
Abstract
Background:
Researchers often conduct small studies on testing a drug’s efficacy in off-label indications. If positive results from these exploratory studies are not followed up by larger, randomized, double-blinded trials, physicians cannot be sure of a drug’s clinical value. This may lead to off-label prescriptions of ineffective treatments. We aim to describe the way clinical studies fostered off-label prescription of the antipsychotic drug quetiapine (Seroquel).
Methods:
In this systematic meta-epidemiological analysis, we searched EMBASE, MEDLINE, Cochrane CENTRAL and PsycINFO databases and included clinical studies testing quetiapine for unapproved indications between May 1995 and May 2022. We then assessed the frequency with which publications providing low-level evidence suggesting efficacy of quetiapine for off-label indications was not followed up by large, randomized and double-blinded trials within 5 years.
Results:
In total, 176 published studies were identified that reported potential efficacy of quetiapine in at least 26 indications. Between 2000 and 2007, publication of exploratory studies suggesting promise for off-label indications rapidly outpaced publication of confirmatory trials. In the 24 indications with a minimum of 5 years of follow-up from the first positive exploratory study, 19 (79%) were not followed up with large confirmatory trials within 5 years. At least nine clinical practice guidelines recommend the use of quetiapine for seven off-label indications in which published confirmatory evidence is lacking.
Conclusion:
Many small, post-approval studies suggested the promise of quetiapine for numerous off-label indications. These findings generally went unconfirmed in large, blinded, randomized trials years after first being published. The imbalance of exploratory and confirmatory studies likely encourages ineffective off-label treatment.
Keywords
Introduction
Clinical trials play a vital role in supporting safe and effective use of pharmaceuticals. New drugs are typically vetted in a series of clinical trials, culminating in randomized phase 3 trials that lead to regulatory approval. Although intended to inform clinical decision-making, clinical trials are sometimes conducted or reported in ways that frustrate this objective. For example, documents uncovered during litigation surrounding the antiseizure medication gabapentin revealed an elaborate strategy whereby selective publication of so-called ‘seeding trials’ was used to encourage off-label use.1–3 Other reports suggest that clinical trials are sometimes used to build relationships with physicians or to habituate them to using an unfamiliar medication.4–8
Another way clinical research can interfere with effective medical management occurs when exploratory, phase 2-like studies are not coordinated with confirmatory phase 3-like trials. After a drug receives approval, companies and academic investigators often conduct studies aimed at extending a new drug to additional indications. 9 Such post-approval studies, while potentially uncovering new applications, often produce spurious suggestion of clinical promise due to their low precision, short follow-up times, reliance on surrogate endpoints or high risk of bias. 10 More rigorous, larger trials that extend and confirm these early findings are expensive to run and need more resources to coordinate; hence, public funding agencies are less likely to sponsor these efforts. However, unless promising findings from exploratory investigations are advanced to confirmatory testing in rigorous trials, their dissemination in reprints, medical journals and news reports encourages off-label prescription of ineffective treatment approaches. Busy practitioners often lack the time or epidemiological acumen to critically appraise such reports.
Quetiapine (Seroquel) is a multimodal action drug in the pharmacological domain of dopamine, serotonin and norepinephrine (previously ‘atypical’ antipsychotic). It received Food and Drug Administration (FDA) approval in schizophrenia (1997), bipolar disorder (first approval 2004) and major depressive disorder (2009).11,12 FDA approvals were backed by strong evidence: two placebo-controlled randomized trials for schizophrenia, three placebo-controlled trials for bipolar disorder and two phase 3 randomized trials for major depressive disorder. As with other psychiatric drugs, however, quetiapine is commonly prescribed off-label for many conditions, including insomnia, agitation in patients with dementia and post-traumatic stress disorder (PTSD).13–18 This widespread off-label use was criticized in 2010 when its manufacturer, AstraZeneca, was fined US$520 million to resolve allegations that it illegally marketed Seroquel for uses not approved as safe and effective by the FDA. 19
In this systematic meta-epidemiological review, we examined how the proliferation of small studies produced findings that encouraged physicians to entertain off-label prescription of quetiapine for a variety of disorders, a phenomenon we have elsewhere called the generation of clinical agnosticism.20,21 In particular, we determined the frequency with which small exploratory studies suggesting efficacy for off-label indications went unconfirmed by large, double-blinded, randomized trials for at least 5 years (‘prolonged agnosticism’). Secondarily, we explored the incorporation of positive exploratory reports for off-label quetiapine use into recommendations within clinical practice guidelines.
Methods
Analyses were prespecified in a study protocol that was registered on the Open Science Framework. 22 The methods employed in our analyses are adapted and extended from a previous study. 21
Searches
We searched Ovid MEDLINE and Ovid MEDLINE In-Process and Other Non-Indexed Citations databases (dates of coverage, 1948–2019), and EMBASE and EMBASE Classic databases (dates of coverage, 1974–2019) on 17 November 2019 adapting a search strategy described previously. 23 On 19 December 2019, we searched Cochrane CENTRAL using the search term ‘quetiapine’ and the PsycINFO database using the search terms ‘quetiapine’ and ‘Seroquel’ with various filters as detailed in the Supplemental material and study protocol. 22 All searches were updated on 12 May 2022. Results were pooled, and duplicates removed.
Studies were included if quetiapine was tested as an intervention in a population not included on the FDA label or an approval was issued less than 1 year prior to the publication of the trial report. Also, studies needed to report at least one clinical or functional efficacy outcome. Studies with fewer than 50 participants receiving quetiapine without a positive outcome were primarily excluded as they would likely not be regarded by practitioners as encouraging use of quetiapine for an off-label indication. In a secondary step, we also included non-positive exploratory studies in off-label indications with clinical agnosticism (see definitions below) to complete insights into the research landscape for quetiapine. On the title/abstract level, all studies were independently screened by two authors using Rayyan QCRI. 24 If one author did not exclude the study, it was moved to the full-text review stage.
