
Abstract
Background
Early prediction of wound healing after flap reconstruction for stage IV pressure injuries remains challenging. This study evaluated the neutrophil-to-lymphocyte ratio (NLR) and systemic immune-inflammation index (SII) as predictors of healing outcomes.
Methods
This retrospective cohort study included 127 patients with stage IV pressure injuries who underwent negative-pressure wound therapy and flap reconstruction between January 2020 and December 2024. Blood samples were collected at baseline, 72 hours, day 7, and day 14 post-surgery. The primary outcome was complete wound healing. Receiver operating characteristic curve analysis was used to assess the predictive performance of inflammatory indices.
Results
Complete healing was achieved in 72 patients (56.7%) over a median follow-up of 18 weeks. The delayed/non-healing group had higher baseline NLR (9.2 vs 6.0, P<0.001) and SII (2068.3 vs 1351.2, P<0.001). Day 7 NLR reduction was greater in the healing group (-22.9% vs -10.6%, P<0.001). Baseline SII had the highest predictive value among individual markers (area under the curve [AUC] 0.774). Day 7 NLR change achieved AUC 0.784. The combined model incorporating baseline NLR and day 7 NLR change yielded an AUC of 0.838, with 81.9% sensitivity and 70.9% specificity. Time-dependent analysis showed consistent performance across 30-day, 60-day, and 90-day time points (AUC 0.798-0.838).
Conclusions
Baseline SII and NLR, combined with early dynamic changes, may serve as potential predictors of healing after flap reconstruction for stage IV pressure injuries. Early assessment of NLR trajectory may provide adjunctive prognostic information, though prospective validation is required.
Keywords
Introduction
Stage IV pressure injuries (formerly termed pressure ulcers) represent severe tissue destruction that extends through the full thickness of the skin into underlying muscle, tendon, or bone.1,2 These wounds affect patients with prolonged immobility due to spinal cord injury, cerebrovascular disease, or critical illness. Despite advances in wound care technology, stage IV pressure injuries remain associated with substantial morbidity, prolonged hospitalization, and mortality rates exceeding 20% in some populations.3,4
Surgical reconstruction with flap coverage is required when conservative management fails to achieve wound closure. 5 The current standard approach combines negative pressure wound therapy to prepare the wound bed followed by definitive closure with local or regional flaps. 6 However, healing outcomes after flap reconstruction remain unpredictable. Reported failure rates range from 15% to 40%, depending on patient characteristics and defect complexity. 7 The inability to identify patients at high risk for delayed healing limits opportunities for early intervention and appropriate resource allocation.
Traditional risk factors for impaired wound healing include older age, diabetes, malnutrition, and larger wound size.8,9 While these factors identify at-risk populations, they provide limited information regarding individual healing trajectories. Measurement of these parameters typically occurs at a single time point and does not capture dynamic physiologic changes during the early postoperative period. More importantly, no established biomarkers exist to predict healing outcomes after flap reconstruction for pressure injuries.
Systemic inflammatory markers have emerged as prognostic indicators in various surgical and critical care settings. The neutrophil-to-lymphocyte (NLR) ratio reflects the balance between innate inflammatory response and adaptive immunity. 10 Elevated NLR has been associated with poor outcomes after major surgery, sepsis, and cardiovascular events.11,12 The systemic immune-inflammation index (SII), which incorporates platelet count alongside neutrophil and lymphocyte counts, provides a more comprehensive assessment of immune-inflammatory status.13,14 Recent studies have demonstrated that SII predicts complications and mortality in cancer surgery and critical illness.15,16
However, the application of these inflammatory markers to pressure ulcer management has not been systematically evaluated. Furthermore, whether early changes in inflammatory indices during the initial postoperative period provide additional prognostic information beyond baseline values remains unknown. Given that wound healing is a dynamic process involving coordinated inflammatory, proliferative, and remodeling phases, 17 serial assessment of inflammatory markers may capture treatment response and predict ultimate healing success.
This study evaluated baseline NLR and SII, along with their early dynamic changes, as predictors of complete wound healing after flap reconstruction for stage IV pressure injuries. We hypothesized that both baseline inflammatory burden and the magnitude of early inflammatory resolution would predict healing outcomes. That combined assessment would provide superior discriminative ability compared with either parameter alone.
Methods
Study design and participants
This retrospective cohort study included patients with stage IV pressure injuries treated at the Affiliated Hospital of Xuzhou Medical University between January 2020 and December 2024. This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines. This study was conducted in accordance with the ethical principles of the Declaration of Helsinki (as revised in 2024). The institutional ethics committee approved the study protocol and waived the requirement for informed consent.
Patients aged 18 years or older with stage IV pressure injuries confirmed by physical examination were eligible. Patients were included if they underwent negative pressure wound therapy followed by flap reconstruction and had complete serial blood test data. Exclusion criteria were incomplete blood test data, active infection requiring antibiotics at admission, malignancy, immunosuppressive therapy, and incomplete medical records.
Of 156 patients screened, 127 met eligibility criteria. Reasons for exclusion were incomplete blood test data (n=18), active infection at admission (n=7), and malignancy or immunosuppressive therapy (n=4). All patient data were fully de-identified prior to analysis in accordance with institutional data protection standards.
Treatment protocol
Following admission, all patients underwent initial debridement and received negative-pressure wound therapy until sufficient granulation tissue was formed for definitive closure. Negative-pressure wound therapy (NPWT) was applied continuously at −125 mmHg without instillation, using commercially available foam dressings. Dressing changes were performed every 48 to 72 hours according to wound status. NPWT duration was determined by wound bed preparation and clinical assessment.
Flap reconstruction was performed using a gluteal fasciocutaneous flap (n=73), a gluteus maximus myocutaneous flap (n=42), or a perforator-based flap (n=12). Flap selection was based on defect characteristics and available tissue. Initial wound management included surgical debridement at admission, which contributed to the reduction of local bacterial burden and systemic inflammatory load during the NPWT preparation phase. Systemic antibiotic therapy was not administered prophylactically during this period unless clinical signs of infection were present. Perioperative antibiotic prophylaxis was administered at the time of flap reconstruction per institutional protocol and discontinued within 24 hours postoperatively.
Nutritional support included high-protein diet supplementation. Enteral nutrition was provided when indicated by nutritional assessment. All reconstructive procedures were performed by a single senior reconstructive surgery team. Flap selection was determined by wound location, defect dimensions, and available local tissue in accordance with institutional reconstructive guidelines. Postoperatively, all patients were managed with a standardized pressure-redistribution protocol, including low-air-loss mattresses, mandatory two-hourly repositioning, and restriction of sitting for a minimum of six weeks following flap reconstruction. Adherence to the repositioning protocol was documented in nursing shift records throughout hospitalization, although a formal standardized compliance measurement tool was not employed. All patients with clinical or radiological suspicion of osteomyelitis underwent bone debridement as part of the initial surgical preparation prior to flap reconstruction. Diagnosis was based on preoperative imaging (plain radiograph and/or MRI) combined with intraoperative findings. Adequacy of bone debridement to viable margins was confirmed before proceeding to definitive flap coverage.
