
Abstract
Background/Aims:
The Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results trial randomized patients with diabetes to liraglutide or placebo. The per-protocol analysis conditioned on post-baseline adherence and therefore lacked a well-defined estimand. This study sought to evaluate a subset of Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results to estimate the effect of sustained liraglutide exposure corresponding to a well-defined per-protocol analysis.
Method:
We used the roadmap of targeting learning to define the estimand for the sustained treatment analysis and estimated it with longitudinal targeted minimum loss-based estimation, accounting for protocol deviations and censoring using post-baseline confounders. The results were compared to the intention-to-treat analysis. We report 3.5-year risks of the primary composite outcome (myocardial infarction, stroke, or cardiovascular mortality) and secondary outcomes (each of the primary outcome’s components, revascularization, unstable angina pectoris, heart failure, and all-cause mortality).
Results:
The intention-to-treat analysis estimated 3.5-year risks for the primary composite outcome of 11.8% (95% confidence interval: 10.8 to 12.8) in the liraglutide arm and 13.3% (95% confidence interval: 12.3 to 14.3) in the placebo arm, with a risk difference of 1.5% (95% confidence interval: 0.1 to 2.9). Accounting for post-baseline confounders, the sustained treatment analysis estimated 3.5-year risks of 11.4% (95% confidence interval: 10.4 to 12.5) for sustained exposure to liraglutide versus 12.6% (95% confidence interval: 11.5 to 13.7) for sustained exposure to placebo, yielding a risk difference of 1.1% (95% confidence interval: −0.4 to 2.6). Sustained exposure to liraglutide showed no statistically significant difference compared with sustained exposure to placebo for any secondary outcomes at 3.5 years.
Conclusion:
We used contemporary methods for causal inference to define and estimate the sustained treatment effects of the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results study by accounting for both baseline and time-varying confounders. The results were consistent with the findings of the original Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results trial.
Introduction
The LEADER (Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results) trial (2010–2015) demonstrated that the glucagon-like peptide-1 receptor agonist liraglutide reduces cardiovascular event rates in patients with type 2 diabetes mellitus compared to placebo. 1 The main analysis was the intention-to-treat analysis. In LEADER, the trial protocols encouraged comprehensive management of diabetes and cardiovascular risk factors, including treatment of high blood pressure, lipid levels, and glycemic control guided by HbA1c targets. Non-adherence to treatment and placebo and differential use of co-medications occurred during the trial. Non-adherence affects the intention-to-treat analysis because non-adherent patients often differ systematically in ways that influence outcomes. Hence, supplementary analyses are warranted.
A per-protocol analysis aims to estimate the effect of treatment had all participants adhered to their assigned regimen. However, the LEADER trial’s per-protocol analysis 2 did not explicitly define the estimand. It used an ad hoc estimation procedure that included only patients that adhered to assigned treatment. However, removing people from the analysis by conditioning on their post-baseline non-adherence is a statistical flaw. 3 Specifically, the per-protocol analysis “included only follow-up data from participants exposed to treatment plus 30 days, considering participants unexposed when drug holidays exceeded 120 days.” 2 These decisions reduce the validity and generalizability of the findings. 4
To address these challenges, we apply causal inference techniques to define and estimate estimands that capture the effects of sustained liraglutide treatment over time. 5 Specifically, we define sustained treatment as the combination of treatment adherence and absence of drop-out and the estimands as contrasts of outcome risks under sustained treatment. We use the longitudinal targeted minimum loss-based estimator (LTMLE), which uses machine learning to minimize modeling assumptions and sequentially updates Robins’ iterative conditional expectation estimator, 6 with models for the propensity of treatment adherence and censoring to achieve double robustness and efficiency, incorporating baseline and post-baseline confounder information.7,8 This method enables estimation of the outcome risks under sustained treatment, yielding clinically interpretable and policy-relevant insights. By examining the long-term benefits of sustained exposure to liraglutide, we provide insights into treatment consequences that can provide valid sensitivity analyses for the intention-to-treat analyses.
Methods
Data sources and study population
The population and variable definitions have been described elsewhere. 1 Compared to the original LEADER trial analysis, a subset of participants was excluded from the present re-analysis due to anonymization procedures and country-specific requirements. Time zero was defined as the date of randomization. The overall trial duration was planned to include an 18-month recruitment period, followed by a 42-month long study period from the randomization date of the last participant, resulting in a maximum of 60 months on the assigned regimen for the first included participant. In the LEADER trial, patients were scheduled for follow-up visits at months 1, 3, and 6 and every 6 months thereafter.
