
Abstract
Background
Cancer clinical trials are vital for improving treatments. Clinical trial decision-making has been examined from the perspectives of patients and oncologists, but caregiver perspectives on clinical trials and roles in patient enrollment decisions remain understudied.
Methods
This scoping review assessed the state of current research on caregiver roles in cancer trial enrollment decision-making. A review of empirical literature was conducted in January 2024 using PubMed and Embase. Articles were evaluated using a review instrument to determine the aspect of decision-making evaluated, the roles of caregivers in clinical trial enrollment decision-making, and recommendations based on study results.
Results
A total of 23 articles were included in the review. Studies focused on awareness and attitudes about clinical trials (7 articles), hypothetical willingness to participate in a trial (6 articles), and experiences with decision-making (10 articles). Caregiver roles included supporting and deferring to patient autonomy, communicating with clinicians, and taking on burden to facilitate participation in the trial. Researchers recommended including caregivers in clinical trial enrollment discussions and educational outreach, developing interventions to reduce caregiver burden, and future research on caregiver clinical trial decision-making using the framework of relational autonomy.
Conclusion
Empirical research on caregiver roles in clinical trial enrollment decision-making is limited. Findings of this review suggest that caregivers experience tension between their perceived role of supporting the patient’s autonomy and their own well-being. More research is needed to understand how caregivers navigate these challenges and identify best practices for their inclusion in clinical trial consent.
Background
Patients often rely on support from caregivers during clinical trials (CTs), which may involve more frequent appointments and procedures. A caregiver is often defined as a person providing informal, unpaid care to a patient. This is usually a family member or spouse, but close friends may also be caregivers. Care provided may include assistance with activities of daily living, transportation, emotional well-being, and decision-making. 1 Owing to close involvement of caregivers, identifying the roles they play in CT enrollment decisions is important for ensuring informed consent and identifying unmet needs. Cancer CTs in particular can have significant implications for caregivers due to uncertain side effects and intensive study protocols. The impact of patient participation in cancer CTs on their caregivers has been recognized, particularly in early-phase CTs.2,3 Numerous studies have evaluated CT decisions from the perspectives of patients 4 and clinicians, 5 but the views of caregivers remain understudied despite intimate involvement in cancer care and decision-making.1,6 When surveyed about their decisional role preferences (active, shared, or passive), most advanced cancer patients preferred a “shared” role with physicians (42.5%) and family (49.6%). 7 An interview study of patients with cancer and their caregivers found that caregivers play a critical role in decision-making. The authors identified CT participation as a type of decision that merits further research. 8
The attitudes of caregivers toward cancer CT participation and roles they take during decision-making need to be identified to guide best practices for when and how to include them in informed consent. This article reports the results of a scoping review to evaluate existing empirical research on this topic. Scoping reviews aim to characterize the current state of research in a particular field and identify gaps in the literature. 9 Specifically, the goal of this review is to identify studies that assessed caregiver attitudes toward patient participation in CTs, caregiver roles in patient enrollment decision-making, and recommendations for caregiver inclusion in informed consent. Articles reporting results from studies that sampled cancer caregivers were included and categorized based on their methodology, aspects of decision-making evaluated, roles of caregivers in CT decision-making, and recommendations.
Methods
Search strategy
PubMed and Embase databases were searched for this review. Preliminary search terms were developed by an investigator with expertise in oncology research and bioethics. The search strategy was refined and implemented in January 2024 through consultation with a health science librarian at Case Western Reserve University. The search was conducted using a combination of the following search terms: family caregiver, informal caregiver, oncology, cancer, neoplasm, CT, randomized controlled trial, cancer trial, decision-making, informed consent, and participation. The terms “family caregiver” and “informal caregiver” were chosen to distinguish results from studies of healthcare providers, who are also often referred to as “caregivers.”“Informal caregiver” was included because not all caregivers are family members; close friends may also serve as a caregiver. The search terms were utilized in the following format for the initial search of PubMed: “((family caregiver) OR (informal caregiver)) AND ((cancer) OR (neoplasm) OR (oncology)) AND ((clinical trial) OR (randomized controlled trial) OR (cancer trial)) AND ((decision making) OR (informed consent) OR (participation)).” Reference lists of in-scope articles were searched to identify additional articles for inclusion.
