
Abstract
Background and objective
Medical specialists have an essential role in promotion of generic medicines. However, misconceptions and negative perceptions about generic medicines among them could be a barrier to utilization of generic medicines. Therefore, the aim of this study was to explore their knowledge, perceptions and views about generic medicines.
Methods
A qualitative methodology was adopted in this study. A qualitative descriptive study with phenomenology overtones was the research strategy. Face-to-face semi-structured interviews were conducted with a purposive sample of medical specialists until saturation of data was achieved. The interviews were audio taped and transcribed verbatim. Then, the subsequent transcripts were analysed using thematic analysis. The themes were generated using both deductive (theoretical) and inductive coding. To ensure reliability of data analysis, peer review and independent analysis of the data were done.
Results
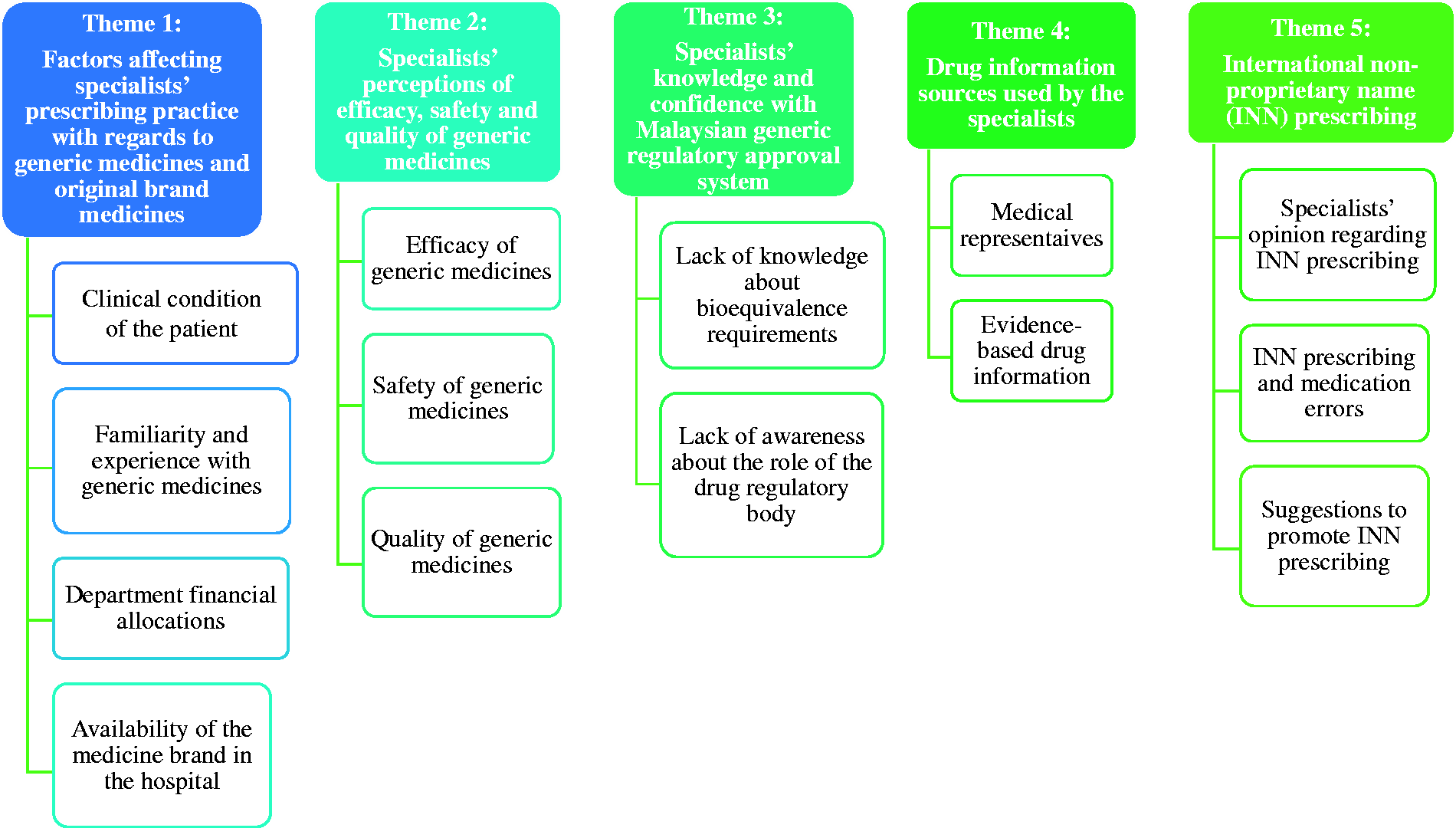
Five major themes were identified: (1) factors affecting specialists' prescribing practice with regard to generic medicines and original brand medicines, (2) specialists' perceptions of efficacy, safety and quality of generic medicines, (3) specialists' knowledge and confidence with Malaysian generic regulatory approval system, (4) drug information sources used by the specialists and (5) international non-proprietary name prescribing.