Estimand
In our analyses of the LEADER trial, we define the estimand as the expected 3.5-year risk of the composite outcome, if hypothetically all participants had fully adhered to the following regimens:
Sustained exposure to liraglutide: Participants maintain liraglutide treatment for at least 50% of the days between scheduled trial visits (at 1 month, 3 months, and every 6 months thereafter until month 42).
Sustained exposure to placebo: Participants maintain placebo treatment for at least 50% of the days between scheduled trial visits (at 1 month, 3 months, and every 6 months thereafter until month 42).
We assume that treatment interruptions of up to 50% of the time between visits would not compromise the drug’s potential effects. In supplementary analyses, we vary the threshold which defines the maximum duration of treatment interruptions. Note that the LEADER trial protocol stated that participants with accumulated interruptions of up to 120 days were still considered on treatment. 2 Note that drop-out and end of follow-up are not allowed before the end of the 3.5-year long study period. Non-cardiovascular mortality is a competing risk which naturally truncates the study period without violating the adherence to the regimens. However, the interpretation of the estimand is affected by potential differences between the regimens regarding the risks of non-cardiovascular mortality: the lower the risk of non-cardiovascular mortality the longer is a person at risk for the composite outcome and hence the higher the risk of the composite outcome. Identification of the estimand from the observed data relies on the following assumptions: (1) no unmeasured confounding: all information that predicts deviations from the regimens, including drop-out and end of follow-up, is available through measured baseline and post-baseline covariates; (2) positivity: the probability of adherence to a regimen including no drop-out and no end of follow-up is strictly larger than zero for all eligible persons; (3) consistency: there is no interference between trial participants and there is only one way to administer the treatments. A formal potential-outcome-based definition of the estimand and additional identification details are provided in Supplementary Material S2.
Outcome
The primary outcome was a composite of cardiovascular death, nonfatal myocardial infarction, or nonfatal stroke (major adverse cardiovascular event (MACE)). Secondary outcomes included each component of the primary composite event as well as unstable angina pectoris, revascularization, heart failure, and all-cause mortality.
Variables
For the primary sustained treatment, follow-up time was discretized into intervals aligned with the visit schedule of the LEADER trial. The first three intervals were 0–1, 1–3, and 3–6 months. Thereafter, follow-up was partitioned into consecutive 6-month long (183 days) intervals (6–12, 12–18, 18–24 months, and so forth) up to 36–42 months.
Treatment
In the primary sustained treatment analysis, patients were categorized as exposed to liraglutide or placebo during a given interval if they received the assigned treatment for at least half of that period. Patients were categorized as unexposed if their treatment usage was less than 50% of the interval. Due to the trial design, participants randomized to the placebo group did not have access to liraglutide treatment and vice versa.
Baseline patient characteristics
Baseline information included the following variables based on the participant’s first visit: sex (male vs female), age group (40–60, 60–80, and 80–90 years), diabetes duration (≤11 years vs >11 years), ethnicity (Hispanic or Latino vs other), estimated glomerular filtration rate using the Chronic Kidney Disease Epidemiology Collaboration (CKD-EPI) method, body mass index (BMI: ≤30 kg/m2 vs >30 kg/m2), and HbA1c (%). Concomitant medications, including glucose-lowering agents, were recorded at baseline using Anatomical Therapeutic Chemical codes listed in Supplemental Table S1. Non-fatal outcomes experienced before baseline and pre-existing comorbidities were included and categorized as detailed in Supplemental Table S2.
Post-baseline variables
The main analyses used a discretized time scale where intervention nodes were set at the scheduled trial visits of the LEADER trial. All time-varying covariates were mapped to the discretized time scale using summary statistics of the data within each interval (see Supplementary Material S3). Glucose-lowering co-medication use recorded after baseline at trial visits was categorized as present or absent in each interval based on any exposure during the interval. Insulin exposure was evaluated as either single-day exposure or longer. Similarly, adverse events of nausea or vomiting and diarrhea were defined as present or absent at post-baseline times according to exposure in each interval. HbA1c levels (in %) were recorded as the most recent measurement before the end of each interval, along with the change compared to the most recent previous HbA1c measurement. Atrial fibrillation and all non-fatal outcomes were defined as post-baseline confounders and categorized as not, newly, or previously occurring based on their occurrence within each interval. Additional technical details on the discretization and classification of time-varying treatment and time-varying covariates are provided in Supplementary Material S3.