Screening for eligibility
Figure 1 shows an overview of article screening and attrition. The search strategy yielded 612 results from the 2 databases. Results were initially screened by title to eliminate irrelevant topics, duplicates, and conference abstracts, which yielded 81 potentially eligible articles. Then, the next stage of screening involved reading abstracts and evaluating eligibility based on these criteria: (1) English language; (2) empirical research; (3) sampled caregivers of adult patients with cancer; and (4) evaluated decision-making or attitudes about the patient participating in a therapeutic CT.
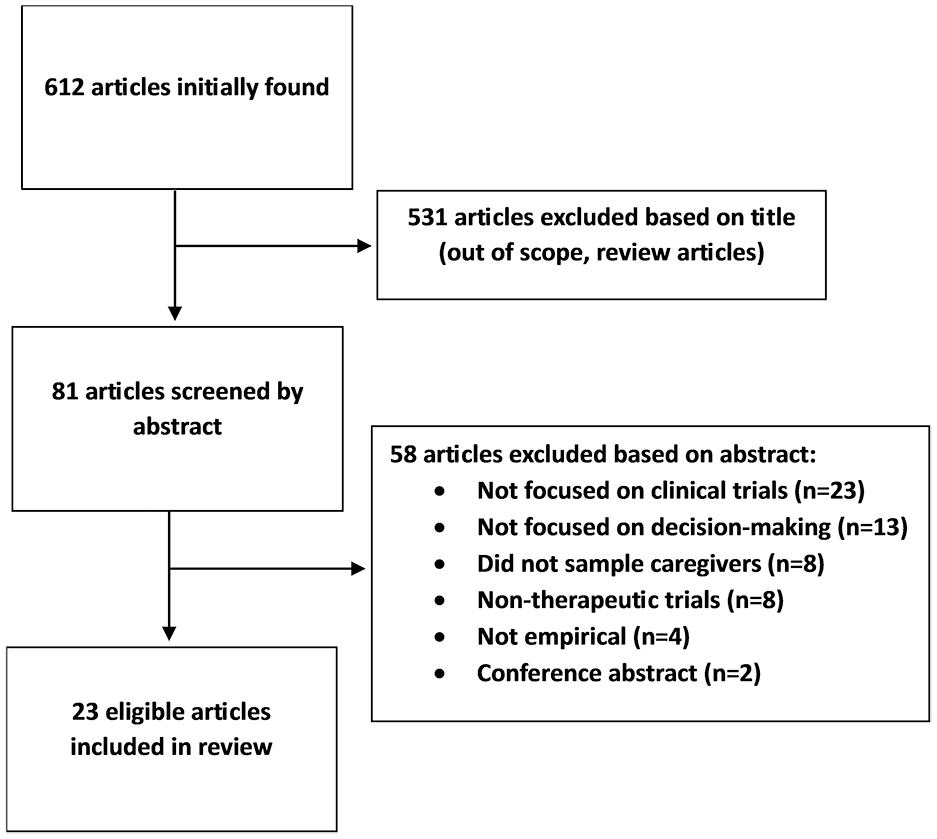
Article screening and attrition.
Several studies focused on the experiences of parents making decisions about CT participation for children with cancer. These articles were excluded because the goal of this review is to evaluate the roles of caregivers in CT enrollment decisions for patients who have decision-making capacity. Studies focused on caregiver quality of life or caregiving burden during CT participation without addressing decision-making were also excluded. In-scope studies published in English focused on any cancer diagnosis or caregiving relationship were included; narrowing eligibility further would not be feasible due to the relative lack of research on this topic. All articles were screened by ECB with borderline cases reviewed by BJD and SL to finalize eligibility decisions. Of the 81 abstracts evaluated, 23 articles were retained for the full-text review.
