
Abstract
Epilepsy is a neurological disorder that requires long-term pharmacological treatment. Conventional oral antiepileptic dosage forms often present limitations such as swallowing difficulties, delayed onset of action, and reduced patient compliance. Orally disintegrating dosage forms (ODDFs) have emerged as a suitable alternative to overcome these challenges. These formulations rapidly disintegrate in the oral cavity without the need for water, making them particularly beneficial for pediatric, geriatric, and epileptic patients. This article reviews the concept and significance of ODDFs in epilepsy management. It focuses on formulation considerations, selection of excipients, methods of preparation, and evaluation parameters associated with ODDFs. The advantages of ODDFs in terms of ease of administration, patient acceptability, and improved therapeutic performance are also discussed. Furthermore, it highlights recent case studies involving antiepileptic drugs, demonstrating the therapeutic potential of ODDFs. The article emphasizes the potential of orally disintegrating dosage forms as an effective drug delivery approach to enhance treatment outcomes and patient compliance in epilepsy therapy.
Keywords
Introduction
Neurological disorders such as Alzheimer’s, Parkinsons, Epilepsy, and Dementia significantly influence global health as they not only affect the quality of life but also hinder cognition and other social aspects. Epilepsy is one such debilitating condition affecting patients world-wide irrespective of age, sex, and nationality. According to the International League Against Epilepsy (ILAE), epilepsy is defined as “Disorder of the brain characterized by an enduring predisposition to generate epileptic seizures, and by the neurobiologic, cognitive, psychological and social consequences of these conditions”.1,2 Roughly 10-20% of the global population is affected by this condition, with many more still undiagnosed.2–4 Accurate diagnosis often classifies epilepsy based on the severity and nature of symptoms as represented in Figure 1. Classification and stages of epilepsy.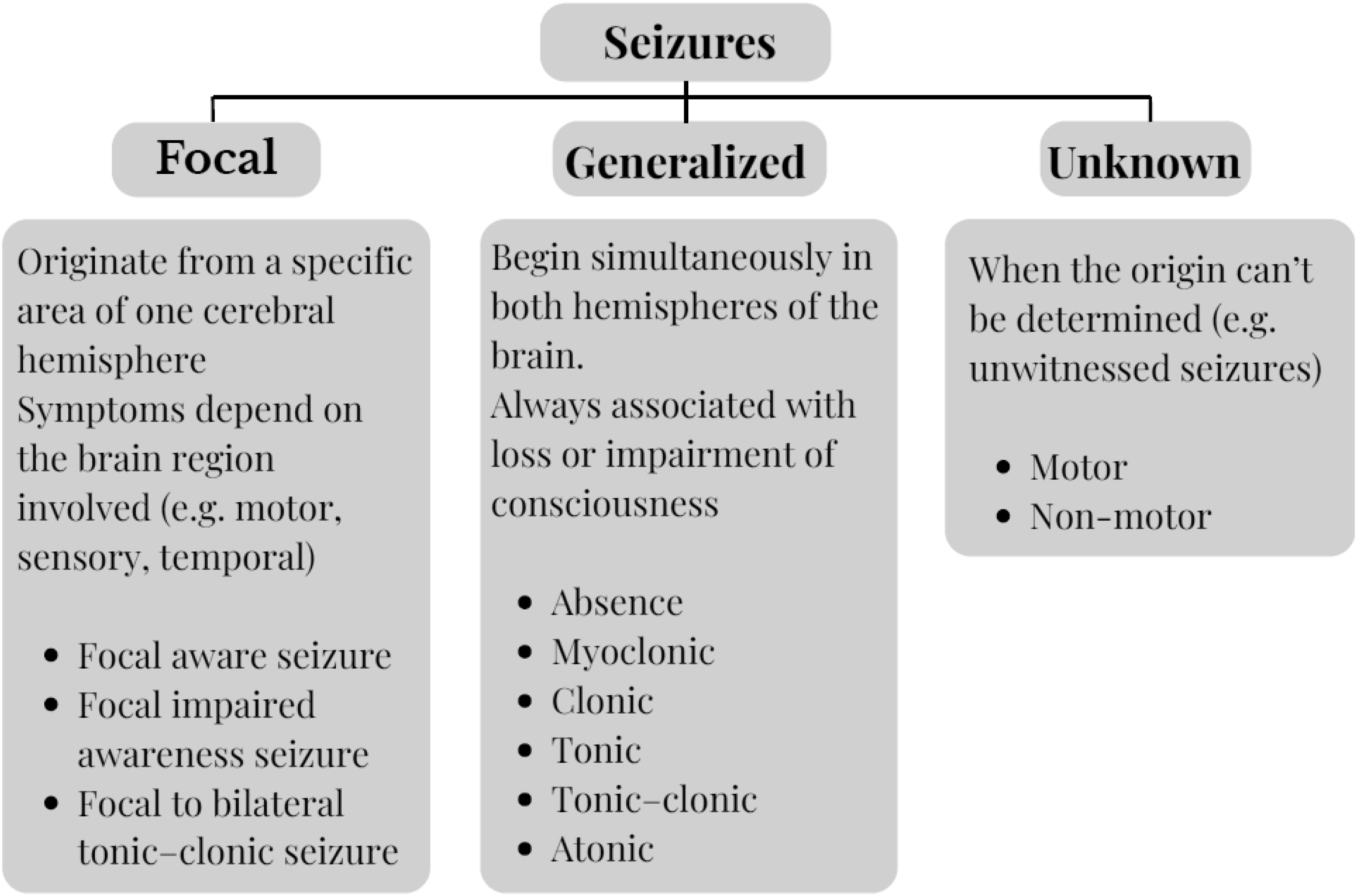
