
Abstract
Background
Low participation rates in randomised controlled trials involving children are almost a universal problem, leading to high cost and low statistical power. Trial, parent/family, child, and physician factors have been reported to influence parental willingness to consent for paediatric trials.
Purpose
To identify modifiable and unmodifiable factors associated with parental consent.
Methods
Demographic and clinical characteristics of children and their families and physician characteristics associated with parental consent were evaluated in a recent randomised placebo-controlled trial of prophylactic antibiotics to prevent recurrent urinary tract infection.
Results
Of 1109 eligible children identified (mean age, 2.0 years), 412 parents (37.2%) consented. On a multivariate analysis, the only modifiable factor associated with consent was request for consent by a member of the research study team rather than by a member of the clinical team (risk ratio (RR) = 1.9, 95% confidence interval (CI): 1.2–2.9). The unmodifiable factors significantly associated with consent were age of the child (≥4 years) (RR = 1.2, 95% CI: 1.1–1.4), presence of vesicoureteric reflux (RR = 1.5, 95% CI: 1.3–1.8), inpatient management of the index infection (RR = 0.8, 95% CI: 0.7–0.9), and multiple (≥4) symptoms at presentation (RR = 1.3, 95% CI: 1.1–1.5).
Limitations
We have reported data from only one of the four participating centres in this trial. Data on non-consenters in other participating centres were not completely collected. Data on characteristics of the recruiting physician were limited. These findings are applicable for those considering a single randomised controlled trial.
Conclusions
Parent, child, and physician factors are associated with consent for trial participation, with most not being modifiable. Having a member of the research study team approach the parent for consent appears to be the only feasible strategy for increasing recruitment to randomised trials in this setting.
Introduction
There is increasing recognition of the need for paediatric t rials by child health professionals and regulatory bodies [1 –3], but the recruitment of participants into clinical trials remains a universal challenge. A survey of published randomised controlled trials in the Lancet and British Medical Journal showed that 60% had either failed to meet or took longer than planned to meet their recruitment target [4]. There is an even higher threshold for consent for children [5]. Trial, parent/family, child, and doctor factors all influence parental willingness to consent for paediatric trials [2,5]. Age, sex, health status, race, and parents’ beliefs play an important role in trial participation [6,7]; parents are more reluctant to enrol younger children, boys, children who are not acutely unwell, and non-white children to trials. Consenting parents generally have less education and less social support and display a greater health-seeking behaviour. Research factors favouring recruitment include non-inferiority trials rather than placebo comparators, because parents prefer any treatment over placebo [8], and pragmatic trials with broad inclusion criteria rather than those with restrictive protocols.
The aim of this study was to examine factors that may be associated with consent to a paediatric randomised controlled trial. By understanding the impact of these factors on parental decision-making, researchers may improve recruitment in paediatric trials.
Methods
Recruitment
The study population included patients from the largest of the four tertiary referring hospitals in Sydney, Australia, who were eligible to take part in a randomised, blinded, placebo-controlled trial designed to determine whether long-term, low-dose antibiotics prevent recurrent urinary tract infection (UTI) in children (Prevention of Recurrent Urinary Tract Infection in Children with Vesicoureteric Reflux and Normal Renal Tracts (PRIVENT) study). Children under the age of 18 years with a symptomatic UTI were eligible to participate; complete details on the methods of this study are published elsewhere [9].
Eligible patients referred by their paediatrician, family physician, urologists, nephrologists, or hospital emergency department (ED) were contacted by the study coordinator to attend the UTI clinic at The Children’s Hospital at Westmead. Patients were not referred to this clinic for clinical care. At the UTI clinic, advice on UTI management and information about the trial were discussed by a physician (who may or may not have been a member of the research study team). The physician whom the referred patients saw at the UTI clinic was chosen by convenience. When a member of the research team was unavailable, the patients were seen by a non-member physician. Informed consent was obtained at the UTI clinic. The research and non-research team members were trained to understand the research study and were well informed to answer study questions. Parental consent was obtained in English; the parent information sheet and consent form were in English. Parents were assisted by an interpreter whenever necessary.