Conclusion
The study findings showed that several factors influenced prescribing decision with regard to the brands of the medicines including familiarity and experience with generic medicines, clinical condition of the patient, availability of the medicine brand in the hospital and department financial allocations. Moreover, misconceptions about quality, safety, efficacy and bioequivalence of generic medicines were prevalent among some participants. Furthermore, many participants were not familiar with the Malaysian generic medicines approval system. Therefore, medical specialists' concerns need to be addressed. Some recommendations and suggestions were made to improve generic medicines utilization in the country.
Introduction
Globally, healthcare expenditures have increased significantly in the last two decades.1–3 Within the context of healthcare expenditures, pharmaceutical costs are reported as the second main driver for healthcare cost escalation. 4 Similar trends have been noticed in the Malaysian healthcare system. Within a span of four years, the Malaysian healthcare expenditure increased by approximately 22.5% from 8.9 USD billion in 2009 to reach 10.9 USD billion in 2012. 5 Similar to the trend of total healthcare expenditure, pharmaceutical expenditure is tremendously growing in recent years. For example, within a span of four years, it increased by approximately 62% from 1.21 USD billion in 2009 to reach 1.96 USD billion in 2012. 5 In this ever challenging scenario of healthcare provision, one of the mechanisms suggested to minimize the cost of medicine is encouraging greater use of generic medicines.6–9
Although generic medicine sales have increased throughout the years in Malaysia, sales are still low compared to original brand medicines. 5 In the year 2011, generic medicines sales hit 0.54 USD billion, whereas original brand sales hit 0.77 USD billion. 5 Percentage wise, generic medicine sales contributed to only 30% of the total sales of medicines whereas original medicine sales contributed to approximately 42%. 5 A potential reason for these differences can be due to medical practitioners' views about generic medicines. It was documented that generic medicines were often viewed as inferior in quality and efficacy when compared to original brand medicines by medical practitioners.10–17 The debate has centered on the issues of bioequivalence and usage of generic medicines.10,12,13
Medical practitioners play an important role in improving the generic medicine utilization rate. In fact, in most countries, the medical practitioner is the key person in the medicine use process. The medical practitioner starts the process by prescribing or ordering medicines, and this is normally followed by pharmacist, who will in turn dispense the prescribed medicines.18,19 Moreover, in Malaysia, dispensing of prescription medicines still follows a traditional ‘dispensing doctors’ system in which medical practitioners dispense medicines as a part of their professional practice. 20 This is because the 1952 Poison Act in Malaysia granted the right for registered medical practitioners to prescribe and dispense medicines in their clinics. 21 Hence, medical practitioners have main influence on patients’ choice of either original brand medicines or generic medicines. In fact, the role of medical practitioners on consumers’ acceptance of generic medicines was reported by previous studies.22–25 Moreover, medical specialists have an important role in procurement of medicines and selecting whether original brands or generic medicines can be purchased by the hospital as they form the majority in the drug and therapeutics committees in the hospitals. Therefore, exploring medical specialists’ knowledge and perceptions about generic medicines and understanding their perspectives are important. In literature, most of the studies investigating knowledge and perceptions of generic medicines were conducted with physicians from high income countries.10,11,14,15,26–30 However, the findings from high-income countries could not be easily extrapolated to low-and middle-income countries because of the differences in healthcare systems.3,19,31 Hence, the objective of this study was to investigate medical specialists’ knowledge, perceptions and views about generic medicines.
Methodology
Ethics statement
Ethics approval for this study was granted by Malaysia Medical Research and Ethics Committee (NMRR 13-35-14876). Written consent was obtained from each medical specialist prior to the interview. In addition, the participants were also informed of the research objective, confidentiality of their responses and their right to withdraw from the study at any time.
Study design and research strategy
This was a qualitative study conducted with medical specialists. The research strategy adopted was qualitative descriptive (QD) study with phenomenology overtones.32,33 A QD study is a distinctive qualitative method, and one of the most widely used methods especially in practice disciplines. 32 QD studies aim to provide a comprehensive summary of an event or issue in the everyday terms of those events or issue investigated.32,34 Thus, this qualitative method seeks descriptive validity (i.e. an accurate detailed description of the topic or issue or event that most people – including both researchers and participants – observing the same event would agree on) and interpretive validity (i.e. an accurate accounting of the meanings participants attributed to those events that those participants would agree is accurate).32,35 One of the main advantages of the QD study is that it is less theorized compared to other qualitative methods, thus it can efficiently and effectively answer questions relevant to practitioners and policymakers in health care (i.e. the researcher stays close to the data and is not limited by theoretical or philosophical commitments such as can happen in other methods).32,33
Study setting
The study was conducted in a tertiary-care public hospital (i.e. Hospital Teluk Intan) in Perak, Malaysia. The hospital consists of 24 wards and 548 beds. 36 There were 25 specialists from 13 specialties available in the hospital. The specialties available in the hospital are outpatient, emergency and trauma, orthopedic, internal medicine, ophthalmology, psychiatry, pediatrics, dental, obstetrics and gynecology, ear, nose and throat (ENT), anesthesiology, radiology and pathology. In Malaysia, the medical specialist must be fully registered with the Malaysian Medical Council and hold a current annual practicing certificate. 37 To become a specialist, it is mandatory to complete a period of formal training and hold postgraduate qualifications in the area of specialty recognized by the National Specialist Register (NSR) secretariat. 37
The study instrument/interview guide
A semi-structured interview guide was used to gather information from the respondents. The interview guide was developed after an extensive literature review and consultation with experts in both generic medicines and qualitative research. The interview guide was piloted with two medical doctors. The interviews focused on the following topics: (1) knowledge of regulatory criteria for generic medicines, (2) knowledge of generic medicines (i.e. efficacy, safety and quality aspects), (3) prescribing practice with regard to generic medicines, (4) views regarding international non-proprietary name (INN) prescribing, (5) drug information sources and (6) suggestions to increase INN prescribing. Probing questions were used to get more in-depth information from the participants whenever necessary.