Epilepsy also referred as epileptic seizures arise from a hypersynchronous (excessive) barrage & displacement of neuronal activities in the human brain. These abnormal activities could be due to hypoxic conditions, infection, mental trauma, brain malformations, etc.3,4 Genetic factors such as family history of epilepsy, genetic mutations, certain other syndromes may also be the underlying cause. Several neurotransmitters such as Serotonin, Glutamate, Dopamine, Gamma-Amino Butyric Acid (GABA), and Noradrenaline are significantly involved in epileptic condition of which GABA plays a key role. GABA generates presynaptic potentials by hyperpolarizing neuronal membranes, thus reducing neuronal excitability in an individual. GABA is also responsible for excitation and inhibition of neuronal networks. Impairment or decrease in GABAergic activity can increase the risk of epilepsy. GAT-1 is responsible for the re-uptake of GABA from the synapses. Any sort of mutation in this GABA transporter could cause myoclonic, atonic seizures.5–7
Challenges associated with current antiepileptic therapy
Despite the availability of multiple antiepileptic drugs, effective long-term seizure control remains a challenge for many patients, primarily due to limitation associated with conventional oral dosage forms.18–20 Swallowing difficulty (dysphagia) is common in pediatric, geriatric, and neurologically impaired populations often resulting in poor compliance or missed doses, which can precipitate breakthrough seizures. 21 Many AEDs possess bitter taste and an unpleasant odour, discouraging adherence-especially in children. The need for frequent dosing due to short half-lives and variable pharmacokinetics further exacerbates non-compliance.18,21 Moreover, during or immediately after a seizure episode, patients may be unconscious, disoriented, or unable to swallow, rendering solid dosage forms impractical. Delayed onset of action with conventional tablets can also be problematic in managing acute seizures or preventing recurrence. 19 In addition, some AEDs exhibit low aqueous solubility and erratic absorption, leading to variable plasma concentrations and suboptimal therapeutic response. 18 Caregiver dependency, particularly in pediatric and cognitively impaired patients, further complicates consistent drug administration. 20 Collectively, these challenges highlight the pressing need for alternative delivery systems that offer ease of administration, rapid onset, improved palatability, and enhanced adherence-criteria ideally fulfilled by orally disintegrating formulations.22,23