Full-text review and assessment
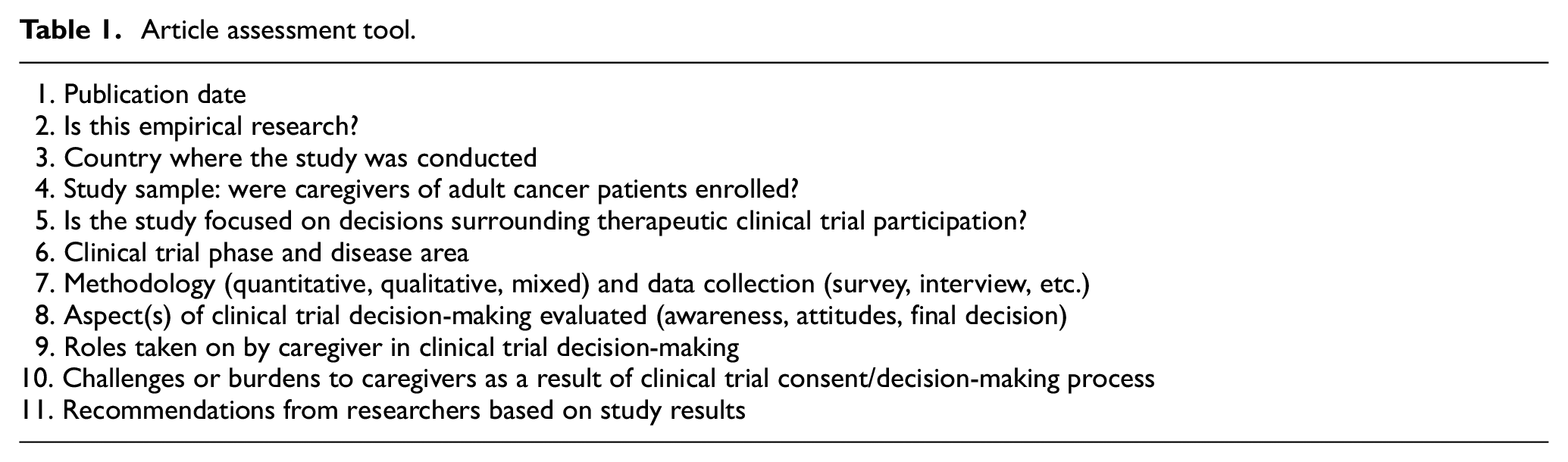
These 23 articles were read in full and evaluated using a structured tool (Table 1). The tool was developed to capture salient characteristics of each study and to categorize results and recommendations from the authors. Articles were categorized based on (1) which aspects of CT decision-making they evaluated, (2) the roles caregivers played in the decision, and (3) recommendations based on study results. When studies did not explicitly report on caregiver roles in CT decision-making, roles were inferred based on study findings (when possible) or categorized as “not assessed.” Data extraction and categorization were conducted by ECB with BJD and SL providing input on categorization decisions when studies could potentially fit into multiple categories.
Article assessment tool.
Results
Characteristics of the 23 eligible articles are shown in Table 2. Most studies (21 out of 23) defined caregivers broadly as anyone providing unpaid care or accompanying a patient to appointments. One study focused on spousal caregivers, 10 and another limited their definition to immediate family members. 11 Nine studies stated that incapacitated patients (and thus their caregivers) were ineligible to participate, while the remaining 14 studies did not explicitly address this. In our experience, inclusion of incapacitated patients in therapeutic cancer CTs is uncommon. Based on this and the fact that these studies did not mention caregivers making surrogate decisions for incapacitated patients, it seems unlikely that caregivers of such patients were included.
Eligible articles.