We excluded all publications that reported (1) review; (2) meta-analysis; (3) case study; (4) abstract only; (5) registry entry; (6) animal study; (7) in vitro study; (8) language other than English, German, Italian, French, Spanish, Dutch and Portuguese; (9) wrong study type (no efficacy endpoint) and (10) US FDA on-label studies in which publication came more than 1 year after regulatory approval for the same indication.
Data extraction
From the eligible full-text publications, we extracted (1) study characteristics, including disease indication, diagnostic system used, approval status and date of publication; (2) design features, including blinding, randomization, sample size for efficacy outcome and comparator; (3) meta-information, such as trial registration number (see Supplemental Material for full codebook). Every study was extracted independently by three coders (L.S., P.G. and J.S.) using Numbat Meta-Analysis Extraction manager. 25 Disagreements were resolved by discussion, and decisions made to specify item definitions were documented in the codebook (for more details, see Supplemental material). The data extraction process was piloted first (n = 12), and results are included in the protocol.
Definitions
We considered an efficacy outcome as ‘positive’ if it demonstrated a statistically significant effect with p < 0.05 (see Supplemental Table 1 for the full coding scheme). We categorized all studies as either ‘exploratory’ or ‘confirmatory’ based on sample size and design characteristics of the study (Table 1).
Overview of concepts and their definitions.
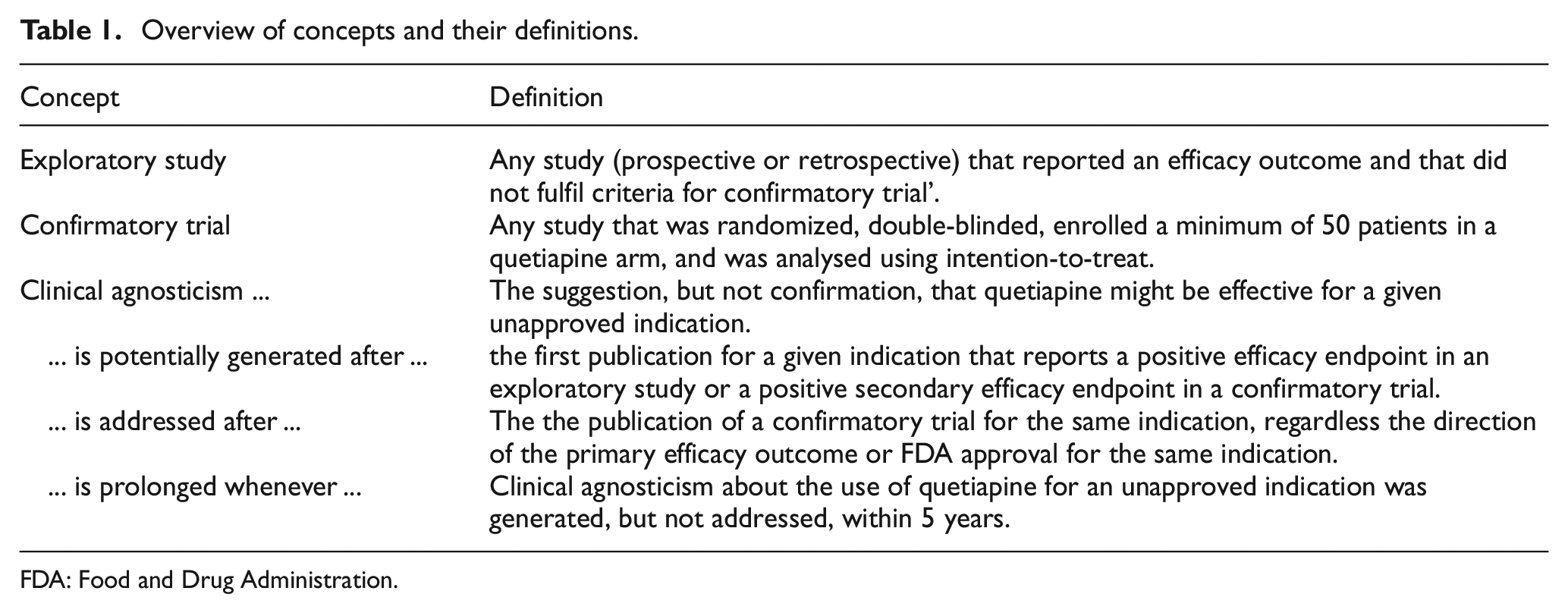
FDA: Food and Drug Administration.
A confirmatory study was defined as any randomized, double-blinded study that enrolled a minimum of 50 patients in a quetiapine arm and analysed using intention-to-treat. An exploratory study is any included study that did not meet the criteria of a confirmatory study. As n ≥ 50 cut-off for our definition of confirmatory trials is arbitrary, we conducted sensitivity analyses using more permissive (n = 30) or restrictive (150, 350) sample size definitions for confirmatory testing. The outcome of an explorative study was deemed positive if at least one reported efficacy endpoint favoured quetiapine at the p ≤ 0.05 significance level. For confirmatory trials, the result of the primary efficacy endpoint determined if the trial was counted as negative or positive (for details, see Supplemental Table 1).