Blood sample collection and laboratory analysis
Venous blood samples were collected at baseline (within 24 hours of admission and prior to any surgical intervention), and at 72 hours, day 7, and day 14 following flap reconstruction surgery. Samples were obtained after overnight fasting and analyzed by the central laboratory. Wound swab cultures were obtained from all patients at baseline as part of routine wound assessment. Blood cultures were obtained when clinical signs of systemic infection were present. Procalcitonin and interleukin-6 were not systematically collected, a limitation acknowledged.
Complete blood count was performed using an automated hematology analyzer. The neutrophil-to-lymphocyte ratio was calculated as the neutrophil count divided by the lymphocyte count. Platelet-to-lymphocyte ratio was calculated as platelet count divided by lymphocyte count. The systemic immune-inflammation index was calculated as (platelet count × neutrophil count)/lymphocyte count.
C-reactive protein was measured by immunoturbidimetric assay. Albumin and prealbumin were determined using the bromocresol green method and the immunoturbidimetric assay, respectively.
Percentage change in inflammatory indices was calculated as: [(value at time point - baseline value)/baseline value] × 100.
Outcome measurements
The primary outcome was complete wound healing, defined as full epithelialization without drainage or infection. Healing time was recorded as days from flap reconstruction to complete healing.
Secondary outcomes were postoperative complications and hospital length of stay. Complications included wound dehiscence (separation requiring intervention), surgical site infection (clinical signs with positive culture when obtained), hematoma or seroma (fluid collection requiring drainage), and partial flap necrosis (tissue loss on clinical examination).
Patients were followed weekly for the first month, then biweekly until healing or for a minimum of 12 weeks.
Statistical analysis
Continuous variables were expressed as median (interquartile range) and compared using the Mann-Whitney U test. Categorical variables were presented as n (%) and compared using the chi-square or Fisher’s exact test.
Receiver operating characteristic curve analysis was used to evaluate the predictive performance of inflammatory indices. Area under the curve with 95% confidence intervals was calculated. The Youden index was used to determine optimal cutoff values. Sensitivity and specificity at optimal cutoffs were reported.
Combined prediction models incorporating baseline values and early dynamic changes were constructed using logistic regression. Model performance was compared using area under the curve.
Time-dependent receiver operating characteristic analysis assessed model performance at 30-day, 60-day, and 90-day time points
Statistical analyses were performed using R software version 4.2.0 (R Foundation for Statistical Computing, Vienna, Austria). Two-sided P values less than 0.05 were considered statistically significant. A formal a priori sample size calculation was not performed, given the retrospective and exploratory nature of this study. This limitation is acknowledged and may affect the precision of the reported effect estimates.
Results
Patient enrollment and baseline characteristics
Between January 2020 and December 2024, 156 patients with stage IV pressure injuries were admitted to our institution. After applying inclusion and exclusion criteria, 127 patients with complete serial blood testing data were enrolled in the final analysis (Figure 1). Twenty-nine patients were excluded due to incomplete blood test data (n=18), active infection requiring antibiotics at admission (n=7), and malignancy or immunosuppressive therapy (n=4). Patient enrollment flowchart. (a) total of 156 patients with stage IV pressure injuries were screened. After exclusion of 29 patients (18 with incomplete blood data, 7 with active infection requiring antibiotics, 4 with malignancy or immunosuppressive therapy), 127 patients were included in the final analysis. Among them, 72 patients achieved complete wound healing and 55 patients experienced delayed or incomplete healing.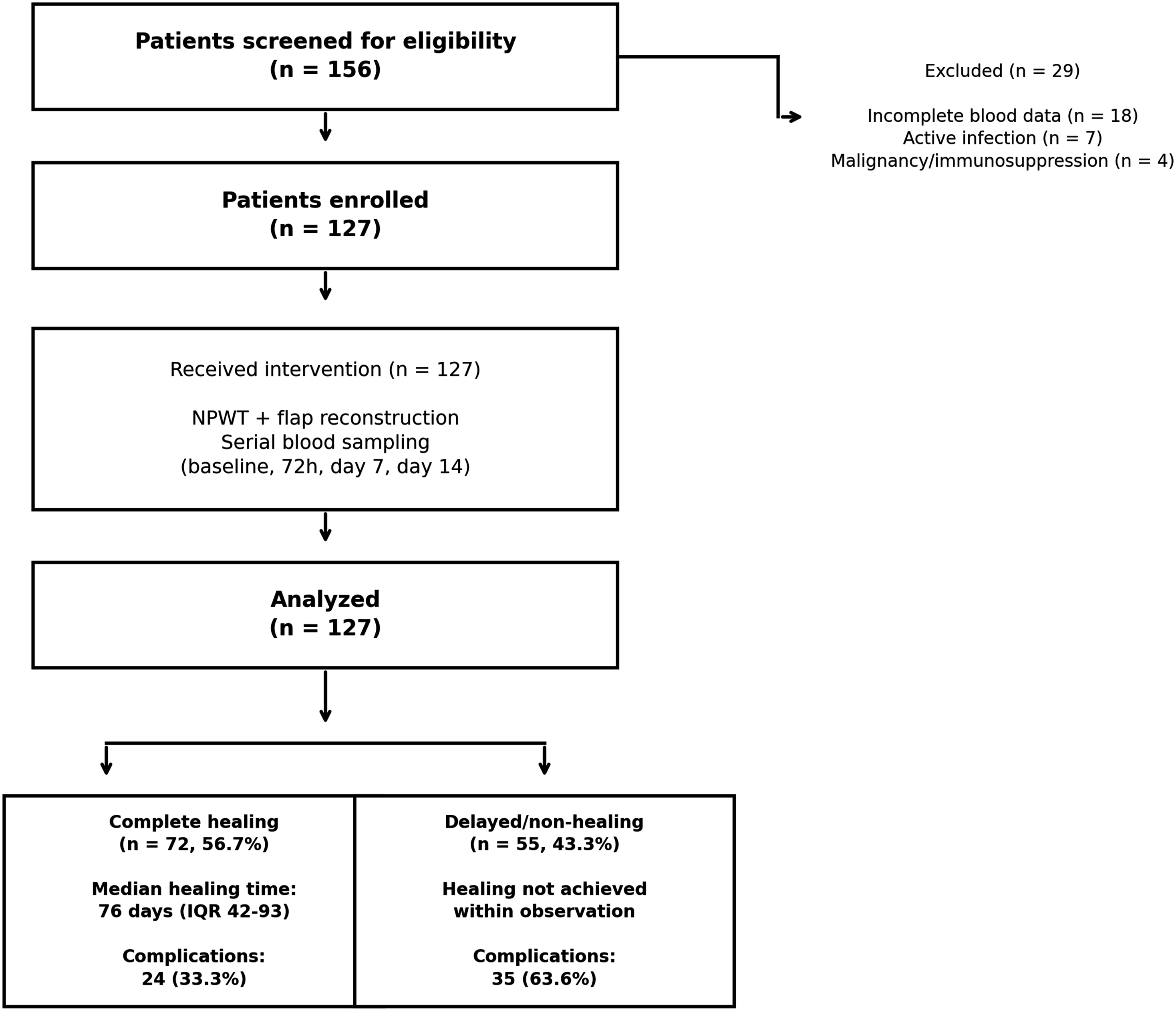
The median age of enrolled patients was 68 years (interquartile range [IQR]: 61-73 years), with 65 males (51.2%) and 62 females (48.8%). The median ulcer duration before admission was 39 days (IQR: 26-54 days). Sacral injuries were the most common location (n=93, 73.2%), followed by ischial (n=25, 19.7%) and trochanteric ulcers (n=9, 7.1%). The median initial wound area was 46.6 cm2 (IQR: 36.5-60.4 cm2). The median Braden score at admission was 10 (IQR: 9-12), indicating high risk for pressure ulcer progression.