Data collection
The outcome of interest was consent to take part in the randomised controlled trial. Many potential predictive factors were measured. Reasons for non-consenting were obtained with an open-ended question. Parent/family factors included socio-economic status, English spoken at home, number of siblings of candidate child, health-seeking behaviour (based on the child having a regular paediatrician or a family physician), previous hospital visits (ED, inpatient, or outpatient), and travel time from The Children’s Hospital at Westmead. Child factors included age at diagnosis of index UTI, gender, past history of UTI (the index UTI was the child’s first presentation with UTI or the child had recurrent UTI), the presence of renal tract abnormalities on renal ultrasound, scarring on dimercaptosuccinic acid (DMSA), vesicoureteric reflux (VUR), hospitalisation during the index UTI, UTI-related symptoms with the index infection (fever, irritability, convulsion, diarrhoea, poor feeding dysuria, urinary frequency, haematuria, vomiting, abdominal pain, malaise, offensive urine, and incontinence), and additional medications that the child was taking. Physician factors such as the referral source to the trial and the recruiting physician (member or non-member of the research study team) were also collected. Other characteristics of the recruiting physician were not collected.
Information on socio-economic status was collected using the Australian Bureau of Statistics Socio-Economic Indexes for Areas (SEIFA) 2001 [10]. Index of disadvantage scores were applied to each participant based on the postcode data. This index is a continuous score with quartiles used to summarise low income, lower level of education, high unemployment, and low-skilled occupations. It has been standardised to a mean of 1000 and a standard deviation of 100 across all collection districts in Australia, that is, 95% of scores are between 800 and 1200. Lower scores indicate relatively greater disadvantage and higher scores indicate least disadvantage.
Data on renal tract abnormalities were collected from the results of the imaging tests performed at baseline. VUR was graded according to the International Study of Reflux in Children scale for VUR [11] and renal damage graded according to the scale by Goldraich et al. [12]. Higher scores of VUR grade indicate worse renal condition.
Data analysis
Data were analysed using SAS version 9.1. Continuous data (age at diagnosis, travel time from the hospital, time between the index UTI, and attendance to the recruitment clinic l) were categorised. The number of symptoms accompanying the index UTI was initially grouped as 0–1, 2–3, and ≥4. Univariate associations between giving consent and potential predictor variables were examined using chi-squared tests. Those variables with P < 0.25 were entered into a multivariable logistic regression model, except for referral source, which was associated strongly with recruiting physician. Categories with similar adjusted odds ratios were combined, and the least significant terms were eliminated from the model sequentially until only those with P < 0.05 from the likelihood ratio test remained in the model. A log binomial model that included only these terms was then fitted to obtain risk ratios (RRs) instead of odds ratios [13]. Although there were missing data for most variables, there does not appear to be systematic bias. Data on patient demographics and the postcode, which was used to determine the socio-economic status, were obtained from patients’ notes. We included all variables in the initial univariate model and excluded from the final model those variables with values missing for >10% of candidate children.
Approval
The study was approved by the Ethics Committee of The Children’s Hospital at Westmead, and the University of Sydney, Sydney, Australia.