We reasoned that physicians or guideline committees might be encouraged to consider the use of quetiapine for off-label use in an indication if they read a report suggesting efficacy in a small study. We thus defined a publication as encouraging practitioners to entertain using quetiapine for an off-label indication (i.e. ‘clinical agnosticism’) if it suggested, but did not confirm, that quetiapine might be effective, using the following two criteria: (a) an exploratory study reported a positive efficacy result, or (b) a confirmatory study reported a positive efficacy result as a non-primary endpoint. We did not assess the quality of studies or apply risk of bias measures since they are not relevant in this context. Studies might be low risk of bias, but nevertheless encourage inflated perceptions of a drug’s promise due to low precision, use of short follow-up times or enrolment of highly selected patients. Furthermore, even small unblinded studies, if published and disseminated, can influence prescription if physicians do not critically evaluate the trials. 26 We considered clinical agnosticism for a given indication to be ‘addressed’ after publication of a confirmatory trial, regardless of outcome. We defined agnosticism as being ‘prolonged’ when more than 5 years elapsed between publication of positive exploratory findings and publication of any confirmatory trials in the same indication.
Guideline searches
To investigate how exploratory studies might influence clinical practice, we conducted searches for clinical practice guidelines recommending quetiapine in indications without confirmatory trials. We limited our searches to four entities: the National Institute for Health and Care Excellence (NICE), 27 the Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften e.V. (AWMF), 28 the American Psychiatric Association (APA) 29 and the Canadian Medical Association national clinical practice guidelines. 30 We noted any guideline recommending the use of quetiapine in the respective indication and recorded recommendations made, grade of recommendation/evidence and the exploratory studies cited to support recommendations. Guidelines were extracted by three independent coders (P.G., L.S. and S.G.S.).
Searches on clinicaltrials.gov
For a post hoc analysis, we searched the study registry clinicaltrials.gov for ongoing or completed confirmatory quetiapine trials in off-label indications in which we identified promising exploratory studies but no confirmatory trials in the published literature. We used the advanced search function and ‘quetiapine’ in the ‘Intervention/treatment’ field and the respective indication in the ‘Condition or Disease’ field.
Analysis and statistics
To calculate the summary measures, we used R version 3.4.4 or higher. 31 To graphically represent the exploration of quetiapine for all indications, we plotted Accumulating Evidence and Research Organization diagrams (AERO diagrams) representing indications on the vertical axis and year of study publication on the horizontal axis; vertical ordering was based on the chronology in which studies for new indications were published. AERO diagrams provide a visual representation of the number of studies done at any stage of research and help to explain the accumulating state of evidence of a clinical research programme. 32 We did not conduct a planned analysis of effect sizes for feasibility reasons since larger standardization and unification across studies would have been needed to achieve comparable results. Other deviations from our prespecified protocol are described in the Supplementary files.
Results
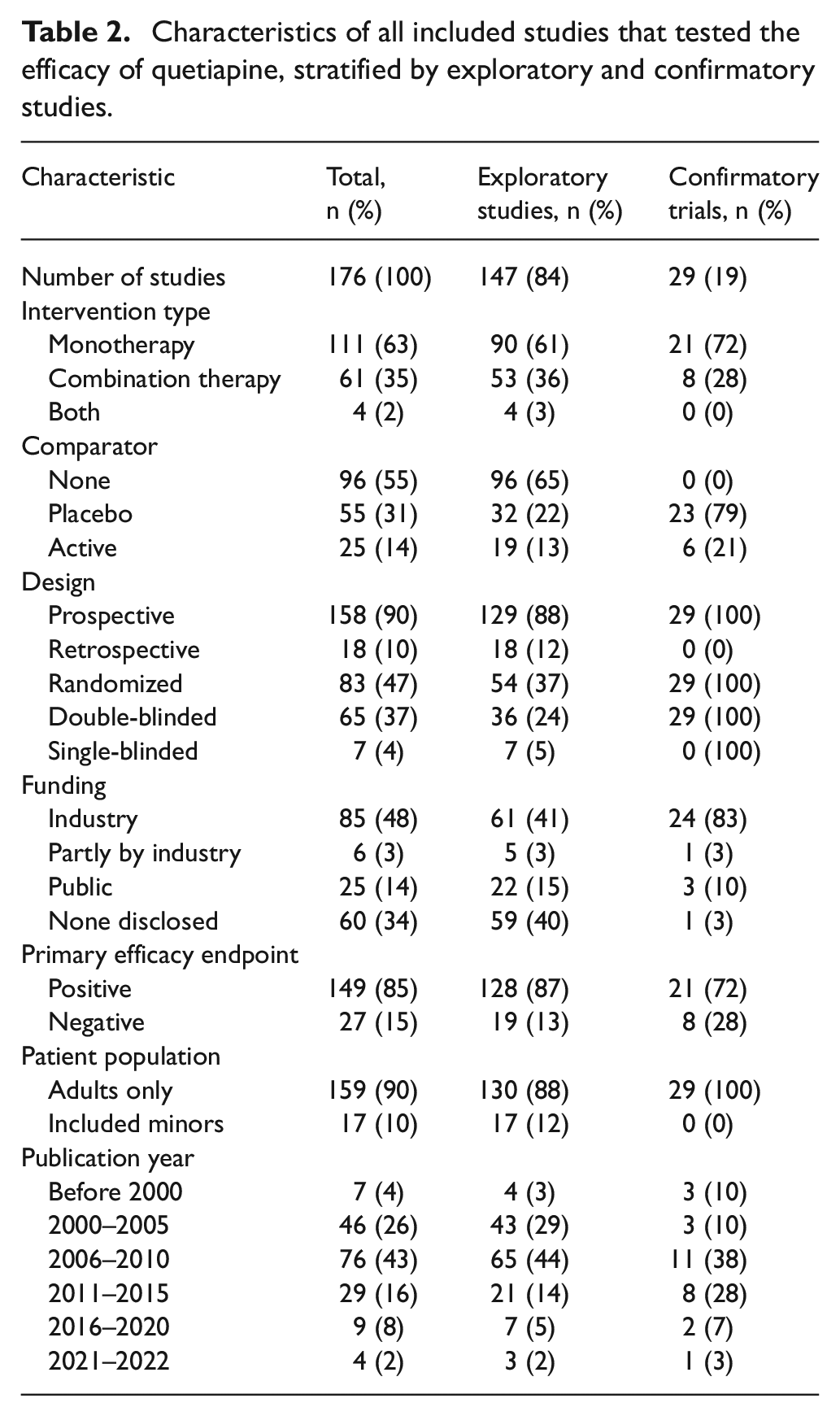
We identified 176 publications (included studies provided in Supplemental material) that reported efficacy outcomes for quetiapine in unapproved indications (see PRISMA diagram, Figure 1). Of these, 147 (84%) were exploratory studies and the remaining 29 (16%) were confirmatory. A total of 128 included exploratory studies (87%) had a positive efficacy endpoint compared to 21 (72%) for included confirmatory studies. Approximately half of studies were funded by industry (85 in total, 48%). Table 2 shows key characteristics of the sample of included studies, stratified by exploratory and confirmatory studies.