Comorbidities were prevalent in this cohort. Diabetes mellitus was present in 65 patients (51.2%), hypertension in 68 patients (53.5%), cardiovascular disease in 41 patients (32.3%), and cerebrovascular disease in 39 patients (30.7%). Eighteen patients (14.2%) had chronic kidney disease. Thirty-seven patients (29.1%) had a history of smoking.
Baseline characteristics of study cohort.
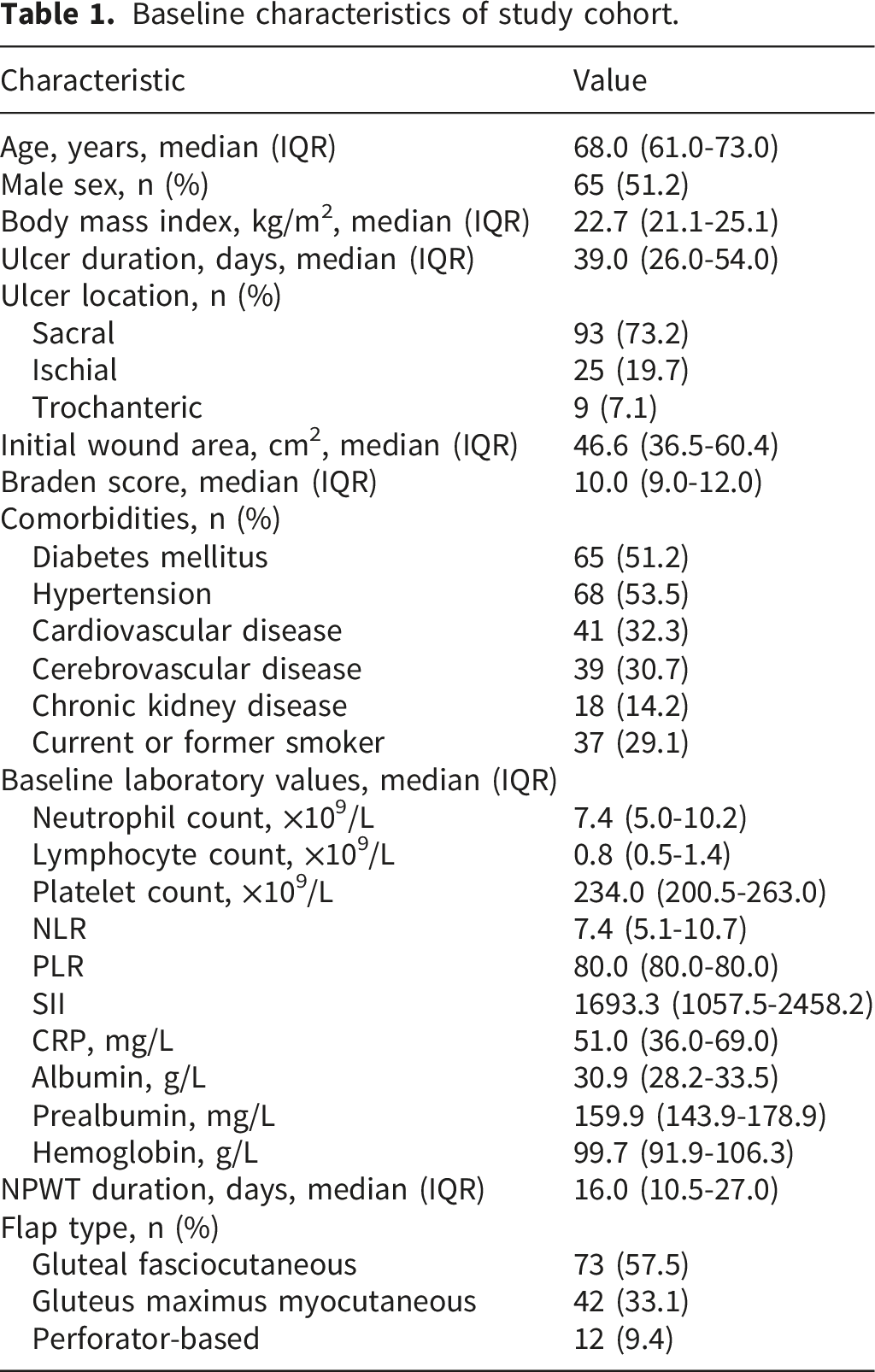
Baseline wound swab cultures were positive in 102 patients (80.3%). The most commonly isolated organisms were Staphylococcus aureus (n=45), Pseudomonas aeruginosa (n=28), and Proteus mirabilis (n=15). Polymicrobial growth was observed in 34 cases. Culture positivity rates were similar between the healing and delayed/non-healing groups (79.2% vs 81.8%, P=0.713).
Treatment outcomes and complications
Complete wound healing was achieved in 72 patients (56.7%) over a median follow-up of 18 weeks. The median time to healing was 76 days (IQR 42-93), with 9 patients (7.1% of total cohort, 12.5% of healing group) achieving healing within 30 days. Postoperative complications occurred in 59 patients (46.5%) and were significantly more frequent in the delayed/non-healing group than the healing group (63.6% vs 33.3%, P=0.001).
Treatment outcomes and complications.