Statistical methods
Time zero for all analyses was defined as the date of randomization. The reverse Kaplan–Meier method was employed to estimate the median potential follow-up time, to characterize the study’s follow-up capacity independently of mortality. 9 The Aalen–Johansen estimator 10 was used was used on the discretized time scale of the primary analysis to estimate the probability of a first treatment interruption, accounting for the competing risks of a primary outcome event and all-cause mortality. At each visit time, we show the cumulative probabilities of being adherent and not lost to follow-up (censored) for participants who were still at risk and adherent to the treatment regime at the previous visit time.
In the intention-to-treat analysis, the Aalen–Johansen estimator was applied to estimate the risk of the primary outcome while accounting for the competing risk of non-cardiovascular mortality. We applied the roadmap of targeted learning and the primary analysis of the sustained treatment estimand was performed with longitudinal targeted minimum loss-based estimation (LTMLE). 5 At each time point on the discretized time scale, the LTMLE algorithm modeled the treatment propensity and the probability of remaining uncensored. Robins’ sequential iterative regression algorithm was applied with a doubly robust TMLE update step to estimate the risk of the primary outcome under the treatment regimens of the sustained treatment estimand. 6 At each time interval, an ensemble super learner 11 used all available information up to the previous interval defined by baseline covariates, treatment variables, and the most recent post-baseline covariates to estimate the propensity of treatment, the censoring probability, and the outcome risk in the interval. By using information only from previous intervals, we avoid conditioning on the future. Each super learner included five learners: LASSO, elastic net, ridge regression, 12 xgboost, 13 and random forest. 14 Propensity scores and censoring probabilities were not truncated. 15 Additional details on the mathematical formulation specification of the estimand and a nonparametric structural equation model which details the dependencies and the assumed temporal ordering of treatment, covariates, and outcomes in our estimation procedure are provided in the Supplementary Material. The primary analysis was repeated for all time horizons on the discretized time scale (1, 3, 6, 12, 18, 24, 30, 36, and 42 months after randomization). All analyses were performed with the R software (version 4.2.1). 16 For the main analyses, we used the R package rtmle which is available at https://github.com/tagteam/rtmle/.
Supplementary analyses