Sampling strategy and sample size
The purposive sampling strategy was adopted in this study. In fact, purposive sampling technique is the primary sampling technique in qualitative studies.38,39 This sampling strategy was used because it can achieve representativeness and capture adequately the heterogeneity in the population. Thus, a full range and spectrum of views and perspectives are all adequately covered to reflect diversity. 39 Therefore, specialists from different disciplines (i.e. outpatient, emergency and trauma, orthopedic, internal medicine, ophthalmology, psychiatry, pediatrics, dental, obstetrics and gynecology, ear, nose and throat) were recruited. In each discipline, one specialist was approached for participation. If not willing to participate, a second one from the same discipline was approached. Among those who were approached, only one declined to participate.
The adequacy of the sample size was determined by the concept of saturation.40–45 In fact, saturation is the ‘gold standard’ used to determine the sample size in qualitative studies using purposive sampling. 46 Saturation is defined as data adequacy and operationalized as collecting data until no new information is obtained 41 and the data set is complete, as indicated data replication or redundancy. 45 Thus, the data collection is stopped at the point of informational redundancy. 40 In our study, in the last four interviews, all the collected data were repetitive. Therefore, the sample size of the study was 10 specialists.
Data collection
Face-to-face interviews were conducted with the participants by an independent trained senior pharmacist. The interviews were conducted at the specialists' offices between 10 May 2013 and 7 June 2013. There were no other people present during the interview except the interviewer and the participant. The interviews were conducted in English and took an average of 30–40 min.
Data analysis
As the qualitative research is a not a linear process but rather a cyclical and dynamic process, data analysis started early and occurred concurrently with data collection. In this process, each interview informs the subsequent interview, and analysis of already collected data shapes the ongoing data collection.47,48 To prepare the data for coding and thematic analysis, the recorded interviews were transcribed verbatim. The principal researcher listened to the interviews and compared them with the transcripts. Then, the subsequent transcripts were analysed using thematic analysis. 49 The themes were generated using both deductive (theoretical) and inductive coding. 50 In this case, the data coding was based on the research questions and areas of interest (theoretical analysis) and also looks into emerging themes and issues raised by participants to form new themes (inductive analysis). 49 To ensure reliability of data analysis, peer review and independent analysis of the data were done. 51 Finally, the research report was written according to consolidated criteria for reporting qualitative research (COREQ).
Results
Specialists' demographic characteristics
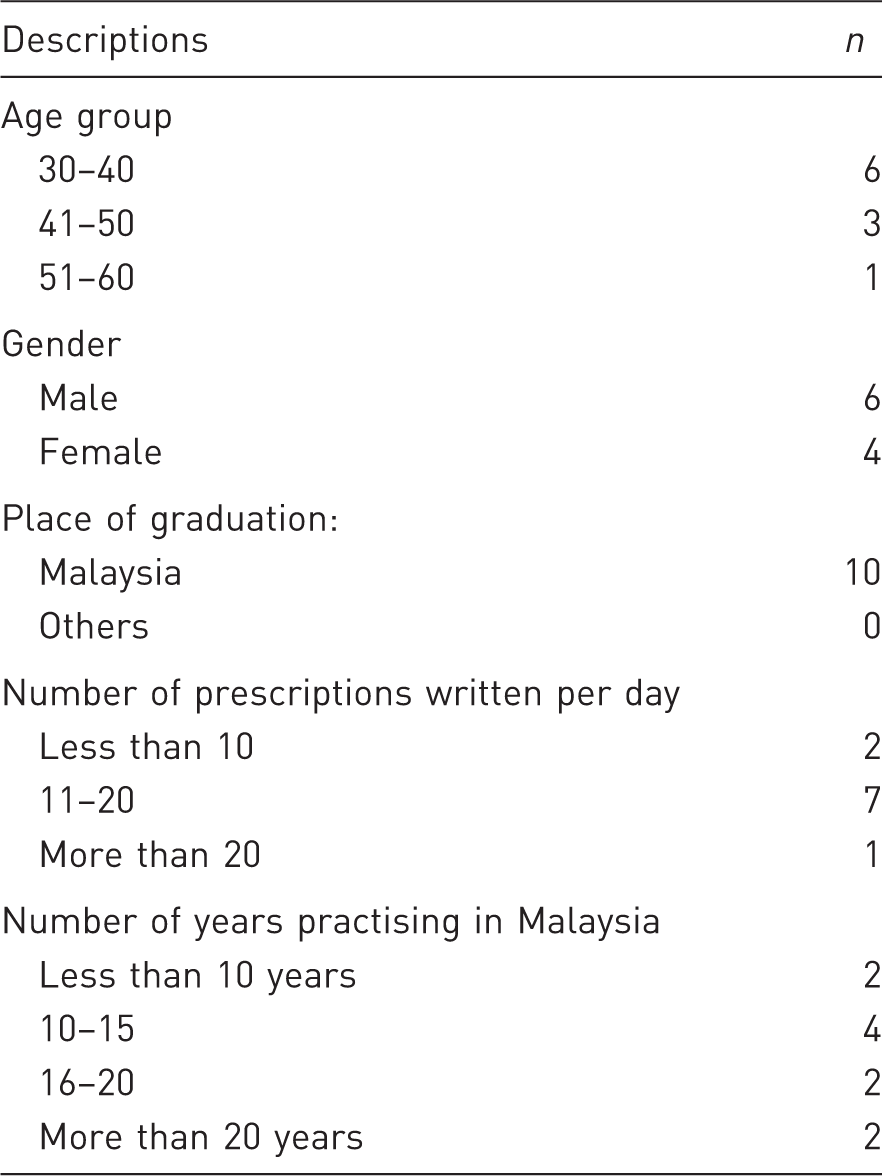
Themes and subthemes.
Theme 1: Factors affecting specialists' prescribing practice with regard to generic medicines and original brand medicines
The prescribing decision was influenced by several factors including clinical condition of the patient, familiarity and previous experience with the medicine brand, availability of the medicine brands in the hospital and department financial allocation.
Clinical condition of the patient
