
Abstract
Background/Aims
Essential to bringing innovative cancer treatments to patients is voluntary participation in clinical trials but approximately 8% of American cancer patients are enrolled onto a trial. We used a domain-oriented framework to assess barriers to cancer clinical trial enrollment.
Methods
Physicians (MD, DO, fellows, residents) and research staff (physician assistants, nurse practitioners, staff and research nurses, clinical assistants, and program coordinators) involved in clinical research at a comprehensive cancer center completed an online survey in 2017; adult cancer patients not currently enrolled in a trial were interviewed in 2018. To inform the construct of our physician/staff and patient surveys and to assess barriers to clinical trial enrollment, we first conducted in-depth interviews among 14 key informants representing medical, hematologic, gynecologic, neurologic, radiation oncology, as well as members of the clinical research team (one clinical research coordinator, one research nurse practitioner). Perceived structural, provider- and patient-level barriers to clinical trial enrollment were assessed. Differences in perceptions, attitudes, and beliefs toward clinical trial enrollment between (1) physicians and staff, (2) patients by ethnicity, and (3) physicians/staff and patients were examined.
Results
In total, 120 physicians/staff involved in clinical research (39.2% physicians, 60.8% staff; 48.0% overall response rate) and 150 cancer patients completed surveys. Nearly three-quarters of physician/staff respondents reported difficulty in keeping track of the eligibility criteria for open studies but was more often cited by physicians than staff (84.4% vs 64.3%, p = 0.02). Physicians more often reported lack of time to present clinical trial information than did staff(p < 0.001); 44.0% of staff versus 18.2% of physicians reported patient family interaction as a clinical trial enrollment barrier (p = 0.007). Hispanic patients more often stated they would join a trial, even if standard therapy was an option compared to non-Hispanic patients (47.7% vs 20.8%, p = 0.002). Comparing the beliefs and perceptions of physicians/staff to those of patients, patients more often reported negative beliefs about clinical trial enrollment (e.g. being in a trial does not help patients personally, 32.9% vs 1.8%, p < 0.001) but less often felt they had no other options when agreeing to join (38.1% vs 85.6%, p < 0.001), and less often refused clinical trial enrollment due to lack of understanding (9.1% vs 63.3%, p = 0.001) than reported by physicians/staff.
Conclusion
Our findings indicate a wide gap between physician/staff and patient attitudes and beliefs about clinical trial enrollment and highlight the importance of focusing future initiatives to raise awareness of this incongruency. Reconciling these differences will require tailored education to reduce implicit biases and dispel misperceptions. Strategies to improve the quality of patient–provider communication and address infrastructure and resource issues are also needed to improve patient enrollment onto cancer clinical trials.
Keywords
Background
Cancer clinical trials are a crucial step in advancing cancer treatment, and greater participation in clinical trials expedites these advances with potential to improve the lives of people with cancer. Most cancer patients, however, do not participate in a clinical trial. Recent estimates put overall clinical trial enrollment (CTE) in the United States at 8%, ranging from 6.3% to 7.0% at community centers and 14.0% to 15.9% at academic centers.1–3 Although higher than the often cited participation rates of 3%–5%,4–7 participation in clinical trials has changed little over the past few decades.