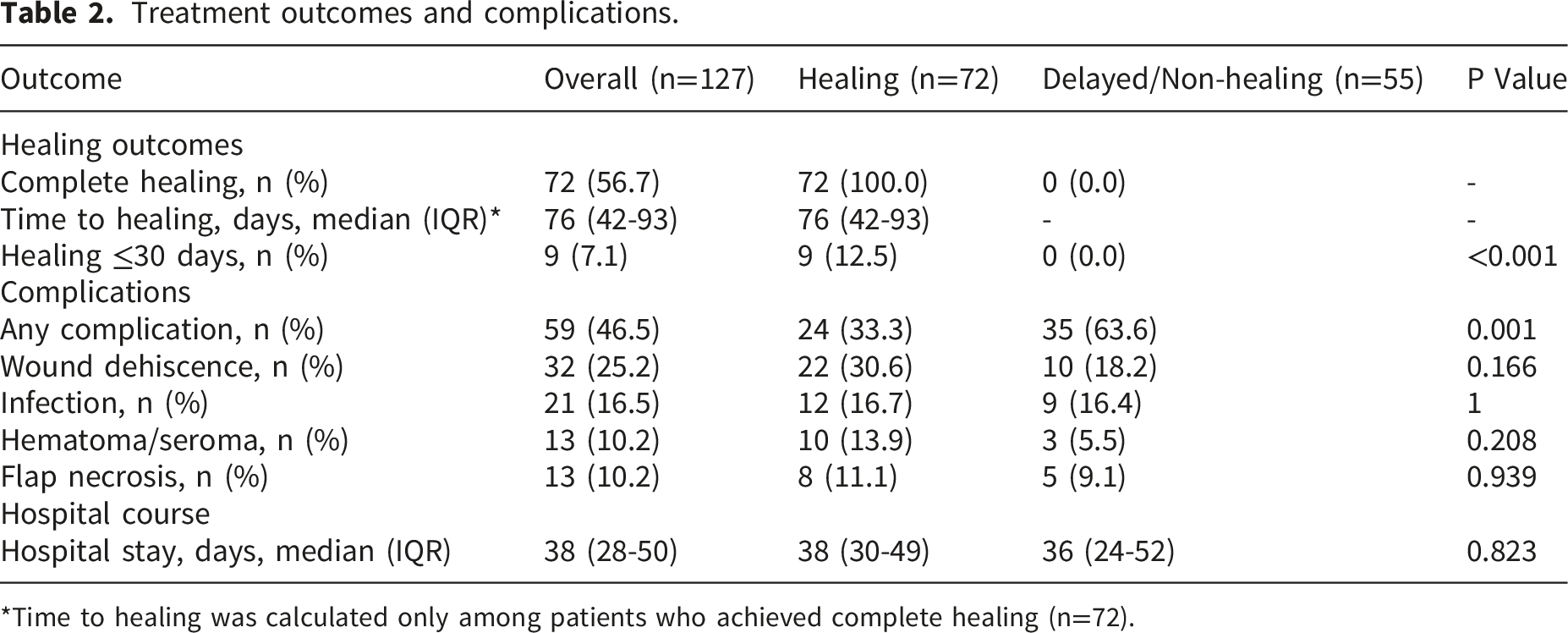
*Time to healing was calculated only among patients who achieved complete healing (n=72).
Comparison between healing and delayed/non-healing groups
Comparison of baseline characteristics between healing and delayed/non-healing groups.
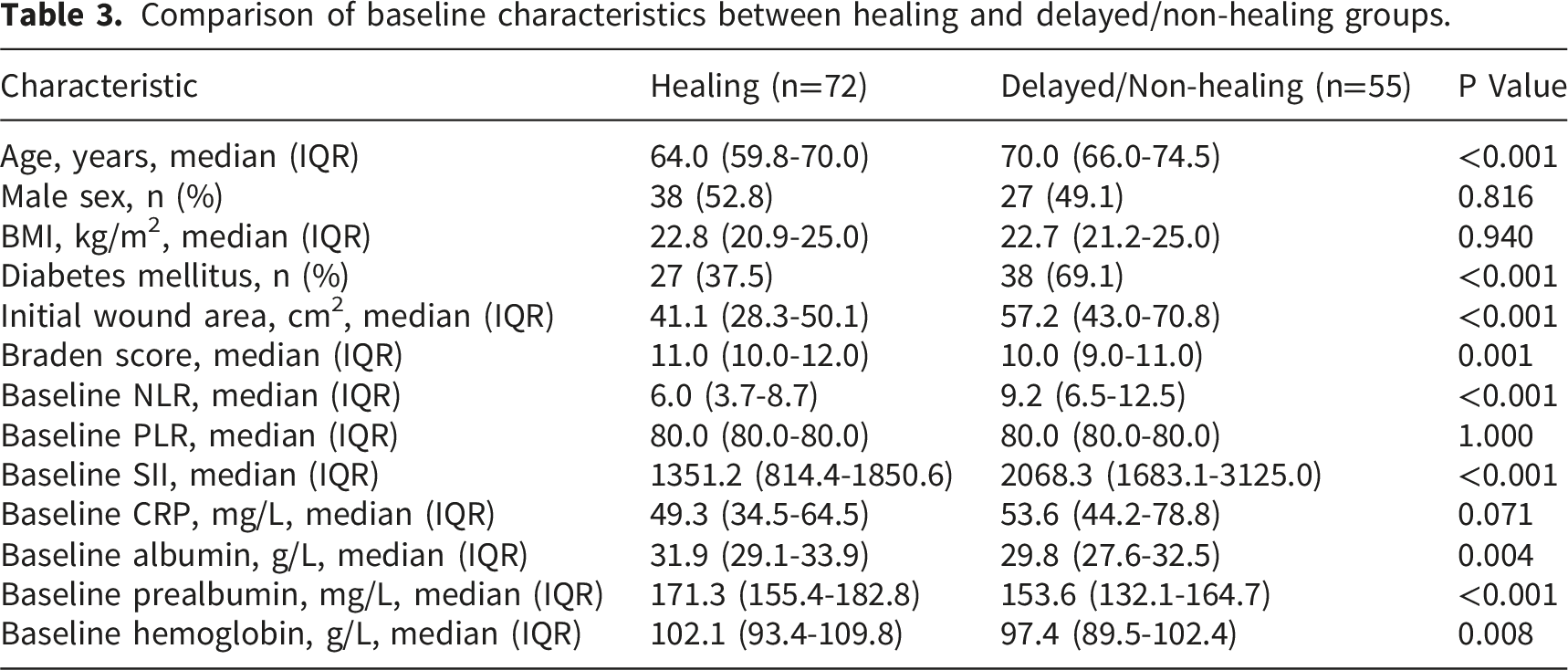
The delayed/non-healing group had higher baseline NLR (9.2 vs 6.0, P<0.001) and SII (2068.3 vs 1351.2, P<0.001). Baseline CRP did not differ significantly (53.6 vs 49.3 mg/L, P=0.071), nor did PLR (80.0 vs 80.0, P=1.000). Albumin (29.8 vs 31.9 g/L, P=0.004), prealbumin (153.6 vs 171.3 mg/L, P<0.001), and hemoglobin (97.4 vs 102.1 g/L, P=0.008) were lower in the delayed/non-healing group (Table 3). These findings indicate that patients with delayed healing had worse baseline inflammatory status, nutritional deficits, and greater disease severity.