In supplementary analyses, we varied the threshold defining sustained exposure to liraglutide and placebo in the estimand definition between 0% and 90%. Sensitivity analyses explored different levels of granularity in the discrete time grid, including coarser intervals (6 months) and finer intervals (3 and 1 months). In addition, we repeated the analyses using truncation of the estimated treatment probabilities to assess the impact of extreme weights. Finally, we conducted a supplementary analysis in which the main analysis was repeated using an ensemble super learner approach.
Data availability statement
The data that support the findings of this study are owned by Novo Nordisk and are not publicly available due to confidentiality and data protection agreements. Qualified researchers may request access to the data through Novo Nordisk’s data sharing program, in accordance with applicable policies and procedures.
Results
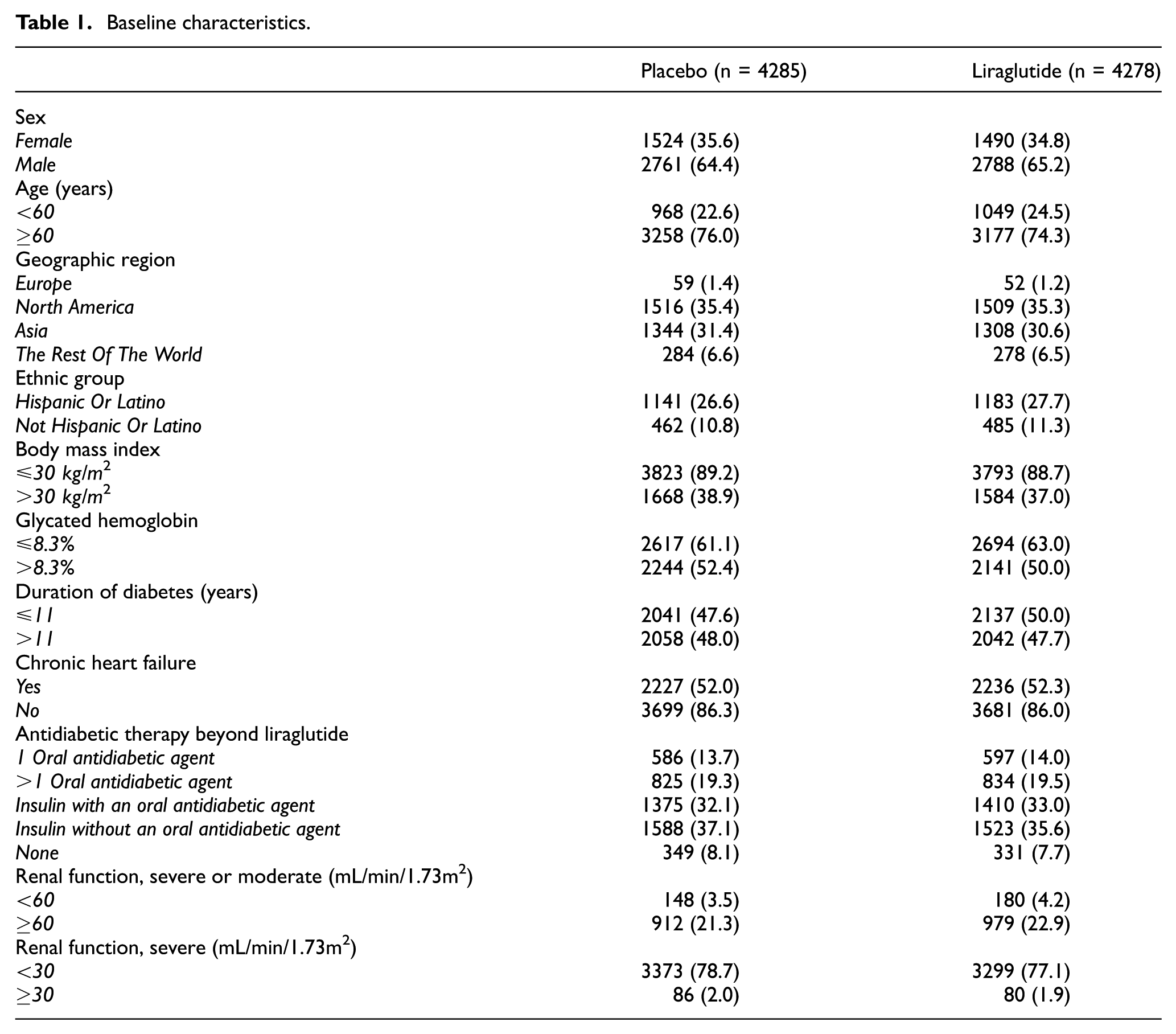
Our analysis included 8563 individuals after exclusion of 777 individuals from the original dataset. Of these, 4278 were randomized to liraglutide and 4285 to placebo. For the sustained treatment analysis, two individuals were excluded due to missing post-baseline HbA1c levels. The median potential follow-up time was 3.85 years in both arms. The baseline characteristics of our subpopulation were comparable to those of the original cohort with key demographic and clinical factors balanced between the randomization groups (Table 1). The cumulative probabilities of adhering to treatment regimen and being uncensored over the follow-up period were bounded away from zero for both regimens of the primary sustained treatment analysis (Supplemental Figure S1).
Baseline characteristics.
Primary outcome
Estimating the risk of the primary composite event for the sustained treatment analysis at 3.5 years, while accounting for reported pre- and post-baseline confounders, the regimen of sustained exposure to liraglutide had a risk of the primary composite event of 11.4% (95% confidence interval (CI): 10.4 to 12.5). In contrast, the regimen of sustained exposure to placebo had a risk of the primary composite event of 12.6% (95% CI: 11.5 to 13.7). This yielded an absolute risk difference of 1.1% (95% CI: −0.4 to 2.6, p = 0.14). The estimated risks of the primary composite outcome for each regimen at the planned trial visits are shown in Figure 1(a). The intention-to-treat analysis revealed a 3.5-year risk of the primary outcome of 11.8% (95% CI: 10.8 to 12.7) for the liraglutide initiators and 13.3% (95% CI: 12.3 to 14.3) for the placebo initiators, resulting in a 3.5-year risk difference of 1.5% (95% CI: 0.1 to 2.9) (Figure 1(b)).