Barriers to cancer trial enrollment are complex and multifaceted. Several models to understand and address low clinical trial participation have been described, and all propose that barriers at multiple levels affect the phenomenon, specifically at the system, provider, and patient levels,1,3 as well as the interaction between each of these levels.8,9 Unger et al. proposed that CTE barriers can be categorized as structural (e.g. trial availability), clinical (e.g. patient eligibility), and attitudinal factors (both physician and patient). To address the structural barrier of trial availability, the National Cancer Institute funds cooperative groups to develop trials that are then available across the country through mechanisms that include the National Cancer Institute (NCI)-Community Oncology Research Program (NCORP). 10 Exclusion of potentially eligible cancer patients due to rigid eligibility criteria,11,12 particularly individuals from underrepresented age, gender, and racial/ethnic groups for many clinical trials where representation is disproportionately low, 13 is an issue that is currently under evaluation by the American Society of Clinical Oncology. 14 For example, ethnic and racial minorities make up 38.7% of the US population 15 but only make up 2%–16% of those enrolled in American cancer clinical trials,13,15,16 with 0.1% are American Indian, 2.2% Hispanic, 3.3% Asian, and 6.1% Black/African American. 17 This, however, conflicts with reports indicating that racial and ethnic minority patients are as willing as whites to participate in health research and clinical trials.18,19 Much research has focused on addressing patient-related barriers as ultimately patients make the final decision whether or not to participate in a clinical trial.2,9,20,21 Interventions targeted toward patients alone, however, have variable effect; flexible and multifaceted strategies that address both patients and providers were found to be more effective. 22
Although, substantial work has been done to understand barriers to clinical trial participation, few studies have specifically targeted minority participation using a domain-oriented framework that includes an evaluation of provider and patient attitudes. Minorities represent 33% of all cancer patients seeking care at our large, urban NCI-Comprehensive Cancer Center and Minority Underserved NCI-Community Oncology Research Program (MU-NCORP) site, 23 21% of whom are Hispanic. However, the proportion of Hispanics in our catchment area is even higher at 27.4%, ranging from 17.0% in Rockland County to 55.4% in the Bronx, New York. Our most recent efforts to increase minority CTE based on the Accrual to Clinical Trial framework 24 included hiring a bilingual clinical trials navigator and conducting awareness campaigns to educate providers and patients. These efforts are expected to increase accrual to clinical trials, specifically among minority patients; however, minority CTE continues to be a challenge.
To identify actionable factors to increase CTE among of minority patients in general and Hispanic patients specifically, we examined the structural, and physician, and patient attitudinal barriers to cancer clinical trial participation among the providers and diverse groups of patients with cancer at our site. We also evaluated the knowledge and attitudes about clinical trials as well as perceptions about the barriers to CTE among key clinical personnel engaged in the conduct of cancer clinical trials and among a racially/ethnically diverse cancer patient population.
Methods
Setting and subjects
All procedures were conducted at a large urban Minority-Underserved NCORP site Columbia University Irving Medical Center (CUIMC). Physicians involved in clinical research and trial staff were identified from Cancer Center membership rosters. Cancer patient participants were recruited at medical, gynecologic, neurologic, and hematologic oncology clinics. Included were patients who were under the care of a cancer center clinical oncologist and were not currently enrolled in a clinical trial. Those not yet diagnosed with cancer or who were seeking second opinions regarding diagnosis were excluded. Participants were interviewed in the language of their preference (English or Spanish) by bilingual research team members. All procedures were approved by the CUIMC Institutional Review Board.
Development of physician, staff, and patient surveys
To inform the construct of our physician/staff and patient surveys and to assess barriers to CTE, we first conducted in-depth interviews among 14 key informants representing medical, hematologic, gynecologic, neurologic, radiation oncology, as well as members of the clinical research team (one clinical research coordinator, one research nurse practitioner). Key informants provided insight to successful strategies to increase accrual such as methods to identify potential participants, the importance of bilingual staff, and the development of a pervasive trials-friendly culture. Barriers identified included space and time constraints; need for increased coordinator support; desire for certain disease-specific trials; and perceived poor communication between oncology groups and subspecialties.
Physicians and staff survey procedures
The physician and staff surveys were conducted August through September 2017. An email invitation addressed from the Chief of the division of hematology/oncology (GS) was distributed to 250 physicians (MD, DO, fellows, and residents), clinical and research staff (physician assistants, nurse practitioners, staff and research nurses, clinical assistants, and program coordinators). A brief introduction to the study was included along with a unique link to a web-based informed consent and survey in Qualtrics. Consent and survey responses were uploaded via a secure Internet connection. Reminders were sent twice at 1-week intervals for non-respondents.
The survey was developed based on a review of the literature and the key informant interviews. Prior to implementation, the feasibility of survey administration was tested among a sample of research coordinators and was found to be acceptable. The survey took approximately 8 min to complete. Structural barriers encountered in cancer CTE 25 and personal positive and negative attitudes toward clinical trials25–27 were assessed. Perceived reasons why, from the participant’s (clinical researcher/staff) perspective, cancer patients enroll in clinical trials 28 and decline participation were determined.25–27 Reasons for study refusal were grouped as patient-related, psychosocial, logistic, and trial-related factors, and financial concerns based on categories identified in the literature.
