
Abstract
Post-stroke patients frequently adopt compensatory trunk movements to accomplish tasks. This can lead to the development of abnormal movement patterns, which can hinder functional recovery. To address this issue, this study proposes a Human-Centric assist-as-needed strategy based on a upper limb rehabilitation robot. By constructing a closed-loop human-machine system, the exoskeleton assistance force is dynamically adjusted to inhibit compensatory trunk movements in hemiplegic patients while ensuring task completion. It employs Long Short-Term Memory (LSTM) networks to predict trunk compensation angles (R2=0.99) and combines Convolutional Neural Networks with Bidirectional LSTM (CNN-BiLSTM) to calculate compensation torque (R2=0.97), thereby achieving personalized and active torque assistance. Eleven patients with upper limb hemiplegia participated in the clinical trial. The results indicated that trunk compensation during training was significantly improved in all patients. Human-centric assist-as-needed strategy significantly reduces the compensatory angles of hemiplegic patients in the sagittal plane (76.79%), coronal plane (75.82%), and horizontal plane (87.47%) (p < 0.01), outperforming both the no intervention and task-centric strategies, with a 100% task completion rate during patient training. Compared to task-centric strategy, human-centric assist-as-needed strategy enhances patient intention consistency (IC) by 31.91% and increases average torque (AT) output by 48.02%. This study represents the first application of deep learning in the suppression of active trunk compensation for upper limb exoskeletons, providing an innovative approach to stroke rehabilitation.
Introduction
Stroke is a prevalent condition among the elderly and a leading cause of adult mortality worldwide. 1 The incidence of stroke has been steadily increasing in recent years, 2 with approximately 80% of stroke survivors experiencing varying degrees of upper limb motor dysfunction. 3 This reduction in limb functionality severely disrupts patients’ daily activities, lowers their quality of life, and amplifies the burden on caregivers.
Task-oriented repetitive motion training has been demonstrated as a highly effective rehabilitation strategy. 4 However, during such training, patients often resort to trunk compensation to achieve task objectives. 5 While this compensatory movement may facilitate short-term task completion, it poses numerous long-term disadvantages for patient recovery.6,7 Excessive trunk compensation not only limits the active use and functional recovery of the affected upper limb but can also solidify abnormal movement patterns, further impeding neuroplasticity-mediated functional restoration. 8 Unlike genuine functional regeneration, which relies on the repair of damaged areas, compensatory movements depend on the substitution of residual structures.9,10 This can lead to patients developing detrimental dependency habits, hindering true paretic limb recovery and even exacerbating postural control and daily living ability deficits. 11
Traditional clinical strategies include manual intervention by therapists and physical constraints. The former relies on one-on-one supervision and correction, which is time-consuming, labor-intensive, and costly. 12 The latter, which involves securing the patient’s trunk to a chair with belts or harnesses,13,14 while effective, can induce discomfort and anxiety. 15
Recent advancements in technologies such as robotics16–19 and biofeedback (e.g., auditory, visual, and force feedback) have introduced new avenues for reducing trunk compensation in upper limb rehabilitation training. Auditory feedback provides auditory cues to remind patients to maintain correct posture when compensation occurs.20,21 Visual feedback displays the patient’s compensation level on a screen to encourage reduction.22–25 Lin et al. reduced trunk flexion through a method of visual and auditory fusion. 26 The aforementioned types of feedback all encourage patients to consciously suppress compensatory behaviors. However, many stroke patients continue to rely on compensation when their motor abilities are inadequate. 27 Additionally, patients may encounter difficulties in simultaneously processing feedback information while inhibiting compensatory actions. 28 Valdés et al. initially established the viability of employing a dual end-effector robot for force feedback in compensation reduction, 29 while our earlier research confirmed that assistive force feedback outperforms audiovisual feedback in achieving compensation reduction. 30 However, these methods only serve to suppress the effects of trunk compensation after they occur, lacking a proactive approach.
In parallel with these developments, rehabilitation robotics has increasingly shifted from rigid task execution toward patient-cooperative and adaptive assistance paradigms. Rather than providing fixed assistance, such strategies emphasize dynamic regulation of robot behavior according to the patient’s residual ability, motor performance, and recovery stage. Dalla Gasperina et al. reviewed patient-cooperative control strategies for upper-limb rehabilitation exoskeletons and highlighted the importance of jointly considering training modality, control strategy, sensing system, and hardware implementation in order to improve treatment effectiveness. 31 More recent work has further shown that adaptive impedance regulation can adjust robot compliance according to the functional state of the affected limb, thereby improving rehabilitation adaptability and safety. 32 In addition, adaptive hybrid-mode assist-as-needed control has been proposed to modulate assistance online according to user performance, so that the robot can better balance support and active patient participation during training. 33
Beyond performance-based adaptation, biocooperative and multimodal control methods have also attracted increasing attention. These methods aim to synchronize robotic assistance with the user’s physiological and kinematic states, rather than relying solely on kinematic error or task completion. For example, cooperative control strategies based on joint-torque estimation and sEMG-related intention information have been shown to promote active patient involvement during upper-limb rehabilitation. 34 Likewise, EMG-driven shared control frameworks demonstrate the potential of integrating biosignals with robot control to generate more personalized and intention-consistent assistance. 35 These studies suggest that rehabilitation robots should not only correct movement errors, but also respond to the user’s voluntary effort and movement state in a human-centered manner.