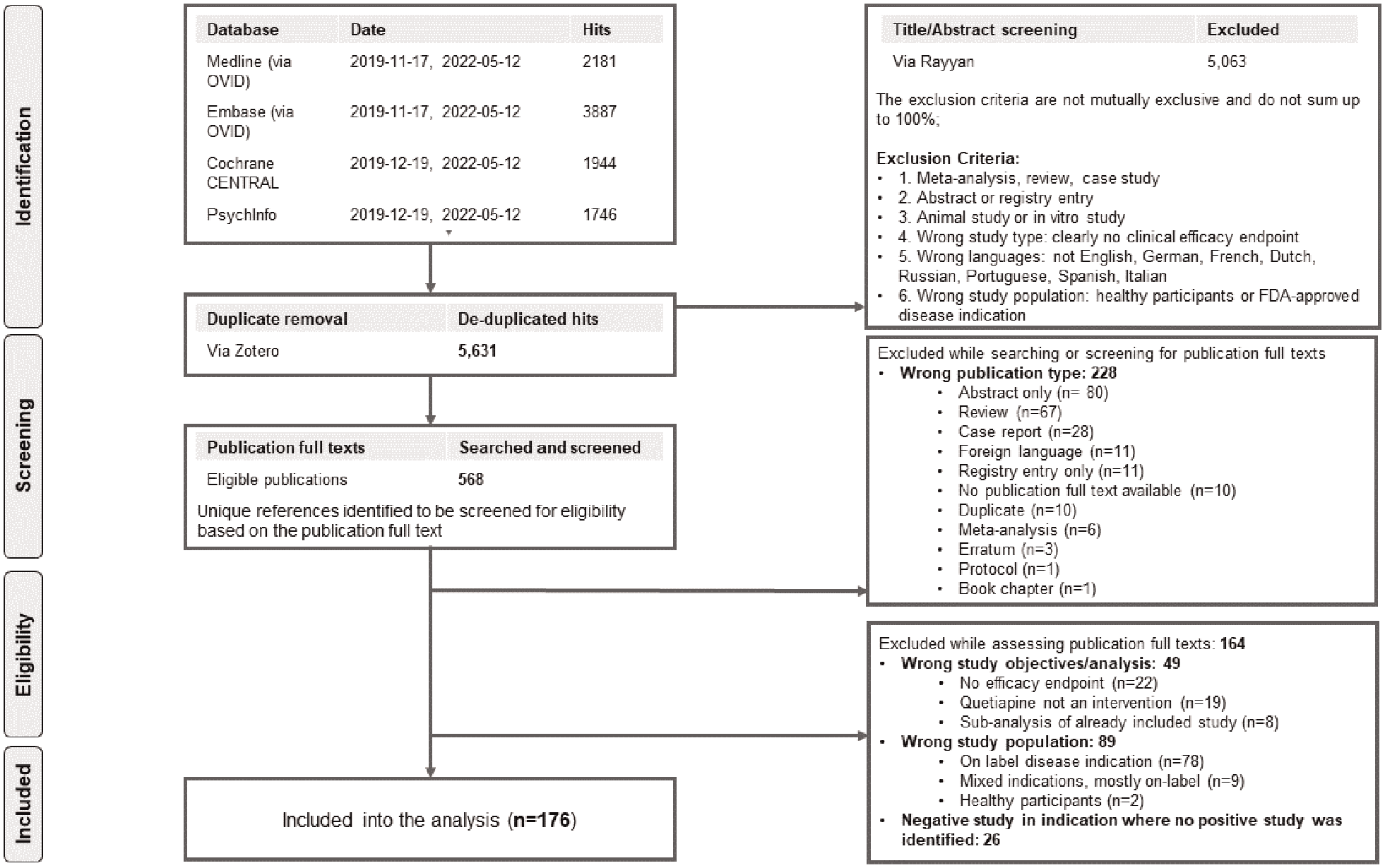
PRISMA flow diagram for included quetiapine studies.
Characteristics of all included studies that tested the efficacy of quetiapine, stratified by exploratory and confirmatory studies.
Quetiapine was tested in exploratory studies for 26 indications: 8 indications were tested in confirmatory trials, and regulatory approval was granted by the FDA for 3 of those. Early in the testing of quetiapine, the number of new indications with positive exploratory studies (dark line, Figure 2) exceeded the number of new indications in which confirmatory trials were published (lighter line, Figure 2). However, 18 indications (69%) were not tested in confirmatory trials.