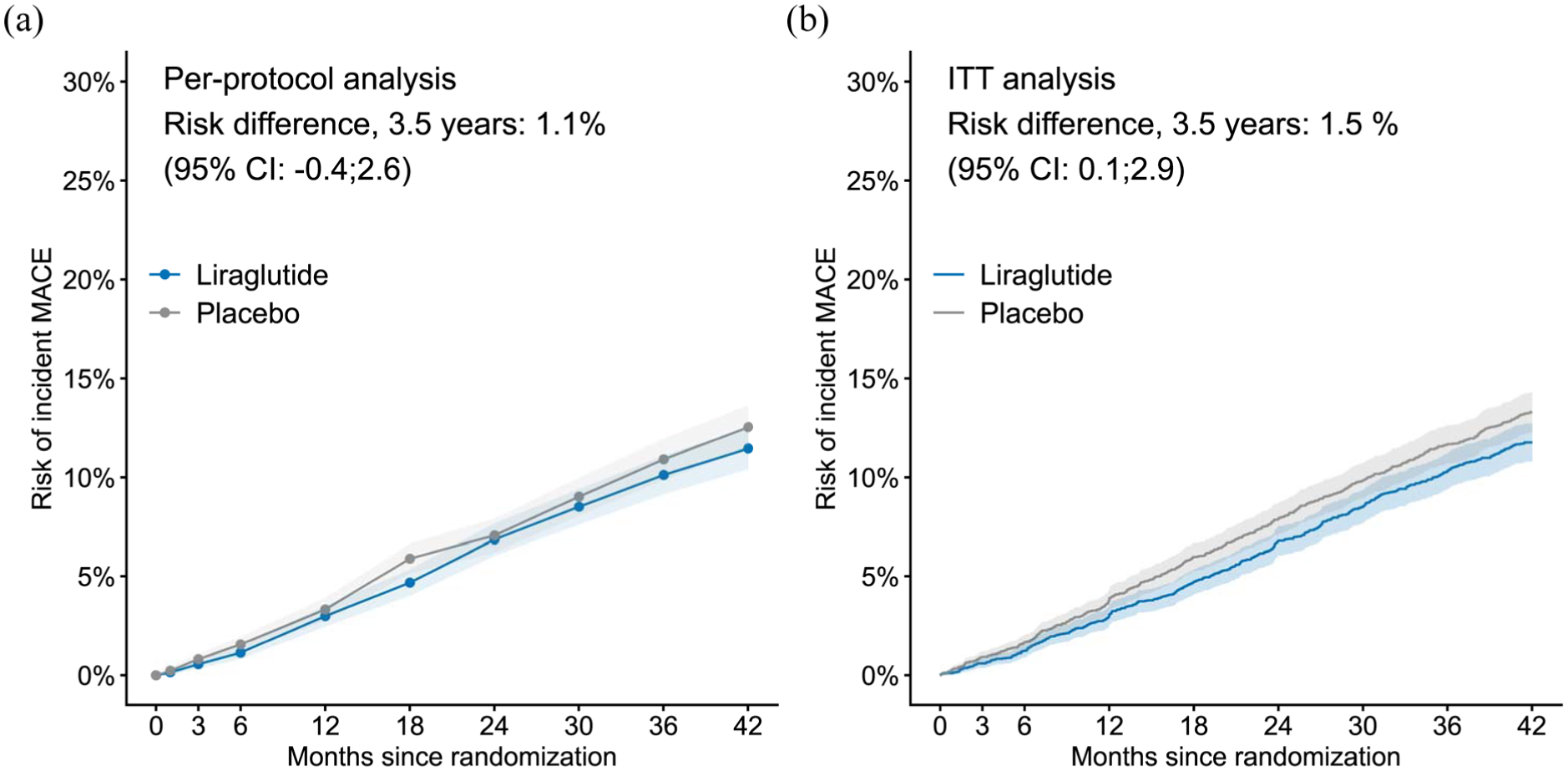
Risk of the primary composite outcome (myocardial infarction, stroke, or cardiovascular mortality). (a) The risk under the liraglutide and placebo regimen estimated by Targeted Minimum Loss-based Estimation. (b) The risk estimated with the Aalen–Johansen method according to the intention-to-treat principle.
Secondary outcomes
At 3.5 years, the regimen of sustained exposure to liraglutide showed no significant difference compared to the regimen of sustained exposure to placebo for all secondary outcomes; myocardial infarction, stroke, revascularization, unstable angina, heart failure, cardiovascular disease mortality, and all-cause mortality. The estimated risks for the primary outcome and all secondary outcomes in each regimen are shown in Supplemental Figure S2. Risk differences at 3.5 years are shown in Supplemental Figure S3.
Treatment adherence
The original publication reported treatment discontinuation rates of 9.5% in the liraglutide arm and 7.3% in the placebo arm, 1 leaving the interpretation of these figures to the reader. In addition, it noted instances of treatment pauses, with the regimen being administered an average of 84% of the time in the liraglutide arm and 83% in the placebo arm. 1 Investigation of time to protocol deviation (defined as exposure falling below 50% in the interval) using the LEADER discretized time grid (1, 3, and 6 months and thereafter) showed that by 1 year, 13.8% (95% CI: 12.7% to 14.8%) of individuals initiating liraglutide were non-adherent compared with 12.4% (95% CI: 11.4% to 13.4%) in the placebo group. By 3.5 years, non-adherence had increased to approximately one-quarter of participants in both groups (Figure 2).
