
Abstract
Background:
Patient reports of expected treatment side effects are increasingly collected as part of the assessment of patient experience in clinical trials. A global side effect item that is patient-reported has the potential to inform overall tolerability. Therefore, the aim of this study was to examine the completion and distribution of such a global single-item measure of side effect burden in five cancer clinical trials.
Methods:
Data from five trials from internal Food and Drug Administration databases that included the Functional Assessment of Cancer Therapy–General single-item measure of overall side effect burden (i.e. impact on degree of bother) were analyzed. Completion rates for the side effect bother item, items adjacent to this item, and two non-adjacent items on the Functional Assessment of Cancer Therapy–General that are related to health-related quality of life were calculated at the baseline assessment and at the 3-month assessment. To evaluate the distribution, the percentage of patients reporting high levels (quite a bit or very much bother) of side effect bother at baseline and 3 months was assessed.
Results:
Completion rates for all items were at least 80% regardless of time point or trial population. However, in three of the five trials, completion rates for the side effect bother item were lower at baseline compared to adjacent and non-adjacent items. This difference was not observed at 3 months. Up to 9.4% of patients reported high levels of side effect bother at baseline.
Conclusion:
Patients may enter trials already reporting some bother from side effects. This can make interpretation of results with respect to the investigational agent under study challenging. Patients may skip an item evaluating side effect bother at baseline, suggesting some difficulty with interpretation of what is being asked. Further study of the wording and utility of a baseline side effect bother assessment is warranted.
Introduction
Clinical trials increasingly collect information about patient experience while on therapy, which includes disease and treatment burden (e.g. disease symptoms, disease impacts, treatment side effects).1,2 Cancer therapies can have significant toxicity, and the use of patient-reported symptomatic adverse events or side effects is an active research area. The National Cancer Institute developed the Patient-Reported Outcomes Version of the Common Terminology Criteria for Adverse Events (PRO-CTCAE) to complement the current collection of clinician-reported adverse events. 3 These efforts acknowledge that patients are best positioned to characterize their own symptoms and reflect both concern about clinician underreporting of symptomatic adverse events 4 and recognition that the patient voice has been underrepresented in safety reporting.1,5
In addition to better understanding the incidence and trajectory of individual symptomatic adverse events, there is also interest in understanding patients’ assessment of their overall side effect burden because of an intervention. One possible way to capture this is to use a single-item global question to evaluate bother from the side effects of cancer therapy. In the Functional Assessment of Cancer Therapy–General (FACT-G), a commonly used patient-reported outcome measure, there is the GP5 item, “I am bothered by the side effects of treatment.” Previous research focused on this item has identified associations with clinician-reported adverse events, patient-reported outcomes relating to health-related quality of life, 6 and risk of early treatment discontinuation. 7 In particular, Wagner and colleagues found that patients with higher levels of pre-treatment side effect bother were more likely to discontinue treatment. 7
In this exploratory study, we sought to investigate how patients in five trials responded at baseline (pre-treatment) to a global single item asking them to report overall side effect bother. Our aims were to characterize the completion rate and degree of side effect bother as measured by FACT-G GP5 at baseline. For comparison, we also assessed completion rates and degree of bother at 3-month follow-up. We focused on the FACT-G GP5 as FACT is a widely used assessment tool in oncology, particularly in certain disease areas such as prostate cancer. 8 Furthermore, although the PRO-CTCAE is a library of individual patient-reported adverse events, at present there is no single summary score or single-item global question. 9 The European Organisation for Research and Treatment of Cancer has a single global side effect item, EORTC Q168, in their item library; 10 however, we were unable to identify studies containing that item in the internal Food and Drug Administration (FDA) database.
Materials and methods
Data source and study population
We identified five randomized clinical trials from internal FDA databases that contained the FACT questionnaire and had acceptable data quality. These trials spanned three cancer types (prostate, renal cell, and breast). Three of the five trials involved patients who had previously been treated with systemic anti-cancer therapy. The evaluated agents varied in terms of toxicity, and all the trials used the FACT-G questionnaire containing the GP5 single-item side effect bother question supplemented with the disease module of interest. The FDA project lead and/or the Center for Drug Evaluation and Research Human Subject Protection Liaison to the FDA Institutional Review Board (IRB) determined that this study is consistent with a “not human subject research” determination and thus does not require IRB review. Trial intention-to-treat population sizes ranged from 1096 to 2840.