For chronic conditions or diseases, some specialists preferred to prescribe original brand medicines. However, almost all specialists stated that they would prescribe original brand medicines for severe conditions in their specialties. For acute diseases, I will choose original brand medicines because in the acute stage, it will be severe. But for the chronic stage, it depends on the severity of the disease. (S8)
Interestingly, some of them stated that prescribing original brand medicines is more cost effective. They believed that full and faster recovery can be achieved with original brand medicines, and number of readmission would be reduced. Hence, it would largely reduce the overall costs. In this regard, they believed that the cost-saving benefits of generic medicines could not offset the readmission costs. I prefer original brand medicines because you want them to be in better control for long term. So in the long run, you actually save a lot of money. (S3)
Moreover, for life-threatening condition and narrow therapeutic index (NTI) drugs, almost all specialists did not want to risk the patients. This indicated specialists' lack of confidence in generic medicines. I will bang with the original brand. For example like meningitis and all that, you really need good antibiotics to work efficiently. You can't risk trying generic and see how the progress is. You can't do that. You have to hit hard. (S5)
Familiarity and experience with generic medicines
Specialists' previous experience with generic medicines was one of the main factors affecting their prescribing practice. They stated that positive experience with certain generic brands improved their confidence in prescribing them. However, they would avoid prescribing certain generic brands when they had negative experience with them. Therefore, specialists reported that they usually try generic medicines with some patients and based on the therapeutic outcomes they decide whether to continue prescribing it. In contrast, the specialists showed high confidence in original brand medicines because they believed that they have gone through extensive clinical trials and hence their therapeutic outcomes are guaranteed. Yes, but I must have some experience of using it [generic medicine] because sometimes with generic we don't know how effective the medicine is, so it will be better if during the initial phase, we can try out the generic medicine first so that we can at least know the effectiveness before we totally use generic. (S4)
Department financial allocations
Specialists took into consideration their department financial allocation. They preferred to prescribe generic medicines when limited amount of money was allocated to their department especially during the end of the year when the budget is limited. However, when adequate funding was available, they preferred to prescribe original brand medicines. If the cost is an issue or our budget is limited, then definitely we will try out the generic first and see how effective it is. If it is okay then we can actually continue the generic. If they can afford it, of course we try original. (S4)
Availability of the medicine brand in the hospital
Specialists’ prescribing decision can be affected by the availability of the medicine brand in the hospital. For some medicines, specialists had no alternative generic medicines to prescribe since only original brand medicines are available. In contrast, for some medicines, only generic versions are available in the hospital. When I work in a certain place I will make sure whether the original brand is available or not. When the original brand is not available, that means I have to change to, resort to, generic version. (S8)
Theme 2: Specialists' perceptions of efficacy, safety and quality of generic medicines
Many specialists expressed concerns regarding generic medicines in terms of their efficacy, safety and quality.
