
Abstract
Background
Latinas with breast cancer suffer symptom and psychosocial health disparities. Effective interventions have not been developed for or tested in this population.
Purpose
We describe community-based participatory research methods used to develop and implement the Nuevo Amanecer program, a culturally tailored, peer-delivered cognitive-behavioral stress management intervention for low-income Spanish-speaking Latinas with breast cancer, and unique considerations in implementing a randomized controlled trial to test the program in community settings.
Methods
We applied an implementation science framework to delineate the methodological phases used to develop and implement the Nuevo Amanecer program and trial, emphasizing community engagement processes.
Results
In phase 1, we established project infrastructure: academic and community co-principal investigators, community partners, community advisory board, steering committee, and funding. In phase 2, we identified three program inputs: formative research, a community best-practices model, and an evidence-based intervention tested in non-Latinas. In phase 3, we created the new program by integrating and adapting intervention components from the three sources, making adaptations to accommodate low literacy, Spanish language, cultural factors, community context, and population needs. In phase 4, we built community capacity for the program and trial by training field staff (recruiters and interventionists embedded in community sites), compensating field staff, and creating a system for identifying potential participants. In phase 5, we implemented and monitored the program and trial. Engaging community partners in all phases has resulted in a new, culturally tailored program that is suitable for newly diagnosed Latinas with breast cancer and a trial that is acceptable and supported by community and clinical partners.
Lessons learned
Engagement of community-based organizations and cancer survivors as research partners and hiring recruiters and interventionists from the community were critical to successful implementation in community settings. Having culturally and linguistically competent research staff with excellent interpersonal skills facilitated implementation. Facilitating and maintaining excellent communication among community partners was imperative to troubleshoot implementation issues. Randomization was challenging due to community concerns about assigning women to a control group. Patient privacy regulations and the need for extensive outreach to establish relationships between community partners and clinical sites hampered initial recruitment.
Limitations
These were resource-intensive processes to develop and implement the program that need to be compared to less-intensive alternatives.
Conclusion
Engaging community members in design and implementation of community-based programs and trials enhances cultural appropriateness and congruence with the community context. If the randomized trial demonstrates that the intervention is effective, it will fill a gap in evidence-based programs to address ethnic disparities in quality of life among Spanish-speaking Latinas with breast cancer.
Background
Breast cancer is the most common cancer and leading cause of cancer death among Latinas [1]. Latinas are diagnosed with more advanced breast cancer [2–4]; after controlling for health insurance, age, stage, and treatment, they experience worse overall and breast cancer–specific survival compared to White women [5,6].
Latinas with breast cancer, especially Spanish speakers, suffer worse health-related quality of life (HRQOL) and more post-surgical pain, body image and partner relationship issues, depressive symptoms, and fatigue compared to whites [7–16]. Spanish-speaking Latinas with breast cancer report greater emotional distress, anxiety, and fears of recurrence than White women [17–19].
Important considerations when designing interventions to address psychosocial health disparities in this population include limited English proficiency and health insurance coverage, unemployment, lack of transportation, and unfamiliarity with the health-care system [20]. Spanish-speaking Latinas with breast cancer are at increased risk of financial hardships, poorer communication with clinicians, and job disruptions [7,11,20,21] and, compared with English-speaking patients, experience greater anxiety because they do not understand their diagnosis and treatment [22,23], are less involved in decision making, and feel less empowered to seek information about treatment options [24,25]. Spanish-speaking patients often report uncertainties about treatment and a need for more information [22,23,26]. A desire to protect their families from the consequences of cancer can intensify their distress, especially when they are unable to fulfill household responsibilities [27].