Instruments and items
The trials included the prostate cancer, breast cancer, and renal cell carcinoma disease-specific FACT modules, depending on the cancer type. For all questions, the recall period was the “past seven days” and the response options ranged from 0 (“not at all”) to 4 (“very much”).
Completion rates were evaluated for GP5 (“I am bothered by the side effects of treatment”) and for items adjacent to GP5 that included the following: item GP4 (“I have pain”) and item GP6 (“I feel ill”). We also evaluated completion rates for items pertaining to health-related quality of life: item GF3 (“I am able to enjoy life”) and item GF7 (“I am content with the quality of my life right now”).
Assessment time points
We considered two assessment time points. The first time point, which was of primary interest, was the study baseline/screening assessment (i.e. before study treatment administration). In addition, we repeated the analyses described below at a second time point: approximately 3 months post-baseline. We chose the 3-month time point as this was relatively similar across trials in terms of the questionnaire assessment schedule and occurred early enough in the trial to minimize attrition.
Completion rate calculation
Completion rates for each item of interest (GP4, GP5, GP6, GF3, GF7) were calculated as the number of patients with non-missing answers to the item in question divided by the relevant denominator. At baseline, the denominator for all trials was defined as the intention-to-treat population. At the 3-month follow-up time point, the denominator was the on-study population, defined as