Efficacy of generic medicines
Many specialists perceived that generic medicines are less effective that their counterpart original brands. No, the effect is different especially [original brand medicine]. The original, it really works. Sometimes the results are not so consistent for the generic version. (S2)
In this study, only some specialists believed generic medicines have the same efficacy as their counterpart original brands. I don't see any difference because so many other things come into play when you want to sort of compare the original version against the generic version. I don't know when comments are made that the generic version is poorer, that we have looked at all the other variables or not. Because of that, I personally would say among the medications that I prescribe, I would say it is good enough. (S7)
Safety of generic medicines
The majority of interviewed specialists had negative perceptions about the safety profile of generic medicines. Moreover, some of them stated that generic medicines can cause more adverse reactions and side effects than original brand medicines. Last time, the patients used the [original brand medicine] tablet now they use the [Generic version]. Patients experienced side effects like muscle pain with [Generic version] but side effects resolved when the patients change back to [original brand medicine]. (S6)
Quality of generic medicines
Most specialists expressed confidence in quality of generic medicines especially the solid dosage forms such as tablets. I have no problem with the quality. As a whole, as long as it is in blister packs, and it doesn't crumble when you touch it or something like that, I am happy with it. (S7)
However, some of them believed generic products especially generic injections are of a lower quality. This in turn would reduce the amount of the active ingredient administered to the patients. Hence, according to some participants, the effectiveness of the product is compromised. Previously, we used this [original brand] IV antibiotic which is from [original brand company] and then I think now we are using the generic version. We found some issues with dilution of the product. The generic version is actually not being diluted completely. That means when we mix the powder with distilled water we can actually still see some particles retained on the bottle. So we don't know if we are actually getting the one gram for the whole bottle or we are getting less than that. (S4)
Theme 3: Specialists' knowledge and confidence with Malaysian generic regulatory approval system
The interviewed specialists had inadequate knowledge and misconceptions about the generic regulatory approval system including bioequivalence requirements and the role of drug regulatory authority in assurance of quality, safety and efficacy of generic medicines. This lack of knowledge and misconceptions had a negative impact on specialists' confidence in generic medicines and hence generic medicine prescribing.
Lack of knowledge about bioequivalence requirements
The study participants had only heard of the term bioequivalence. However, they lacked in-depth knowledge about bioequivalence requirements and its clinical importance in determining the therapeutic equivalence of generic medicines. I know it is checked and somebody has to give the green light in terms of bioequivalence of the generic medicine under the approval process but I am not sure based on which standard they accept the bioequivalence data. (S7)
Lack of awareness about the role of the drug regulatory body
When the participants were asked about the role of drug regulatory body, most of them were aware of its existence. However, they were not clear about its roles in ensuring the quality, safety and efficacy of generic medicines. Yes, I’ve heard of it but I’m not really sure what their actual job scope is. I think I read some articles from the Ministry of Health and from their website. They actually mentioned that. (S4)
Moreover, some of the specialists believed that original brand medicines are registered via more stringent regulatory criteria compared to generic medicines. May be there is a certain percentage that generic medicines need to achieve but definitely not 100% like original brand medicines (S4).
Despite the lack of knowledge of the technical details, scientific principles and regulatory requirements for generic medicine approval system, the participants still expressed confidence with regulatory approval system. ‘It's okay. I am confident as long as it is approved by the Ministry of Health’ (S1).
Theme 4: Drug information sources used by the specialists
The interviewed specialists reported that medical representatives were their main source of drug information. Other sources mentioned by participants were journals, conferences, books and the internet. Although specialists stated that medical representatives were their main source of drug information, most of them stated that it is not ethical to force the hospital to purchase their products. For me if you [medical representative] want to promote, no problem I will accept, but I won't promise I will get a drug from you [medical representative]. I think it is not right to force a hospital to buy a medicine. (S10)
In this study, the specialists were mostly visited by medical representatives from original brand companies, while representatives from generic companies seldom visited them. The reason, according to the participants, might be due to lack of resources in generic companies. ‘Yes, they [original brand companies] have more money and will come out [visit] more often’ (S7).