Orally disintegrating dosage forms
Orally Disintegrating Dosage Forms (ODDFs) have the property to rapidly disintegrate and/or dissolve promptly on coming in contact with the salivary fluid, thus releasing the actual drug in the oral cavity itself.
24
These formulations differ from the conventional oral dosage forms, in that they disintegrate and release the drug in the oral cavity itself as opposed to the disintegration in the GIT.25–27 ODDFs are suitable forms for dysphagic, psychotic, paediatric, and geriatric patients; and could also be beneficial for epileptic patients.28,29 The ideal properties, advantages, and disadvantages of ODDFs are highlighted in Figure 2. An ODDF usually dissolves in the mouth within a matter of seconds, making it suitable for waterless administration. Orally Disintegrating Tablets (ODT), Orally Disintegrating Films (ODF), Orally Disintegrating Mini Tablets (ODMTs), and Effervescent Orally Disintegrating Systems are the most common types of ODDFs researched upon; however, ODTs and ODFs mostly take precedence.
34
ODTs are solid unit dosage forms that quickly disintegrate after coming in contact with the salivary fluid; approximately within 30–60 s. ODFs are thin strips composed mainly of a hydrophilic polymer which dissolve rapidly when placed on the surface of the tongue. While the rapid disintegration of ODTs is attributed to the presence of superdisintegrants or sublimating agents, the swift dissolution of ODFs is owing to its negligible thickness and the presence of hydrophilic polymers.34–36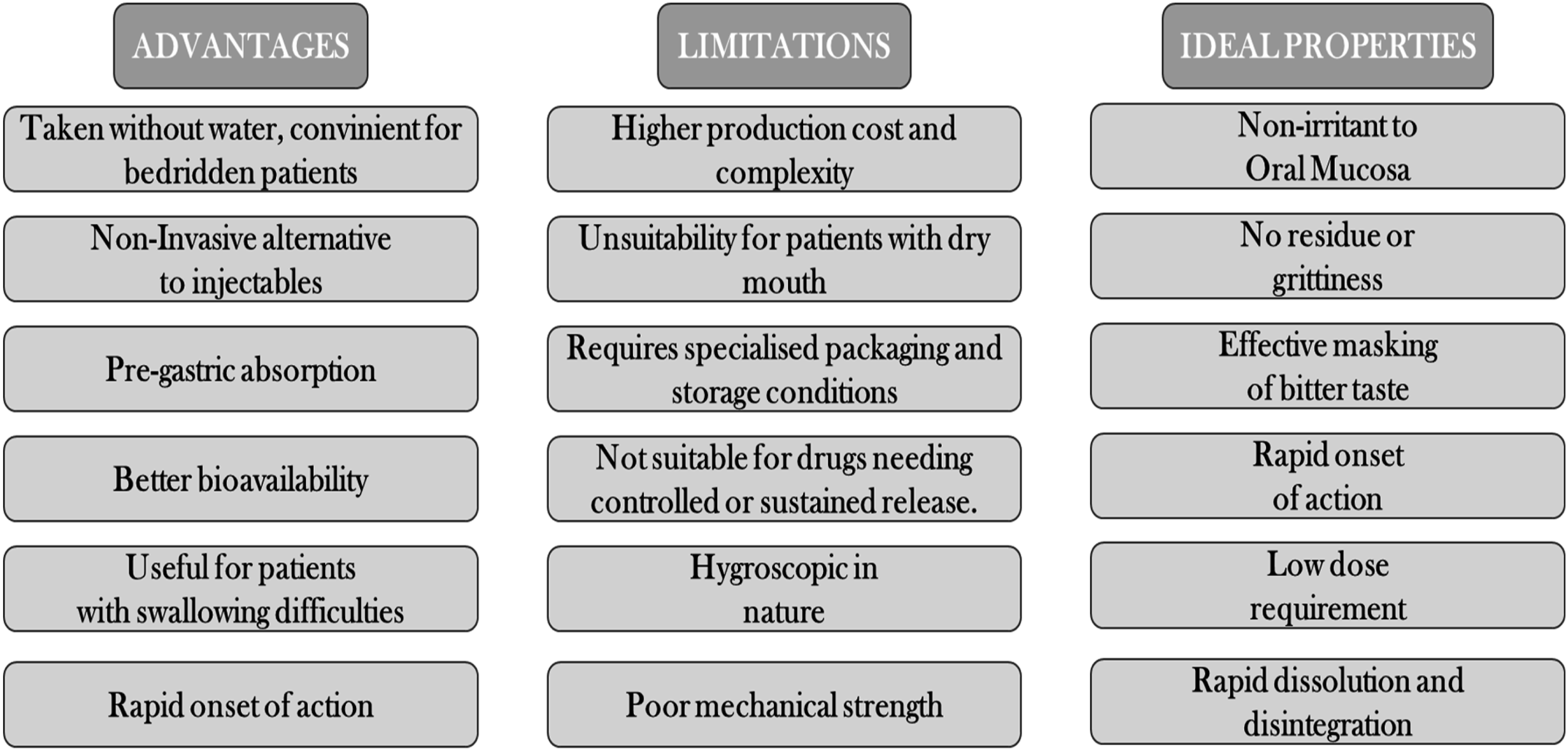
Formulation aspects of ODTs and ODFs
An ideal drug candidate for the development of ODDFs must have a small dose to allow maximum loading and a molecular weight less than 500 Da to allow for pre-gastric absorption through the mucosal linings of the oral cavity, acceptable taste, and good stability. The commonly incorporated drug candidates for ODTs and ODFs usually include analgesics, antihypertensives, antihyperlipidemics, anti-inflammatories, and antibiotics.37–40
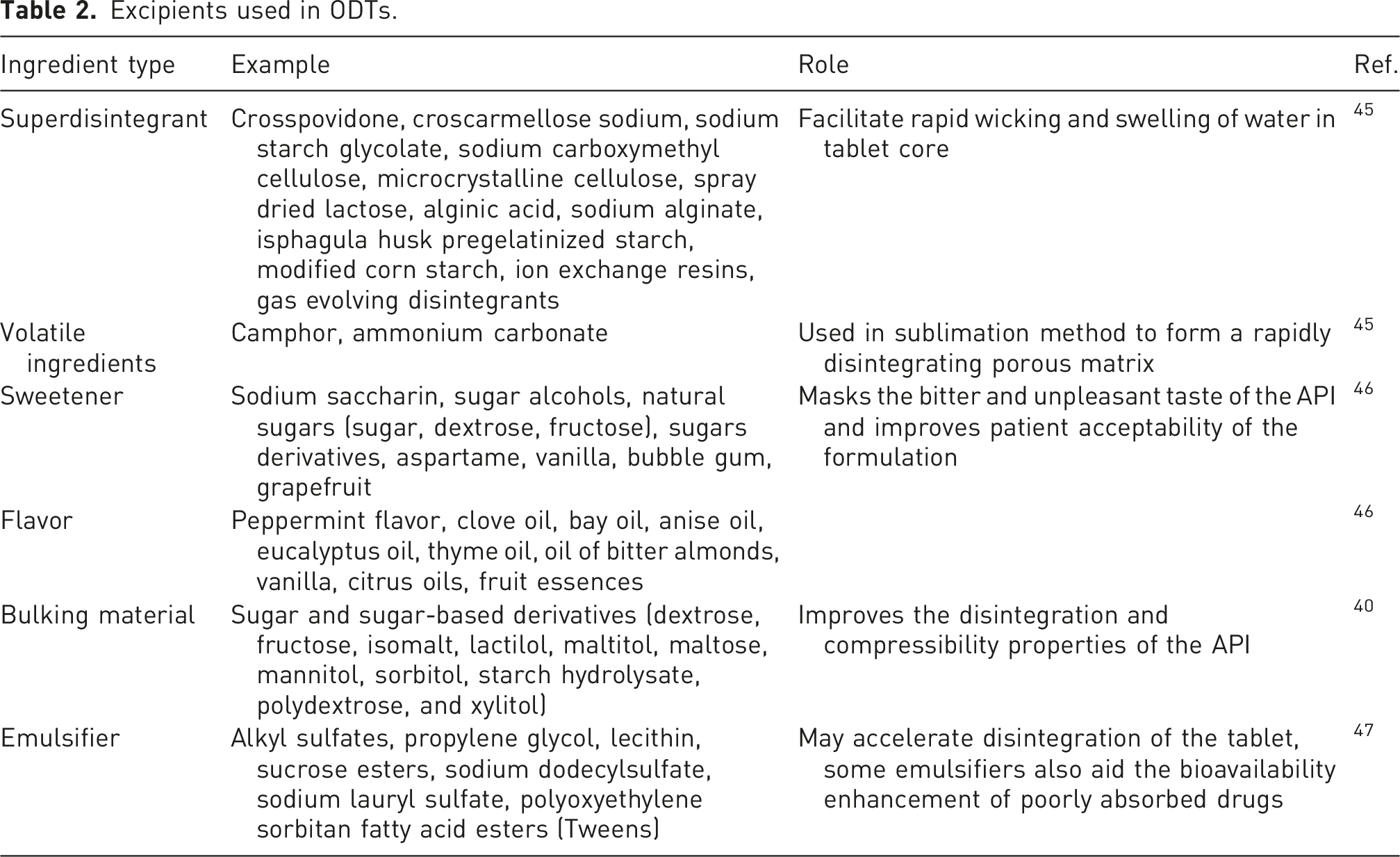
Excipients used in ODTs.