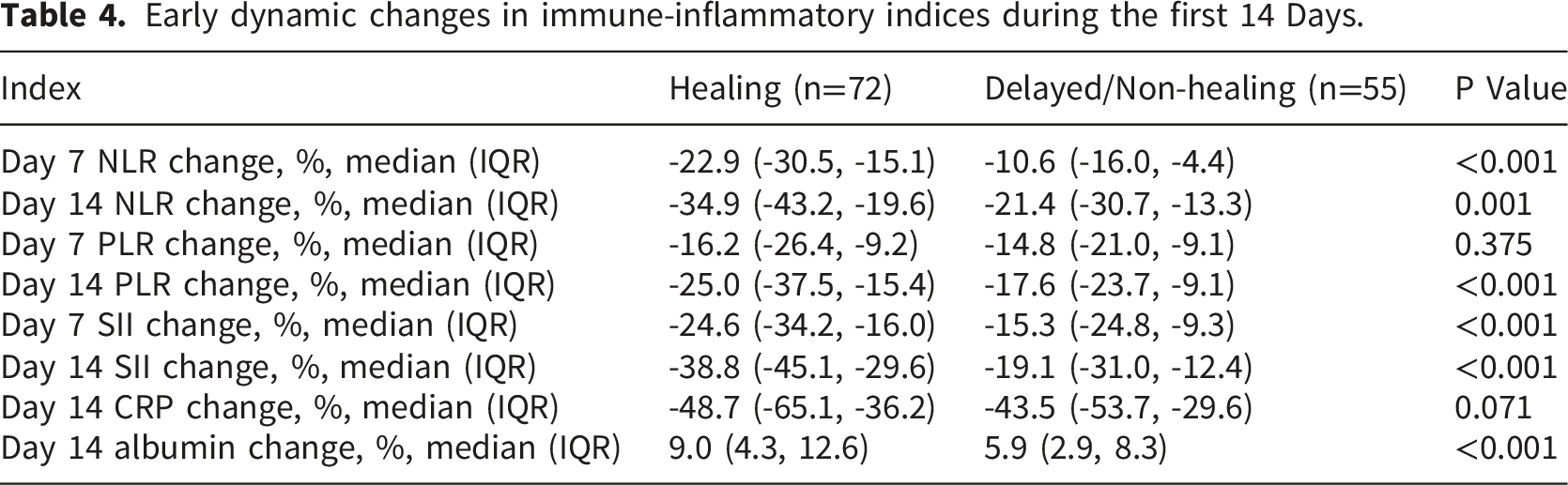
Early dynamic changes in immune-inflammatory indices
Early dynamic changes in immune-inflammatory indices during the first 14 Days.
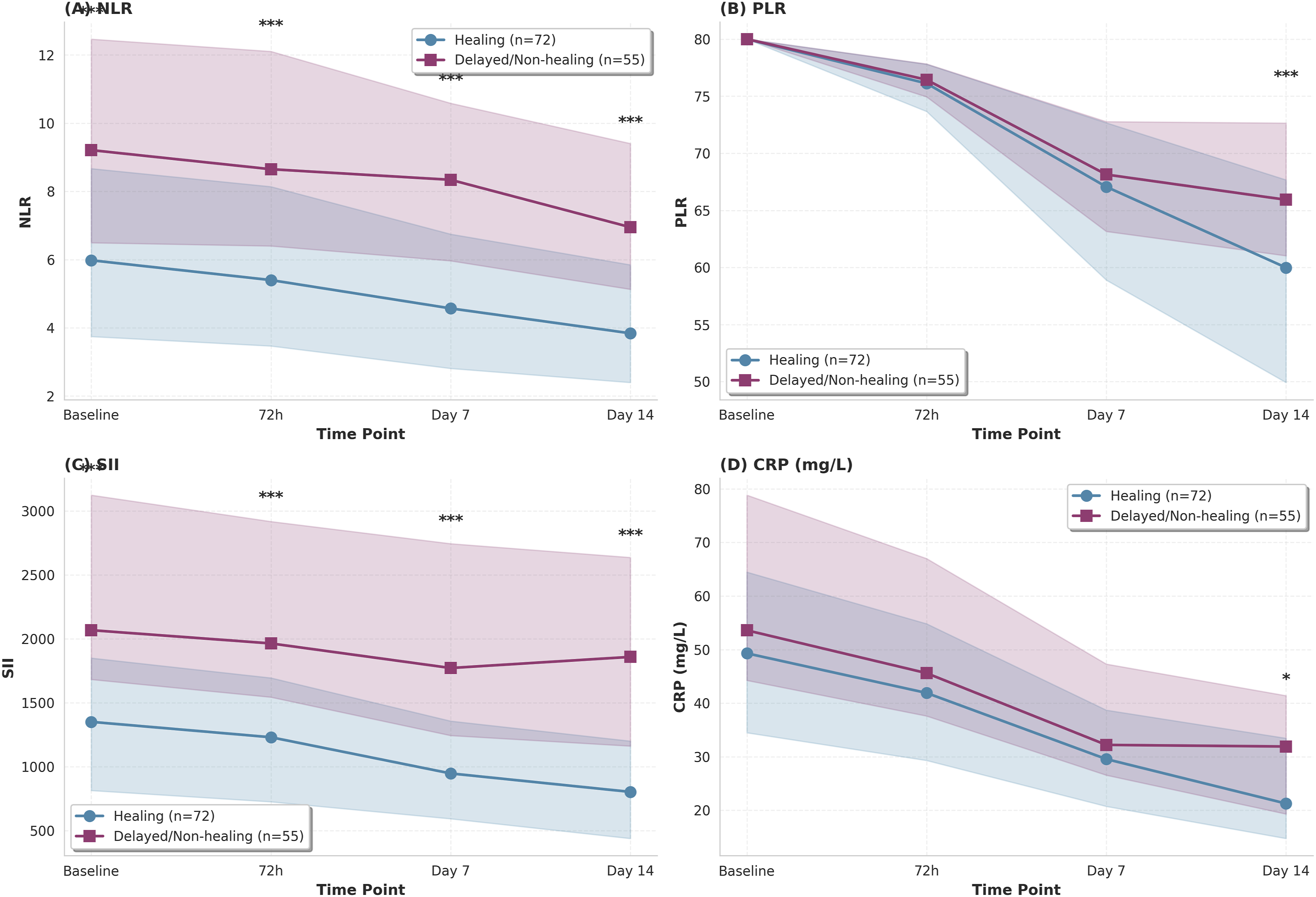
Temporal evolution of immune-inflammatory indices during early treatment. (a) Neutrophil-to-lymphocyte ratio (NLR), (b) Platelet-to-lymphocyte ratio (PLR), (c) Systemic immune-inflammation index (SII), and (d) C-reactive protein (CRP) from baseline through day 14 post-treatment. Data are shown as median with interquartile range (shaded areas). Blue lines represent the healing group (n=72); red lines represent the delayed/non-healing group (n=55). Asterisks indicate statistical significance: *P<0.05, **P<0.01, ***P<0.001 (Mann-Whitney U test).