Patient survey procedures
We used a convenience sampling strategy to approach adult cancer patients, aged 18 years and older in oncology clinic waiting rooms over a 6-month period. Patients who were under the care of a physician from the institution and who were not currently participating in a clinical trial were considered eligible to participate in this study. Surveys were conducted in the language preferred by the participant (English or Spanish) in a private area or examination room by bilingual research team members. Language in which the survey was conducted was recorded. Demographic information including age, gender, race/ethnicity, educational level, and marital status was collected. Health literacy was determined using a brief literacy screener, 29 and awareness of clinical trials was evaluated by asking a single question, “Do you know what a clinical trial is?” with responses recorded as “Yes/No.” Patient participants were asked if a clinical trial was ever offered to them and, if so, did they participate along with reasons for joining 28 or declining.25–27 These questions, as well as questions regarding personal attitudes and beliefs toward clinical trials, mirrored questions asked of the physicians and staff. Finally, a series of five questions to ascertain the circumstances under which a patient would consider joining a clinical trial were posed to patient participants (e.g. “If you had tried all available standard treatment but it did not work, would you consider participating in a clinical trial for a new treatment?”).
Data analysis
Descriptive analyses include frequency distributions, and mean, standard deviation, median, and range for continuous variables. Univariable tests of association using the chi-square test were performed to assess differences in categorical type questions and Student’s t test for continuous variables between physicians and clinical research staff and between Hispanic and non-Hispanic cancer patients. Comparison between positive and negative clinical trial attitudes, and reasons for clinical trial participation and declination as perceived by physicians/staff versus cancer patients was conducted using chi-square test. P values <0.05 were considered statistically significant, and all analyses were performed using IBM SPSS (version 24). 30 All procedures were reviewed and approved by the Columbia University Medical Center Institutional Review Board.
Results