Furthermore, our prior research indicated the potential for rehabilitation robots to reduce compensatory movements by providing assistive forces.36,37 In our pilot study, we provided horizontal assistive forces to mitigate compensatory movements; however, we did not account for the individual differences among subjects. To enhance the training quality of patients during robotic rehabilitation, it is advantageous to explore dynamic assistance based on the degree of trunk compensation, which can correct compensatory movements in real time. 38 Nevertheless, most existing compensation-suppression approaches remain reactive, in the sense that intervention is triggered only after abnormal trunk motion has already emerged. There remains a lack of human-centered control strategies that can proactively predict trunk compensation trends, estimate the required assistance, and deliver individualized intervention while preserving the patient’s active role in task completion.
In this context, the use of deep learning is motivated by the fact that trunk compensation is a nonlinear and time-dependent behavior jointly influenced by historical trunk posture, affected-limb motion, task demand, and interaction torque. Likewise, the estimation of compensation-related assistance torque also involves complex nonlinear relationships and temporal dependencies. Compared with simple threshold-based or linear predictive models, deep learning architectures are better suited to capturing these multivariable temporal dynamics and supporting real-time individualized assistance regulation.
The main contributions of this study are summarized as follows: 1. To the best of our knowledge, this study presents the first clinical validation of an upper-limb exoskeleton that applies deep learning to achieve proactive trunk compensation suppression during rehabilitation training in chronic stroke patients. 2. Unlike conventional assist-as-needed strategies that provide assistance only after compensatory movement or task error has already occurred, the proposed method introduces a predictive and feedforward assistance mechanism. Specifically, an LSTM-based trunk compensation angle prediction model is first used to estimate the upcoming compensation state, and a CNN-BiLSTM-based compensation torque calculation model is then employed to generate individualized assistance in advance. Based on these models, a multi-layer control framework, termed the human-centric assist-as-needed (HCAAN) strategy, is developed to intervene before excessive trunk compensation is fully developed. 3. Clinical experiments demonstrate that the proposed HCAAN strategy can significantly reduce trunk compensation in the sagittal, coronal, and horizontal planes while maintaining a high task completion rate during rehabilitation training.
Experimental setup
To achieve the control strategy for inhibiting trunk compensation, an integrated rehabilitation training platform was constructed for assistance training and monitoring evaluation. As shown in Figure 1, the platform is divided into three components: an upper limb exoskeleton robot, a trunk compensation monitor, and a virtual rehabilitation training game system. Rehabilitation Training Platform Based on Trunk Compensation Inhibition. a) represents the Upper Limb Rehabilitation Robot, which is utilized to detect the active torque and provide assistive training. b) denotes the Trunk Angle Monitor, which measures the trunk compensation angle and evaluates the extent of trunk compensation. c) refers to the Virtual Rehabilitation Training Game System, which presents training objectives in a game format.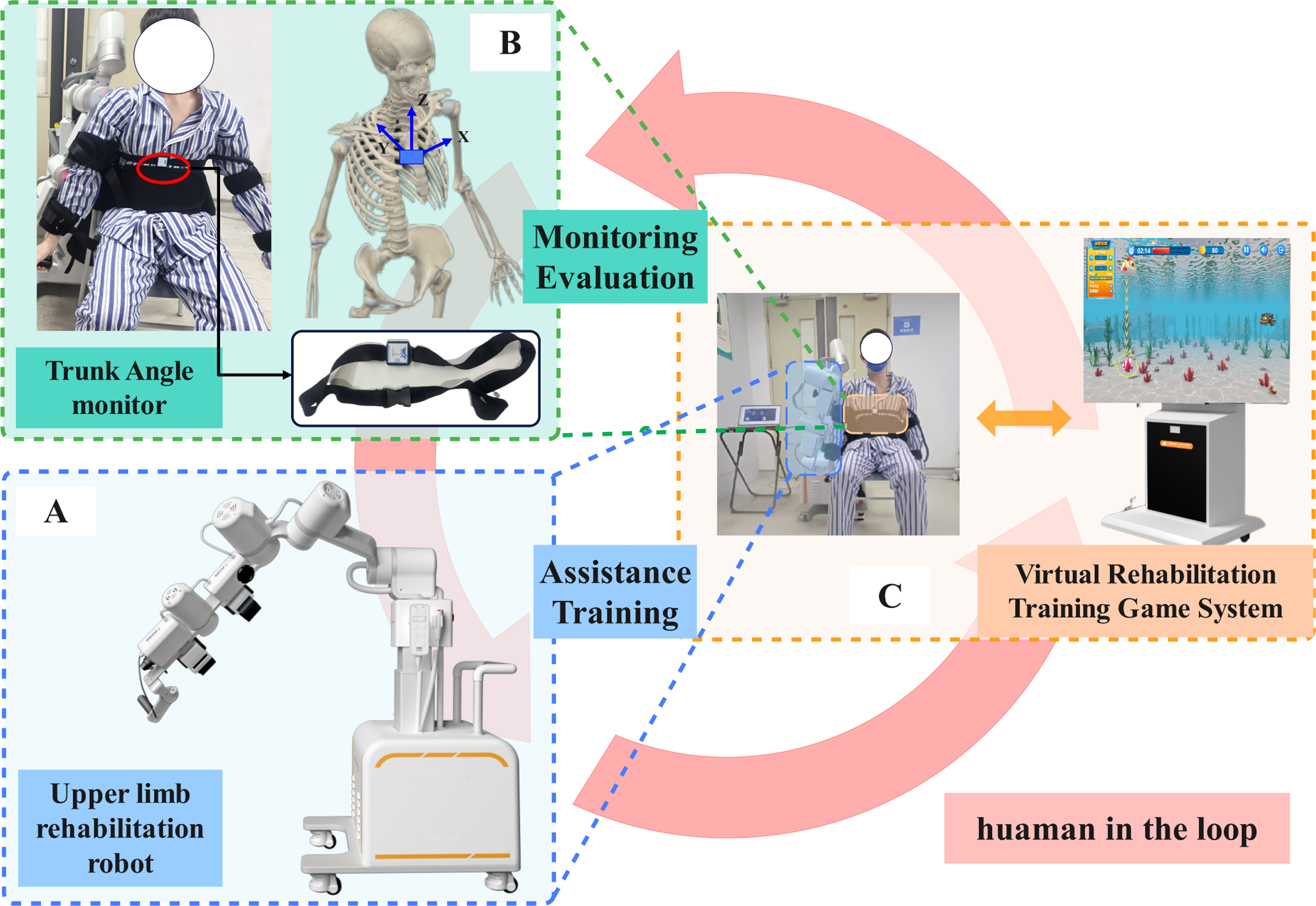
Upper limb rehabilitation robot
The upper limb rehabilitation robot is designed to detect the active torque exerted by patients and to provide assistive torque during their training sessions. The robot features a self-developed serial mechanism with four degrees of freedom, as illustrated in part A) of Figure 1. Of these degrees, three are dedicated to the movement of the shoulder joint—specifically for flexion/extension, abduction/adduction, and external/internal rotation—while the fourth degree facilitates the extension/flexion of the elbow joint. Each joint module of the robot is equipped with a brushless DC motor (48 V) paired with a 100:1 harmonic reducer and a torque sensor. Specifically, joints J1 and J3 employ HJ25 motors (rated power: 440 W; rated speed: 2950 rpm; rated load torque: 115 N⋅ m) to meet the high-load demands of proximal shoulder tasks. Joint J2 employs an HJ20 motor (366 W; 3500 rpm; 78 N⋅ m), and the elbow joint J4 employs an HJ17 motor (183 W; 3500 rpm; 40 N⋅ m) to reduce distal inertia and improve comfort. The shoulder torque sensors have a rated load of 100 N⋅ m with a comprehensive error of ±0.1% F.S., while the elbow torque sensor is rated at 50 N⋅ m with the same accuracy. The system communicates via CAN bus (CANopen protocol) at 1000 Hz, transmitting joint position, velocity, current, and temperature in real time. For safety, each motor integrates a permanent-magnet friction brake that passively locks the joint upon power loss or emergency stop, and software-level torque limits are enforced at each joint throughout training.
Trunk angle monitor
To detect the trunk compensation angle of patients and assess the extent of trunk compensation, a trunk angle monitor was constructed using the MPU9250 nine-axis inertial sensor (InvenSense), which integrates a triaxial accelerometer, gyroscope, and magnetometer. Attitude estimation was performed using an Extended Kalman Filter (EKF), in which the accelerometer provides a gravity reference for roll and pitch correction, while the magnetometer provides a heading reference for yaw correction, thereby suppressing accumulated gyroscope drift over time. Before each experimental session, a two-stage calibration procedure was conducted. First, hard-iron and soft-iron calibration was performed in a magnetic-field-free environment to correct sensor bias and cross-axis sensitivity. Second, the subject maintained a standardized upright seated posture for static initialization, during which the sensor output was recorded as the zero-angle reference to eliminate individual postural offset. After these procedures, the trunk angle monitor achieved a measurement accuracy of 0.2° in the sagittal and coronal planes and 1° in the horizontal plane, with an output frequency of 200 Hz. The monitor is worn on the chest of the subject, as illustrated in Figure 1, and transmits trunk angle data to the upper limb rehabilitation robot in real time.