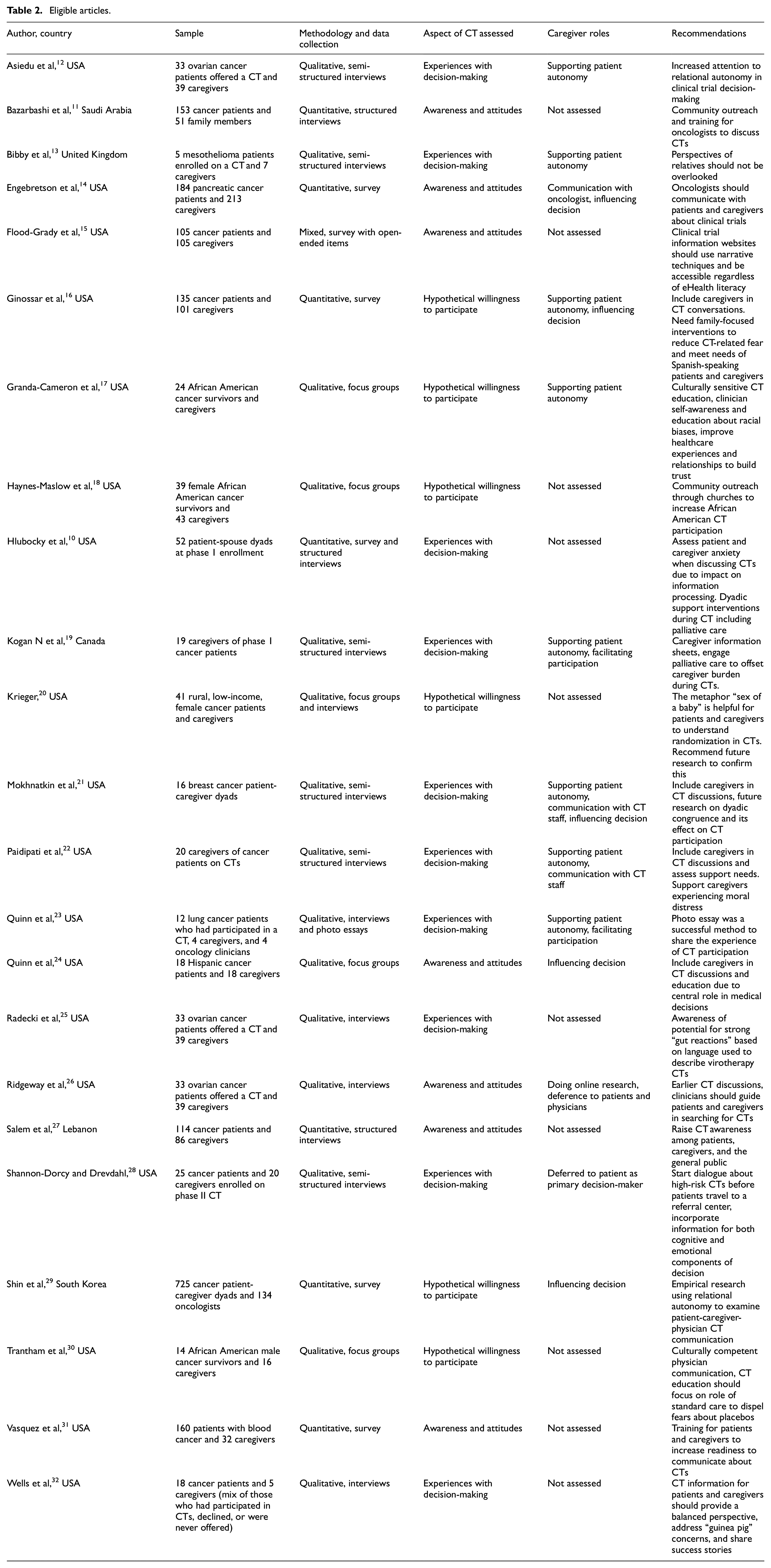
Studies examined three aspects of CT decisions: awareness and attitudes, hypothetical willingness to participate, and experiences with decision-making. These categories were developed after reviewing eligible studies and identifying the aspects of CT decision-making assessed by each. Seven studies evaluated preconceptions about CTs (attitudes and awareness) that one would bring to informed consent. The remaining 16 studies explicitly addressed a decision about the patient participating in a CT; these were separated based on whether the studies sampled caregivers of patients that made a real decision (10 studies) and those that asked about a hypothetical CT (6 studies).
