appendix_2 for Monitoring and managing medication adherence in community pharmacies in Quebec, Canada by Rébecca Fénélon-Dimanche, Line Guénette, Alia Yousif, Geneviève Lalonde, Marie-France Beauchesne, Johanne Collin and Lucie Blais in Canadian Pharmacists Journal / Revue des Pharmaciens du Canada
Footnotes
Funding:
This work was supported by the Cercle du Doyen of the Faculty of Pharmacy of Université de Montréal.
Author contributions:
This manuscript was conceived and designed by RFD, LG, GL, MFB, JC and LB and drafted by RFD, AY and LB. LG, MFB, JC and LB supervised the project and reviewed the final draft.
Conflict of interest statement:
The authors have no conflicts of interest to declare.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.