Psychosocial interventions that employ cognitive-behavioral approaches can reduce distress and improve the HRQOL of breast cancer patients [28]. Cognitive-behavioral interventions improve patients’ self-efficacy, optimistic outlook, and adaptive coping strategies [29,30]. However, they have not been designed for and tested among Spanish-speaking Latinas with breast cancer [31–33]. Employing peer cancer survivors to deliver support could increase access to these services in communities [34,35], especially because Latinas view other Latina survivors as sources of hope and information [23,26]. Peers have been trained to promote cancer screening [36–38] and provide breast cancer treatment decision support [23], but peer-delivered cancer support interventions for Latinas have not been tested rigorously. We are aware of only one small study that tested a psychosocial intervention for Latinas with breast cancer, but it did not differentiate between English- and Spanish-speaking Latinas; the investigators did not find significant quality of life differences between intervention and attention control groups [14].
To address this gap, an academic–community partnership, utilizing community-based participatory research methods, developed a new cognitive-behavioral stress management intervention for Spanish-speaking Latinas newly diagnosed with breast cancer. Nuevo Amanecer (A New Dawn) is an 8-week peer-delivered intervention that integrates an evidence-based stress management program that improved HRQOL among White women with breast cancer [39], a community best-practices model, and formative research to culturally tailor the intervention [26]. We use the term ‘peers’ to refer to Spanish-speaking Latinas with breast cancer. The partnership is conducting a 6-month randomized controlled trial (RCT) to assess the effects of Nuevo Amanecer on HRQOL among Spanish-speaking Latinas in the year following diagnosis, compared to a wait-list control group. We describe the methods and processes used to develop and implement Nuevo Amanecer and to conduct the RCT using a community-based participatory research approach in which community partners were involved in every step of the process.
Methods
Design and implementation of the culturally tailored program and the RCT in communities utilized a framework of methodological phases for implementing and evaluating evidence-based interventions that has been adapted for use in health disparity communities [40,41].
Phase 1: establish infrastructure for project
Academic and community co-principal investigators
The project was directed jointly by an academic co-principal investigator (Co-PI) at the University of California San Francisco and a community Co-PI at Círculo de Vida Cancer Support and Resource Center with project support from their staff members, all of whom were bilingual Latinas. The academic Co-PI is a bilingual–bicultural Mexican-American behavioral epidemiologist. Academic staff consisted of a project director and interviewer. The community Co-PI is Executive Director of Círculo de Vida. She is a bilingual–bicultural Puerto Rican clinical psychologist and breast cancer survivor. Círculo de Vida is a community-based organization (CBO) offering comprehensive cancer support programs for low-income Latinos with cancer and their families. Project staff at Círculo de Vida were a clinical supervisor and three peer counselors.
Community partners
To build infrastructure to enable broad community involvement, we drew from organizations and clinical sites in five California counties (Alameda, Contra Costa, San Francisco, San Mateo, and Santa Clara) that served Spanish-speaking breast cancer patients. The Co-PIs identified 10 CBOs and 6 clinical sites for the project that had staff with experience serving this population and venues for recruiting Latina breast cancer patients. Individuals working or volunteering at these places were identified and screened to be our field staff of recruiters and interventionists (compañeras). We paid CBO and clinical partners a service fee (from US$500 to US$5000, depending on the extent of their involvement).
Community advisory board
Our advisory board comprised Latina cancer survivors, advocates, oncologists, and social service providers, including representatives from the CBO partners. This group had been convening on a yearly basis as an advisory group to the academic partner to guide outreach, education, and research activities.
Steering committee
This committee constituted the main governing body of the project and consisted of the Co-PIs, project director, and study field staff (recruiters and compañeras). The committee maintained regular contact through emails, telephone calls, and monthly teleconferences. These calls were important to review progress, announce events, extend mutual support, discuss ways to address challenges, and suggest future research topics. With community advisory board (CAB) advice, the Co-PIs wrote the grant application that was funded by a California Breast Cancer Research Program Community Research Collaboration Award. This unique mechanism calls for separate but linked awards to academic and community Co-PIs.
Phase 2: identify multiple inputs for intervention
We used three sources to design the new program: formative research, a community best-practices program, and an evidence-based intervention for coping with breast cancer developed for non-Latinas.