As shown in Figure 2, the rotation angle around the X-axis (sagittal plane) is regarded as positive in the counterclockwise direction, indicating forward flexion of the trunk, and negative in the clockwise direction, signifying backward extension of the trunk. Counterclockwise rotation around the Y-axis (coronal plane) is classified as a positive angular change, indicating left lateral flexion of the trunk, while right lateral flexion is recorded as a negative value. Additionally, counterclockwise rotation around the Z-axis (horizontal plane) is noted as a positive value, reflecting left rotation of the trunk, whereas clockwise rotation is recorded as a negative value, corresponding to right rotation, with a dynamic range of ±90°, which meets the requirements for activities of daily living (ADL). Prior to commencing the test, the subject is instructed to sit in a chair for static calibration. The angle of trunk compensation is transmitted via WiFi to the upper limb rehabilitation robot, enabling the robot to determine when to assist the patient and thereby inhibit trunk compensation. Trunk compensatory movements and angles in the coronal, sagittal and horizontal planes.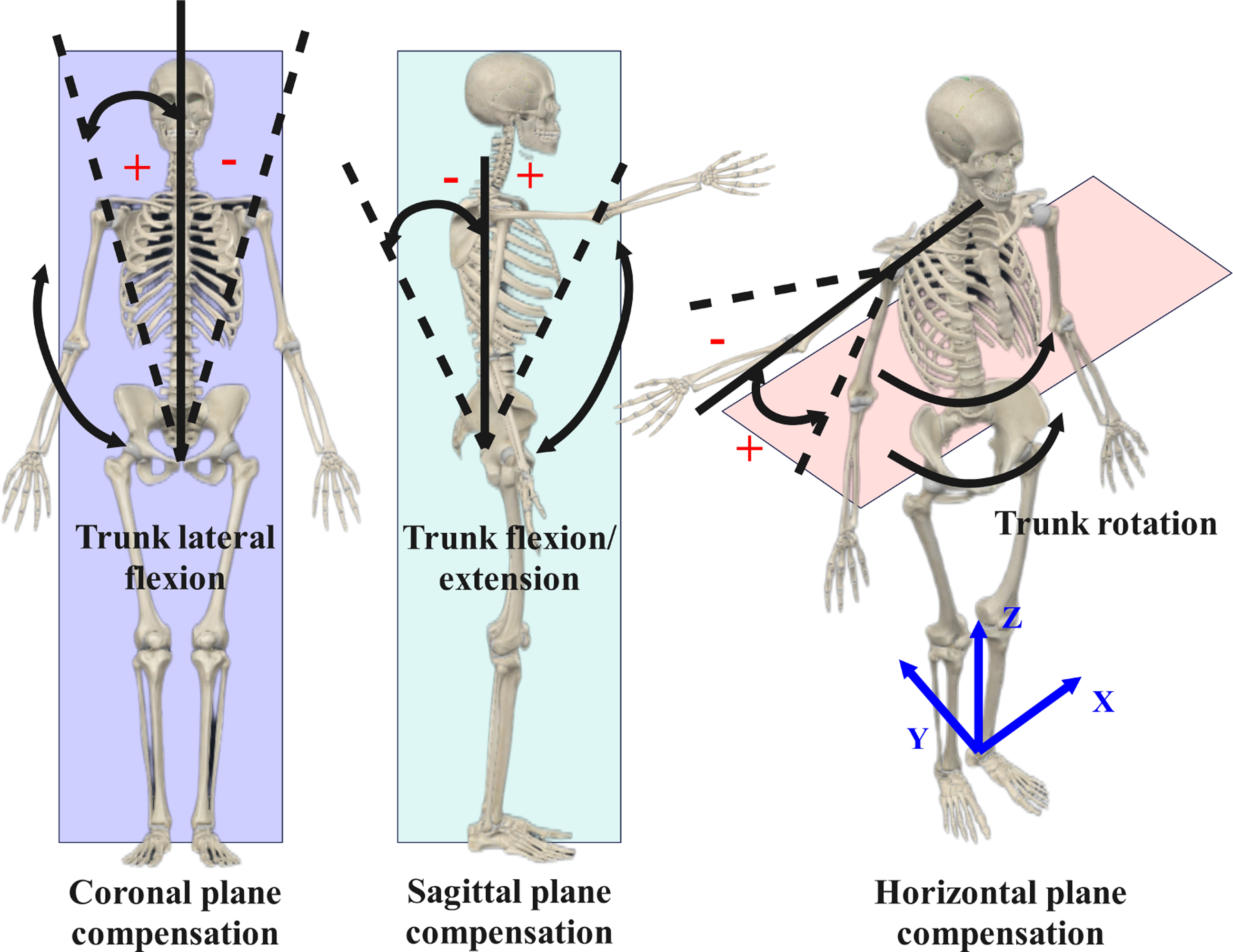
Virtual rehabilitation training game system
The rehabilitation training game system is designed to present training objectives in an interactive format, as shown in Figure 3, thereby improving patient engagement while promoting functional upper-limb movement patterns. The game is based on task-oriented training theory, and the selected movement—bilateral shoulder flexion—corresponds to a fundamental ADL reaching pattern. The controlled object (red circle) is driven in real time by the endpoint position of the upper-limb exoskeleton, creating a direct visuomotor loop between physical movement and visual feedback. The task target (green circle) is counted as hit once contact is made. Directional arrow cues encourage proactive upper-limb initiation in the correct direction, thereby reducing reliance on trunk-dominant compensatory strategies. Each target remains visible for 7 s, a duration determined from pilot observations of hemiplegic patients’ reaction and movement times. In our experiments, each control condition lasted 5 min with a 5-min rest interval, and task completion was scored out of a maximum of 42 points. Interface of the virtual rehabilitation training game.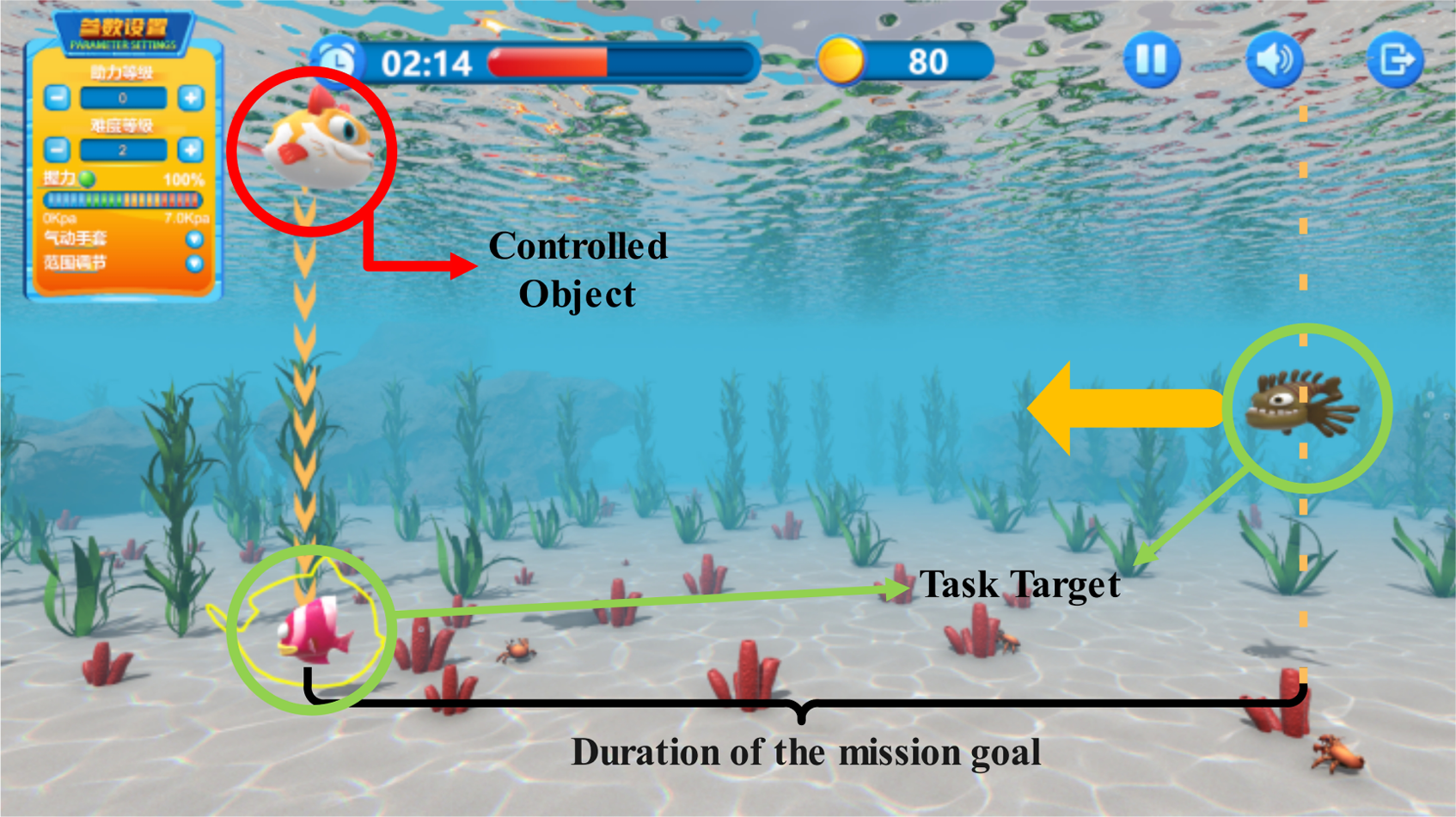
Methods
In response to the potential hazards associated with trunk compensation during task-oriented training, we propose a novel human-in-the-loop hierarchical architecture termed the HCAAN control strategy, as illustrated in the Figure 4. This control strategy comprises three layers: the trunk compensation assessment layer, the inhibition torque calculation layer, and the robot compliant drive layer. The trunk compensation assessment layer primarily focuses on determining the optimal timing for providing trunk compensation assistance. The inhibition torque calculation layer is responsible for calculating the required magnitude of torque to aid the patient in suppressing trunk compensation. Finally, the robot compliant drive layer ensures the smooth application of the assisting torque to the individual. Control framework of the HCAAN strategy. It is composed of the Trunk Compensation Assessment Layer, the Inhibition Torque Calculation Layer, and the Robot Compliant Drive Layer. Initially, the compensation status of the subject is assessed to determine whether assistance is needed. Following this assessment, the required assistance torque is calculated using the Trunk Compensation Torque Calculation Model. Finally, the Robot Compliant Drive Layer drives the exoskeleton to assist the subject during training.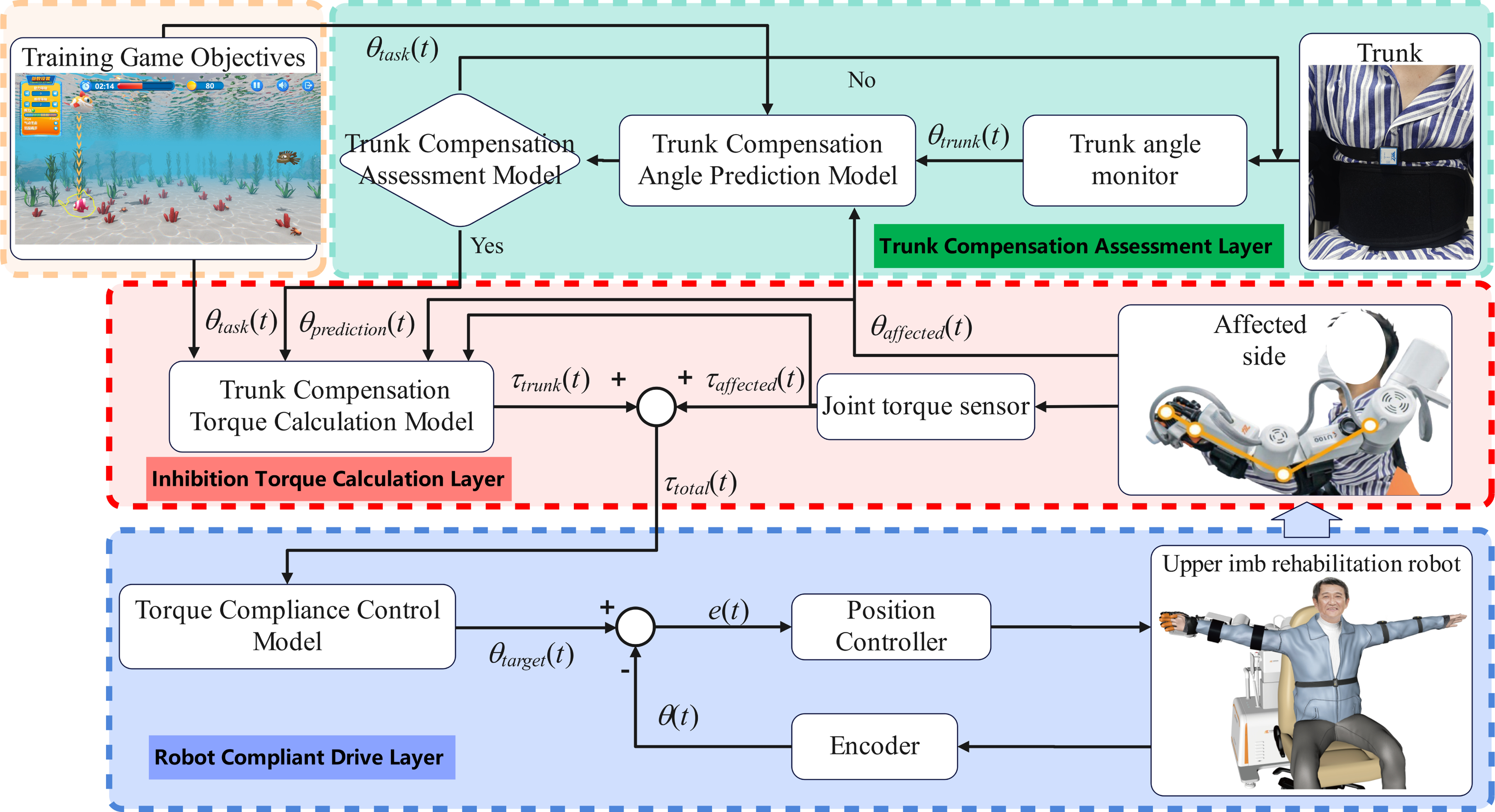
Trunk compensation assessment layer
The core of the Trunk Compensation Assessment Layer lies in evaluating the appropriate timing for assistance. It should be emphasized that the prediction models adopted in this study follow a personalized modeling paradigm. Specifically, an independent model is trained for each subject using only that subject’s own data. The training, validation, and testing datasets are all derived from the same individual, rather than pooled across different subjects. To prevent overfitting and ensure model robustness, we implemented a rigorous data partitioning strategy: the dataset for each subject was split into training (70%), validation (15%), and testing (15%) sets. The test set remained entirely independent and was used solely for final performance evaluation. Furthermore, During training, the validation set was used to monitor the model’s performance; training was terminated as soon as the validation loss reached its minimum to prevent the model from learning noise within the training data.
Accordingly, the objective of the proposed model is not to achieve cross-subject generalization, but to accurately capture individual-specific trunk compensation patterns in real time, in order to support personalized assist-as-needed control. It primarily consists of three components: the trunk angle monitor, the trunk compensation angle prediction model, and the trunk compensation assessment model. The trunk angle monitor measures the historical trunk angle (θ trunk ). It, combined with the angle of the affected arm (θ affected ), and the target task angle (θ task ), serves as inputs to the trunk compensation angle prediction model.
The outputs of the model are the predicted trunk compensation angles at 100 ms (θ
trunk−100
), 150 ms (θ
trunk−150
), and 200 ms (θ
trunk−200
). The prediction horizon of 100–200 ms was selected as a compromise between control usefulness and prediction reliability. It provides sufficient lead time for compensation assessment, torque computation, and smooth robotic assistance delivery, while remaining within a short-term interval where near-future trunk motion can still be predicted reliably. The model structure is illustrated in Figure 5. Structure of the Trunk Compensation Assessment Layer. It was used to assess the trunk compensation status of the subjects by predicting the future trunk angles.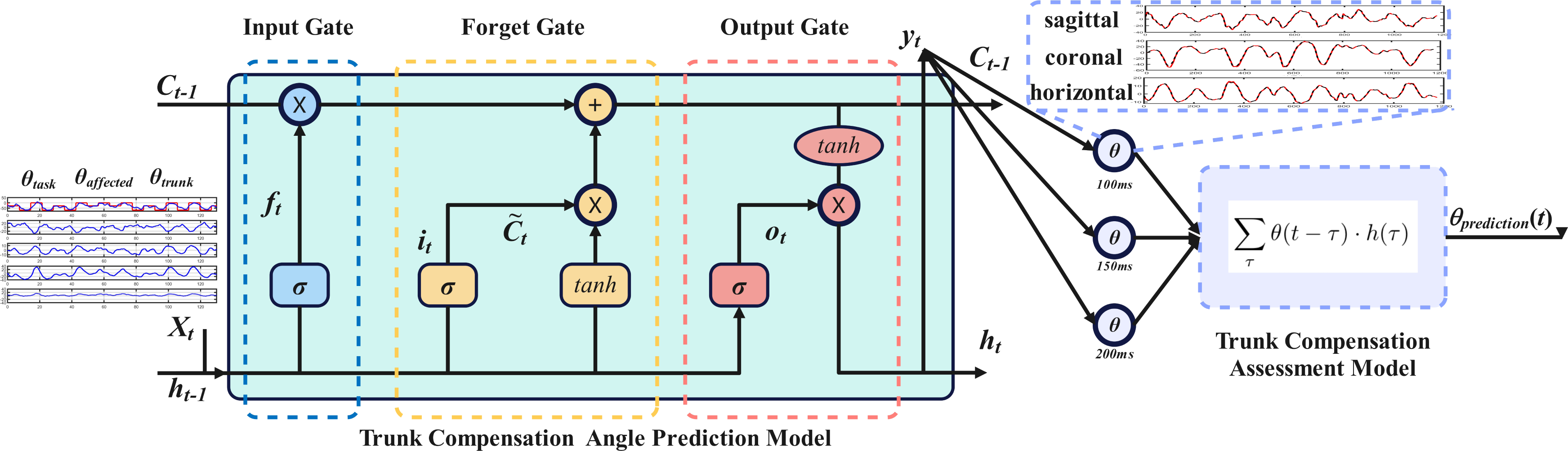
Input data were preprocessed using Z-score standardization. Input-output pairs were constructed using a sliding window approach with a window size of 200 ms (40 sample points at 200 Hz) and a stride of 100 ms (20 sample points), yielding 50% temporal overlap. For each subject, approximately 5 min of bilateral shoulder flexion data were collected per condition at 200 Hz, corresponding to about 60,000 raw samples per condition. After segmentation, each condition yielded about 3,000 input-output pairs, and the combined dataset contained approximately 9,000 pairs per subject. Forget Gate:

The forget gate determines the retention of previous time-step cell state information Ct−1.
Input Gate:



The cell state C t undergoes dynamic memory updates by discarding historical information through the forget gate and incorporating new information through the input gate.
Output Gate:


The output gate controls the cell state’s contribution to the hidden state h t , representing the current time-step output.
After processing the entire time window, the LSTM network outputs the final time-step hidden state h
tw
, which is mapped to a single output via a fully connected layer:

This study employed the Adam optimizer with an initial learning rate of 0.005 to facilitate rapid initial convergence. A learning rate decay strategy was implemented, reducing the learning rate to 50% of its previous value every 40 training epochs. The maximum training epoch was set to 150, and validation was performed every 30 iterations. Gradient clipping was applied with a threshold of 1.
To obtain suitable assistance opportunities, this paper establishes a trunk compensation assessment model by integrating the predicted compensation angles at three distinct time points. To emphasize the overall trend of trunk compensation, we process θ(t) using the convolution kernel h(t).

The Gaussian kernel effectively filters out high-frequency noise through weighted averaging while preserving the underlying trunk compensatory trend.

The discrete Gaussian kernel is:

If the compensation angle θ prediction (t) of the trunk in any single anatomical plane exceeds the threshold θ th , the trunk compensation assessment layer will activate the inhibition torque calculation layer, thereby triggering the calculation of the auxiliary torque to suppress trunk compensation.
Inhibition torque calculation layer
The Inhibition Torque Calculation Layer primarily focuses on determining the appropriate amount of auxiliary torque to provide to the patient. Traditional assistive forces are established based on the error relative to the task objective,39–41 which overly relies on the task objective while neglecting the patient’s autonomous control. The control strategy in this section is human-centric, calculating the minimal assistive force necessary to inhibit trunk compensation. The torque measured by the torque sensor (τ
man
) can be regarded as the torque exerted by the subject’s arm and trunk:

The τ man represents the minimum amount required for the subject to complete the task. To calculate the necessary torque (τ trunk ) for the subject to achieve various task objectives, we designed a trunk compensation torque calculation model that establishes the relationship between external conditions and τ trunk .
The model is based on a CNN-BiLSTM structure and utilizes the predicted compensatory angle (θ
prediction
), arm angle (θ
affected
), task objective angle (θ
task
), and current torque (τ
affected
) as inputs. This architecture was selected because compensation-related torque estimation involves both local short-term patterns in multivariable sequential inputs and temporal dependencies across the movement process. The CNN blocks extract local features and improve robustness to signal variation, whereas the BiLSTM block captures temporal context relevant to the generation of compensation-related assistance torque. This design enables predictive torque estimation while maintaining real-time feasibility. The model structure is illustrated in Figure 6. Structure of the Trunk compensation torque calculation model.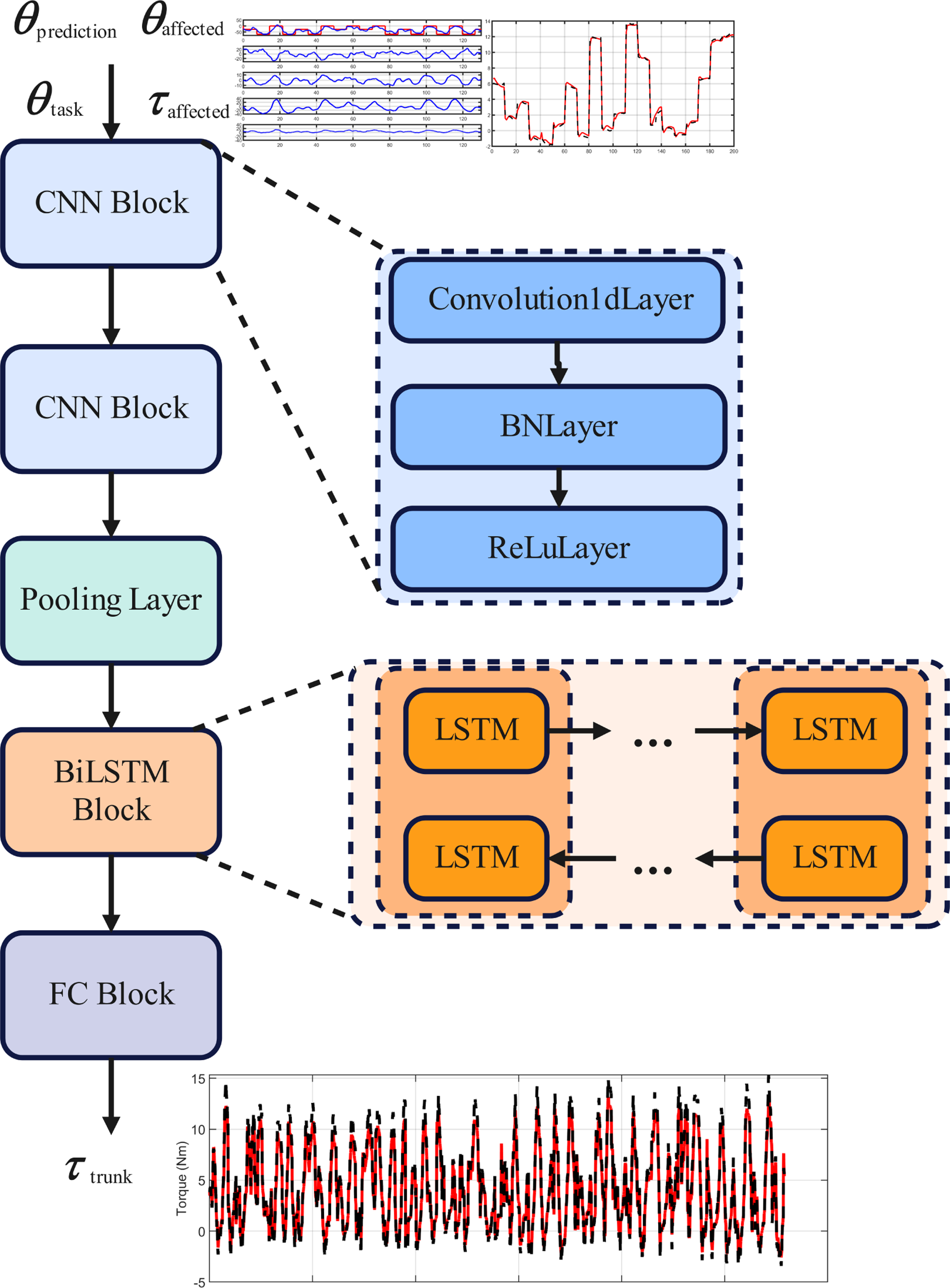
The first CNN block employs one-dimensional convolution with 32 kernels, each of size 3, to extract local features from the input data. The second CNN block further refines higher-level features, utilizing 64 kernels of size 3. The pooling layer reduces the sequence length while retaining the most significant features by taking local maxima along the time dimension. The pooling window size is 2, with a stride of 2. This pooling operation filters out secondary information, highlights prominent patterns, and reduces computational complexity.
The BiLSTM block, central to processing time series, comprises 256 units to capture long-term dependencies. Its “bidirectional” nature enables simultaneous processing of the sequence in forward (past to future) and reverse (future to past) directions, integrating both perspectives to enhance predictive accuracy, with 256 forward and 256 reverse units. The final output is
Finally, the model incorporates two fully connected layers: the first fully connected layer maps the 512-dimensional output of the LSTM to 128 dimensions, performing initial feature integration. The second fully connected layer maps the 128-dimensional features to 1 dimension, outputting the predicted torque value τ trunk (t).
The final output torque value is given by:

Robot compliant drive layer
During upper-limb rehabilitation for hemiplegic patients, the exoskeleton robot must deliver smooth, physiologically compliant assistive torque to ensure natural and safe motion trajectories. Based on the predicted and current torque values, a cubic polynomial interpolation method transitions the torque smoothly from the current torque (τ0) to the target value (τ
target
) within a specified timeframe.

The time step Δt is 1/f s . The total time T, representing the transition time from the starting point to the peak, is 100 ms in this paper. The time vector t = [0, Δt, 2Δt, …, T].
Cubic polynomial interpolation, a commonly used method for generating smooth trajectories, is expressed as:

At t = 0, the torque equals the starting value.

Substituting into the polynomial:

At t = T, the torque value is the peak value:


The final cubic polynomial equation is:

Admittance control can generate reasonable motion trajectories through force input, thereby avoiding rigid collisions.
42
Subsequently, admittance control is utilized as the outer loop control, while PID control is employed as the position controller.
43
The expression for admittance control is:

M is the mass matrix, B is the damping matrix, and K is the stiffness matrix.
Experiment
The clinical experiment aims to verify whether the HCAAN strategy can effectively reduce the trunk compensation angle of patients during rehabilitation training.
Participants
Participant characteristics.
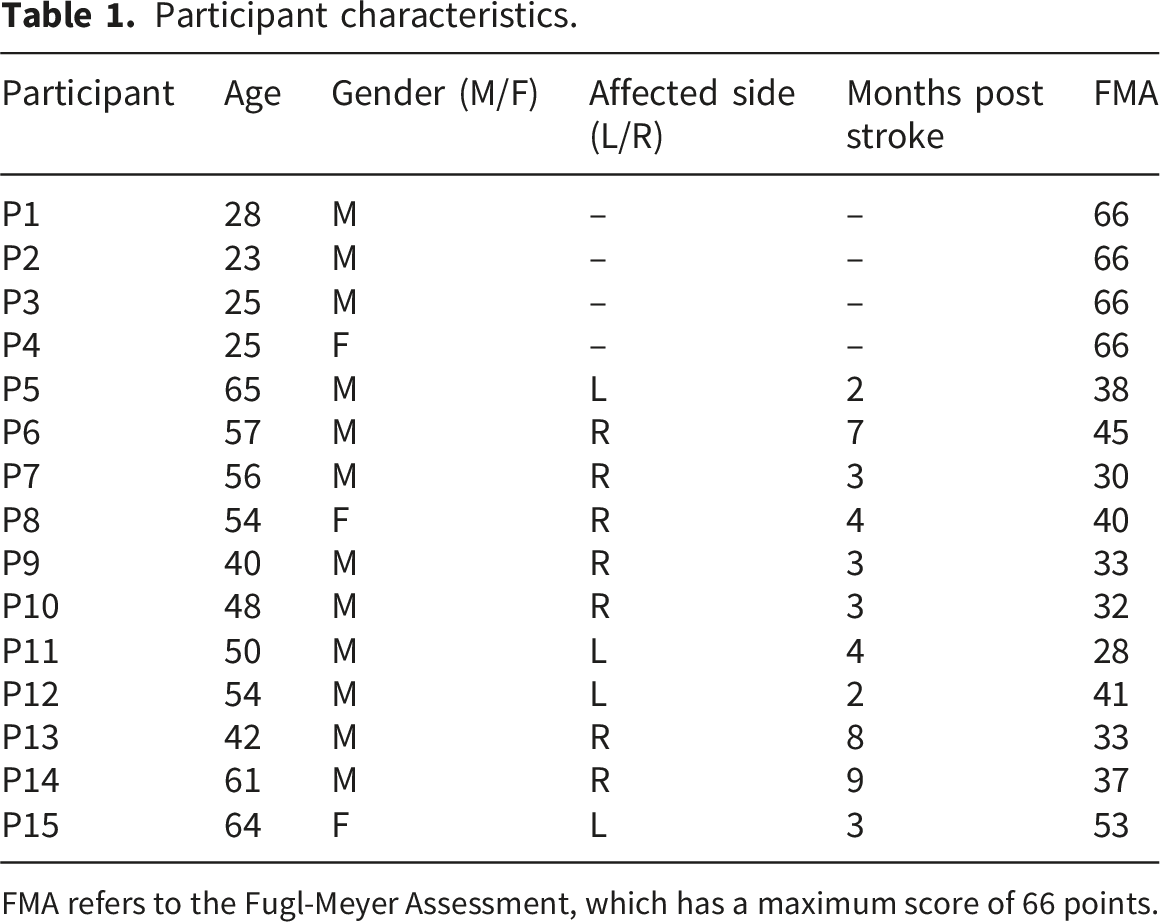
FMA refers to the Fugl-Meyer Assessment, which has a maximum score of 66 points.
Experimental protocol
The subjects were divided into two groups: the healthy group served primarily as a reference baseline for non-pathological trunk motion characteristics, whereas the stroke group served as the main experimental cohort for evaluating the proposed control strategy. There were a total of three control modes: 1) No Intervention (NI) strategy, in which the exoskeleton provided no assistance; 2) Task-Centric Assist-As-Needed (TCAAN) strategy, when trunk compensation occurs, the exoskeleton delivered assistive torque based on task objectives and proportional-derivative (PD) control 44 ; and 3) HCAAN strategy, in which the exoskeleton provided assistive torque based on model calculation results.
Controller parameters of NI, TCAAN and HCAAN.

As shown in the Figure 7, the Participants completed the training task according to the target guidance of the virtual rehabilitation training game system. The exoskeleton is in admittance mode and can follow the movement of the participants. The order in which each control strategy appears is random. The duration was set to 5 minutes to ensure subjects reached a stable motor state while preventing muscle fatigue, which could otherwise act as a confounding variable by triggering additional compensatory behavior. During these 5 minutes, the virtual rehabilitation training game system presented a total of 42 task points. To mitigate potential learning effects and motor adaptation, the sequence of the three control modes was randomized for each subject, and a 5-minute rest interval was provided between trials to ensure a complete washout effect. Experimental Procedure, each mode trained for 5 minutes.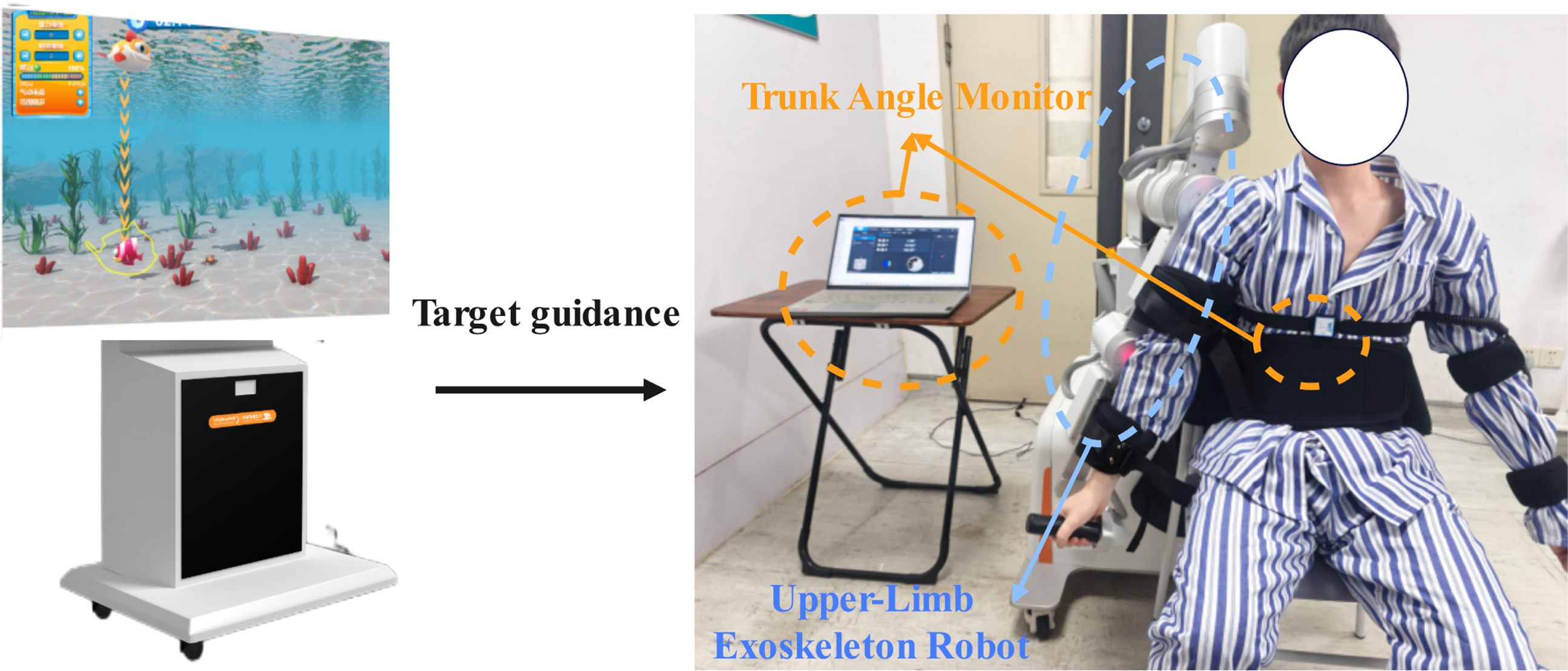
Experimental evaluation metrics
The experiment was evaluated based on trunk compensation angles, active engagement, and task completion rates. Statistical analysis was performed using SPSS. To evaluate the significance of differences across the three control modes (NI, TCAAN, HCAAN), a One-way Repeated Measures ANOVA was conducted for parametric data, followed by Bonferroni post-hoc tests. For non-parametric data, the Friedman test with Nemenyi post-hoc analysis was employed. Significance levels were set at p< 0.05 and p< 0.01.
Trunk compensation angles
Trunk compensation angles were evaluated in the sagittal, coronal, and horizontal planes for subjects under NI, TCAAN and HCAAN.
Intention consistency
During the rehabilitation training process, assuming the patient is fully focused on the rehabilitation task, the direction of the force applied by the patient should be synchronized with the acceleration of the preset motion trajectory over time. To quantify the level of the patient’s active participation and its alignment with the training objectives, an index called Intention Consistency (IC) has been established based on the cross-correlation coefficient. IC measures the correlation between the torque actively generated by the patient and the acceleration of the affected side’s trajectory in the rehabilitation task, thereby assessing the degree of alignment between the patient’s active intention and the rehabilitation goals throughout the training process. Its mathematical expression is as follows:
T p (t) represents the torque actively generated by the patient at a specific moment, while a(t) signifies the acceleration signal of the affected side’s trajectory. According to this formula, the IC value ranges from -1 to 1. A value closer to 1 suggests that the trajectory’s force primarily originates from the patient’s active intention on the affected side, rather than from assistance provided by the exoskeleton, indicating a higher level of patient engagement. Conversely, a value approaching -1 reflects completely opposing intentions between the two. A value near 0 indicates a lack of significant correlation, suggesting that during the rehabilitation training process, the patient did not actively engage, and the trajectory produced by the affected side was predominantly influenced by the assistive force generated by the exoskeleton.
Average torque
Quantifying the magnitude of the patient’s active force is crucial for assessing the quality of their training. The average torque (AT), as a key evaluation metric, effectively reflects the patient’s average force exertion throughout the training cycle. The calculation formula is as follows:
Rehabilitation training scores
Rehabilitation training scores, a critical indicator, reflects the patient’s performance in rehabilitation training game, measured by task outcomes per unit time. As task duration and difficulty were consistent across participants, task completion per unit time corresponds to the number of targets hit in each strategy, equivalent to the patient’s game score, with a maximum of 42 points.
Results
Performance of the trunk compensation angle prediction model and trunk compensation torque calculation model
Model performance.