Surveys were distributed to 115 physicians and 135 clinical/research staff involved in the conduct of clinical trials. Of these, 161 responses were received (response rate = 64.4%; 79/115 = 68.7% physicians and 82/135 = 60.7% clinical/research staff). Duplicates and surveys with ≥50% missing data were removed, resulting in 120 surveys for analysis; 47 physicians (39.2%) and 73 (60.8%) clinical/research staff. A total of 150 cancer patients completed interviews; 98 (65.3%) were non-Hispanic and 44 Hispanic (29.3%).
Physician and staff responses
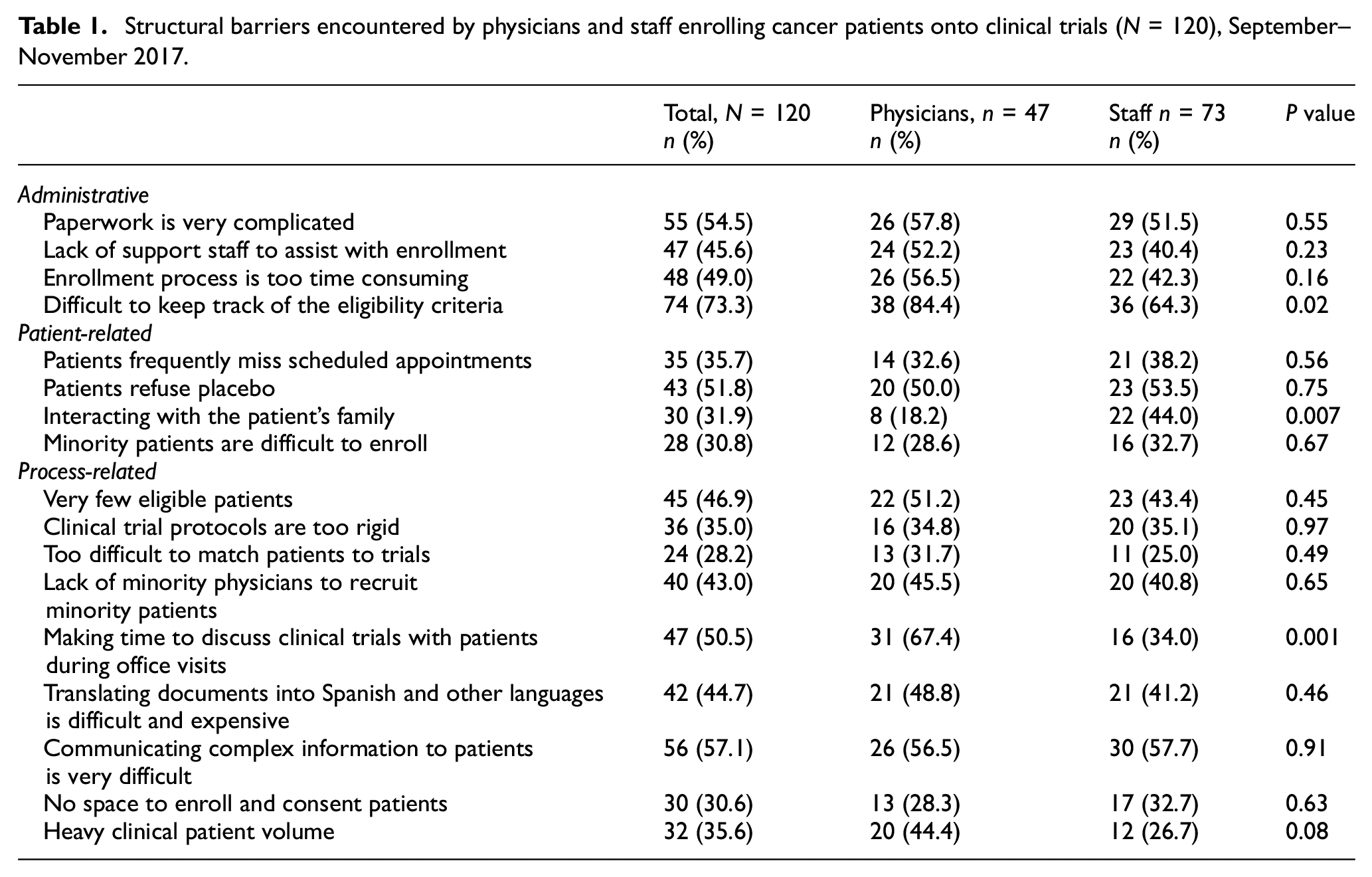
Nearly three-quarters (n = 74, 73.3%) of respondents reported difficulty in keeping track of the eligibility criteria for open studies (Table 1). This was more often cited by physicians than staff (84.4% vs 64.3%, p = 0.02). Other barriers included complicated paperwork (n = 55, 54.5%), difficulty in communicating complex information to patients (n = 56, 57.1%), and patients refusing placebo (n = 43, 51.8%). While overall only 31.9% of respondents found interacting with the patient’s family to be a barrier to enrollment, staff twice as often as physicians (44.0% vs 18.2%, p = 0.007) reported this barrier. Conversely, physicians twice as often as research staff found making time to discuss clinical trials with patients during office visits to be difficult (67.4% vs 34.0%, p = 0.001).
Structural barriers encountered by physicians and staff enrolling cancer patients onto clinical trials (N = 120), September–November 2017.
Patient responses
The majority of cancer patient surveys were conducted in English (78.0%); most participants were female (59.3%), White (61.3%), and non-Hispanic (70.7%) (Table 2). Approximately one-quarter did not know what a clinical trial is, and only 21.3% had ever been invited to participate in a trial; of those, 66% joined the trial (14.0% of all participants). When asked about circumstances under which they would “definitely” participate in a clinical trial, only 24% stated that would join today if asked. The highest proportion of participants (72.7%) would “definitely” consider a clinical trial if they thought their cancer was incurable and the clinical trial offered a new treatment, followed by 66.0% who would “definitely” consider a trial of a new treatment if all available treatment had failed.
Cancer patient clinical trials knowledge, attitudes, and beliefs by ethnicity (N = 150), May–September 2018.