Formative research
Key informant and focus group interviews were conducted with community advocates and Latina breast cancer survivors, including members of the CAB [26]. Survivors relayed several culturally salient themes, the most prominent being intense fear of dying, strong desire for cancer information, and overwhelming sense of powerlessness. Many expressed a desire to give back by helping other women who might benefit from their experience. Advocates stressed that overcoming cultural factors of humility and deference to health-care professionals required teaching patients self-advocacy and coping skills.
Community best-practices model – Las Angelitas (The Angels)
This Círculo de Vida program was founded on principles of early intervention, familismo (emphasis on the family unit), and personalismo (preference for positive interpersonal relationships). For Las Angelitas, trained Spanish-speaking Latina breast cancer survivors (peers) provide culturally tailored one-to-one support to newly diagnosed clients.
Evidence-based program – New Directions
A literature review identified evidence-based programs that had improved HRQOL among White women (at the time, none had been tested with Latinas). We selected New Directions because it focused on coping skills training to build self-efficacy for managing cancer [39]. In a group setting, a cancer center clinical psychologist taught skills related to restructuring negative thoughts, relaxation, and assertive communication. The program manual was obtained and the investigator served as a consultant to the project.
Phase 3: integrate and adapt intervention components
The Co-PIs and staff reviewed, adapted, and synthesized the formative research results, Las Angelitas, and New Directions to create Nuevo Amanecer. Components were selected that could be integrated and adapted for a good fit to low-income Latinas and the community context and delivery by peers. Formative research led to selection of a delivery mode where peers provide one-to-one support in patients’ homes to address issues of limited transportation, lack of trust, lack of culturally and linguistically appropriate services, financial hardship, lack of child care, and preferences for in-person support. Based on formative work, we created new content on cancer information, assertive communication with family members and health-care professionals, and spiritual factors. Aspects of Las Angelitas that were selected were early intervention, a shared breast cancer experience with the interventionist, familismo, and personalismo. New Directions components that were retained included goal setting, communication skills, cognitive reframing skills, and stress management.
Drafts of participant and interventionist manuals were developed initially in English by the Co-PIs and staff who had extensive relevant experience. The manuals then were translated rigorously into Spanish (sixth-grade level) by research team members. Drafts were reviewed by steering committee and CAB members for cultural and linguistic appropriateness.
Adaptations to accommodate low literacy included translation into simple Spanish, simplification of exercises and homework, and simplification of stress management and cognitive reframing concepts. Graphics supported written text. Adaptations to address community contextual factors included selecting recruiters and interventionists from the partner CBO and clinical sites that were embedded in and served the local Latino communities. Adaptations to address needs among Spanish-speaking Latinas included provision of comprehensible cancer information, emotional support, and coping skills training. Critically, for vulnerable populations, coping skills training may reduce the impact of stressful environments and engender a sense of control. We provided a list of community resources to assist with common financial and social hardships.
The final Nuevo Amanecer program is an individualized Spanish-language 8-week intervention that emphasizes cognitive-behavioral coping skills to manage stress and emotions. It includes emotional support, informational resources, training in self-care behaviors, and modeling provided by compañeras using a structured program manual (Table 1).