Results
Baseline characteristics
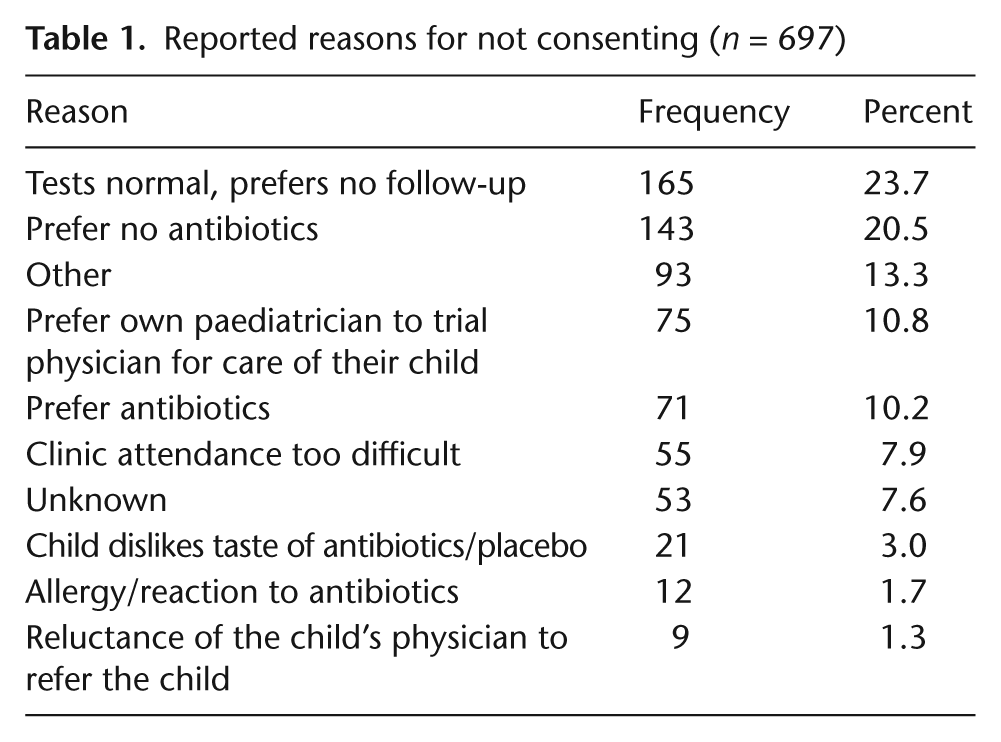
Of 1109 eligible children, the parents of 412 (37%) consented to take part in this study. Table 1 describes the reasons for not consenting. Most frequent reason for non-consent was normal test results (23.7%). These children were eligible to enrol in the trial as they all had a symptomatic UTI proven by a urine culture test. A renal ultrasound, micturating cystourethrogram, and a test to evaluate renal scarring (DMSA) were booked at the discretion of the primary clinician following the UTI and are not a requirement for the study. These kidney tests after the index UTI appeared normal; hence, the parents less often consented to the trial. Children with known sulphur allergy were excluded from the trial before they came to our UTI clinic to discuss the trial. Over a third of the reasons for non-consent were related to antibiotics.
Reported reasons for not consenting (n = 697)
Of candidate children whose parents did not consent, 36% were less than 6 months of age; the majority had experienced only one UTI (93%); VUR was present in 22%; most had a febrile UTI (85%); and 40% received outpatient treatment for the index UTI.
Associated factors suggested by univariate analysis
Parent/family factors
Parents of candidate children with siblings, girls, older candidate children, those who had a regular family physician, and those who spoke English at home were more likely to give consent (Table 2).
Frequency of consent stratified by parent/family, child, and doctor factors

SEIFA: Socio-Economic Indexes for Areas; UTI: urinary tract infection; DMSA: dimercaptosuccinic acid; VUR: vesicoureteric reflux; CI: confidence interval.
Data are missing for this variable.
Child/clinical factors
Parents of children with VUR, abnormality observed in the renal ultrasound, scarring on DMSA or with four or more presenting symptoms with the index UTI, or who had waited ≥4 weeks from the presenting UTI were more likely to consent to the study. Hospitalisation for the UTI reduced the likelihood of providing consent. Unknown VUR, unknown abnormality in the renal ultrasound, and unknown scarring on DMSA were associated with lower likelihood of providing consent.
Physician factors
Referral to the study by a paediatrician or a nephrologist increased the likelihood of providing consent compared to referral from an ED. Consent was more likely when the recruiting physician was a member of the research study team.
Independently associated factors from a multivariate analysis
Table 3 shows the unadjusted RR and adjusted RR (ARR) for those variables that were associated independently with providing consent to the study in the multivariable model. After allowing for the other characteristics, parents of children ≥4 years of age were more likely to consent to participation in this study than parents of younger children (ARR = 1.2). Parents of children who had four or more symptoms with the index UTI were more likely to consent to the study (ARR = 1.3); the presence of VUR increased the likelihood of providing consent by almost 50%. Parents of children who received inpatient care for the index UTI were less likely to consent to this study (ARR = 0.8). Consent was more likely when the recruiting physician was a member of the research study team (RR = 1.9).