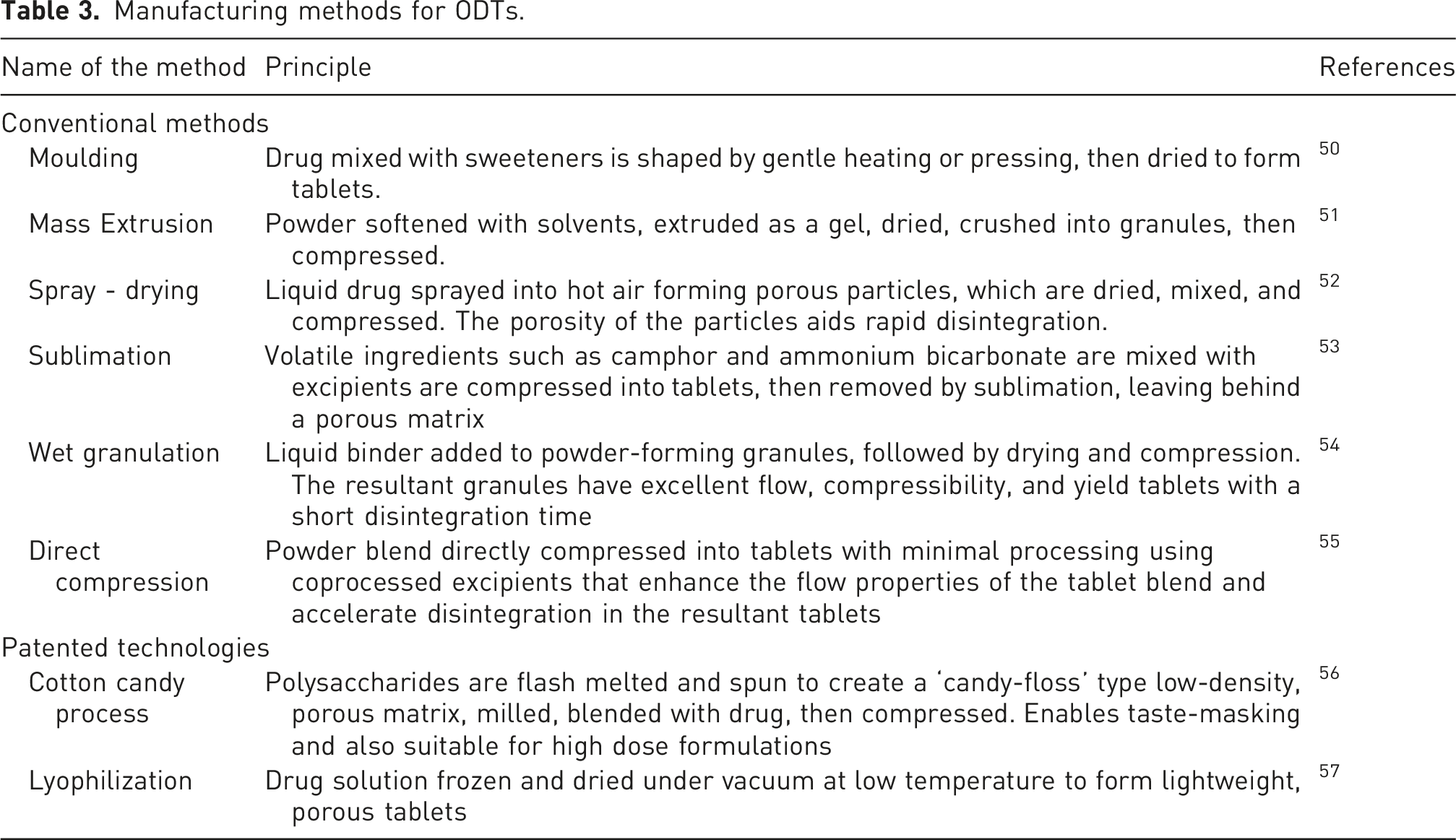
Manufacturing methods for ODTs
Manufacturing methods for ODTs.