It can be observed that the RMSE and MAE values of the trunk compensation angle prediction model across the three anatomical planes are all less than 1.5°, indicating that the model exhibits excellent predictive performance on the sagittal, coronal, and horizontal anatomical planes. Additionally, the R2 value of the trunk compensation torque calculation model is close to 1, signifying a high degree of consistency between the predicted and actual values. The performance metrics RMSE and MAE of the torque calculation model are both less than 1 Nm, demonstrating that the model effectively captures the dynamic changes in compensatory torques of the trunk.
Distribution of trunk compensation angles under NI, HCAAN and TCAAN
(a) Sagittal Plane for Healthy subjects (b) Coronal Plane for Healthy subjects (c) Horizontal plane for Healthy subjects (d) Sagittal Plane for Hemiplegic subjects (e) Coronal Plane for Hemiplegic subjects (f) Horizontal plane for Hemiplegic subjects
Figure 8 presents the experimental results of trunk compensation angles in healthy individuals and hemiplegic patients across three anatomical planes (sagittal, coronal, and horizontal) and under three control strategies (NI, HCAAN, and TCAAN). Under the NI strategy, as illustrated in the probability distribution plots of Figure 8(a)-(c), the trunk compensation angles of the healthy group exhibit a unimodal distribution centered at 0 degrees across all three anatomical planes. The box plots in Figures 8(a)-8(c) indicate that the median of the healthy group is 0°, with inner fences (IF) ranging from [-2°, 2.2°], suggesting that the trunk compensation angles of healthy individuals fluctuated within a narrow range for the majority of the training task duration. Statistical distribution of trunk compensation angles for healthy and hemiplegic participants. On the left side of the six small figures (a)-(f), the probability density distribution plots of the trunk compensation angles illustrate the distribution trend of these angles. The right side features box plots and violin plots that depict the specific distribution characteristics of the trunk compensation angles.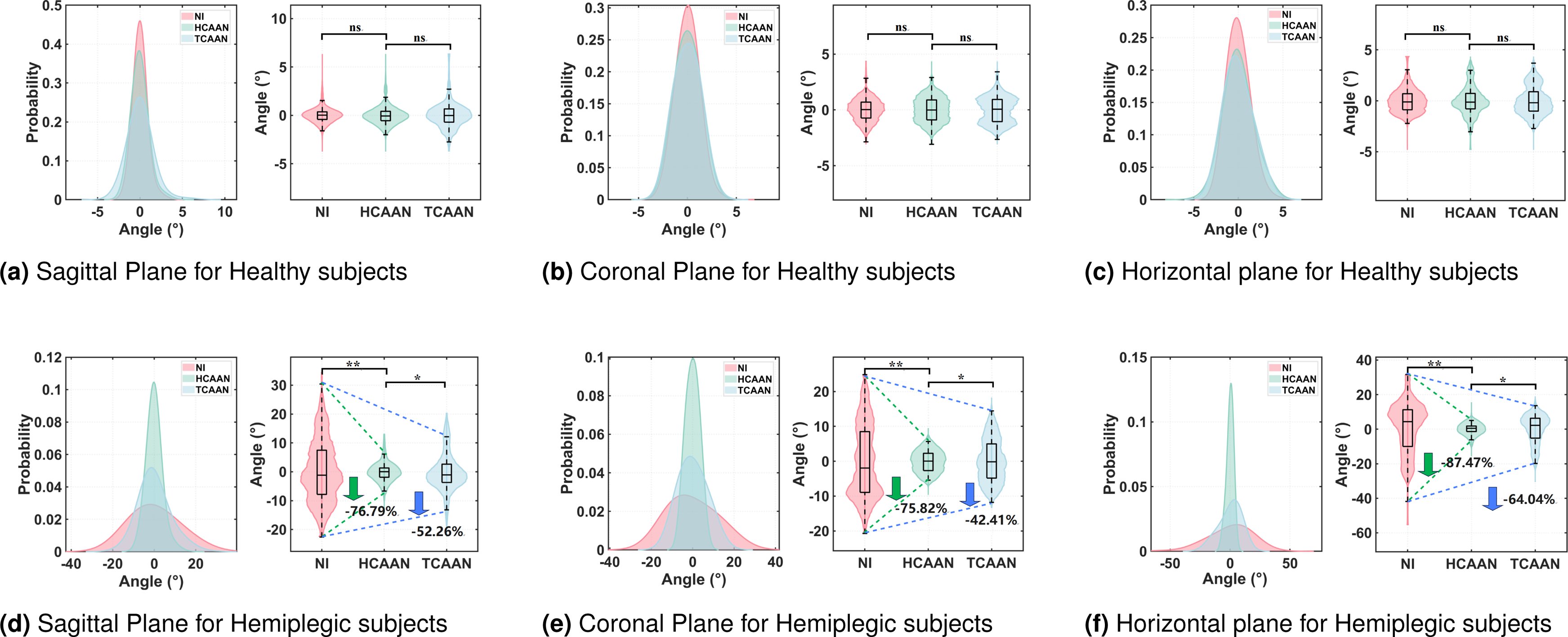
In contrast, under the NI control strategy, the patient group exhibited a broader unimodal distribution across the three anatomical planes (Figure 8(d)-(f)). While the overall distribution remained unimodal, the median on the sagittal plane was -1.2°, with an IF of [-22.6°, 30.4°]; the median on the coronal plane was -3.8°, with an IF of [-20.7°, 24.8°]; and the median on the horizontal plane was 4.7°, with an IF of [-41.8°, 31.6°]. These findings suggest that hemiplegic patients demonstrate significant trunk compensation across the three anatomical planes. Under the assistive torque of the HCAAN strategy, the changes in the three anatomical planes within the healthy group were not significant (p>0.05); however, the peak probabilities across these planes decreased in comparison to the NI strategy. Similarly, under the assistive torque of the TCAAN strategy, the changes in the three anatomical planes of the healthy group were also not significant (p>0.05), with peak probabilities across these planes decreasing relative to the HCAAN strategy.
In the hemiplegia group, the HCAAN strategy showed a tendency for the median to approach 0 degrees across all three anatomical planes when compared to the NI strategy. Furthermore, the compensatory angles of the trunk were significantly reduced in all three planes (p < 0.01). In the sagittal plane, the IF decreased to [-6.2, 6.1] degrees, representing a reduction of 76.79%; in the coronal plane, the IF decreased to [-5.4, 5.6] degrees, reflecting a reduction of 75.82%; and in the horizontal plane, the IF decreased to [-4.9, 5] degrees, indicating a reduction of 87.47%. These findings suggest that the HCAAN strategy effectively reduced the compensatory angles of the trunk in hemiplegic patients and decreased their variability. The TCAAN strategy also significantly reduced trunk compensation angles across the three anatomical planes (p < 0.05), although the probability distribution of the compensation angles at 0 degrees was lower than that observed with the HCAAN strategy. When compared to the NI strategy, the IF in the sagittal plane decreased by 52.26%, in the coronal plane by 42.41%, and in the horizontal plane by 64.04%. Overall, the HCAAN strategy was more effective in reducing trunk compensation angles than the TCAAN strategy and aligned the distribution characteristics of trunk compensation angles in the patient group more closely with those of the healthy group.
Intention Consistency under NI, HCAAN and TCAAN
Figure 9 illustrates the IC values for both the healthy group and the patient group across three different control strategies. IC reflects the proportion of the influence that the subject’s exertion of active force has on the motion trajectory. Under the NI, the median IC for the healthy group was 0.91, while that for the patient group was 0.90, showing no significant difference between the two. This suggests that, in non-intervention conditions, there is a strong correlation between movement acceleration and the actual torque applied in both groups. Under TCAAN, a more pronounced decrease in IC was noted in the patient group, with an average reduction of 43.63% and a median of 0.51. When HCAAN was implemented, the IC of the patient group decreased further, with subjects exhibiting a reduction of 24.81% and a median of 0.68. Compared to TCAAN, HCAAN increased the IC value by 31.91%, indicating that HCAAN is more effective in enhancing the IC value in the patient group. Statistical Graphs of Intent Consistency (IC) in Healthy and Hemiplegic participants.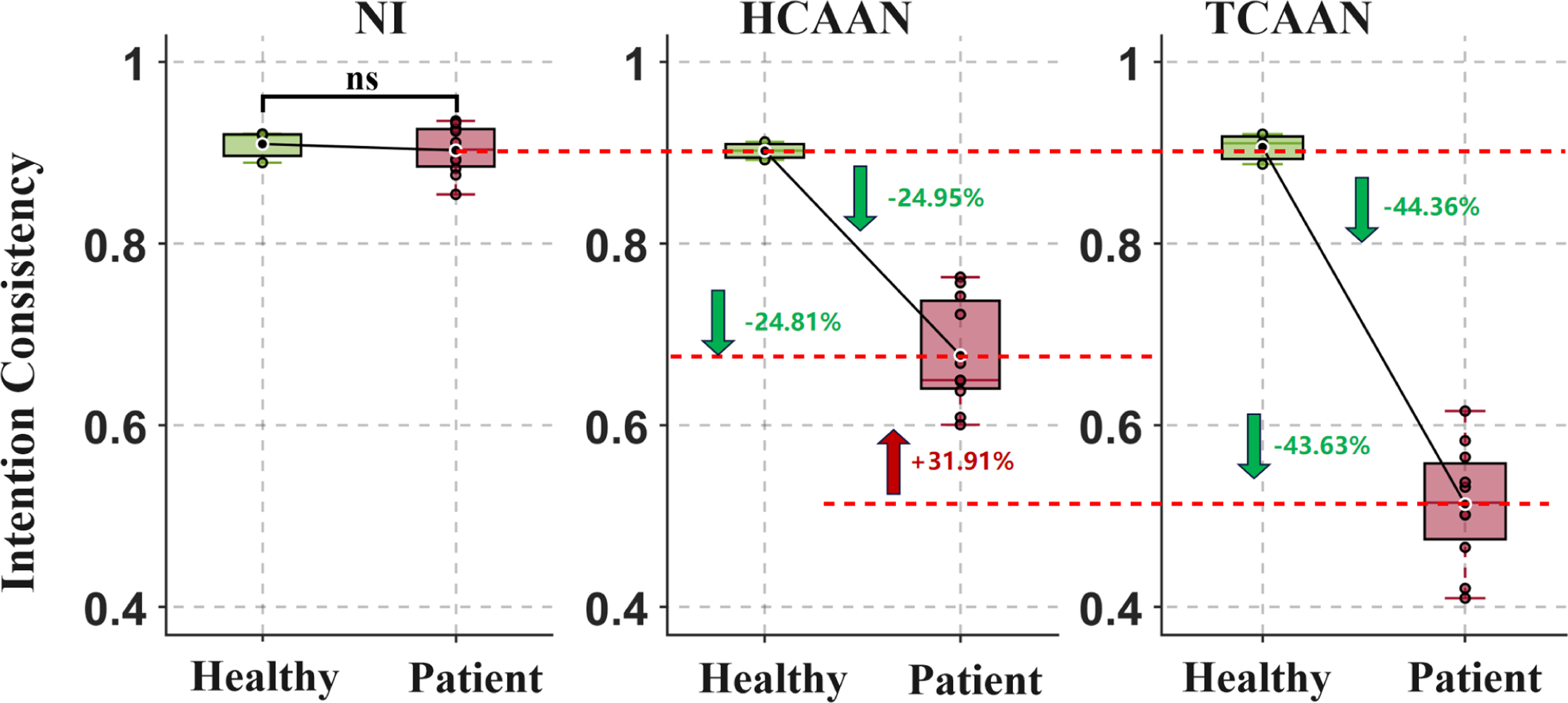
Average torque under NI, HCAAN and TCAAN