Day 7 PLR changes were similar between groups (-16.2% vs -14.8%, P=0.375), though day 14 changes differed (-25.0% vs -17.6%, P<0.001). Day 14 CRP reduction did not differ significantly (-48.7% vs -43.5%, P=0.071) (Table 4). Figure 2 shows the temporal evolution of NLR, PLR, SII, and CRP from baseline through day 14, with the healing group showing steeper declines in NLR and SII. The magnitude of early NLR and SII reduction, rather than baseline CRP or PLR, discriminated between healing outcomes within the first week.
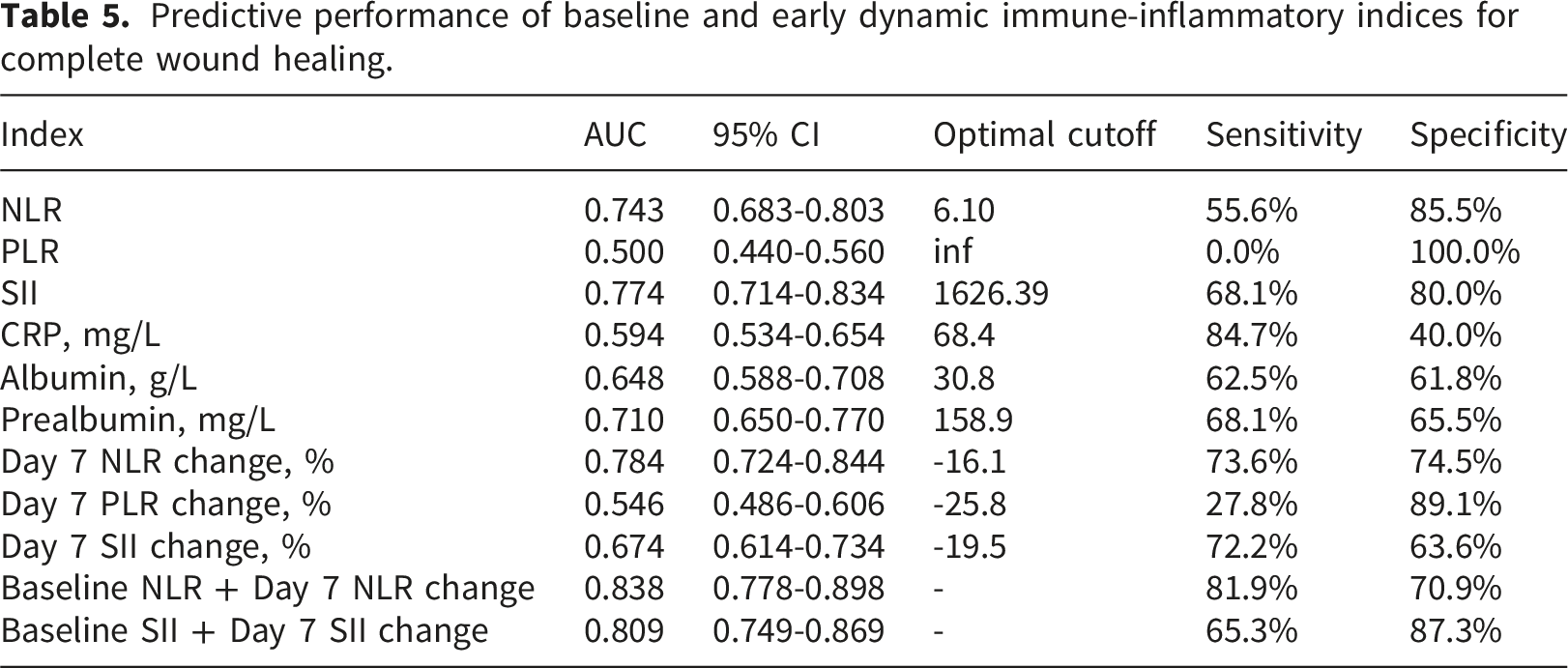
Predictive performance of immune-inflammatory indices
Predictive performance of baseline and early dynamic immune-inflammatory indices for complete wound healing.