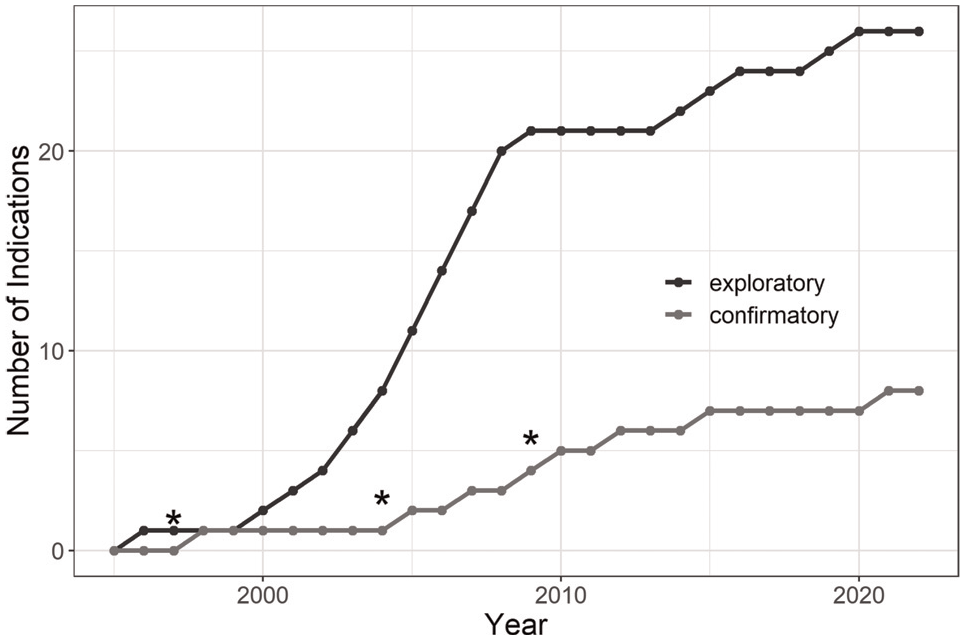
Cumulative number of indications with exploratory and confirmatory testing as a function of time, asterisks indicate years in which quetiapine received FDA approvals for new indications (1997 schizophrenia, 2004 bipolar disorder, 2009 major depressive disorder).
Primary outcome
In total, 24 of the 26 indications (92%) had at least 5 years of follow-up since the first publication of an exploratory study suggesting promise for an off-label use. For 16 of these (67%), we were unable to find any published trials aimed at confirming positive effects from exploratory studies (Figure 3).
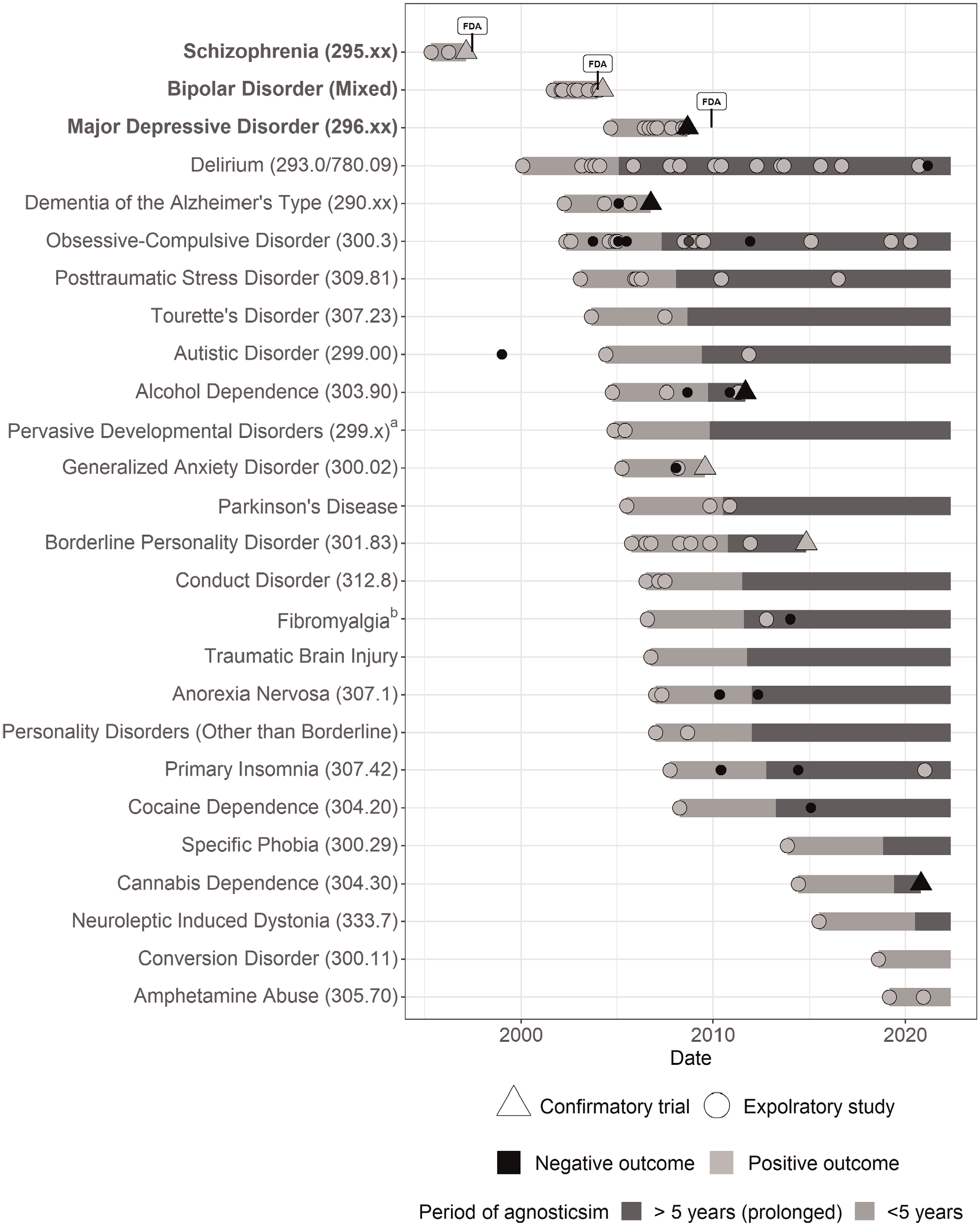
AERO diagram of the publications reporting the efficacy of quetiapine as a function of time, nodes represent published study reports ordered by publication date of first positive studies on the horizontal axis. The vertical axis presents indications as classified by Diagnostic and Statistical Manual of Mental Disorders (4th edition; DSM-IV). Indications for which quetiapine received FDA approval are displayed in the top three rows and the date of approval is labelled. Dark segments mark unaddressed clinical agnosticism within 5 years following publication of a first positive exploratory study in an indication. Periods of prolonged agnosticism (no confirmatory trial published more than 5 years after first exploratory testing) are marked in grey. Studies published after agnosticism that resolved in the respective indication are not displayed.