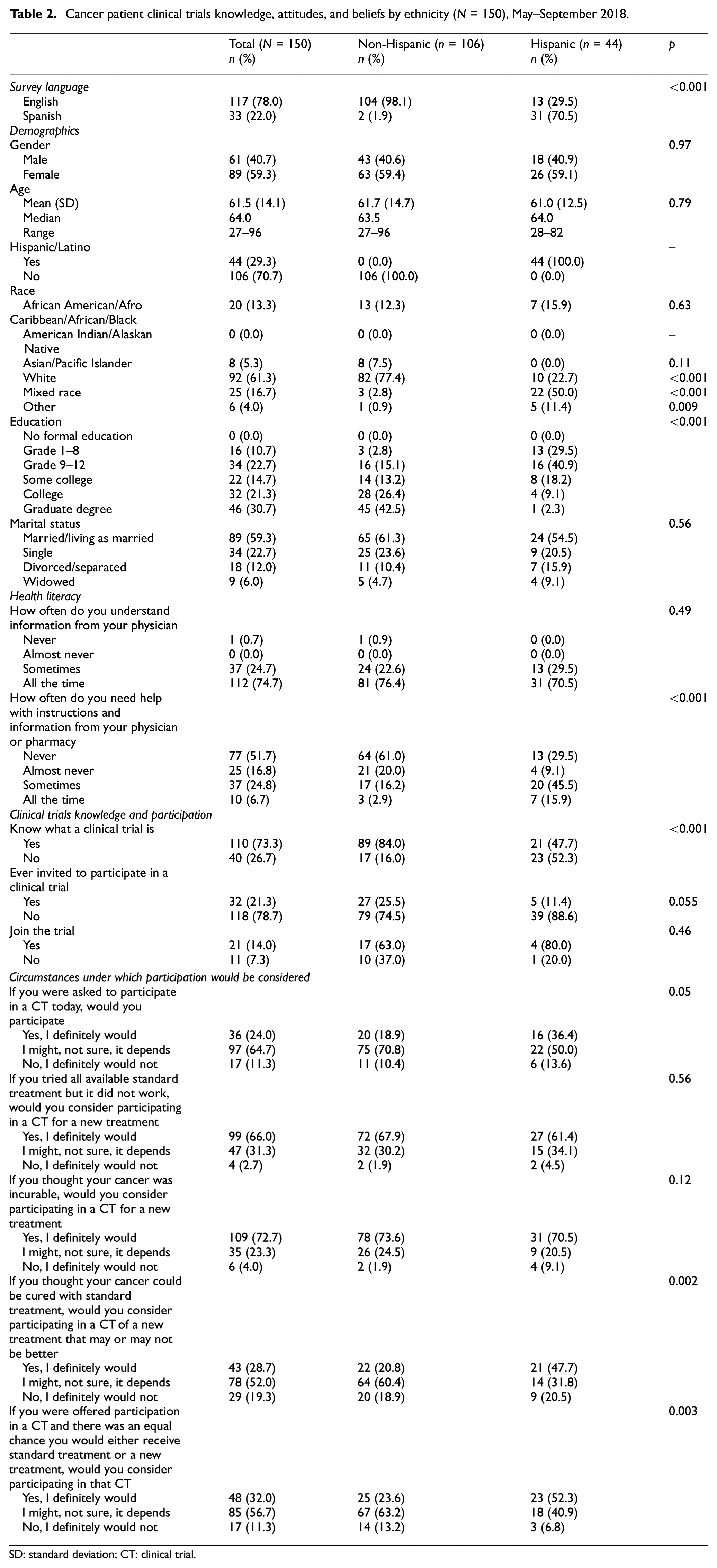
SD: standard deviation; CT: clinical trial.
Hispanics were more likely to state that they did not know what a clinical trial is compared with non-Hispanic patients (52.3% vs 16.0%, p < 0.001), but were as likely as non-Hispanics to report being invited to participate in a clinical trial (11.4% vs 25.5%, p = 0.055). However, when asked if they would participate in a clinical trial today if asked, 36.4% of Hispanic patients versus 18.9% non-Hispanic patients responded they would (p = 0.05) and twice as often responded “I definitely would” to joining a clinical if they thought their cancer could be cured with standard treatment but were offered a new treatment that may or may not better (47.7% vs 20.8%, p = 0.002) and if there was an equal chance of receiving either the standard treatment or the experimental treatment in a trial (52.3% vs 23.6%, p = 0.003) than non-Hispanic patients.