Evaluation of ODTs
Evaluation of ODTs primarily involve the assessment of pre-compression and post-compression parameters. Pre-compression parameters assessed for ODTs involve the determination of bulk density, tapped density, and angle of repose. These parameters are particularly important for ODTs manufactured by direct compression method, since they are related to the compressibility and flow-properties of the tablet blend.58,59
Post-compression parameters involve the usual pharmacopoeial tests performed for tablets such as dimensions, weight variation, hardness, friability, and disintegration time. Of these friability and weight variation are very crucial; since the former evaluates if the tablet is robust enough to mechanical stresses associated with shipping and transportation and the latter determines if the tablet adheres to the pharmacopoeial requirement of an ODT. Besides these, water absorption test and wetting time test may also be performed that confirms the rapid water absorption and swelling of the tablet, which is a prerequisite for faster disintegration.60–62
Orally Disintegrating Films (ODFs)
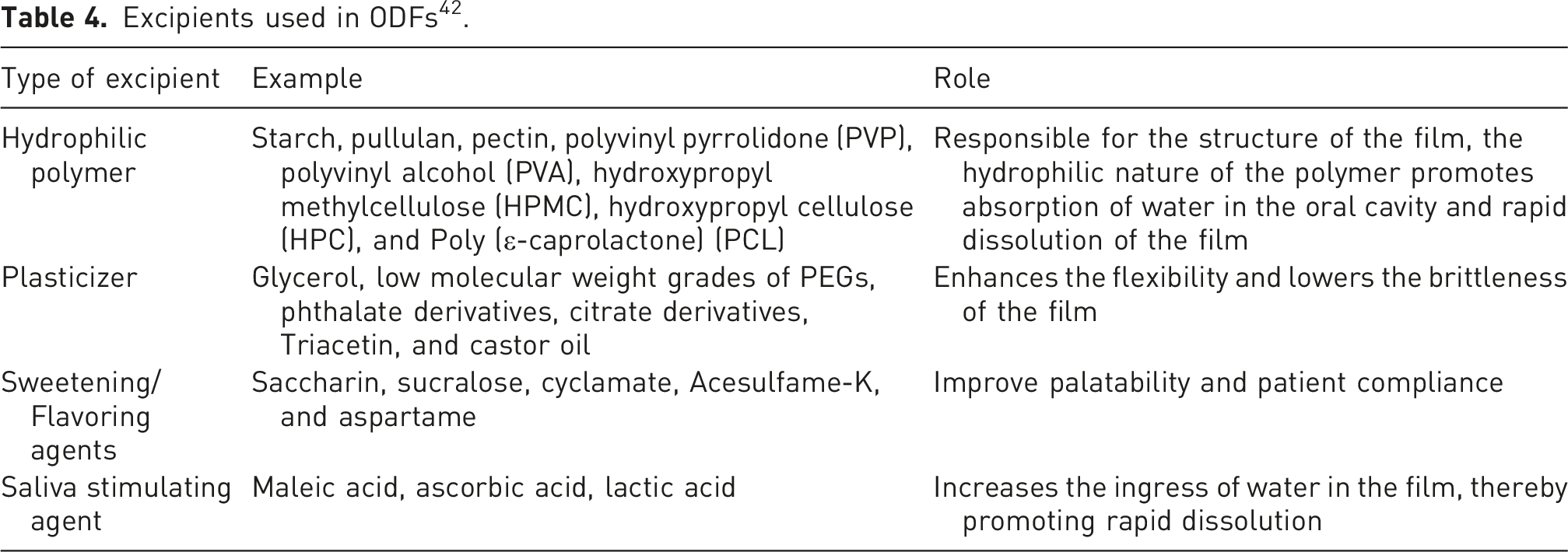
Excipients used in ODFs 42 .
Manufacturing methods for ODFs
Manufacturing methods for ODFs. 62 .
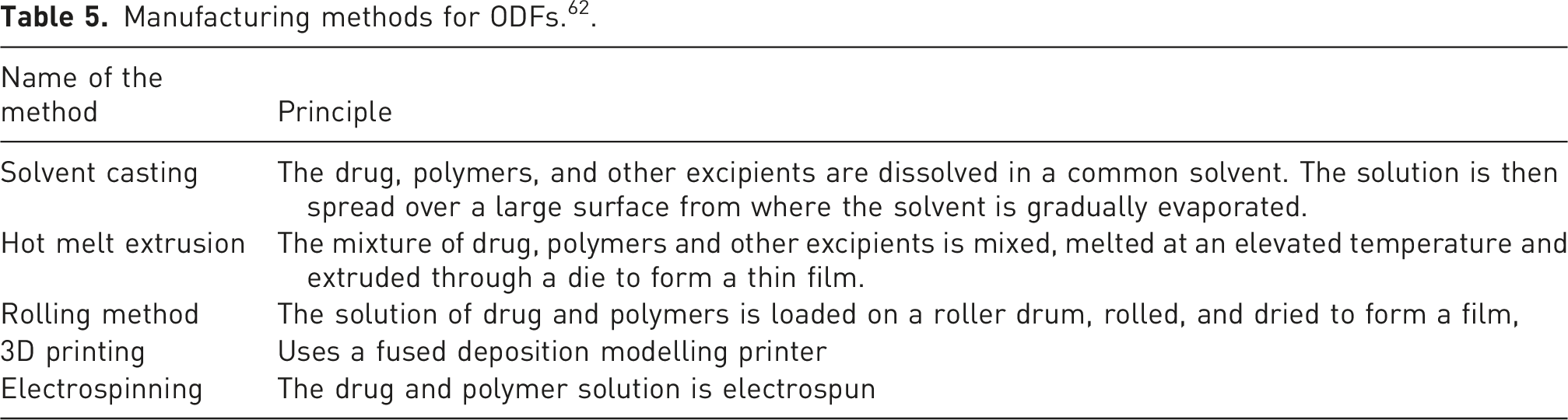
A few other patented technologies used for the manufacturing of ODFs include Pharmfilm®, VersaFilmTM, ThinsolTM, SmartFilm®, BEMA®. ODFs are often evaluated in terms of thickness, content uniformity, tensile strength, percent elongation, degree of swelling, and more significantly the wetting time and disintegration time.