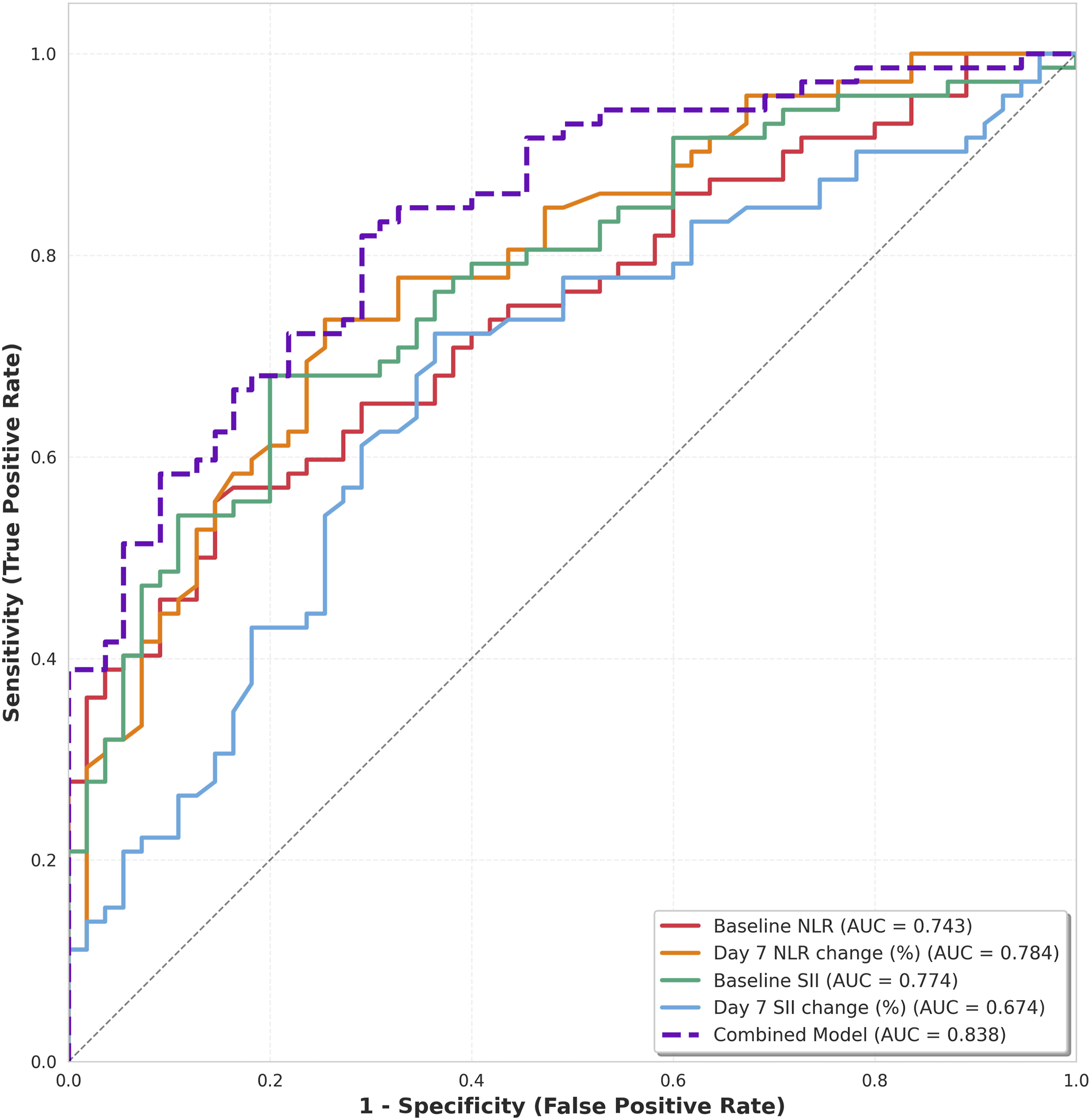
Receiver operating characteristic (ROC) curves for predicting complete wound healing. Comparison of baseline NLR (red), day 7 NLR change (orange), baseline SII (green), day 7 SII change (blue), and combined model incorporating baseline NLR plus day 7 NLR change (purple dashed line). The combined model achieved the highest area under the curve (AUC 0.838, 95% CI 0.778-0.898), outperforming individual markers. The diagonal dashed line represents random chance (AUC 0.5).
For early dynamic changes, day 7 NLR change had AUC 0.784 (95% CI 0.724-0.844; cutoff -16.1%, sensitivity 73.6%, specificity 74.5%). Day 7 SII change had AUC 0.674 (95% CI 0.614-0.734), while day 7 PLR change showed poor performance (AUC 0.546, 95% CI 0.486-0.606).
Combined models outperformed individual markers. Baseline NLR plus day 7 NLR change achieved AUC 0.838 (95% CI 0.778-0.898; sensitivity 81.9%, specificity 70.9%). Baseline SII plus day 7 SII change had AUC 0.809 (95% CI 0.749-0.869; sensitivity 65.3%, specificity 87.3%) (Table 5, Figure 3). These results indicate that combining baseline values with early dynamic changes provides superior predictive accuracy compared to either parameter alone.
Time-dependent analysis of healing prediction
To evaluate the temporal stability of predictive value, time-dependent ROC analysis was performed for 30-day, 60-day, and 90-day healing outcomes. The combined model incorporating baseline NLR and day 7 NLR change demonstrated consistent discriminative ability across different time horizons: AUC 0.798 (95% CI: 0.715-0.867) for 30-day healing, 0.834 (95% CI: 0.759-0.895) for 60-day healing, and 0.838 (95% CI: 0.778-0.898) for 90-day healing (Figure 4). Consistent performance across different time horizons supports the prognostic value of this model for both short- and long-term healing prediction. Time-dependent ROC analysis for healing prediction at different time points. The combined model (baseline NLR + day 7 NLR change) demonstrated consistent predictive performance for (A) 30-day healing (AUC 0.798, 95% CI 0.715-0.867), (B) 60-day healing (AUC 0.834, 95% CI 0.759-0.895), and (C) 90-day healing (AUC 0.838, 95% CI 0.778-0.898), indicating robust prognostic value across different time horizons.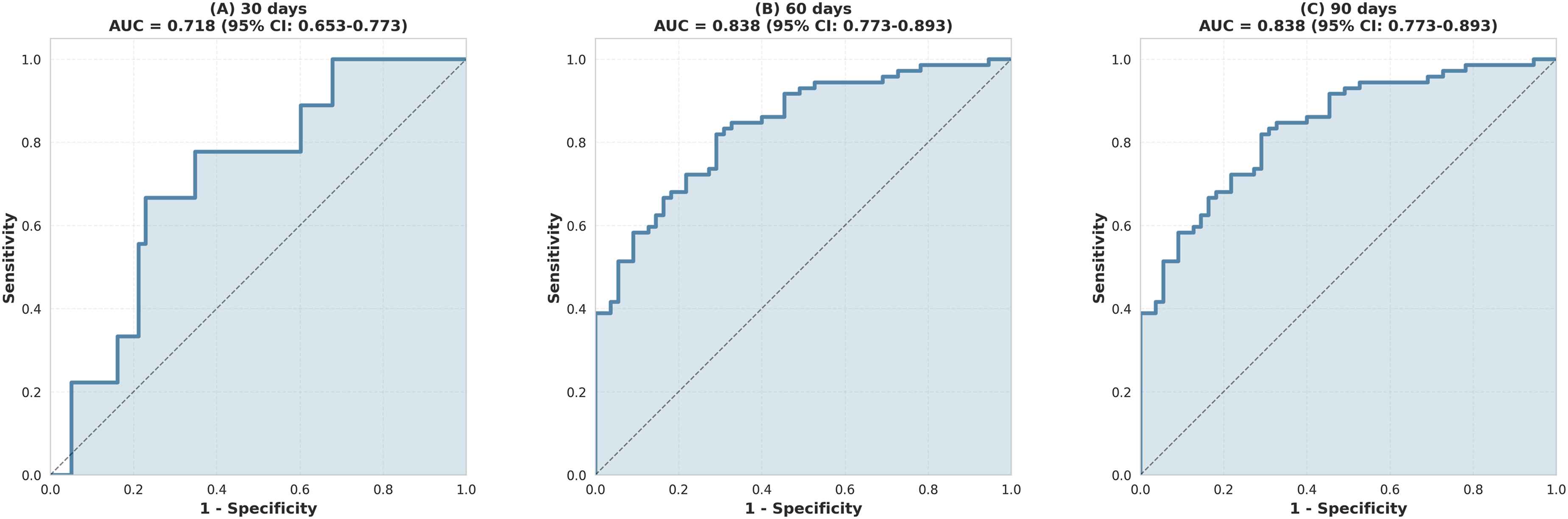
Discussion
This study demonstrates that baseline systemic immune-inflammation index and neutrophil-to-lymphocyte ratio, combined with early dynamic changes, predict healing after flap reconstruction for stage IV pressure injuries. The combined model achieved superior discriminative ability compared with individual markers, and temporal analysis confirmed consistent performance across different time horizons.