In addition, some of the specialists reported that some of the original brand companies only promote the benefits of the medicines. Therefore, this biased information could affect specialists’ choice of medicines. They give me all the data but I want to know whether it is actually that effective or not because the medical representative will come and tell you everything is good. They will tell you the positive sides only. (S4)
Theme 5: INN prescribing
Specialists' opinion regarding INN prescribing
Some specialists supported INN prescribing as it overcomes patient confusion, improves the image of generic medicines and saves pharmacist time in handling the prescriptions. I will write in the generic name but I am not sure about others. First, it is easy for the pharmacy to read and also because they know what we want to give. (S1) We usually put the generic name e.g., Loratadine and Cetrizine. What we know, that it is not in original form we will write in the generic because different companies will come with some different names. (S3)
However, few specialists held different point of view and did not support INN prescribing. They mentioned that for some generic names it is difficult to remember and some medicines had long generic names. Therefore, they prefer to write original brand names because of their familiarity with it. In contrast, it is difficult to get familiar with the different generic brands for the same original brand medicine. Sometimes the original brand name is shorter and easier to pronounce so I am writing by using the original brand name.' (S10) I think they [medical doctors] will write using the original brand name because sometimes we [medical doctors] don't know what the INN is. Like Cefoperazone, you started off with [original brand] but now it may be that you have different [generic] company names. (S4)
INN prescribing and medication errors
Some participants supported INN prescribing because it could reduce medication errors arising from different brand names used during prescribing. They [different brand names] were one source of errors, if they [medical doctors] use the trade name instead of the generic name. I think if everything is standardized and everybody is using the generic name, people become familiar with it. (S7)
However, some of them claimed that medication errors still occurred even though they prescribe using INN. In fact, they stated that the main cause of medication errors was doctors' illegible handwriting. I don't think it [INN prescribing] makes any difference. There was once, I wrote the patient's prescription in generic name and the patient was given an antiepileptic. So even if I write in generic name, there is still a chance of error. It can happen anytime no matter if it is the generic name or brand name. (S3) I think it is not related to the name but it is the handwriting … the chances that people can read will be higher compared to you scribble. (S4)
Suggestions to promote INN prescribing
In the interviews, some strategies were suggested to promote INN prescribing including mandatory INN prescribing, educational interventions, using drug index, use of technology and mobile applications, and e-prescribing.
Mandatory INN prescribing
Some recommended that mandatory INN prescribing is needed. ‘I think we should [implement Mandatory INN prescribing]’ (S7).
However, some warned that mandatory INN prescribing might lead to medication errors. I think it [mandatory INN prescribing] will never work because most of the times I think people are taught by brands. The juniors are trained by the seniors by brands and they may not know the generic name, which is longer. Suddenly, you force them to memorize new generic names which in turn will cause mistakes. (S2)
Educational interventions
Some specialists agreed that education has a role in changing doctor's prescribing habits, and the educational campaign should be continuously conducted to achieve optimal effect. I think you have to start from young doctors really. You have to educate them, give them a course or workshop to teach them what the generic name is and encourage them to write out the name in full. (S2) Educate and they might forget. You can put a CME [continuing medical education] and talk about it and then next week they will forget about it. It is important to carry out periodically so it will stick on people mind. (S5)
Use of drug index
Some specialists suggested that drug index with both brand and generic names could serve as a reminder for them to prescribe using INN since they have difficulty to remember generic names. You can come with the chart or a list with the brand name and generic name and hand it over to all the departments. When we have it here, it will be easier for us to write. (S5)
Use of technology and mobile applications
Using innovative and advanced technologies could ease the dissemination of drug information. Doctors could easily check the generic name of the drugs by using local developed mobile applications. You should have mobile applications. We don't have any local conversion apps because books are very difficult and thick. Sometimes you are in a hurry; you don't know where to look for the books. (S4)
E-prescribing
E-prescribing was considered a good way to promote INN prescribing. It could overcome the difficulty of remembering since all generic names were available in the computer. I think we have to move towards technology. If you go to a country like Singapore, all the prescriptions are in a computerized form. When you print it out, it is actually much easier to read. Even if you key in this medicine, if it is not available in the pharmacy, then straight away the doctor can change it. (S4)
Discussion
The study finding showed that the prescribing decision with regard to generic medicines and original brand medicines was influenced by several factors including medical and clinical condition of the patient. In literature, the clinical condition of the patient including the type of disease (serious vs. non-serious), the medical condition (chronic vs. acute), the severity of the condition (severe vs. moderate vs. mild)10,53–55 and accordingly the pharmacological group of the medicine (i.e. therapeutic class)10,13,15,17,56 are the factors that influence prescribing in general, and whether to prescribe an original brand or a generic medicine in particular. For instance, the severity of the disease was an obstacle to the prescribing of generic medicines as physicians in Iraq prescribe original brand medicines for severe cases rather than generic medicines. 54 In fact, this is not surprising as in severe cases, a rapid and potent therapeutic response is required, but a baseless belief that original brand medicines give a faster effect is a barrier to prescribing the generic versions. One study conducted in Spain showed that more than half of physicians (51.7%) believed that generic medicines need a longer time to produce a therapeutic effect. 57 In Italy, approximately only half of prescribers wrote generic medicines for chronic diseases. 10 Similarly, with regard to the type of therapeutic class, approximately half of surveyed general practitioners (GPs) in Pakistan were reluctant to prescribe generic medicines in some therapeutic classes of medicines.17,56 In fact, medicines of perceived higher safety and used for a lower perceived seriousness, such as some antibiotics, analgesics and some gastrointestinal medicines, are more prescribed as generic medicines compared to medicines used in cardiology and endocrinology, including NTI drugs.10,13,15 In such cases, physicians are more likely to prescribe original brand medicines regardless of the price or even affordability, especially when they believe that the therapeutic effect can be provided only by the original brand medicines.58,59