Applications of ODDFs for the treatment of epilepsy
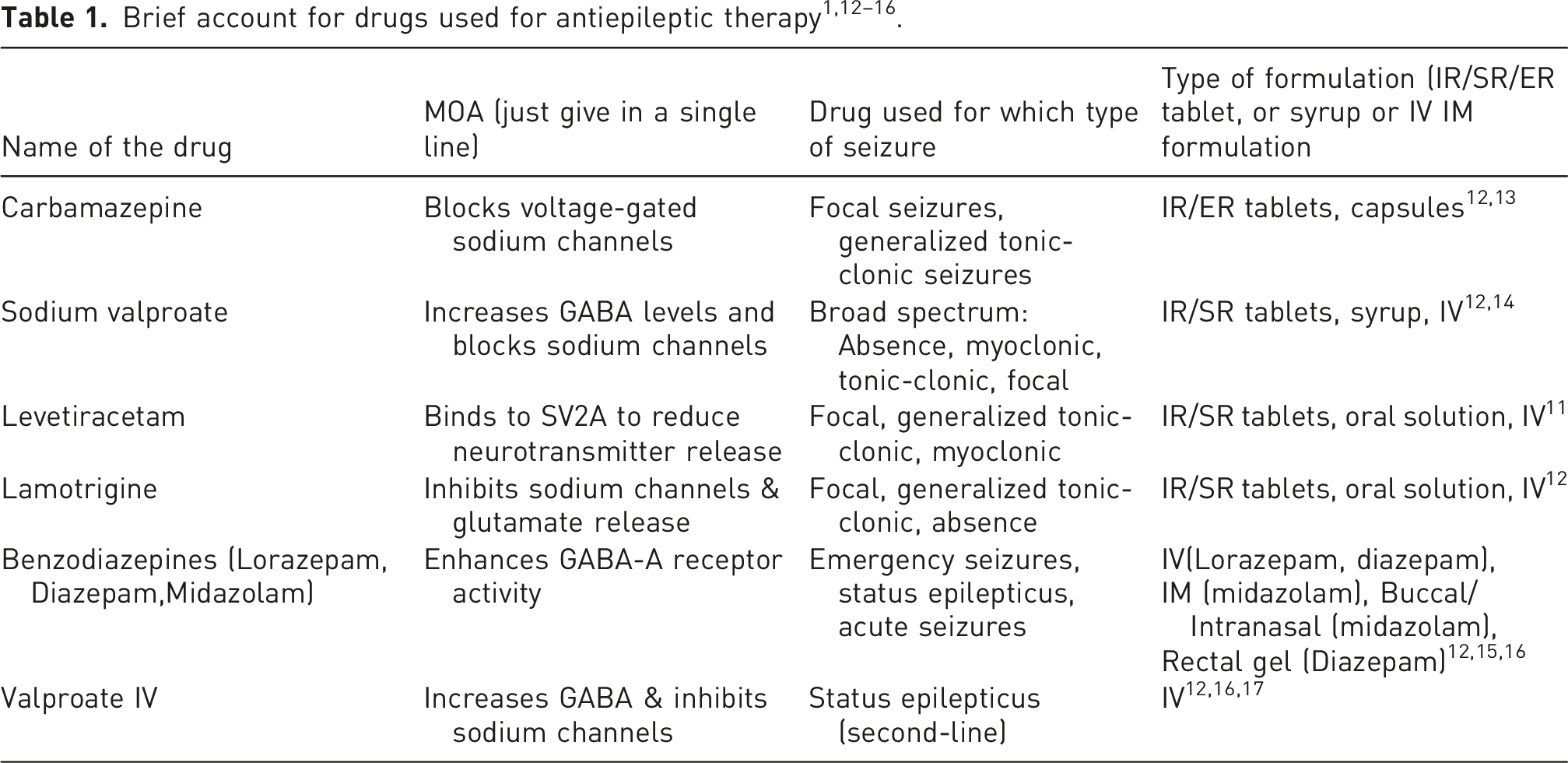
ODDFs represent a significant breakthrough in the patient-friendly approach of drug delivery. This approach can be particularly beneficial for the administration of antiepileptic drugs. Epilepsy management demands accurate dosing, rapid onset of action, and sustained patient adherence—requirements that are often hindered by the conventional oral dosage forms used for the delivery of antiepileptic drugs as stated in Table 1. Epileptic patients often experience dysphagia, cognitive impairment, or postictal confusion, all of which compromise effective oral administration and clinical outcomes.58,59 ODTs which disintegrate rapidly upon contact with saliva obviating the need for water, overcome these challenges by facilitating ease of administration and ensuring accurate dosing even for a non-cooperative patient. Moreover, the rapid disintegration and dissolution of the drugs enable rapid absorption and a faster onset of therapeutic action, which is particularly desirable in preventing seizure recurrence. Improved palatability, portability, and better patient-compliance further boost their therapeutic utility across pediatric, geriatric, and neurologically compromised populations. Thus, ODDFs offer a practical and efficacious platform for antiepileptic drug delivery, corroborating pharmacokinetic performance with the real-time needs of patients and caregivers while achieving better therapeutic outcomes. 65 The following section highlights some of the case studies that demonstrate the development of ODDFs, for the delivery of antiepileptic drugs and the benefits offered by the ODT formulation compared to the conventional ones.