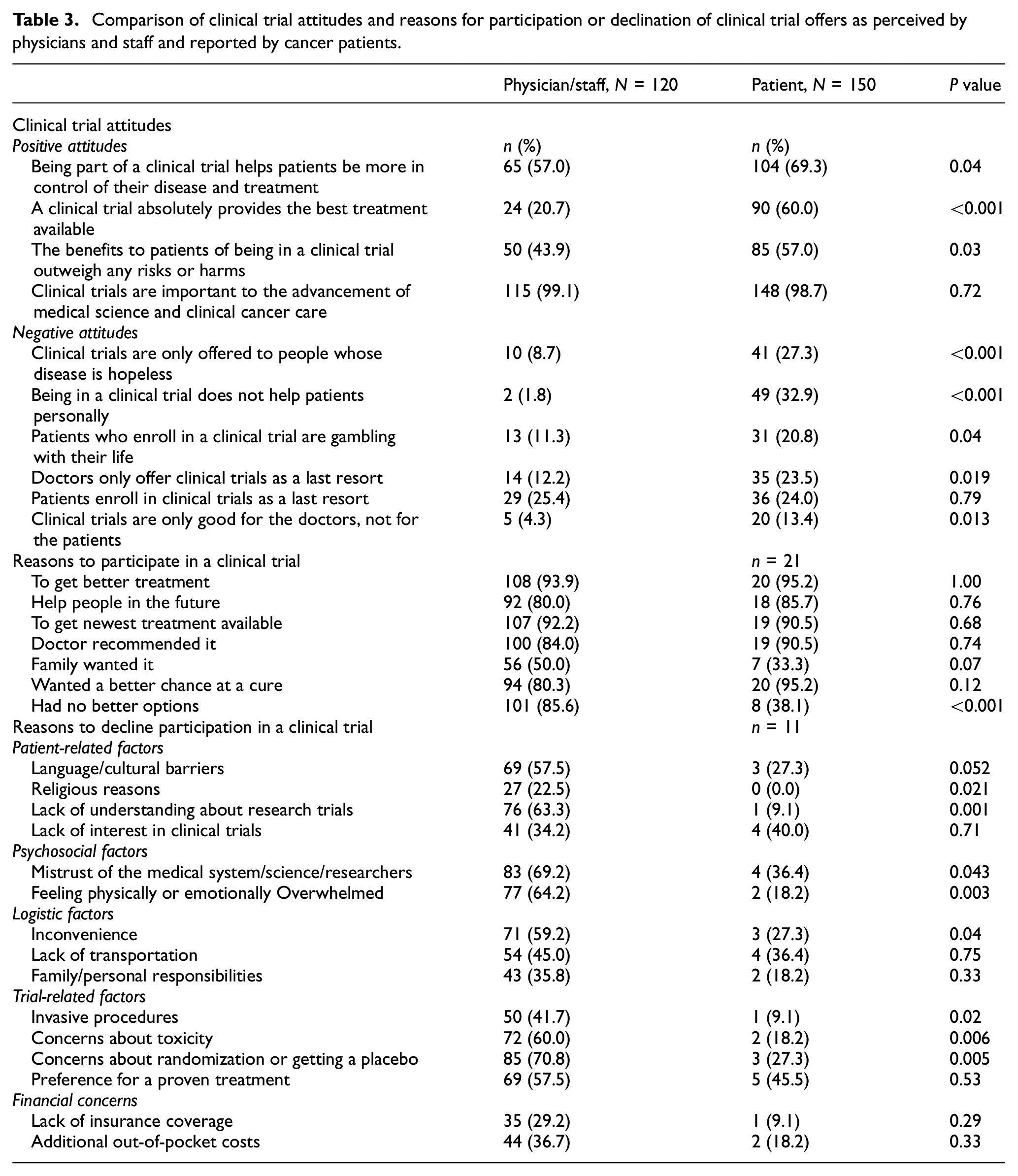
Few physicians and staff (20.7%) agreed that clinical trials absolutely provide the best treatment available, and less than half (43.9%) believed that the benefits of clinical trial participation outweighed any risks or harms. However, 57.0% felt that being in a clinical trial helps a patient be more in control of their disease and treatment (Table 3). One quarter of physicians and staff believed that patients enroll in clinical trials as a last resort. Researchers and staff perceived the most common reasons for patients to enroll in trials were to get better treatment (93.9%), to get the newest treatment available (92.2%), and because the patient had no better options (85.6%). The most frequently cited reasons for declining a trial perceived by researchers and staff were concern about randomization or getting a placebo (70.8%), followed by mistrust of the medical system, science, or researchers (69.2%).
Comparison of clinical trial attitudes and reasons for participation or declination of clinical trial offers as perceived by physicians and staff and reported by cancer patients.
Comparison of results among physicians, staff, and patients
Comparison of the perceptions of the physicians and staff to patient attitudes showed that more often, patients endorsed a positive attitude about trial involvement, differing significantly from the views of the physicians and staff (Table 3). Patients more often agreed that the benefits of participation outweigh the risks or harms (57.0% vs 43.9%, p = 0.03). In addition, patients also more frequently reported negative attitudes toward clinical trials, many of which diverged significantly from the perceptions of physicians and staff. Patients more often than researchers believed that clinical trials are only offered to people whose disease is hopeless (27.3% vs 8.7%, p < 0.001), that being in a clinical trial does not help patients personally (32.9% vs 1.8%, p < 0.001), that enrolling in a clinical trial is gambling with their life (20.8% vs 11.3%, p = 0.04), and that clinical trials are offered as a last resort (23.5% vs 12.2%, p 0.019).