Contents of the Nuevo Amanecer program: a cognitive-behavioral stress management intervention for Spanish-speaking Latinas with breast cancer
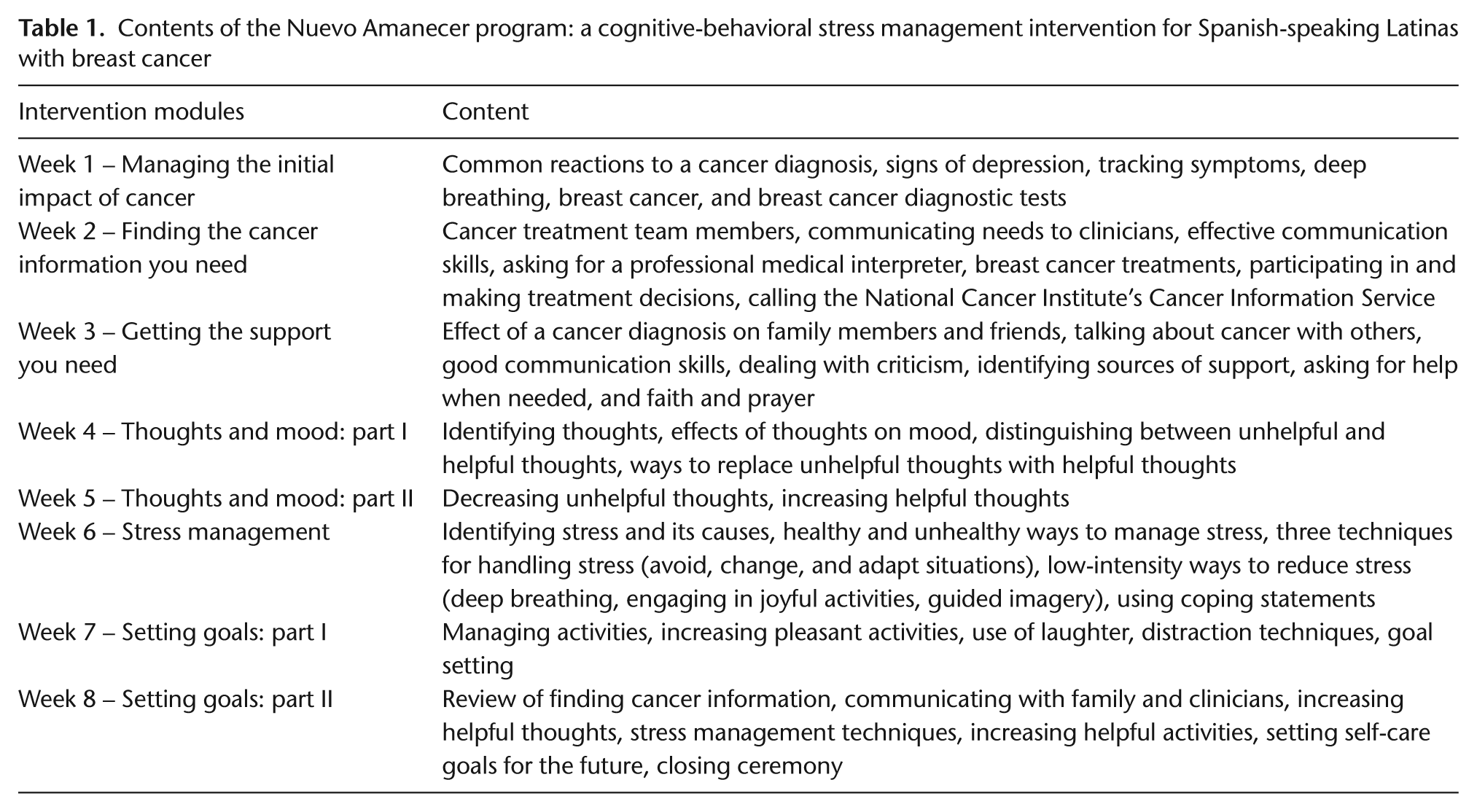
Each of the 8-week sessions includes an overview, a review of the prior session, content for that week, interactive activities, time for participants to restate the main concepts in their own words, homework, and a session recap. For example, in the cognitive restructuring session, ‘Thoughts and Mood: Part II’, using compañera and participant manuals, the compañera teaches participants to recognize ‘helpful’ thoughts to reduce stress and ‘unhelpful’ thoughts that increase stress by reviewing examples of each and then having the participant generate her own examples. Through a series of interactive exercises, the compañera assists the participant in replacing unhelpful thoughts with helpful ones. For example, ‘I will never feel better’, can be replaced with ‘I’m doing all I can to help myself feel better’. For homework, participants identify several more unhelpful thoughts and replace them with helpful ones. Homework is reviewed the following week. For participants who do not read or write, the compañera reads aloud the material and completes the homework with the participant during the session.