Development of ODDFs for the delivery of antiepileptic drugs
Stiripentol (STP) is the drug of choice for the treatment of ‘Dravet Syndrome’, which is a severe myoclonic epilepsy occurring in infants. It is classified as a resistant childhood epilepsy that is frequently not adequately treated with first-line antiepileptic drugs. STP is a poorly water-soluble drug with low and variable bioavailability that hinders its clinical efficacy. Moreover, STP is formulated as orally administered reconstitutable powders that may be difficult for pediatric patients to swallow. Hence the need to develop an easy to swallow and rapid acting formulation for STP. Affi (2014) incorporated STP in ‘Fast-Dissolving Tablets (FDTs)’ using different concentrations of sodium starch glycol (SSG) and croscarmellose sodium (CCS) as superdisintegrants using direct compression. The effect of the concentration of superdisintegrants on the disintegration time for the formulation was studied and it was found that the formulation containing the highest concentration of SSG (6.6%) and CCS (15%) in combination had the shortest disintegration time (21 s) and the fastest wetting time (22.3 s). The disintegration test was performed in distilled water at 37 ± 2°C using a standard disintegration apparatus, and the wetting time was determined by placing the tablet on tissue paper soaked with 0.5% eosin dye solution until the upper surface was completely wet. The in vitro dissolution study revealed that this formulation achieved nearly complete drug release (99.89%) within just 15 min in 900 mL of phosphate buffer (pH 6.8) containing 0.25% sodium lauryl sulfate (SLS) using the USP Type II dissolution apparatus at 50 rpm. Thus, compared to the conventional tablet lacking superdisintegrants, which released only 41.2% of the drug within the same period, the optimized formulation containing SSG and CCS demonstrated markedly enhanced dissolution and drug availability, confirming the synergistic action of these superdisintegrants in promoting rapid disintegration and efficient drug release. 66
Another compelling case study published by Patel et al. (2024) demonstrates the development of a Pregabalin loaded ODF to address the difficulties associated with delivery of Pregabalin for the treatment of paediatric epilepsy. By avoiding first-pass metabolism, achieving rapid drug release, and masking the natural bitterness of the drug, the researchers hoped to improve patient compliance and clinical outcomes. A solid dispersion of pregabalin with β-Cyclodextrin in a 1:2 ratio was first made using the kneading method to improve the solubility and effectively mask the bitter taste of the drug. The solid dispersion was then loaded in the ODF by solvent casting method. The concentration of the hydrophilic film-forming polymer (HPMC E15) and plasticizer (glycerol anhydrous) were found to be crucial determinants of tensile strength, disintegration time, and drug release in a 32 full factorial design used to optimise the film. The case-study also demonstrated the effectiveness of a Quality by Design (QbD) approach in developing a stable, patient-centric, and fast-acting ODF for antiepileptic drugs. The optimised film incorporating 3% w/v of HPMC E15 and 15% v/v of glycerol anhydrous, along with the solid dispersion containing Pregabalin:β-Cyclodextrin (1:2), demonstrated excellent properties, including a rapid disintegration time of 25 s and a rapid drug release of over 90% within 6 min in comparison to a conventional marketed pregabalin tablet that released only about 60% in the same time-frame. Palatability tests confirmed successful taste masking, and stability studies showed no significant changes the film’s critical attributes over 3 months under accelerated conditions. 67 Stability studies conducted at 40°C ± 2°C/75% ± 5 % RH for 3 months showed no significant changes in tensile strength, disintegration time, or cumulative drug release, confirming the formulation’s stability. Palatability tests confirmed successful taste masking and high acceptability.