Awareness and attitudes
Seven studies focused on awareness and attitudes about CTs. Two evaluated CT awareness in countries (Lebanon and Saudi Arabia) that do not have widespread CT availability and access.11,27 Using structured interviews of patients and caregivers, they found prevalent misconceptions about CTs and mistrust of randomization. They suggested raising awareness of CTs through community outreach and educating clinicians to communicate about CTs. Although these studies sampled caregivers, they did not focus on caregiver-specific issues and instead gave more general advice about raising CT awareness in their respective countries.
Next, Engebretson et al. surveyed patients with pancreatic cancer and their caregivers, finding that almost half (49%) had never discussed CTs with their oncologist. Caregivers were found to be the second most likely to raise the possibility of the patient participating in a CT (behind oncologists). Recommendations largely focused on encouraging oncologists to talk about CTs with their patients, but the authors acknowledge that caregivers likely play an influential role in treatment and CT decision-making. 14 Ridgeway et al. interviewed ovarian cancer patients and caregivers about their experiences searching for CTs. Caregivers reported feeling “unqualified” and were cautious about sharing information with the patient, fearing that it might be inaccurate. The authors suggested oncologists have earlier CT discussions and provide guidance for how to search for CTs. 26
Finally, three studies obtained feedback from patients and caregivers for educational tools. Quinn et al. conducted focus groups with Hispanic cancer patients and caregivers to develop a video intervention aimed at raising CT awareness. Participants reported low awareness and knowledge about CTs, and a preference for shared decision-making with their families and doctors. Based on their results, the authors planned to focus the video intervention on encouraging patients to ask their doctors about CTs and supporting their ability to make decisions with their families. 24 Flood-Grady et al. 15 tested comprehension of key CT information and assessed whether a cancer research website improved understanding. Both patients and caregivers had poor comprehension scores in several key areas. For example, 67% of patients and 77.2% of caregivers thought the goal of a CT was to “match people to the best treatment for them.” Vasquez et al. 31 evaluated online training to improve readiness of patients with blood cancer and their caregivers to discuss CTs. They found that CT knowledge increased, and participants reported greater readiness and intention to communicate about CTs with their clinicians. The study sample contained significantly more patients than caregivers (160 and 32, respectively), and caregiver data were not reported separately, limiting caregiver-specific conclusions. Overall, studies in this category had quite different aims; most recommended discussing CTs earlier and suggested including caregivers in those conversations.