Phase 4: build community capacity for program and RCT
Select and train compañeras (interventionists)
CBO leadership identified candidates. Compañera requirements were bilingual or Spanish monolingual Latina breast cancer survivor and at least 2 years post-diagnosis with no recurrence. The community Co-PI screened candidates using a structured interview protocol. As breast cancer survivors, they serve as role models who inspire hope which helps address fatalistic responses to a cancer diagnosis. Compañeras needed to display warmth and compassion to create a strong sense of familismo (familial interconnectedness) and confianza (trust). Sensitivity to spirituality was important as Latinas often use faith as a source of support, meaning, and acceptance of cancer.
Compañeras participated in three 8-h training sessions that utilized role playing and demonstrations and were conducted in Spanish by the Co-PIs and their staff. The training covered psychosocial issues among Latinas with breast cancer, the theoretical basis of Nuevo Amanecer, communication skills, cognitive-behavioral stress management skills, breast cancer and its treatment, and local community resources. Compañeras were provided with a step-by-step Spanish-language manual covering the 8-week program sessions. Compañeras were compensated for attending training and received a certificate of completion. They received a 4-h refresher course 10 months later for which they were compensated. The community Co-PI accompanied the compañeras on their initial intervention sessions until she was satisfied they were delivering the intervention as intended; she provided ongoing supervision.
Select and train recruiters of trial participants
Recruiters were identified by CBO or clinical site leadership. Recruiters had to be bilingual Latinas, have prior health education or outreach experience, and have access to newly diagnosed Latina breast cancer patients, for example, through their health education or patient navigation activities. The academic Co-PI and project director screened candidates using a structured interview protocol that assessed their interpersonal communication skills, relevant experience, and outreach skills.
Recruiters participated in a 4-h training session, which prepared them to recruit, enroll, and randomize trial participants and to conduct baseline assessments. They completed human subject’s protection training on the Collaborative Institutional Training Initiative website. Recruiters were compensated for completing the training. The project director accompanied recruiters on their initial enrollments to assure the study protocol was followed; she provided ongoing supervision.
Compensate personnel and CBOs
Once in the field, monetary compensation of recruiters and compañeras was handled according to CBOs’ preferences. In some cases, CBOs treated recruitment and compañera duties as part of the person’s employment, in which case the CBO was remunerated. In other cases, the CBO preferred that each person be compensated directly as an independent contractor. These arrangements were specified in advance in a memorandum of understanding between the CBO and the academic and community Co-PIs.
Identify potentially eligible patients for the randomized trial
One recruiter was a medical assistant employed by one of the clinical sites; the others were patient navigators at the clinical sites who were employed by a CBO partner. Recruiters verified eligibility of potential participants either through review of medical records or confirmation by medical staff (medical assistants, nurses, patient navigators, and social workers) at the clinical sites. For the few cases that were identified through community outreach, eligibility initially was established by self-report with final confirmation by medical records review.
Phase 5: evaluate the intervention in a randomized trial
Design RCT
We employed a RCT design to compare the Nuevo Amanecer intervention group to a wait-list usual care control group with respect to breast cancer-specific quality of life. After obtaining informed consent and completing the baseline interview, women were randomized by the study recruiter to the intervention or control group. Control group participants are offered the intervention after the 6-month assessment. Because evidence on the effectiveness of these types of interventions among Latinas is scant, assessing the benefits of adding psychosocial interventions to routine clinical care is appropriate and necessary. The individual is the unit of randomization. Randomization is stratified by recruitment site to achieve between-group comparability on unmeasured factors associated with the outcomes that may differ by site. The academic partner’s Institutional Review Board approved the protocol, and written informed consent was obtained from participants.