The study findings showed that interviewed specialists were familiar with original brand medicines which are ‘well known’ to them. However, for generic medicines, they prescribe only generic medicines that they have had positive practical experience with. In fact, this behaviour is not surprising, as a large body of literature reported that prescribers’ familiarity with a product, personal (i.e. practical) experience with the drug product (i.e. they have trialled it), the popularity and recognition of the product are all influencing factors that affect medical practitioners’ choice of a certain product or a range of brand names of products in their practice, especially with generic medicines.17,30,53,55,56,58,60,61 For example, in Sweden, participants have explained that the first drugs marketed (i.e. brand medicines) are those with which they had most experience. Furthermore, they have highlighted that some original brand medicines became part of ‘therapeutic traditions’ in some specialities. 58
Moreover, department financial allocation was mentioned by specialists as one of the factors affecting prescribers' brand selection. This finding showed that participants were aware of the cost-saving benefit of the generic medicines and they prefer to use generic medicines especially when limited budget is available. 15 Another factor to be considered when prescribing medicines was availability of the medicine brand in the hospital. This is consistent with the findings reported in a previous study. 54 In Malaysia, the medicine procurement system in Ministry of Health (MOH) institutions is guided by the Malaysian national essential drug list (NEDL) and Malaysia MOH Drug Formulary. The MOH Drug Formulary serves as a guide to Drug and Therapeutic Committee (DTC) in selection of medicine and development of the drug formulary for each hospital. 62 However, in this system, specialists have a great influence in DTC meetings in selecting either brand or generic medicines in the hospitals because procurement of certain brands of drugs depends upon the decision of the DTC, members of which majority are specialists. In addition, specialists have the power to request certain brands of medicines based on their clinical judgment and the cost-effectiveness of the medicine.
In this study, some medical specialists were sceptical about quality, safety and efficacy of generic medicines. In literature, medical practitioners expressed similar concerns about generic medicines.14,54 In fact, several studies shared the fact that the perceived clinical effectiveness of the drug product is one of the most, if not the most, important factor that influences whether the medical practitioner prescribes a generic product or not.12,53,54,58,63 For example, clinical effectiveness is the most important factor considered by physicians according to more than 90% of surveyed physicians in Greece and Cyprus. 27 Moreover, in this regard, many studies reported that some medical practitioners did not consider generic medicines, or some of them, therapeutically equivalent to the original brand medicines.12,16,29,54,63,64 Due to this misconception, they expressed their concern about therapeutic failure with some generic medicines.15,16,54,56 Such misconception and negative perception not only lead to a lack of confidence in generic medicines,16,54 but prevent or deter or decrease the rate of prescribing generic medicines.12,54,63 Therefore, having a correct understanding of generic medicines is important among specialists. Moreover, in developing countries without dispensing separation, such as in Malaysia, specialists and doctors have great influence on a patient's decision in selecting either generic or original brand medicines.3,65,66 Furthermore, specialists have great influence on junior medical practitioners' prescribing behavior. 67 Therefore, by having a good understanding of generic medicines, specialists' confidence and acceptance of generic medicines could be improved. As a result, usage of generic medicines in public healthcare institutions could increase.
The study findings showed that the interviewed specialists lacked in-depth knowledge about bioequivalence requirements. Similarly, poor knowledge of the regulatory limits for bioequivalence was reported in previous studies conducted with medical practitioners from other countries.12,26,54,68,69 In Malaysia, as in most countries, the accepted criteria to demonstrate bioequivalence is when the 90% confidence intervals for the logarithmically transformed Cmax ratio and AUC ratio (generic: branded innovator products) fall within the range of 80% to 125%.70,71 The Cmax in this case refers to maximum plasma drug concentrations, and AUC is the area under the plasma drug concentration versus time curves. In addition, the interviewed specialists were not clear about the roles of drug regulatory body in ensuring the quality, safety and efficacy of generic medicines. Moreover, some of the specialists believed that original brand medicines are required to meet higher standards and more stringent regulatory criteria compared to generic medicines. In fact, both generic medicines and original brand medicines have to comply with the same quality control standards and requirements set by Malaysian Drug Control Authority. Therefore, all drug companies are required to follow good manufacturing practice (GMP) requirements, guidelines for pharmaceutical development, product testing (i.e. both compendial and non-compendial testing), and the content of the common technical documents for regulatory submission has been adopted from competent, regulatory agencies in the European Union, the United States of America, and the International Conference on Harmonization (ICH).70,72 The only difference is that generic medicines manufacturers are not reuqired to repeat the pre-clinical and clinical testing as they have the same active ingredients. 73 Taken together these findings, i.e. lack of knowledge about bioequivalence requirements and unfamiliarity with the generic regulatory approval system, could have a negative impact on specialists' confidence in generic medicines and hence generic medicine prescribing.