Hypothetical willingness to participate
Six articles evaluated willingness to participate in CTs in a hypothetical context. Three studies focused on attitudes of African American patients and caregivers toward the patient participating in cancer research using focus groups. Participants expressed skepticism of research and mistrust due to potential conflicts of interest and historical abuses.17,18 Responses from caregivers were reported together with patients, so the caregiver role in decision-making was not discussed except for a finding from Granda-Cameron et al. 17 that “support from others” was reported as a facilitator to patient CT participation. Recommendations focused on building trust and knowledge of CTs through culturally sensitive CT education, community outreach, and communication with the physician.17,18,30 Ginossar et al. surveyed patients and caregivers at a minority-serving cancer center, finding similar willingness to participate in underrepresented compared to majority populations. Overall, caregivers were less likely to endorse CT participation compared to patients (50% and 65%, respectively). The authors concluded that families often have unmet CT information needs and suggest more family-focused interventions. 16
Krieger conducted focus groups with rural, low-income patients and caregivers and presented them with a decision to participate in a hypothetical phase III CT. The aims were to identify metaphors used by participants to describe the CT and to elicit feedback on common metaphors used to explain CTs during informed consent. Participants used the metaphors “trial and error,”“guinea pig,” and “last resort” to describe the CT. They disliked gambling metaphors commonly used to describe to randomization, such as “flip of a coin” or “roll of the dice.” Instead, they preferred the family-focused “sex-of-a-baby” metaphor to describe equal chance of allocation to study arms. 20 Shin et al. surveyed patient-caregiver-oncologist triads in South Korea, asking each to take on the role of a patient, caregiver, and oncologist in a hypothetical decision to participate in a phase I CT. Both caregivers and oncologists were more willing to recommend CT participation to a patient than they were willing to participate themselves when acting in the patient role. The authors recommend further empirical research to replicate these results during real rather than hypothetical CT decisions. 29
Experiences with decision-making
The remaining 10 articles sampled caregivers of patients who made an actual decision about CT participation. Two articles leveraged the CT decision-making experiences of patients and caregivers to elicit feedback about CT education projects. Quinn et al. 23 used interviews with patients and caregivers who participated in a lung cancer CT to create a photo essay project to share their stories and raise CT awareness. Only four caregivers were included, and the project was primarily focused on creating and evaluating the photo essays, limiting ability to ascertain caregiver decision-making roles. Wells et al. 32 conducted in-depth interviews and elicited feedback from patients and caregivers about a DVD titled, “Clinical Trials, Are They Right for You?” They included patients and caregivers who had participated in a CT, declined participation, or had never been offered a CT. For those that had made a decision about CT participation, they were asked about why they chose to participate or not. Again, only five caregivers were included and results were combined with patient data, limiting the ability to draw caregiver-specific conclusions.
Hlubocky et al. 10 conducted a survey of 52 patient-spouse dyads at phase I CT enrollment to examine associations between quality of life measures and expectation of therapeutic benefit. Spousal caregivers and patients with higher anxiety were found to have lower expectation of benefit from the trial. The authors recommend assessment of psychological symptoms due to their impact on CT decision-making and provision of concurrent palliative care during CT participation. Two articles reported results from an interview study of ovarian cancer patients who were offered a CT and their caregivers.12,25 Asiedu et al. reported that caregivers played a vital role in shaping the CT decision while still wanting the patient to “maintain the final say.” They recommend greater attention to relational factors in the informed consent process for CTs. 12 Radecki et al. 25 focused on patient and caregiver reactions to language in vaccine and virotherapy CTs, finding that certain terminology led to adverse “gut reactions” that may distort understanding of risks and benefits. These studies share rich qualitative data including direct quotes from caregivers regarding their decision-making experiences.