The RCT population consists of Spanish-speaking Latinas with breast cancer. Inclusion criteria are (1) ≤1 year since diagnosis with Stage 0 to IIIC primary breast cancer; (2) living in Alameda, Contra Costa, San Francisco, San Mateo, or Santa Clara counties; (3) primarily Spanish speaking or Spanish monolingual; and (4) self-identifies as Latina. Exclusion criteria are (1) previous cancer diagnosis except for non-melanoma skin cancer, (2) terminal illness, or (3) Stage IV breast cancer (distant metastasis).
We hypothesize that the Nuevo Amanecer intervention, which employs emotional support, informational resources, training in self-care behaviors, modeling, and coaching provided by compañeras, results in greater cancer coping self-efficacy, use of positive cancer coping skills, and perceived social support, which improve HRQOL significantly more than that of women in the wait-list control group. Primary outcomes are the total score from the Functional Assessment of Cancer Therapy–Breast Quality of Life Instrument and its five subscale scores [42]. Assessments occur at baseline (60-min in-person survey) and 3 and 6 months after randomization (30-min telephone surveys) to collect data on descriptive, hypothesized mediating, and outcome variables. Women are paid US$30 per assessment completed.
Target enrollment is 170 participants. Sample size estimates assumed 80% power, two-tailed alpha equal to 0.05, 3- and 6-month follow-up assessments with 80% retention at 6 months, and intention-to-treat analysis. The primary group comparison will focus on HRQOL total score outcomes. Group-by-linear interaction (baseline and 3 and 6 months) and time-averaged group comparisons (3 and 6 months) will be tested using linear mixed models.
Establish a steady number of monthly enrollments
In addition to fortifying relationships between the recruiters and medical staff at the clinics, 9 months after recruitment started, we expanded our eligibility window from 3 to 12 months post-diagnosis. This change was made to address difficulties in identifying women immediately after diagnosis due to the overburdened nature of public hospitals, patients’ demanding treatment regimens, and providers’ concerns about patient privacy. Several recruiters were granted access to patients by signing memoranda of understanding between the CBOs and health-care providers that stipulated strict adherence to patient privacy requirements. Other efforts included distributing flyers and letters to clinical providers with testimonials from study participants, radio announcements, outreach, and health education talks at community events.
Maximize retention
We used standard retention methods including requesting mobile phone numbers and alternate contacts, telephone, and mail reminders regarding scheduled assessments, reiterating the value of trial participation, and cash incentives. When a mobile phone number was disconnected, we would call 2 weeks later, at which time service often had been reinstated. Excellent communication between the project director and recruiters, compañeras, and telephone interviewer often led to reestablishing contact with difficult to reach participants.
Monitor recruitment, retention, and intervention delivery
Monthly targeted and actual recruitment were tracked by the project director and reviewed by steering committee members during monthly teleconferences. Recruitment results by county and recruiter were distributed in advance to facilitate troubleshooting. Compañeras’ active cases were reviewed during the calls to obtain suggestions for intervention delivery.
Monitor fidelity
We tracked several measures of fidelity, defined as the adequacy of delivering the intervention as designed. Compañeras tracked the date, mode, duration, nature, and outcome of each call or visit using structured tracking forms and collected weekly homework. The community Co-PI randomly selected two sessions for each compañera which she observed and audio-recorded. She rated sessions using a structured rating scale that assessed the extent to which compañeras accurately delivered the intervention. Two independent observers listened to and rated audiotaped sessions using the same rating scale.
Lessons learned
Dedicate ample resources to infrastructure development
Initially, we overestimated the extent to which the CBO partners had established relationships with clinical providers. Once we realized that several CBO partners needed help, the academic Co-PI and staff focused intensive efforts on developing relationships between medical staff and recruiters from the CBOs using flyers, one-to-one meetings, mailings, emails, and telephone calls. In several cases, the effort invested in establishing relationships with medical staff was unproductive due to staff turnover. In three clinical sites, we waited months for medical staff positions (e.g., oncology social worker) to be filled and then had to establish rapport with new staff. Thus, we underestimated the time and effort to recruit patients. It took over a year to establish firm relationships in our five-county area and to achieve a stable stream of referrals. Organizational and service fees for CBO and clinical partners were critical to secure their continued collaboration.