Variables independently associated with consent in the multivariable analysis
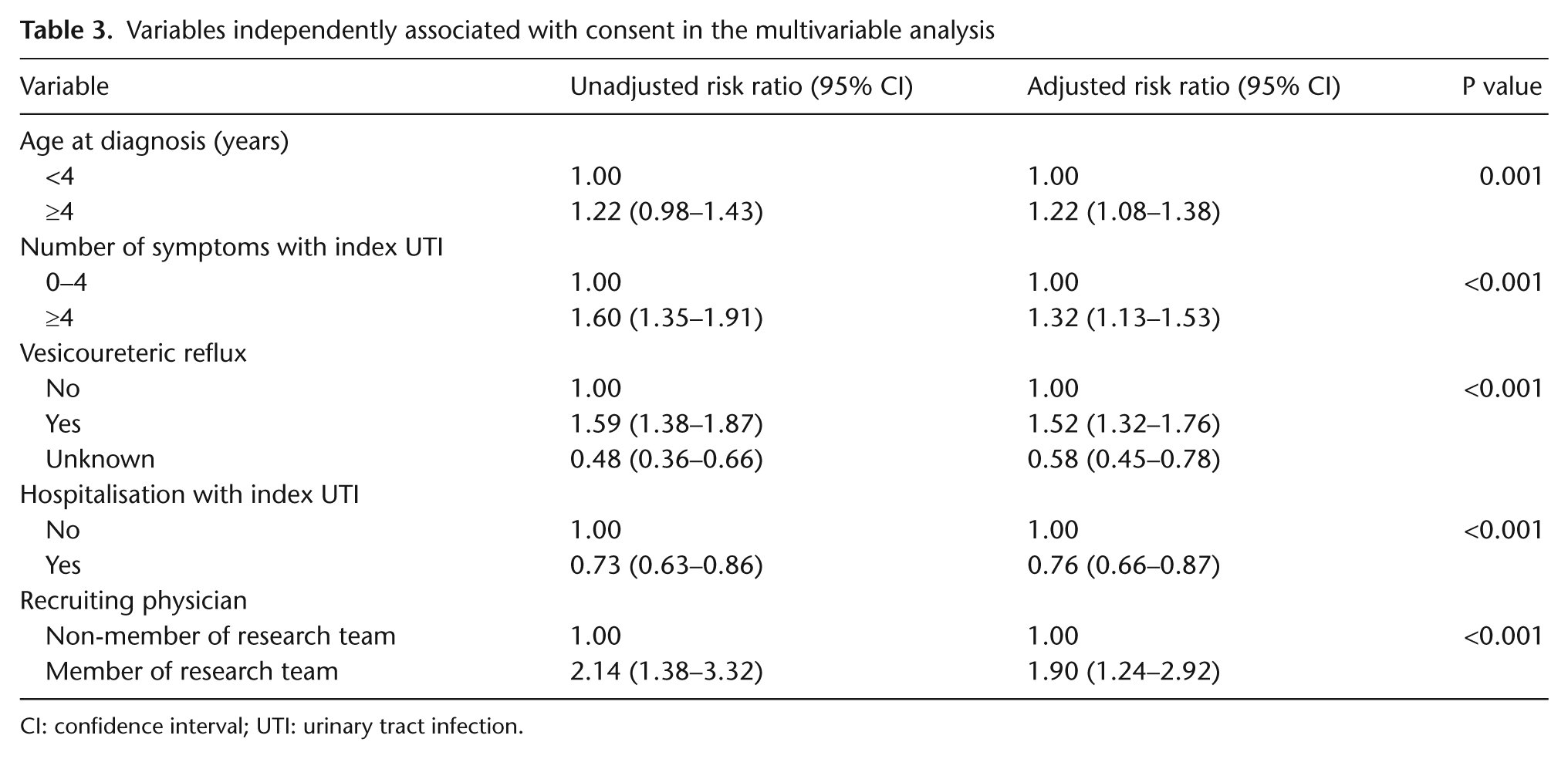
CI: confidence interval; UTI: urinary tract infection.