Of patients offered a clinical trial and who agreed to participate (n = 21), opinions differed from those of the physicians and staff with 38.1% of patients who stated that having no better options was a consideration when making their decision to join compared to 85.6% of physicians who believed this was an important consideration for patients (p < 0.001). Among patients who were offered participation in a clinical trial but declined (n = 11), most frequent reasons for this choice were preference for a proven treatment (45.5%), lack of interest (40.0%). Reasons for declining participation cited by patients also varied significantly from those perceived by physicians and staff. For example, physicians/staff more often believed that patients decline clinical trial participation because of language and cultural barriers (57.5% vs 27.3%,p < 0.001), lack of understanding about clinical trials (63.3% vs 9.1%, p = 0.001), and mistrust of the medical system (69.2% vs 36.4%, p = 0.043) compared to patient report. Patients also less often reported declining participation because of invasive procedures (9.1% vs 41.7%, p = 0.02), concerns about toxicity (18.2% vs 60.0%, p = 0.006), and reluctance to be randomized or to receive a placebo (27.3% vs 70.8%, p = 0.005).
Discussion
Our findings demonstrate barriers to trial participation are frequent at the structural, provider, and patient levels. In addition, we found significant differences in perceived patient barriers to trial enrollment between research physicians and their staff; differences in barriers, attitudes, and beliefs between Hispanic and non-Hispanic patients; and, most importantly, differences between what research physicians and staff believe are barriers for patients and what patients report as barriers.
The process of enrolling a cancer patient onto a clinical trial is multifaceted with the potential for breakdown at several key junctures along the way. Typically, patients newly diagnosed with cancer visit a cancer clinic and, depending on site infrastructure and protocols, are evaluated for trial eligibility. Assessment of eligibility, however, is contingent upon the availability of trials for the particular histology or stage of a patient’s cancer. 3 In a recent systematic review and meta-analysis of multi-level clinical trials barriers, Unger et al. reported that structural barriers are perhaps the greatest of barriers to trial participation; clinical trials were not available for 55.6% of cancer patients, and another 2.15% were ineligible for trials that were available. 3 The structural barriers identified in our study that included difficulty in keeping track of eligibility criteria and carving out time during a visit to discuss trials and enrollment further complicate the first crucial step in the process of enrolling patients to clinical trials.
Once assessed as eligible for an available trial, the physician may or may not choose to discuss and offer trial enrollment to the patient. Physician bias and its impact on the decision whether or not offer a given patient a clinical trial has not been fully investigated. One example is a study conducted by Kornblith et al. that examined physician perceptions of barriers to clinical trials among elderly breast cancer patients. Physicians reported reluctance to enroll elderly patients due to comorbid conditions not excluded by trial protocol; that elderly patients would not fully understand trial procedures and would therefore likely be non-compliant; and that older patients may experience greater toxicity. 31 Others have similarly reported how conscious and unconscious implicit physician bias against a patient’s age and comorbidities as well as bias against members of minority groups and perceptions of patient mistrust of researchers. 17 These biases sometimes result in spontaneous and reflexive decisions about the candidacy of a patient for a trial, influence patient–provider interactions, and lead to foregoing clinical trial options during discussions about treatment thus limiting offers of enrollment.17,32,33 Physician bias may also contribute to poor accrual to trials and early trial closure in addition to the lost opportunity to provide new treatments and better ancillary patient care.3,17
Only at the end of this process of negotiating structural and provider-level barriers does the patient’s decision to participate enter the equation. Patients in our study more frequently endorsed negative attitudes about clinical trials, such as only being offered to those whose disease is hopeless, not helping patients personally, participation is gambling with one’s life, and only being good for the doctor, not the patient. Consistent with prior literature, a significant number of patients cited a preference for standard treatment or a lack of interest in participating in clinical research as a reason for declining. 34 Furthermore, our results demonstrate a significant difference in clinical trial knowledge and attitudes by ethnicity, with Hispanics reporting less awareness about clinical trials which is consistent with previously literature reporting lower participation in clinical trials in racial and ethnic minority groups. 13 We also found that, despite less awareness of clinical trials and greater reported negative attitudes toward trials, Hispanic patients were more willing to consider a trial than their non-Hispanic counterparts were. When posed hypothetical conditions under which a patient might consider clinical trial participation, only a small proportion of patients overall stated that they definitely would not participate with Hispanics twice as often stating they would definitely participate. These findings are aligned with those of Comis et al. who reported that most Americans hold favorable views of clinical trial participation. 19