Formation of a strong project steering committee and CAB composed of community and academic partners who brought with them a tremendous amount of experience was critical to overcome recruitment and program delivery challenges. The steering committee made decisions on day-to-day operations by consensus. The CAB provided detailed input on funding initiatives, intervention content, and recruitment. By actively engaging partners who are extremely dedicated and active in community cancer control efforts, our reach was multiplied in ways that are difficult to measure. With few exceptions, study partners, including project leadership, were bilingual or Spanish monolingual Latinas, which helped to establish project credibility and relevance among community members at large.
Facilitate open and honest communication
The academic–community partnership facilitated negotiating important tradeoffs between internal and external validity while maximizing program adoption. Negotiations required excellent and respectful communication by partners. For example, everyone on the study team had difficulty accepting randomization when they saw women’s distress. However, through frank discussions, consensus was reached that a wait-list control group was an acceptable compromise as it allowed for stronger evidence of the program’s effectiveness and provided full access to the intervention at a later date. Because of these early and frank discussions among staff, recruiters were able to discuss randomization with potential participants openly and effectively; only one woman refused participation because we could not guarantee assignment to the immediate intervention group. Thus, randomization has not interfered with meeting recruitment goals and retention has been similar for intervention and control groups.
Another issue discussed in detail was that in real-world settings, we could not prevent women from accessing other cancer support services in their communities. Although access to other services pose a potential threat to internal validity and may dilute the effect of the Nuevo Amanecer intervention, to steer women away from these other services was unacceptable to the team.
Be willing to go the extra mile
Powerful aids to effective recruitment and retention have been the excellent interpersonal skills of steering committee members and intervention delivery by breast cancer survivors. Steering committee members did a lot to assist participants, for example, helping with translating correspondence, faxing insurance documents, baby sitting while women received radiation, and finding community resources, such as transportation, wigs, or breast prostheses.
Discussion
Our RCT is the first to test a psychosocial intervention developed specifically for Spanish-speaking Latina breast cancer patients. This project, generated and implemented by an academic–community partnership, serves as a model for translating and adapting evidence-based interventions for ethnically diverse communities. Translation was achieved by integrating an evidence-based cognitive-behavioral intervention with community wisdom (a best-practices model and formative research) to create a culturally and linguistically tailored cancer support intervention. If proven effective, the Nuevo Amanecer program will advance our ability to address important informational and psychosocial health disparities of Latina breast cancer patients.
This project brought together a strong coalition of Latina cancer survivors, community advocates, and academic partners that worked together to develop the program and study. Active engagement of community members in the design and implementation of this community-based RCT was essential. Their involvement enhanced cultural appropriateness and congruence with the community context. Training compañeras situated in CBOs and using peer support enhanced the likelihood of sustainability and usefulness to other CBOs. Our experiences should help investigators anticipate and offset problems conducting similar studies in community settings to reach disparity populations.
Footnotes
Acknowledgements
We are grateful for the support and commitment of the community advisory board and the referring agencies and health-care providers. We are indebted to the staff at the following organizations and institutions: Alameda County Medical Center, Breast Cancer Connections, Círculo de Vida Cancer Support and Resource Center, Contra Costa Regional Medical Center, John Muir Medical Center, Latinas Contra Cancer, San Francisco General Hospital, San Mateo Medical Center, Santa Clara Valley Medical Center, Shanti, and Women’s Cancer Resource Center. Finally, we are extremely grateful to the Latinas living with breast cancer who shared their lives with us, making this study possible. Que Dios las guarde.
Funding
This research was supported by funds from the California Breast Cancer Research Grants Program Office of the University of California grant numbers 15BB-1300 and 15BB-1301, grant number 1U54CA153511 from the National Cancer Institute, and grant number 1 P30 AG15272 from the National Institute on Aging.
Conflict of interest
None declared.