In another study, Lacosamide was used as a model antiepileptic drug which when administered orally gave results as 100% bioavailability by in vivo drug release. It shows its mechanism of action by inactivation of voltage gate Na + channels thereby reducing the hyperactivity of brain cells, and exercising effective control in epilepsy. FDTs of Lacosamide were prepared using Guar Gum as a natural superdisintegrant and Microcrystalline cellulose (MCC) was used as a binder/filler in comparative synthetic formulation. The tablets were manufactured by Direct compression method. The optimized batch of compressed tablets containing 5% Guar Gum was found to rapidly disintegrate within 28 s. The wetting time of the formulation was merely 3.48 s, while it absorbed 60% water. The formulation achieved almost complete release within 12 min in a pH 6.8 phosphate buffer. Thus, the developed Lacosamide FDT offered a better alternative than the conventional formulations for the treatment of pediatric epilepsy. 68
Lamotrigine is another antiepileptic drug that is used for pediatric epilepsy. However, the poor water-solubility of the drug restricts a rapid onset of action which is indispensable to epilepsy management. Lamotrigine was coformulated with polyvinylpyrrolidone to form an amorphous solid dispersion which was then mixed with different proportions of superdisintegrants to develop fast-dissolving tablets by direct compression. The optimized formulation containing a higher proportion of Crospovidone disintegrated within 52 s with a wetting time of 18 s. The formulation released almost 92% of the drug within 30 min 69
A study published by Boudria et al. concerns use of a three-dimensional (3D) printed fast-melt formulation of Levetiracetam (LEV) to improve convenience and bioavailability while maintaining pharmacokinetic equivalence to standard tablets. The 3D printing method generated almost porous tablets that were then compared to the conventional immediate-release tablet under fasted and fed conditions in healthy human volunteers. While the fast-melt tablets showed an almost 1.2 times increase in the Cmax compared to the conventional tablets in both fed and fasted conditions., the Tmax, AUC, and t1/2 of both the formulations were almost identical. However, the fast-melt tablet disintegrated in less than 10 s, that of the conventional tablet was almost 3 min.
Furthermore, 3D printing enabled precise dose uniformity and a customised tablet structure. Drug stability was also preserved in the absence of high-temperature and high-stress manufacturing steps like drying and compression. 3D printing thus offered an innovative approach to produce fast-melting levetiracetam tablets that perform equivalently to conventional tablets in the body, combining precise manufacturing with effective therapeutic outcomes. 70
Kandilli et al. developed ODTs of a combination of Carbamazepine and Levetiracetam for pediatric patients freeze-drying (lyophilization) and direct compression methods. The comparative antiepileptic effect of the individual drugs, their combination, and the ODT formulations were evaluated in the rats with pentylenetetrazole (PTZ)-induced epilepsy model. The ODTs prepared by both the methods had optimum hardness, friability values less than 1% and rapid disintegration times. Compared to the seizure scores obtained for groups treated with the individual drugs or combination of drugs, the score obtained for the group treated with ODT was significantly lower. Thus the ODT formulation not only offered a patient compliant approach of combination drug delivery, but also enabled a better therapeutic outcome. 52
The earlier sections emphasise on the importance of coprocessed excipients to develop a tablet blend suitable for direct compression as well as achieving the rapid release typical to ODTs. Teaima et al. explored the effect of different coprocessed excipients on the flow properties, compressibility, and disintegration time of the resultant ODTs. Antiepileptic drug, Leviteracetam was used as the model drug and coprocessed excipients such as Pharmaburst® 500, F-melt® type C, Prosolv® ODT, Prosolv® EasyTab SP, Prosolv® HD90 Prosolv®, EasyTab Nutra, Spress® B820 were investigated by direct compression method. The lowest wetting time and fastest disintegration time was found in the tablets compressed with Pharmaburst® 500 which is a combination of spray-dried mannitol and sorbitol, along with crospovidone and, in some formulations, colloidal silicon dioxide. The presence of crospovidone and mannitol, besides the porous nature of the particles obtained by spray-drying may have been responsible for the rapid wetting and disintegration of the tablets. The tablet released almost 99% of the drug within 10 min. In vivo pharmacokinetic studies performed in male Wistar rats showed a 3x increase in the Cmax and a 4x increase in AUC for the ODT formulation compared to an oral solution of the drugs. 71 This concludes the ability of the ODTs incorporating coprocessed excipients to enhance the bioavailability of the drugs significantly.
Conclusion
Orally disintegrating dosage forms have emerged as a promising alternative to conventional oral dosage forms for the effective management of epilepsy. Their rapid disintegration, ease of administration without water, and improved patient acceptability make them particularly suitable for pediatric, geriatric, and dysphagic patients. This review comprehensively discusses formulation strategies, excipient selection, manufacturing techniques, and evaluation parameters essential for the development of orally disintegrating tablets and films for antiepileptic therapy. The case studies included in this review further demonstrate the practical applicability of orally disintegrating dosage forms, highlighting improvements in disintegration time, dissolution behavior, and overall formulation performance when compared with conventional systems. These studies provide supportive evidence for the feasibility and therapeutic relevance of such dosage forms in epilepsy management. Although challenges such as taste masking, dose uniformity, and stability remain, continuous advancements in formulation technology and excipient engineering are addressing these limitations. Overall, orally disintegrating dosage forms offer a robust and patient-centric drug delivery platform and hold considerable potential for enhancing treatment outcomes and quality of life in patients with epilepsy, supporting their expanded development and future clinical application.
Footnotes
Author contributions
Vanitha Mudhalayar and Yash Bari: Conceptualization of the idea, literature survey, writing the manuscript
Dhruv Bhanushali, Aradhya Gavali, and Tanmay Patil: Literature survey, manuscript writing, proofing
Manasi Chogale: Conceptualization of the idea, manuscript checking, and proof-reading
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.