Discussion
Parents balance benefits and risks when making decisions regarding trial participation for their child [5,7]. Based on our findings from the multivariate analysis, the only independent and statistically significant factors that influenced consent to this trial were child and physician factors. Previous studies have shown that the health status of the child influenced trial participation, although increases or reduces consent by parents [5,14,15]. We were particularly interested in the finding that reflux was related positively to trial consent. At the time of trial conduct, the standard treatment for reflux was prophylactic antibiotics, although the rationale for this treatment had been questioned. Many parents preferred that the child not be placed on prophylactic antibiotics (Table 1), although they may have been fearful of the consequences of defying conventional standard therapy [5]. Participation in the trial provided the opportunity to avoid medication but ensured careful monitoring of the child during the trial period. An advantage of trial participation previously reported was the perception by parents of better care and monitoring of their children within a clinical trial [5]. A higher number of presenting symptoms was also associated with parental consent, consistent with the known association between increased consent and the perception of increased disease severity [5,16]. In contrast, higher grade VUR (compared with lower grade VUR) and hospitalisation for the index UTI were associated with lower likelihood of consent, possibly due to heightened anxiety among parents of children with higher grade VUR and hospitalisation. Parents may have been less to risk not using prophylactic antibiotics as part of the trial. This dichotomy reflects the parental dilemma in making decisions on trial participation when faced with an ill child [5].
The study affiliation of the recruiting physician was associated with consent. This finding confirms the important role physicians play in encouraging trial participation [17,18]. This factor is the only modifiable factor that was found to be associated independently with consent. Other studies of the role of the recruiter demonstrated that the seniority of the recruiter did not affect consent [19,20]. Our comparison was between physician recruiters who were part of the research team (and therefore were more closely identified with the study) compared with those who were not part of the research team, suggesting that commitment and ownership of the recruiter are associated with consent.
In summary, in our study, several child factors were associated independently with consent, but these factors were not modifiable. The only modifiable factor was the trial affiliation of the recruiting physician. Approaching the parent for consent by one of the study investigators rather than an unaffiliated physician may be an important strategy for increasing recruitment of children to randomised trials in this setting. More evidence from a randomised controlled trial will be useful to support our findings.
Limitations
A limitation of this study was that data for some factors were missing for some candidate children. Demographic data were collected routinely by the study coordinator. We did not find that missing data were selective for any particular group; missingness is even across all patient groups. Whenever the data for a particular variable were missing for more than 10% of children, the variable was included only in the univariate analysis and not in the multivariate analysis. The absence of additional data regarding the recruiting physician is an important limitation. Although we have assumed in our interpretation of the findings that study affiliation is the important component, other characteristics, for example, age, gender, and clinical trial experience, may have contributed to this finding. Future investigations of this association should explore these and other characteristics of recruiting physicians.
Conclusion
Consent for trial participation by their child is a complex decision faced by parents of eligible children. Many factors interplay in this decision-making. Some factors such as the status of the child’s health and approaching the parent for consent by a physician who is affiliated with the research team clearly are associated with the decision, while other factors such as parental factors have a less certain role. Our finding is that the only modifiable factors to improve recruitment to trials in this setting are related to the extent of involvement in the trial of the recruiting physicians. This finding may not be generalisable to other diseases or other study design but is worth exploring further, perhaps in a randomised controlled trial.
Footnotes
Acknowledgements
The authors acknowledge the Prevention of Recurrent Urinary Tract Infection in Children with Vesicoureteric Reflux and Normal Renal Tracts (PRIVENT) study investigators.
Trial registration number: 12608000470392 (Australian New Zealand Clinical Trials Registry).
Funding
This study was funded by The Financial Markets Foundation for Children, private donation by J.T. Honan of the Manildra Group, and the National Health and Medical Research Council of Australia.
Conflict of interest
The authors declare that there is no conflict of interest.