The nuanced caregiver role identified by Asiedu et al. of supporting patient CT enrollment decision-making without over-exerting influence was supported by several qualitative studies. Kogan et al. interviewed caregivers of patients participating in phase I CTs to understand their role in the patient’s decision to enroll. Caregivers reported deferring to patients during the CT decision despite most endorsing a more collaborative approach to other, non-medical decisions. They supported the patients’ autonomy by gathering information and weighing pros and cons. Caregivers also reported setting aside reservations about the patient enrolling in the CT and taking on significant burdens to facilitate participation. 19 Paidipati et al. observed a similar phenomenon when interviewing caregivers of CT participants. They identified the theme “Caregiver Moral Distress” of which disagreement over CT decision-making was a component. Caregivers wanted to advocate for their loved ones but experienced moral distress due to fear that they were “taking agency away” if they overstepped. 22 Through interviews with mesothelioma patients participating in a CT and their caregivers, Bibby et al. 13 similarly found that caregivers expressed concerns about side effects and regret about the patient participating, but still supported the patient’s decision. An interview study by Mokhnatkin et al. compared breast cancer patient and caregiver perspectives on CT decision-making. Caregivers described their roles as a “liaison” between the patient and CT staff or a “touchstone” to validate the patient’s choice regarding enrollment. Several patient-caregiver dyads disagreed about how much influence the caregiver had over the final decision, with different patients recalling lower and higher levels of caregiver influence than their caregivers reported. 21 Shannon-Dorcy and Drevdahl interviewed patients participating in a phase II hematopoietic cell transplant CT and their caregivers to understand how they decided to participate. The majority of patients (92%) and caregivers (75%) had already decided to participate in the CT prior to the informed consent discussion. 28 Overall, studies that explicitly assessed the caregiver role in CT decision-making found that caregivers view supporting the patient’s autonomy as highly important, even when doing so involves taking on additional burdens or suppressing their own concerns about the patient participating in the CT.12,13,19,21,22
Discussion
Caregiver roles in CT decisions
These studies build on the existing CT literature by including caregivers as significant stakeholders in CT decisions. In the awareness and attitudes category, caregivers were found to be more likely than patients to raise the idea of CTs 14 and were recognized as important targets for CT outreach and education.11,14,24,26,27 Caregiver-focused CT education and communication were also recommended based on studies assessing hypothetical willingness to participate in CTs, particularly because caregivers exhibited lower willingness than patients. 16 The attitudes of caregivers toward CT participation were somewhat inconsistent between studies, with two studies finding caregivers to be more likely to bring up CTs 14 and more willing to participate if they were a patient, 29 yet Ginossar et al. 16 found that caregivers were less likely to support CT participation than patients. These inconsistent findings may reflect differences in the populations studied or could be a results of the hypothetical context in which these studies evaluated CT decision-making.
When recalling actual CT decisions, multiple studies found that caregivers viewed their roles as supporting patient autonomy and facilitating communication.12,21 They sought to help the patient make a better decision by weighing pros and cons, yet were cautious about exerting too much influence and wanted the patient to make the final choice. This created challenges when caregivers were concerned about risks and side effects, yet still wanted to support the patient’s autonomy.13,19,22
The roles of caregivers in enrollment decisions for CTs have been recognized in other fields such as neurology. 33 Similar caregiver roles have been identified for neurology CTs, including assistance with enrollment decision-making and facilitating protocol adherence. 34 Caregivers are often included (and may be required) as “study partners” in neurology research to provide proxy consent and assist with adherence due to the prevalence of patient cognitive impairment.33,34 Based on waxing and waning decision-making capacity in patients throughout the course of illness, the notion of “interdependent decision-making” has been formulated as a way for caregivers to reinforce the patient’s ability to make decisions when possible rather than taking over as a surrogate decision-maker. 35 This model is consistent with roles of caregivers identified in this review—caregivers sought to improve the patient’s decision-making ability rather than superseding the patient’s decisional authority.
Limitations of current studies
The current empirical literature on caregiver roles in CT decisions is limited in several ways. Although all studies included in this review sampled caregivers, most (21 out of 23) included a combination of patients and caregivers. While this approach can be advantageous if used to compare patient and caregiver perspectives as Mokhnatkin et al. 21 did, many studies combined the patient and caregiver results. This limited analysis of caregiver-specific concerns and ability to evaluate differences in decisional role based on phase of CT or caregiving relationship. Several studies also had significantly more patients than caregivers in their samples, diluting caregiver perspectives.11,23,31,32 While all articles included in this review evaluated some aspect of caregiver involvement in CT decision-making, their aims varied widely. The goals of these studies ranged from evaluating awareness of CTs to eliciting feedback on specific CT education initiatives. These factors made it difficult to compare findings across studies or ascertain what role caregivers played in CT decision-making.