Figure 10 illustrates the AT of both the healthy group and the patient group across three distinct control modes. Under the NI mode, the median average torque for the healthy group was 12.8 Nm, whereas for the patient group, it was 5.7 Nm. In the absence of intervention, the overall torque magnitude of the patient group was 55.41% lower than that of the healthy group. Under the HCAAN mode, the median torque for the patient group was recorded at 4.86 Nm, reflecting a 15.01% decrease compared to the NI mode. Under the TCAAN mode, the median torque decreased to 3.29 Nm, indicating a 42.58% reduction in AT for the patient group relative to the NI mode. In comparison to the TCAAN mode, the AT of the patients increased by 48.02% under the HCAAN mode. Statistical Graphs of Average Torque (AT) in Healthy and Hemiplegic participants.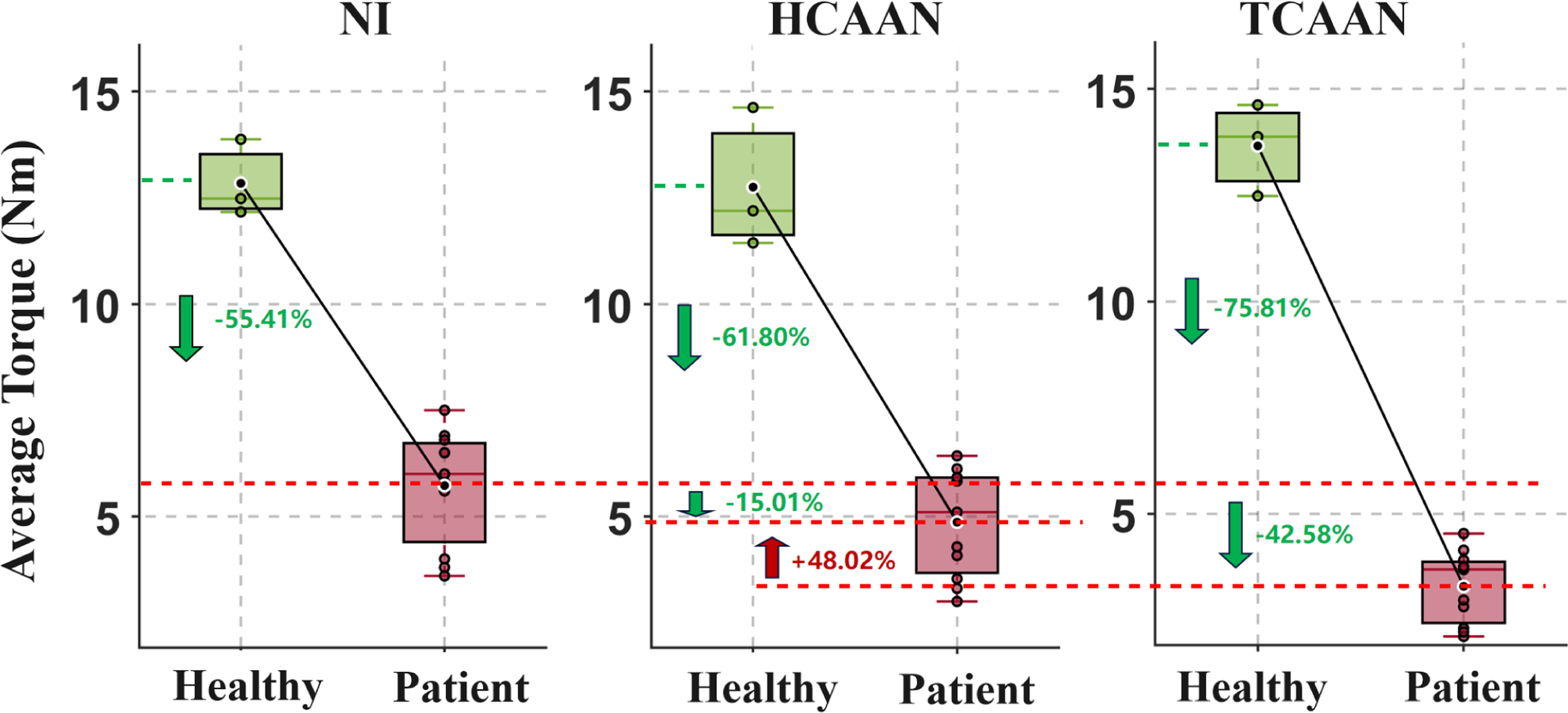
Rehabilitation training scores under NI, HCAAN and TCAAN
The healthy group achieved a score of 42 points in rehabilitation training across all three control modes (NI, HCAAN, TCAAN). The patient group scored between 35 and 42 points in the NI mode. Under the TCAAN mode, hemiplegic patients scored between 40 and 42 points. Under the HCAAN mode, all hemiplegic patients reached the same maximum score as the healthy group, which was 42 points.
Discussion
This study aims to explore effective methods for suppressing trunk compensation during rehabilitation training. Through clinical experiments, we have found that human-centered control strategies can significantly reduce compensation and, compared to traditional torque control methods, can effectively minimize excessive intervention in patient training. To our knowledge, this is the first instance in which a deep learning approach has been utilized to predict both the angle of trunk compensation and the magnitude of torque resulting from it. Based on these, the suppression of trunk compensation in patients is achieved through multilayer control with assist-as-needed strategy. Babak Taati et al. utilized a camera-based system for real-time detection of compensation through a multi-class classifier, achieving an accuracy of 86% among healthy participants. 48 Classifiers based on pressure distribution data can exceed 95% accuracy, 30 and our prediction model for trunk compensation angle achieved an R2 of 0.99. These results validate that our method can effectively identify and predict the angle of trunk compensation, and it can be further applied in rehabilitation robots to provide timely assistance in suppressing trunk compensation for stroke patients.
These results validate that our method can effectively identify and predict the angle of trunk compensation. According to the ’learned bad-use’ theory (Ref 7), suppressing these compensatory movements is essential for forcing the patient to engage the affected limb’s motor pathways. By significantly reducing compensation variability compared to the NI group, the HCAAN strategy creates the necessary kinematic environment for neuroplasticity-driven functional recovery, which is a prerequisite for long-term clinical improvements in FMA and ADL scores.
Previous studies have indicated that visual or auditory feedback can alert stroke patients to the presence of compensatory trunk movements, thereby assisting them in adjusting their movement patterns to counteract such compensations24,49. Tactile feedback can also directly intervene in the physical actions of stroke patients, alerting them to the occurrence of compensatory issues. Bulmaro Adolfo Valdes et al. investigated whether tactile feedback could reduce compensatory trunk movements and examined which type of feedback, 50 tactile or visual, was more effective in reducing compensations.
Results evaluation involved comparing baseline data and post-measurement data across three anatomical planes, followed by the calculation of the percentage change. The calculation formula is as follows:
Inhibition performance of trunk compensation under different methods.
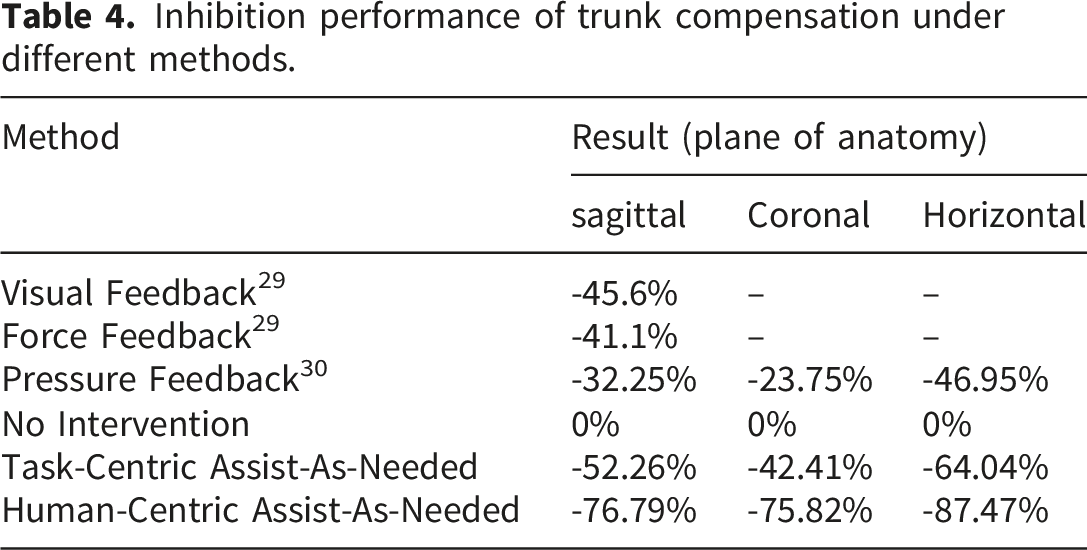
However, the additional torque intervention does not yield better auxiliary effects than visual or auditory cues, indicating that the applied torque is not effectively converted into auxiliary torque for patients to complete tasks. Instead, similar to visual or auditory cues, it merely serves as a reminder for the patients. Previous studies on force feedback36,37 have primarily concentrated on suppressing trunk compensation after it has occurred in patients. At this stage, the consequences of trunk compensation have already manifested, rendering such delayed intervention methods less effective in inhibiting patients. To ensure that the applied torque can effectively assist patients in completing tasks, we designed the Trunk Compensation Torque Calculation Model, which accurately calculates the appropriate torque value (R2=0.97). Combined with the developed multi-layer control strategy, HCAAN significantly suppressed trunk compensation angles (p< 0.01) by 76.79%, 75.82%, and 87.47% in the sagittal, coronal, and horizontal planes, respectively, compared to the NI mode.
The effectiveness of HCAAN in achieving excellent inhibitory effects can be attributed to two primary factors. On one hand, there is a certain delay in the process from when tactile torque feedback or visual and auditory feedback act on the human body to when the patient makes a decision. Moreover, such feedback is often provided after trunk compensation has already occurred, which further reduces the inhibitory effect on trunk compensation. On the other hand, in the process of inhibiting trunk compensation, in addition to providing assistive force, it is also necessary to consider the timing and magnitude of the torque provided. Specifically, HCAAN can provide corresponding assistive torque in advance and according to the patient’s own characteristics before trunk compensation occurs. This proactive assistance allows the patient to perceive their shoulder strength reserve as more adequate, thereby reducing the necessity for the body to engage trunk compensation to supplement torque for task completion. Additionally, the torque magnitude is personalized based on the patient’s condition, ensuring that the intervention process is smoother and more natural while minimizing excessive interference with the patient’s training.