Discordance between what physicians and research staff perceive as barriers and what patients state has not been previously reported. In our study, physicians and research staff often over- and under-estimated the importance of patient-reported barriers and highlight the ongoing communication that is needed between the provider/staff and patient. A study by Albrecht et al. of videotaped outpatient interactions between oncologists and patients and their family, when present, at two comprehensive cancer centers found that clinical trial participation was only offered to 20% of participants previously determined to be eligible for a trial, but when offered, 75% of these eligible patients assented. Greater shared conversation control with the physician was significantly related to the patient’s decision to enroll highlighting the importance of content and relational communication between physicians and patients, provider–patient alliance building, and supportive dialogue in a full, clear, and open discussion of clinical trial participation. 35
Our study had some strengths worth highlighting. First, we developed the survey from key informant interviews which revealed key structural and provider-related topics that we included in our quantitative survey. This participatory research process ensured that we were asking relevant questions related to the topic. However, we did not include a patient representative in the development of our survey; this would have strengthened our study further. This is a single site, observational study conducted at a large urban Minority-Underserved NCORP site within an NCI-designated comprehensive cancer center in New York City, which may limit generalizability of our findings to other geographic areas and patient populations. A major strength of this study is the unique assessment of the knowledge, attitudes, and beliefs of physicians and staff in parallel with those of patients. This allows us to have greater insight into the individual groups, but also to better develop tailored interventions within appropriate groups. Tailored, multi-level interventions have been cited as the most successful to reduce barriers to CTE, and the level of granularity and comparison that our data provides will support future initiatives.
Conclusion
Our study highlights the knowledge, attitudes, and beliefs about CTE from provider, staff, and patient perspectives and support previously defined barriers to clinical trial participation, specifically between Hispanic and non-Hispanic groups. These data also provide new information about the gaps between provider-/staff- and patient-perceived barriers. Specifically, to our knowledge, this is the first published comprehensive assessment across physicians, staff, and patients to understand differences in perceptions about CTE barriers. Attitudes can be defined as a “learned tendency to evaluate things in a certain way” that are informed by personal experience, social norms, conditioning, and observation. 36 Differences in attitudes between providers and patients are important to understand in order to focus future initiatives to raise awareness about incongruency between each group and reduce implicit biases. One possible strategy to address discordant provider/patient attitudes could be to incorporate these same factors that lead to the development of attitudes into educational interventions to effect attitude change. For example, enhancing personal CTE experiences for patients and providers through improved communication and streamlined workflow or promoting the enrollment of racial and ethnic minorities onto clinical trials as an institution-wide desired social norm. Clear, transparent communication between providers, staff, and patients about clinical trials should also be emphasized, as this will help to reduce inconsistencies across provider/patient continuum and in addition, help to reduce medical mistrust. 22 Other strategies such as educating patients about clinical trials prior to their first oncology visit, 37 engaging the community, diversifying the clinical and research staff to be more representative of the community, and providing education to the community and providers/staff may also help to reduce these barriers. 22
Supplemental Material
Supplemental_Material – Supplemental material for Discordant attitudes and beliefs about cancer clinical trial participation between physicians, research staff, and cancer patients
Supplemental material, Supplemental_Material for Discordant attitudes and beliefs about cancer clinical trial participation between physicians, research staff, and cancer patients by Grace C Hillyer, Melissa Beauchemin, Dawn L Hershman, Moshe Kelsen, Frances L Brogan, Rossy Sandoval, Karen M Schmitt, Andria Reyes, Mary Beth Terry, Andrew B Lassman and Gary K Schwartz in Clinical Trials
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Outside the submitted work, ABL declares personal compensation in the last 3 years from Karyopharm, Abbott Molecular, QED Therapeutics, Forma, Bayer, Northwest Biotherapeutics, AbbVie, Agios, Orbus, Bioclinica as an expert blinded independent reviewer of clinical and imaging data for a BMS-sponsored trial, Celgene, and Novocure.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a National Cancer Institute Minority/Underserved Community Oncology Research Program (MU/NCORP), UM1 CA189960 and Cancer Center Support Grant P30CA013696.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.