those patients still on treatment. Treatment discontinuation was determined by patient withdrawal from active treatment prior to the maximum number of cycles being reached (where applicable) or data cutoff (if no maximum number of cycles was specified). Discontinuation criteria varied by trial; however, in all trials, patients could withdraw for any reason and investigators could withdraw patients for reasons such as disease progression or adverse events.
Categorization of degree of bother
Patients who reported a 3 (“quite a bit”) and 4 (“very much”) were considered to experience a high degree of bother.
Results
Four of the five trials included patients with metastatic disease (Table 1). Of the three prostate trials, only one included patients who had previously received systemic chemotherapy. However, patients in the other two trials had received locoregional therapies. Similarly, in the renal cell trial, although nearly all patients had not received systemic therapy, most had received locoregional therapies. Patients in the breast cancer trial previously received extended adjuvant therapy following human epidermal growth receptor 2–targeted therapy. Patient-reported outcome collection methods were not always specified in the protocol. In two trials, these outcomes were collected by paper; the method was not clear for the remaining three trials.
Trial populations.
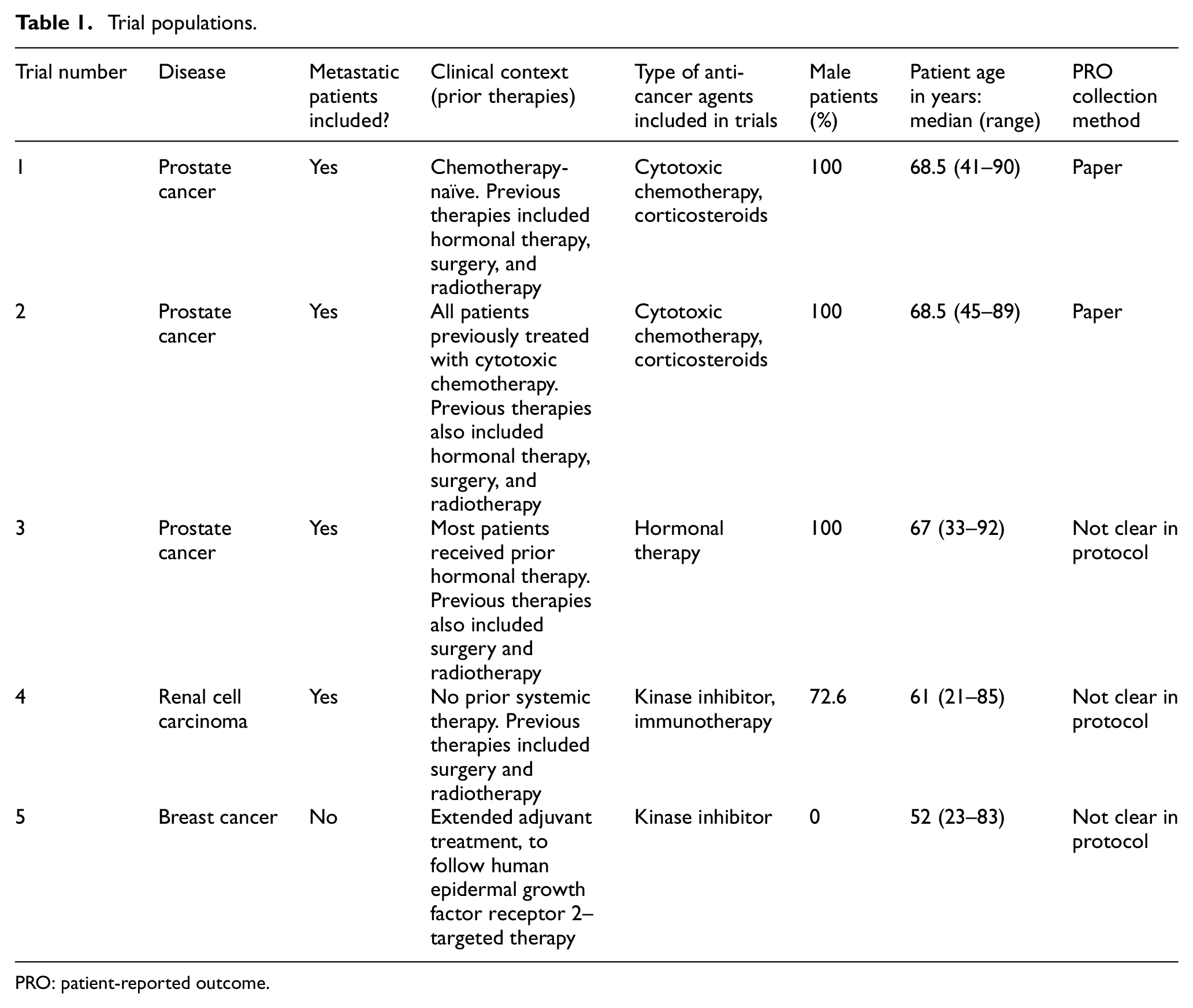
PRO: patient-reported outcome.
Completion rates