Similar to previous studies,14,27,54,56,58,74 the participants in our study reported that pharmaceutical industry and medical representatives are an important source of drug information regarding medicines. Moreover, it is widely reported in the literature that prescribing decision and choice of medicine brands are influenced by the pharmaceutical industry and their medical representatives.12,17,27,54-56,68,74,75 In this study, specialists might be influenced more by original brand companies because generic company representatives seldom come to promote their products to them. Similar finding was found in Saudi Arabia. 28 In addition, some specialists reported that original brand medicines representatives just promote the good side of the medicines. This scenario, if left unattended, biases drug information obtained from brand original drug companies and may have a negative impact on generic prescribing. As drug representatives are one of the main sources of drug information,30,54 there is a need for a regulatory body to monitor drug information provided by medical representatives.
Regarding implementation of INN prescribing, there were two different opinions. Some participants supported its implementation because it could improve the image of generic medicines, save pharmacists' time in handling the prescriptions and reduce medication errors arising from patient confusion. However, few participants did not support it because they felt some generic names are difficult to remember and might even lead to medication errors. Similarly, in literature, some studies reported that many medical practitioners considered brand names to be easier and more memorable compared to generic names.56,76,77 The interviewed specialists made some recommendations to promote INN prescribing, including mandatory INN prescribing and educational interventions. In fact, the current generic medicines policy stated that INN prescribing shall be encouraged at all levels. 78 However, there are gaps between formulation of these policies and its implementation in Malaysia.72,79 Therefore, educational interventions (e.g. workshops, seminars) are important to promote the INN prescribing. In fact, the effectiveness of educational interventions was confirmed by previous studies.80–83 Other strategies suggested the use of information technology and the use of passive interventions such as use of drug index. Previous studies showed that passive strategies in changing physician's behavior are relatively less effective compared to more active strategies (e.g. education).80,84–86 Although generally ineffective and unlikely to result in behavioral changes when used alone, passive interventions are useful in raising awareness of targeted behavioral changes. 87 In contrast, active interventions are more effective but also more costly. 87 Policy makers need to take into consideration advantages and disadvantages of the suggested strategy before formulating an effective way to improve specialists' perception and knowledge about generic medicines.
Several recommendations can be made. First, communication between the drug regulatory authorities and medical practitioners is important to make them aware of the registration system requirements, and the standards that medicines must pass through before being granted approval. This will make them confident in the generic medicines as essentially the same as the original brand medicines and that all medicines go through the same registration process. Second, there is a need to conduct educational interventions. It could be done in the form of workshops, seminars or lectures as part of their continuing medical education. The education intervention should cover quality, safety and efficacy aspects of generic medicines. Moreover, the concept and principles of bioequivalence should be introduced to the medical practitioners. Furthermore, it is important to introduce the relevant topics such as quality control, quality assurance and GMP concept to the medical practitioners. Third, in view of the current limited information sources available to the medical practitioners especially about generic medicines, it is important to have a formulary of bioequivalent and interchangeable medicines. Moreover, in the formulary, the available options, available brands of a medicine and their prices need to be included so that medical practitioners can compare the prices and hence adopt cost-effective prescribing.
Limitations
The study has managed to provide detailed, relevant information and a better understanding of medical specialists’ views and perspectives and also addressed the current issues surrounding the prescription of generic medicines in public hospital settings. Nevertheless, it had some limitations. The study was conducted in one state (i.e. Perak state). Therefore, generalization of the findings to whole Malaysia might not be possible. Moreover, although qualitative research is very useful and perhaps the most appropriate method in addressing and exploring real-world complex issues or phenomena, it is not usually intended to be generalized. However, the findings could be ‘applicable’ to similar cases or participants and ‘transferable’ to similar situations or settings in Malaysia.88,89 The small sample size might be seen as a limitation when judged by quantitative standards—which is not appropriate. However, the adequacy of sample in qualitative research is determined by data saturation. Our sample size is comparable to other studies in literature specifically the studies that used the same methodology (i.e. qualitative study), the same topic (i.e. generic medicines) and the same population (i.e. healthcare professionals).12,17,54,90–95 More importantly, based on our analysis by using the concept of saturation—which is the gold standard method that determines the adequacy of the sample size—the sample size is considered adequate.
Conclusion
The study finding showed that several factors influenced prescribing decision with regard to the brands of the medicines including familiarity and experience with generic medicines, clinical condition of the patient, availability of the medicine brand in the hospital and department financial allocations. Moreover, misconceptions about quality, safety, efficacy and bioequivalence of generic medicines were prevalent among the participants. Furthermore, the participants were not familiar with the Malaysian generic medicines approval system. Therefore, medical specialists' concerns need to be addressed. Some recommendations and suggestions were made to improve generic medicines utilization in the country.
Footnotes
Acknowledgements
The authors would like to thank the Director of Health Malaysia for permission to publish this article. The authors wish to thank all doctors for their participation in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.