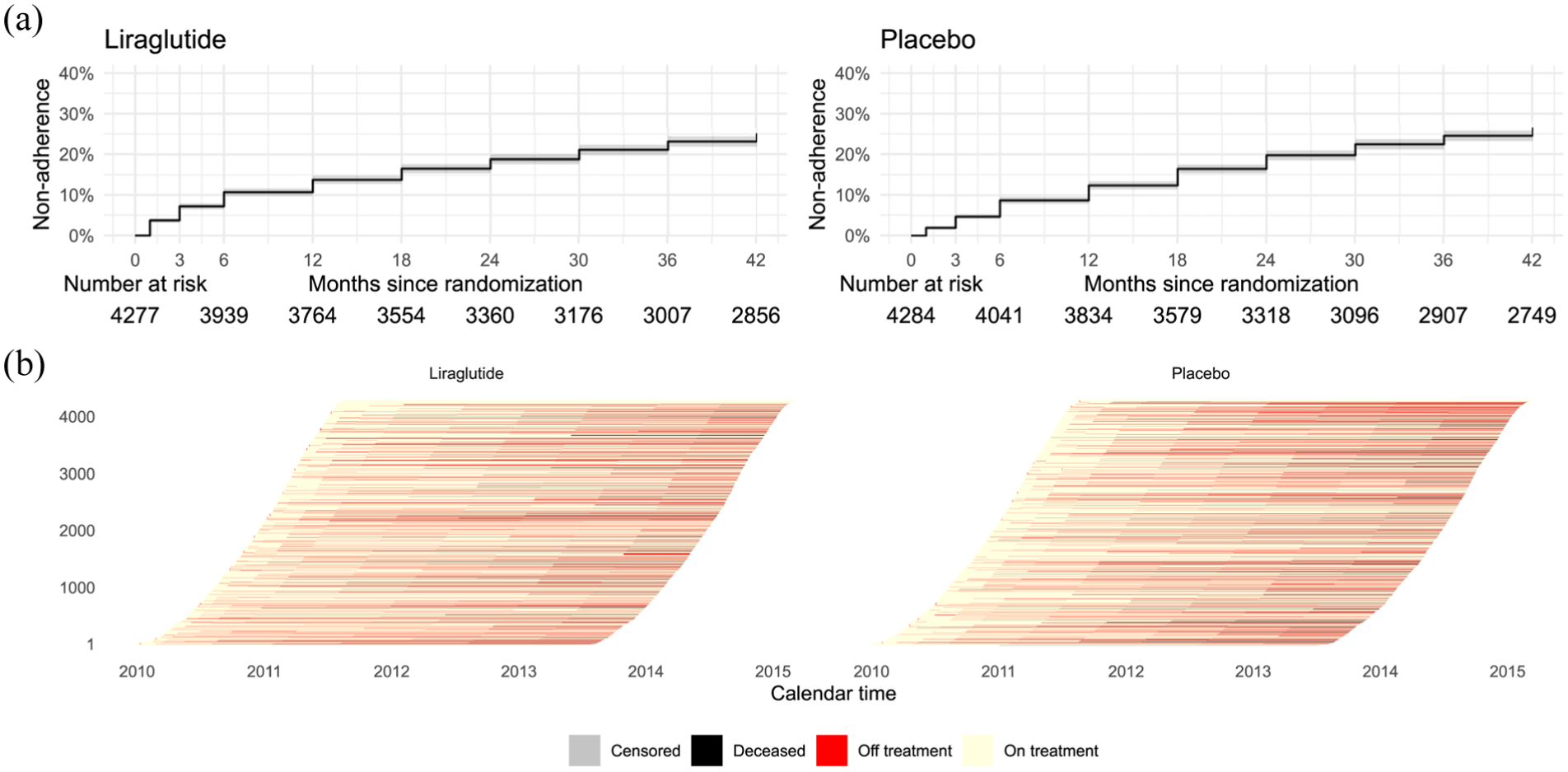
Adherence. (a) Time to non-adherence, defined as the first protocol deviation (treatment coverage <50% within a time interval). (b) Individual trajectories display periods on treatment, off treatment, censoring, and all-cause mortality.