Of the five items investigated, completion rates at both baseline and 3 months were at least 90% except in three trials where the GP5 item had a lower completion rate at baseline (Table 2). In these three trials, the median difference in completion relative to the adjacent items was 7.1% (range, 5.8%–11.3%) and relative to the health-related quality of life items was 6.5% (range, 5.6%–10.9%). The other two trials had the same completion rate for all items at baseline. One of these two trials was in a chemotherapy-naïve population and one was not; however, as noted above, in all trials patients received some form of anti-cancer therapy. Due to the lack of information on PRO collection methods, it is not clear whether these trials used the same collection approach or not.
Completion rates: baseline and follow-up.
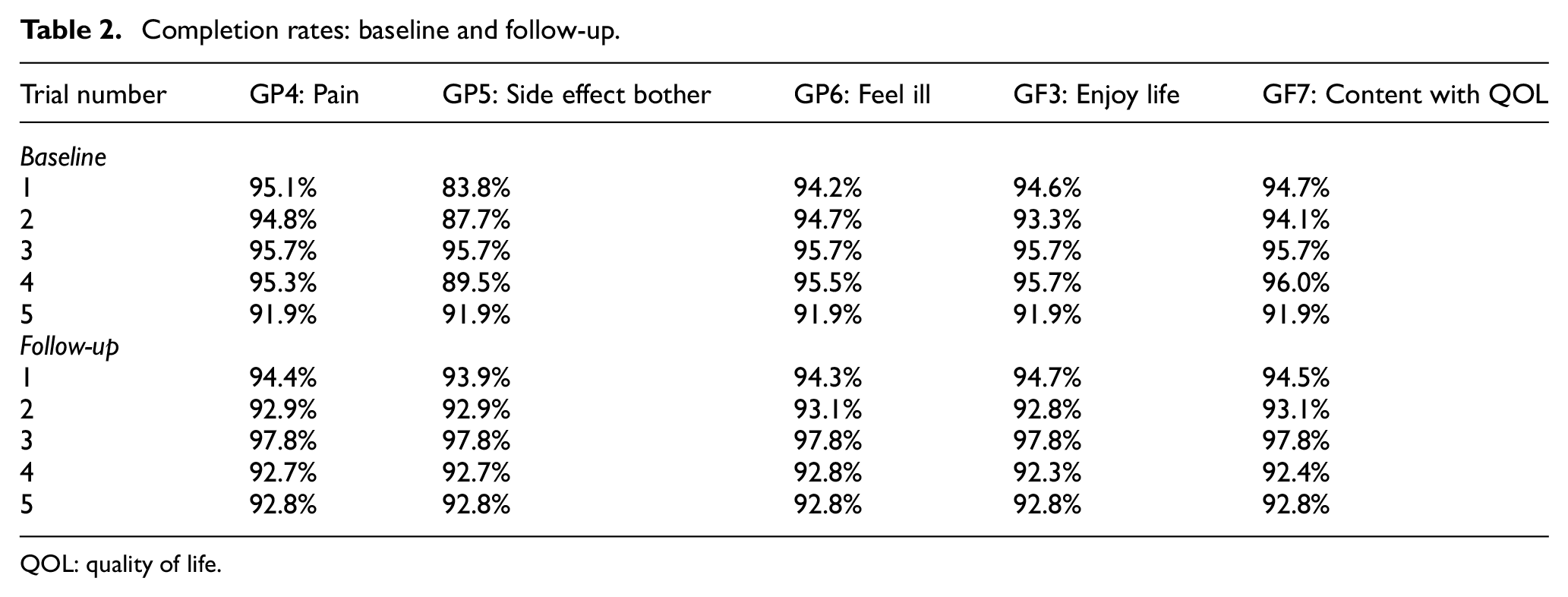
QOL: quality of life.
At 3 months, completion rates for the side effect bother item were comparable to the completion rates for other items (completion difference <1% across items). The two trials that had identical completion rates across all items at baseline also had identical completion rates across all items at 3 months.
Degree of bother
At baseline, prior to starting any new investigational therapy, 2.1%–9.4% of patients reported high degree of bother (Table 3). For these trials, patients were more likely to report “quite a bit” of bother, rather than the maximum score of “very much” bother.
Degree of bother over time: baseline and follow-up.
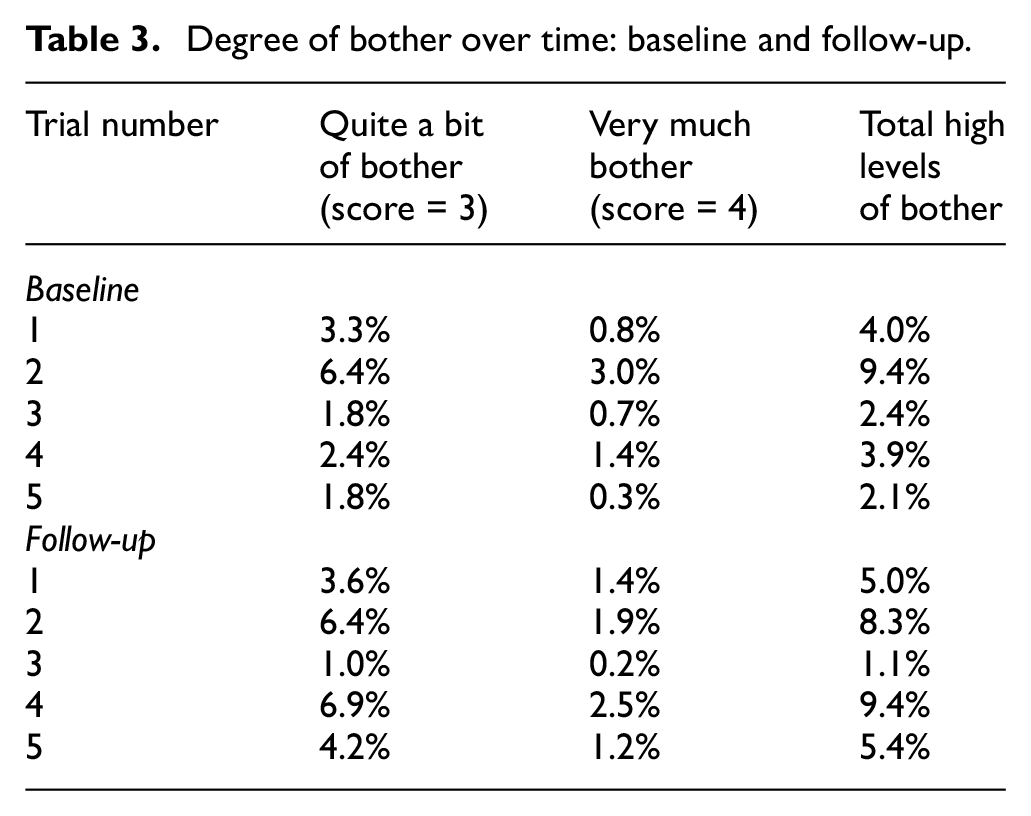
At 3 months, 1.1%–9.4% of patients reported high degree of bother. In all trials, higher percentages of patients with a high degree of bother had reported “quite a bit” of bother, rather than “very much” bother.