Six studies assessed CT decision-making in a hypothetical context, which is a major limitation. Decision-making research shows real and hypothetical decisions can be made very differently. 36 Real-world decisions can involve time pressure, stress, and other influences that a hypothetical vignette would not reproduce. 37 Hlubocky et al. 10 illustrated this by showing that anxiety affected expectations of therapeutic benefit from CTs. These considerations underscore the importance of real-world CT decision-making research.
CT decision-making and caregiver burden
Several studies found that caregivers suppress their own concerns and take on burdens to support patient autonomy and facilitate CT participation.12,13,19,21,22 Indeed, multiple studies have evaluated the impact of CT participation on caregivers. Phase I trials can be particularly burdensome; participation has been shown to result in significant emotional, financial, and logistical burden for caregivers.2,3,38 To lessen caregiver burden during CTs, the researchers recommended support and education from clinicians, referral to online and community resources, palliative care, psychological support, and financial assistance.2,3,38
These foreseeable risks for caregivers could also raise the bar for their inclusion in decision-making for such CTs. While findings from Asiedu et al. 12 suggest that caregivers would prefer to let patients make the final decision, the moral distress reported by caregivers in the Paidipati et al. 22 study suggests that they struggle in this role and may prefer to exert more influence over decision-making in certain situations. Identifying the appropriate role and degree of influence for caregivers in CT decisions will require research to explicitly address these issues.
Recommendations for future research
Three articles in this review explicitly endorsed relational autonomy to guide research on caregiver involvement in CT informed consent.12,22,29 In relational autonomy, an individual is viewed through the lens of their relationships to others and society at large. 39 This framework recognizes that interpersonal connections and social roles are integral to a person’s identity and decision-making. 40 Future research should use this framework to understand how caregivers view their own autonomy when they defer to patients in CT decisions, and potential sources of decisional, emotional, and logistical support that may lessen burdens of CT participation on caregivers. This could include development and testing of shared decision-making interventions that promote caregiver involvement.
Research comparing patient experiences with CT informed consent and participation among those with and without a caregiver would also be beneficial to fully characterize the impact of caregiver support in CTs. Based on the caregiver roles identified by studies in this review, variables of interest for such research would include patient comprehension of CT information, participation rates, quality of life, and protocol adherence. Finally, future studies could compare caregiver decision-making roles across CT phases or cancer diagnoses to identify best approaches for different communities.
Limitations
The scope of this review is limited by the focus on therapeutic cancer CTs. While the narrow scope excluded research examining caregiver roles in decisions in other areas such as neurological research, 34 it allowed for comparison of relatively homogeneous CT decisions. Scope was also limited to caregivers of adult patients with decision-making capacity; thus, several studies evaluating proxy decision-making for pediatric cancer CTs were excluded. Caregivers already have a legally (and ethically) recognized role in pediatric research participation decision-making, and the distinct issues raised by proxy decision-making for research participation have been characterized. 41 Thus, this review evaluated the state of research identifying the roles of caregivers in CT enrollment decisions for adult patients with capacity.
Conclusion
Results of these studies highlight the important roles caregivers take on during CT decision-making. The tension between their perceived role in supporting the patient’s autonomy and their own reservations about CT participation needs further exploration. While families regularly navigate decisions that impact one another, participation in medical research is a type of decision that merits additional protections. It is likely not appropriate to require caregiver involvement if a patient is unwilling, or to give caregivers the authority to “veto” a patient’s decision to participate in a CT. However, there may be ways to more formally include caregivers in CT decisions without allowing their authority to stifle patient autonomy. Indeed, previous research has shown that caregivers experience moral distress when their needs diverge from those of the patient. 42 The study by Paidipati et al. 22 showed that moral distress can be a factor in CT decision-making as well, making it unlikely that they would want such authority. Further research and ethical analysis are needed to identify the proper method of including caregivers in CT decisions given the risks and burdens they incur.
Footnotes
Acknowledgements
The authors thank Stephanie Diaz, MLIS, librarian at the Cleveland Health Sciences Library of Case Western Reserve University, for assisting with the development of the search strategy.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.