For example, quetiapine was reported as showing efficacy for treating Tourette’s disorder in a small clinical trial published in September 2003. 33 In the 18 years since, we were unable to find any published large double-blind, randomized trials confirming activity.
For bipolar disorder, efficacy was confirmed after grant of FDA approval in 2004. In the other two approved indications (schizophrenia and major depressive disorder), a confirmatory trial was published before FDA approval was granted. In only two off-label indications (9% of those with more than 5 years of follow-up, namely dementia of the Alzheimer’s type and generalized anxiety disorder), promise suggested by an exploratory study was tested in a confirmatory trial within 5 years of publication. For three indications (borderline personality disorder, alcohol dependence and cannabis dependence), we identified at least one confirmatory trial more than 5 years after the publication of a positive exploratory study. Hence, altogether, exploratory studies supporting off-label use of quetiapine were not promptly followed up with confirmatory testing for 19 out of 24 indications with adequate follow-up time (79%).
Additional searches for registered but not published confirmatory trials in these 18 indications in clinicaltrials.gov revealed two potentially confirmatory trials have not been published.34,35 One trial assessed quetiapine in cannabis dependence, and one is testing quetiapine in Parkinson’s psychosis with a completion date in October 2024. 35
Relationship of funding to exploratory testing
Of those indications for which there were at least 5 years between positive exploratory findings and a confirmatory trial or no confirmatory trial at all, eight (42%) began with a publication of an industry-only sponsored study, one study (5%) was supported by some industry sources, one (5%) was publicly funded and nine (47%) did not disclose a funding source. Confirmatory studies were more likely than exploratory studies to be sponsored by industry-only sources (83% versus 41%; Table 2).
Recommendations of quetiapine use in clinical practice guidelines
We identified nine clinical practice guidelines recommending the use of quetiapine in at least seven indications for which we could not identify confirmatory trials of quetiapine (for more details, see Table 3 and Supplemental Table 2).
Past clinical practice guidelines recommending the use of quetiapine in off-label indications without confirmatory testing.
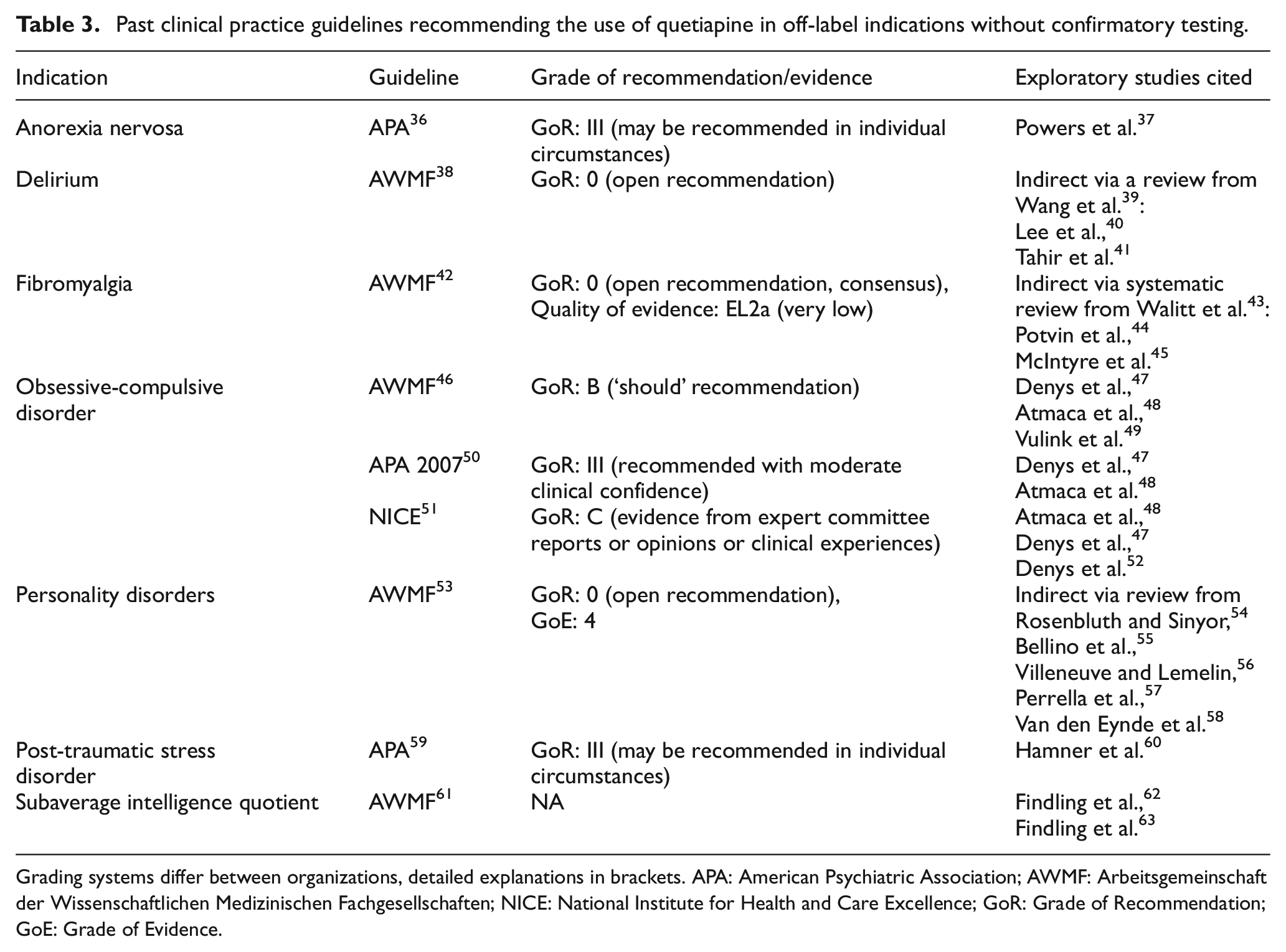
Grading systems differ between organizations, detailed explanations in brackets. APA: American Psychiatric Association; AWMF: Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften; NICE: National Institute for Health and Care Excellence; GoR: Grade of Recommendation; GoE: Grade of Evidence.