Discussion
Completion rates for the side effect bother item in these trials were >80%; however, at baseline, in three trials this item was completed less frequently than adjacent items as well as other items assessed later in the FACT instrument. This difference in completion was seen regardless of the patient population. Furthermore, in all five trials, a minority of patients commenced the study reporting a high degree of bother prior to receiving any investigational therapy. These findings illustrate both the potential importance and the challenge of understanding patient perception of side effect bother at the beginning of a trial.
Of note, the concept of bother can be challenging to measure as it can vary as a function of disease stage and individual tolerance. For example, patients may report being bothered by a symptom that is not very severe, or alternatively, a patient may become tolerant to a symptom and report less “bother” even though the symptom remains severe. Furthermore, different patients may have different levels of perceived bother with the same level of symptom intensity.
In evaluating the completion rates, we also found relatively higher missingness in the side effect bother item at baseline in several trials. Two of the five trials had consistent completion rates across all items and no reason for this could be identified in the trial protocols; however, one possibility may have been the use of an electronic device to capture responses that prevented skipping an item. As few trial protocols explicitly discussed their approach for PRO collection, we cannot confirm whether collection approach was related to completion. In addition, in the trials we investigated, there was no clear association between previous treatment with systemic anti-cancer therapies and baseline completion rates for the side effect bother item. The discrepancy in completion across items was not observed at the 3-month follow-up visit; it may be that some patients were unsure how to respond to an item about side effect bother when they were not currently receiving therapy. Qualitative studies could further elicit how patients understand and interpret this type of question at baseline and perceive its appropriateness. Such a study could lead to improved baseline completion rates for this item or a reevaluation of how it is asked or to whom it is asked.
Further research is particularly important because patient reports of side effect bother and/or adverse events at baseline have been used in other studies. In an analysis of patients with breast cancer, Wagner et al. 7 found that patients reporting bother from side effects at baseline were at greater risk of early discontinuation of aromatase inhibitor therapy. Since patients have yet to receive the investigational therapy at baseline, by definition, these reports of bother cannot be attributed to the agent(s) under study. In all trials in our study, some patients reported high levels of side effect bother at baseline. The patients were not completely treatment-naïve as many had received some kind of prior treatment (e.g. locoregional therapies) which may have had long-lasting side effects. It is possible that patients may be reporting long-term side effects from previous therapies, other medications they are taking, or disease symptoms. In addition, some approaches for evaluating PRO-CTCAE data have tried to account for patient reports of adverse events at baseline.11,12 Given the levels of missingness seen in this study, such analyses would be challenging. In this context, asking a question about side effect bother at baseline is of questionable utility.
In addition, our findings point to the importance of defining completion rates. Previous FDA studies have documented the variability in definition of completion rates in trials. 13 If analyses of side effect bother are of interest, completion rates that require the “completion of at least one item” may not be helpful in understanding how many patients are included in the analysis of a single-item global side effect bother item. This further highlights the importance of standardizing approaches for missing data, as advocated by consortia such as Setting International Standards in Analyzing Patient-Reported Outcomes and Quality of Life. 14
In addition to measuring individual symptomatic adverse events of interest, post-baseline follow-up assessments of an overall summary side effect measure remain of great interest to inform a cancer product’s tolerability. However, our exploration of the single item, GP5 from FACT-G, identified some challenges with completion rate of baseline assessments. Further work is needed to explore the utility and relevance of baseline assessment of overall side effect summary measures in prospective cancer trials.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: B.L.K.-K. reports previous employment with Pharmerit International. J.K.R., P.R., C.W., D.K., S.R.D., D.L.S., J.A.B., and P.G.K. declare that there is no conflict of interest.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Disclaimer
This paper reflects the views of the authors and should not be construed to represent FDA’s views or policies.