Supplementary analyses
Varying the threshold used to define sustained exposure to liraglutide and placebo in the estimand, from 0% to 90%, revealed a decreasing risk with higher thresholds for liraglutide, whereas no consistent pattern was observed for placebo (Figure 3). Sensitivity analyses evaluating different levels of granularity in the discrete time grid did not alter the interpretation (Supplemental Table S3). Similarly, truncation of the estimated treatment probabilities did not materially change the results (Supplemental Table S4), and results were consistent when using an ensemble superlearner approach (Supplemental Table S5) compared with the estimates obtained in the main analysis (Supplemental Table S6).
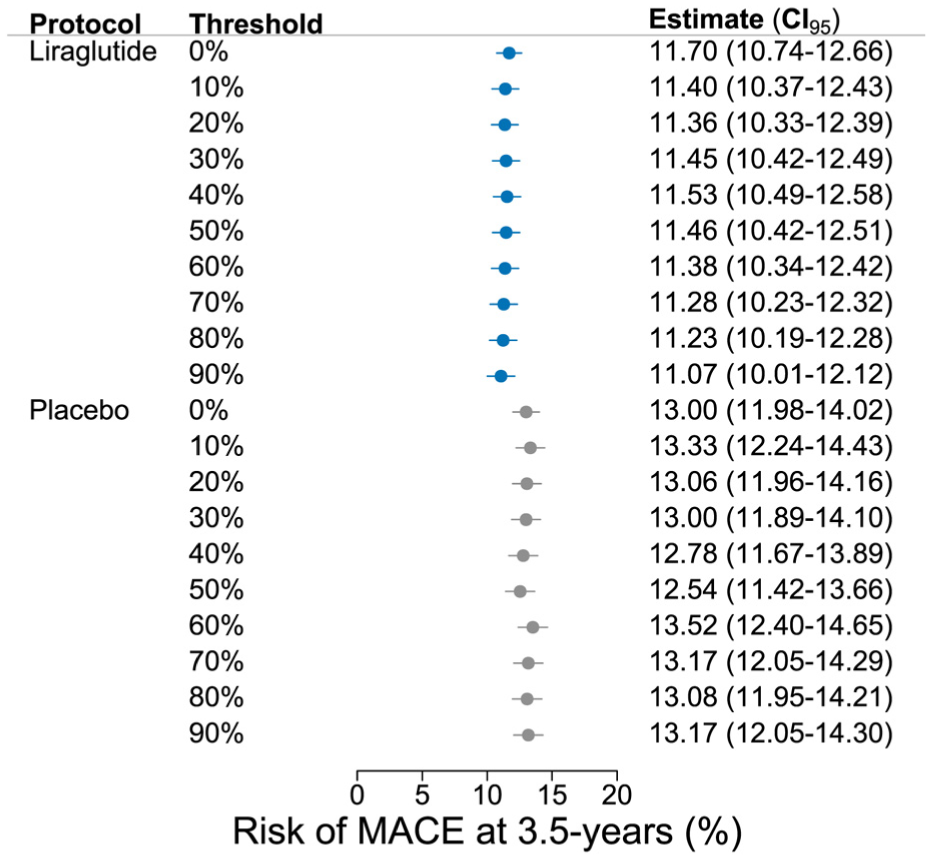
Risk of the primary composite outcome (myocardial infarction, stroke, or cardiovascular mortality) at 3.5 years in supplementary analyses in which the threshold defining sustained exposure to liraglutide and placebo in the estimand was varied from 0% to 90%.
Discussion
This study re-analyzed LEADER trial data to estimate the effect of sustained exposure to liraglutide on cardiovascular outcomes. By applying longitudinal causal inference methods, we defined and estimated an unambiguous and clinically relevant estimand that reflects the effect of maintaining treatment as intended. Our analysis supports non-inferiority of sustained exposure to liraglutide.