Sensitivity analyses
Defining studies with 30, 50 or 150 patients receiving quetiapine as confirmatory resulted in the same number of off-label indications associated with prolonged agnosticism (19/26, see Supplemental Tables 3 and 4).
Discussion
Between 1995 and 2022, quetiapine was reported as showing promising activity in small exploratory studies for at least 26 different indications and given FDA approval for 3 others. Of the remaining indications for which small studies suggested potential utility for off-label prescription, only eight were followed up with large, randomized, double-blinded clinical trials within 5 years of the initial report of promise. For example, in 2003, quetiapine showed promising efficacy as adjunctive treatment in an open-label trial of patients with PTSD. This study enrolled 20 veterans and found that quetiapine ‘may have efficacy in reducing PTSD symptoms’ in patients who did not adequately respond to prior treatments. However, we were unable to identify any large, randomized trials confirming this promise with at least 18 years of follow-up in either the published literature or in clinicaltrials.gov.
Such studies are likely to influence clinical practice by encouraging physicians and guideline developers to entertain the possibility of using quetiapine off-label – a phenomenon we call ‘clinical agnosticism’. Using a limited set of influential clinical practice guidelines, we identified nine documents recommending the use of quetiapine across seven indications for which we had identified exploratory testing that had not been followed up with a confirmatory trial. For example, a pilot-trial published in January 2007 found that quetiapine significantly decreases measures of anxiety and depression in outpatients with anorexia nervosa. While still in press, this study was referenced by the 2006 APA clinical practice guideline on eating disorders. 36 Although the guideline acknowledged the low quality of evidence, it stated that ‘quetiapine may improve […] associated symptoms’ in anorectic patients. For at least 14 years after this early positive signal, no confirmatory trials were published rejecting or supporting the use of quetiapine in this indication. The lack of confirmatory evidence for quetiapine to treat anorexia is echoed in a more recent AWMF guideline, yet prescription in clinical and ambulatory settings is still common. 64
The widespread use of quetiapine in off-label indications with limited evidence is well documented. While off-label quetiapine in a refractory patient in a controlled clinical setting suffering from schizophrenic or affective symptoms may be viewed as well justified, more problematic and extreme prescription behaviours have been linked to the context of family medicine.65,66 Common off-label indications that unconfirmed exploratory studies in our sample likely encouraged include insomnia,18,67 PTSD, 15 behavioural symptoms of dementia and substance misuse. 17
Industry seems to have played a role in fostering prolonged clinical agnosticism about off-label use of quetiapine. Of the 116 studies in which a sponsor was referenced, 85 were funded by industry. During the period when publication of exploratory studies in new indications surged, AstraZeneca (the manufacturer of quetiapine) was found to have ‘engaged doctors […] to conduct studies on unapproved uses of Seroquel’. 68 In 2010, the company signed a civil settlement to resolve these allegations by the United States and agreed to pay fine of US$520 million for off-label marketing.19,69
Our findings on the imbalance between post-approval exploratory research and confirmation are consistent with other reports. The majority of published reports on the clinical activity of eculizumab, a monoclonal antibody against complement C5 that received FDA approval for the treatment of rare haematological diseases, are small studies involving off-label indications. As with quetiapine, concerns that increased revenue from the drug based on off-label prescriptions have been voiced. 70 Pregabalin, a gabapentinoid approved for the treatment of specific seizures, neuropathic pain and fibromyalgia, showed promise in 27 exploratory studies for off-label indications. 21 Of these, 17 (63%) were not put into confirmatory testing within 5 years. Pregabalin was recommended for at least four of those indications in clinical practice guidelines 21 and is used extensively for off-label indications. 71
Our findings have several ethical and policy implications. First, many off-label indications in which quetiapine showed promising effects would likely not withstand confirmatory testing. Exploratory studies (like phase 2 trials in general) tend to use shorter observation periods, surrogate endpoints and are more prone to spuriously large effect sizes. 10 Quetiapine, though safer than other antipsychotics, nevertheless has side effects and costs. 72 Prescription absent confirmatory evidence makes it likely that quetiapine is often used ineffectively. Second, patients are exposed to experimental therapies in unapproved indication trials based on the expectation that positive results would later be advanced up the ladder of clinical development. Not following up on positive results disregards the contribution patients are making in these early studies. Third, our results suggest existence of publication bias in the published literature on the clinical use of quetiapine in off-label indications. In total, only 15% (27/176) of included studies were classified as negative. Moreover, in our sample, published confirmatory trials are more than twice as likely to be negative than exploratory studies (19/147, 13% versus 8/29, 28%). Last, the patterns of trialling for quetiapine suggest that research systems lack adequate safeguards against potential cooptation towards drug promotion. FDA maintains a policy of granting companies safe harbour for circulating reprints of trials describing off-label drug use. It states, ‘FDA does not intend to use [the] distribution [of scientific or medical journal articles] as evidence of the manufacturer’s intent that the product(s) be used for an unapproved new use’, provided certain conditions are met. One of these conditions is that the article derives from a peer-reviewed publication. FDA’s policy likely encourages companies to foster clinical agnosticism by conducting and publishing exploratory studies without corresponding confirmation.73,74
To mitigate the above concerns, we propose the following four measures. Regulatory authorities should reconsider safe harbour policies for reprint circulation to reduce the spread of reprints of small exploratory studies. Clinical practice guideline developers should be very cautious about grounding recommendations in post-approval exploratory studies, given their propensity for bias. When they do include them, they should clearly highlight missing confirmatory evidence when exploratory studies are used as the basis for recommendations. Given the high risk of bias for exploratory studies like those described above, they should consider sunsetting recommendations that are based on low-level evidence after 5 years. Residency programmes and medical training programmes should provide instruction in the critical assessment of study design, analysis, data quality and reporting so that physicians can form valid interpretations of exploratory studies. They should also sensitize students and trainees the ways exploratory studies, when performed in high volume as described here, encourage off-label prescription. Finally, research funders should support larger, confirmatory trials, especially in indications with high clinical relevancy and prolonged agnosticism. In funding decisions, they should also consider whether small trials, if positive, are unlikely to be followed up by confirmatory trials.