The biological basis for these inflammatory markers as predictors relates to their reflection of systemic immune and inflammatory status. Elevated neutrophil counts indicate ongoing inflammation, while decreased lymphocyte counts suggest immune dysfunction.10,18 Previous studies have demonstrated that elevated NLR predicts poor outcomes in various surgical conditions, including major oncologic surgery and cardiovascular procedures.19–22 In wound healing, persistent systemic inflammation impairs angiogenesis and collagen deposition, delaying epithelialization.23–25 The threshold identified in this study aligns with prior reports that NLR is a marker of impaired wound healing.26,27
The systemic immune-inflammation index incorporates platelet count in addition to neutrophil and lymphocyte counts, providing a more comprehensive assessment of immune-inflammatory balance.13,28 Platelets release growth factors essential for wound healing, including platelet-derived growth factor and transforming growth factor-beta. 29 Recent studies have shown that SII predicts complications after major abdominal surgery and sepsis outcomes,30–32 but application to pressure ulcer management has not been previously reported. Among baseline markers in this study, SII demonstrated the highest predictive value, suggesting that integrating platelet count provides clinically relevant information beyond NLR alone.
NLR and SII are non-specific markers of systemic immune-inflammatory burden. Elevated values may reflect occult infection, metabolic stress, or comorbidity load in addition to impaired healing capacity. The absence of a significant difference in CRP between groups argues against acute active infection as the primary driver of elevated NLR and SII in the delayed healing group. The lack of systematic procalcitonin or interleukin-6 data prevents a definitive separation of infectious from non-infectious contributions to the observed indices, representing a limitation of this study.
The magnitude of early reduction in inflammatory markers was a stronger predictor than baseline values. This finding suggests that treatment response, rather than initial severity alone, determines outcome. Similar observations have been reported in other surgical contexts, where failure to normalize inflammatory markers within the first week predicts complications.33,34 Day 7 NLR changeoutperformed baseline measurements, indicating that dynamic assessment captures the evolving physiological response to surgical intervention and wound healing. The practical implication is that serial measurement, rather than single baseline assessment, provides more actionable prognostic information.
Platelet-to-lymphocyte (PLR) ratio showed no predictive value in this study, with identical median values in both groups. This contrasts with reports of PLR predicting outcomes in cancer surgery and cardiovascular disease.35–37 The lack of discrimination may relate to the specific pathophysiology of pressure injuries, where platelet function is less critical than in thrombotic or malignant conditions. Alternatively, PLR may lack sufficient dynamic range in this patient population to differentiate healing trajectories.
The combined model demonstrated superior performance to individual markers. This improvement reflects the complementary information provided by baseline status and early dynamic response. Time-dependent analysis confirmed consistent performance across multiple time points, indicating that the model maintains accuracy regardless of when healing occurs. This temporal stability supports clinical utility for both early intervention and long-term prognostication.
Several factors contribute to the substantial proportion of patients in this cohort who experience delayed or incomplete healing. Older age, higher prevalence of diabetes, larger wound area, and lower Braden scores all impair healing capacity.38–40 The combination of multiple comorbidities and advanced tissue destruction creates a hostile local environment for reconstruction. Nutritional deficits, evidenced by lower albumin and prealbumin levels in the delayed healing group, further compromise healing potential. 41
Clinical application of these findings could modify management strategies. Patients with elevated baseline NLR or SII warrant heightened surveillance and may benefit from delayed definitive closure until the inflammatory burden decreases. Serial NLR measurement at day 7 identifies patients with inadequate treatment response, potentially prompting investigation for occult infection or adjustment of nutritional support.
This study has limitations. The retrospective design limits causal inference and introduces potential selection bias. Although offloading and positioning protocols were applied uniformly per institutional protocol, individual variation in patient adherence may constitute residual confounding that cannot be fully excluded in a retrospective design. Furthermore, while repositioning adherence was documented in nursing records, the absence of a formal compliance measurement tool limits the quantification of protocol adherence. Blood sampling times were protocol-driven but may not capture peak inflammatory responses in all patients. The single-center experience may not generalize to institutions with different patient populations or surgical techniques. Flap selection was not randomized, introducing confounding by indication. Follow-up duration varied among patients, although time-dependent analysis partially addressed this. A formal a priori sample size calculation was not performed, given the retrospective and exploratory nature of this study. The final sample of 127 patients was determined by eligibility criteria rather than a pre-specified power calculation, which may affect the precision of the reported effect estimates and the generalizability of the optimal cutoff values identified. External validation in an independent, prospective cohort is required before these findings can be translated into clinical practice.
The lack of data on specific interventions following the identification of unfavorable inflammatory profiles limits the assessment of whether early recognition translates into improved outcomes. Future studies should evaluate whether protocolized responses to elevated markers or inadequate early reduction improve healing rates. The optimal timing and frequency of inflammatory marker assessment beyond the initial postoperative period remains undefined. Whether these markers predict specific complications or only general healing failure warrants investigation.
Conclusions
Baseline SII and NLR, combined with early postoperative dynamic changes, may predict healing outcomes after flap reconstruction for stage IV pressure injuries. Early assessment of inflammatory marker trajectory may identify patients at risk for delayed healing within the first postoperative week. These readily available indices may serve as adjuncts to clinical judgment in guiding surveillance intensity and the timing of interventions, though prospective validation in independent cohorts is required before clinical implementation.
Footnotes
Ethical considerations
Ethical approval was obtained from the Ethics Committee of Medical Ethics Committee of the Affiliated Hospital of Xuzhou Medical University (Approval no. XYFY2026-KL086-01) at Affiliated Hospital of Xuzhou Medical University on On January 21st, 2026.
Consent to participate
Written informed consent was obtained from a legally authorized representative(s) for anonymized patient information to be published in this article. This study was a retrospective analysis of de-identified data. The institutional ethics committee approved the study protocol and waived the requirement for written informed consent.
Author contributions
Jingwei Wang and Xiaojie Zhao designed the study and carried them out, Jingwei Wang and Xiaojie Zhao supervised the data collection, Jingwei Wang and Xiaojie Zhao analyzed the data, Jingwei Wang and Xiaojie Zhao interpreted the data, Jingwei Wang and Xiaojie Zhao prepare the manuscript for publication and reviewed the draft of the manuscript. All authors have read and approved the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The authors declare that all data supporting the findings of this study are available within the paper and any raw data can be obtained from the corresponding author upon request.