The ICH E9 (R1) Addendum emphasizes the importance of defining estimands to transparently specify treatment effects of interest. 17 The intention-to-treat principle does not always reflect the most clinically relevant questions, particularly in contexts like the LEADER trial where treatment adherence varied.1,18 The US Food and Drug Administration has provided guidance on conducting per-protocol analyses, requiring pre-specification of the analysis but offering limited direction on the statistical estimand and estimator. 19 The per-protocol analysis conducted for the LEADER trial lacked a clearly defined estimand and the analysis is susceptible to bias. 2
In this re-analysis, we used LTMLE to account for post-baseline information, such as adherence to the randomized treatment arm. This approach provides estimates of treatment effects had all patients adhered to sustained liraglutide use, addressing the limitations of traditional intention-to-treat and per-protocol analyses. In addition, it facilitates clearer communication of treatment benefits by offering risk differences that are more clinically intuitive than hazard ratios, 20 which were the primary estimates reported in the original publication. 1
Previous causal inference analyses of the LEADER trial, such as those by Chen and colleagues, 21 focused on other aspects of the data and did not include treatment adherence or post-baseline confounding in their analyses. Our work takes a different approach by incorporating these factors, providing additional insights into liraglutide’s effects. However, our analysis does not address the issue of differential use of rescue medicine and time-dependent improvements in the standard of care. For example, Rytgaard et al. 22 incorporated insulin use into their estimands to balance the exposure to insulin between the active and the placebo arms.
The causal inference framework allows researchers to explicitly discuss assumptions that must be satisfied to identify the estimand based on the available data, namely exchangeability, consistency, and positivity. 23 In the LEADER trial, the randomization process supports baseline exchangeability, but to identify our estimand, we also need exchangeability at each post-randomization time point where treatment options are revised (sequential exchangeability). 23 Post-baseline residual confounding occurs when unmeasured factors, such as side effects that drive the individual motivation to adhere, also affect the outcomes. Consistency is likely to hold for the defined regimes because the intervention is well-defined. However, our operationalization of exposure using a 50% threshold warrants discussion, as this level can be reached in different ways, for example, by taking the medication every other day or only at the beginning and end of the time interval. We varied this threshold in sensitivity analyses, and the results were consistent with our primary findings.
A limitation of our analysis is the reliance on time discretization, although our sensitivity analyses used several alternative discretizations to address this concern. Future research could explore alternative methods for handling the continuous time nature of the data. 24 Adherence results are important for motivating the sustained treatment analysis. Although non-adherence was substantial, it was sufficiently high to support the validity of the sustained treatment analysis while limiting concerns about potential violations of the positivity assumption. Another limitation is our use of a 50% cutoff for sustained treatment adherence. Although sensitivity analyses using alternative thresholds did not materially change the results, any dichotomization of adherence may oversimplify complex adherence patterns and may not fully reflect clinically meaningful behavior.
The public health relevance of the estimand where persons are forced to sustain to a treatment regimen warrants further consideration. Specifically, “the effect of sustained use unless medically contraindicated” might better reflect clinical realities but would require detailed data on reasons for non-adherence, 25 which were not available in the LEADER trial dataset.
Finally, our analysis was limited by access to only a subsample of the original LEADER trial data because of country-specific data-reuse agreements. While this may limit direct comparability with the original results, repeating the Cox regression analysis demonstrated similar hazard ratios to those observed in the original trial.
Conclusion
We defined and estimated a well-defined sustained treatment estimand for the LEADER trial by accounting for pre- and post-baseline confounders. This approach should be considered when conducting per-protocol analyses of randomized trial data.
Supplemental Material
sj-pdf-1-ctj-10.1177_17407745261449668 – Supplemental material for Accounting for non-adherence: A re-analysis of the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results trial
Supplemental material, sj-pdf-1-ctj-10.1177_17407745261449668 for Accounting for non-adherence: A re-analysis of the Liraglutide Effect and Action in Diabetes: Evaluation of Cardiovascular Outcome Results trial by Kathrine Kold Sørensen, Johan Sebastian Ohlendorff, Anders Munch, Puriya Daniel Würtz Yazdanfard, Mikkel Porsborg Andersen, Ulrik Pedersen-Bjergaard, Bochra Zareini, Thomas Alexander Gerds and Christian Torp-Pedersen in Clinical Trials
Footnotes
Acknowledgements
The authors wish to acknowledge the anonymous reviewers for their thorough evaluation and thoughtful recommendations. Their constructive input substantially enhanced the rigor and clarity of the final manuscript.
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funded by the European Union under contract number 101095556. Views and opinions expressed are, however, those of the author(s) only and do not necessarily reflect those of the European Union or European Health and Digital Executive Agency (HADEA). Neither the European Union nor the granting authority can be held responsible for them. This work has received funding from the UK Research and Innovation.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: U.P.B. has received speakers’ fees from Abbott, Novo Nordisk, and Sanofi and has served on advisory boards for Novo Nordisk and Sanofi. C.T-P. reports grants for studies from Bayer and Novo Nordisk that are unrelated to the current study. All other co-authors declare no competing interests.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.