Our results have limitations. First, our study does not establish that a proliferation of unconfirmed exploratory results caused off-label prescription of quetiapine. We present direct evidence ascribing the publication of exploratory studies in our sample to a marketing campaign, and we have no way of knowing whether articles canvassed in our analysis were supplied by manufacturers to guideline developers. Second, our study should be interpreted in light of various methodological assumptions. For instance, to classify the very large and heterogenous set of studies, we used a minimal definition of ‘confirmatory’ testing. We did not assess factors such as choice of comparators or adequacy of outcomes. While there are likely no uncontroversial definitions of these concepts, we erred on the side of labelling agnosticism as having been addressed by picking a small sample size for defining a study as confirmatory. We considered the effect of negative exploratory studies on clinical agnosticism and showed that little negative evidence in off-label indications of quetiapine was published (13% of included exploratory studies had negative endpoints only). Meta-analyses and systematic reviews that include negative and positive exploratory studies in an indication might attenuate agnosticism generated by a single positive study. However, synthesizing trials of variable quality is no substitute for properly designed confirmatory trials. 75 In addition, high-quality meta-analyses are likely not available for many indications we identified. We regard it as unrealistic to expect busy physicians to always critically assess the strengths and weaknesses of exploratory studies producing conflicting results. Third, our analysis may have included studies enrolling unclear or mixed patient populations (e.g. ‘patients receiving SSRIs’) 76 or indications that are no longer relevant due to changing disease classification, thus overcounting indications with prolonged agnosticism. Anticipating this, we limited our primary analysis to studies where the patient population (a) could be subsumed under one specific disease code (such as DSM-IV) and (b) did not suffer from a comorbid on-label disease. This may have led to an undercount of agnosticism-generating trials. Fourth, our study did not consider confirmatory findings that were disseminated as abstracts or that went unpublished. ClinicalTrials.gov registry searches did not uncover a large number of confirmatory trials.
In summary, many small, post-approval trials suggested the efficacy of quetiapine for numerous off-label indications. These promising findings generally went unconfirmed in large, randomized trials years after first being published. The lack of coordination between exploratory and confirmatory studies, combined with the safe harbour for reprint circulation provided by regulatory authorities, likely encourages ineffective off-label treatment in many areas of medicine.
Supplemental Material
sj-docx-1-ctj-10.1177_17407745231225470 – Supplemental material for Research encouraging off-label use of quetiapine: A systematic meta-epidemiological analysis
Supplemental material, sj-docx-1-ctj-10.1177_17407745231225470 for Research encouraging off-label use of quetiapine: A systematic meta-epidemiological analysis by Peter Grabitz, Lana Saksone, Susanne Gabriele Schorr, Johannes Schwietering, Merlin Bittlinger and Jonathan Kimmelman in Clinical Trials
Footnotes
Acknowledgements
The authors thank Kerstin Müller for supporting this project with data extractions and Daniel Strech for commenting on the protocol and offering support throughout the project. They thank Deborah Zarin for input in an earlier draft. This project did not receive any funding.
Author’s note
J.S. and P.G. have accessed and verified the data, and all authors decided to submit for publication.
Author contributions
P.G., M.B., S.G.S. and J.K. were involved in study concept and design. P.G., L.S. and M.B. contributed to acquisition, analysis or interpretation of pilot data. P.G. and M.B. drafted the protocol. S.G.S., J.K. and L.S. carried out critical revision of the protocol for important intellectual content. P.G., L.S. and J.S. performed acquisition and analysis of study data. All authors participated in interpretation of data. P.G. drafted the article. All authors contributed to critical revision of the article for important intellectual content. P.G. contributed in data curation and statistical analysis. J.K. provided administrative, technical or material support and performed study supervision. P.G. is the Guarantor.
Declaration of conflicting interests
All authors have completed the ICMJE Uniform Disclosure Form at ![]() and declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
and declare no support from any organization for the submitted work; no financial relationships with any organizations that might have an interest in the submitted work in the previous 3 years and no other relationships or activities that could appear to have influenced the submitted work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project did not receive any funding.
Data sharing statement
Data extracted from the included sample of clinical studies will be made available. This concerns specifically data underlying Figures 2 and 3 as well as Table 2 and the study protocol including statistical analysis plan. Data will be made permanently and publicly available on the Open Science Framework for any use immediately following publication.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.