Due to factors such as friction caused by the assembly of the mechanism, the IC correlation coefficient of the patient’s torque and motion acceleration in the NI mode without external intervention is slightly below 1. It is noteworthy that under the control of HCAAN, IC is 31.91% higher than that of TCAAN. This indicates that the TCAAN assistance strategy excessively influences patient training, and causes a misalignment between the direction of the assistance force and the patient’s intended direction. Consequently, this results in a lower IC value. In contrast, HCAAN can predict the patient’s movement intent in advance, ensuring that the direction and timing of the intervention align effectively with the patient’s intentions. Furthermore, as illustrated in the average torque variation graph, TCAAN exhibits the lowest torque among the three modes. This deficiency arises because TCAAN does not assess the patient’s motor ability, resulting in a mismatch between the assistance force provided and the subject’s active intentions. Additionally, the calculation of torque is task-based rather than individualized to the patient, leading to excessive assistance torque that causes patient dependency. In contrast, HCAAN provides the assistance force generated based on the subject’s characteristics. On one hand, it can avoid providing assistance torque when the patient does not need it, and on the other hand, it can prevent providing excessive torque when the patient requires assistance. Therefore, the average torque of subjects under the HCAAN mode is increased by 48.02% compared to TCAAN. These aspects demonstrate that the HCAAN mode can effectively convert torque into assistance for patients, rather than merely serving as feedback, thereby further validating the clinical significance of the human-centric control strategy.
This study is the first to investigate the optimal timing and minimal assistance force required to suppress trunk compensation during upper-limb rehabilitation. Furthermore, clinical experiments validated the feasibility of the proposed HCAAN control strategy in inhibiting trunk compensation. Notably, real-time monitoring and prediction of compensatory movements, combined with personalized assistance torque, significantly reduced trunk compensation in stroke patients during robotic rehabilitation.
The integration of the HCAAN strategy into real-world rehabilitation workflows offers several transformative advantages. Currently, managing trunk compensation in clinics relies heavily on physical constraints (such as belts) or constant manual correction by therapists—both of which are limited by patient discomfort and high labor intensity. Our strategy facilitates a shift toward automated supervision. In a typical clinical session, the robot provides autonomous, high-fidelity monitoring and inhibitory force, ensuring patients maintain correct posture without constant human intervention. This significantly reduces the physical and cognitive burden on therapists, potentially increasing clinical throughput by evolving one-on-one supervision into multi-patient oversight.
Despite these encouraging results, several limitations should be acknowledged. First, the present study involved a relatively small sample size (n = 11 stroke patients), and therefore the current results should be interpreted as a preliminary clinical validation of the proposed HCAAN framework rather than a large-scale efficacy study. This limitation may restrict the generalizability of the findings. Future research will include a larger and more diverse cohort to further strengthen the conclusions.
In addition, the stroke cohort was clinically heterogeneous in terms of impairment severity and time since stroke, as reflected by the variability in FMA scores and post-stroke duration. Because the primary aim of this study was to validate the feasibility of the proposed HCAAN framework, stratified subgroup analysis was not performed. Moreover, the proposed prediction models were trained in a subject-specific manner and are therefore not directly transferable across patients. This design choice was adopted in the present proof-of-concept study to better capture individual trunk compensation patterns and to provide personalized feedforward assistance within the HCAAN framework. However, for a new patient, an additional calibration and data collection phase is required before model deployment, which may reduce scalability and increase preparation time in broader clinical applications. Future studies with larger cohorts will therefore not only examine whether the effects of HCAAN differ across impairment levels and recovery stages, but also explore transfer learning or few-shot learning strategies to reduce the amount of subject-specific data required while preserving personalized prediction accuracy and improving clinical scalability.
Conclusion
In conclusion, this study innovatively addresses the issue of trunk compensation in stroke patients during rehabilitation through the HCAAN strategy. Utilizing deep learning, it accurately predicts trunk compensation angles (R2=0.99) and trunk torque (R2=0.97), establishing a multi-layer control model that offers active, personalized assistance torque to patients. This approach results in a significant reduction in trunk compensation (p< 0.01) — 76.79% in the sagittal plane, 75.82% in the coronal plane, and 87.47% in the horizontal plane — surpassing non-intervention modes and traditional feedback methods such as visual, auditory, and tactile cues (41.1-46.9%). Additionally, compared to the TCAAN mode, it enhances the torque output of patients during training by 48.02%. It provides a new approach for inhibiting trunk compensation in rehabilitation training, and future work will focus on improving model generalization across patients, reducing the dependence on subject-specific calibration, and enhancing the clinical scalability of the proposed framework through more efficient and cost-effective deployment strategies.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by the Natural Science Foundation of Guangdong Province (Grant No.2024A1515011190), and the Guangdong S&T Program(Grant No. 2026B0101110003).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.