
Abstract
Keywords
Introduction
Overweight and obesity are associated with elevated blood pressure and high percentage of hypertensive patients are overweight and obese. 1 Subjects gaining weight are at higher risk for hypertension, 2,3 whereas the weight reduction decreases blood pressure levels as well as the complications related to hypertension. 4 Obesity has also been recognized as an independent risk factor for arterial hypertension 5 and, in particular, the Frammingham Heart Study showed that approximately 65–75% of overweight and obese patients are at risk for hypertension. 6 Examining 3216 outpatient subjects who were never treated with antihypertensive medication, Kotsis et al. showed that confirmed ambulatory blood pressure hypertension was found to be higher in both overweight and obese individuals compared with normal weight subjects. 7 As far as fat distribution is concerned, visceral fat has the most important impact on blood pressure elevation. 8
Concerning the mechanism relating obesity to hypertension, most obese humans have increased sympathetic activity. 9 Some authors have recently shown that sympathetic activation is higher in subjects with central than with peripheral phenotype of obesity. 10,11 Moreover, most obese patients have hyperinsulinaemia, and it has been shown that obesity may independently increase insulin resistance; 12 it is well known that insulin stimulates sympathetic activity, 9 and that this effect occurs even when the insulin levels are included within the physiological range. 13 The renin–angiotensin–aldosterone system (RAS) has also been identified as an additional abnormality that can explain the association between obesity and hypertension. 14–16 Lastly, it has been shown that blood pressure and obesity covariation is mediated by circulating high levels of leptin, suggesting that the body fat has only a weak independent effect on blood pressure variation after adjustment for leptin levels. 17
The relationship between obesity and hypertension is widely recognized. However, very few information is presently available on the relationship between body mass index (BMI) and 24-h mean blood pressure levels in normotensive overweight or obese persons or in age- and BMI-matched persons with recent history of hypertension who had never received antihypertensive medication.
It has been also shown that hyperinsulinaemia is determinant for unfavourable metabolic aspects of metabolic syndrome, whereas catecholamines seem to be important for the development of impaired glucose metabolism and hypertension. 18 free thyroxine (FT) FT3 and thyroid stimulating hormone (TSH) serum levels are independently associated with waist circumference, but do not seem to be involved in the pathogenesis of hypertension in this syndrome. 18 At the best of our knowledge, no study has simultaneously evaluated 24-h mean blood pressure levels, insulin concentrations, insulin resistance, 24-h urinary catecholamines, and aldosterone and thyroid function in a population of both overweight and obese subjects, with or without hypertension, in the absence of any antihypertensive treatment.
Therefore, the present study was addressed to examine whether some of anthropometric parameters, hormones (insulin, TSH, FT3 and FT4 serum levels, daily urinary catecholamines, and aldosterone concentrations), and metabolic variables may predict 24-h mean blood pressure levels in overweight and obese patients. To this aim, a cohort of 180 euthyroid overweight and obese patients, aged 20–63 years, without or with recently diagnosed hypertension, was investigated.
Methods
Subject population
The patients were consecutively enrolled at the outpatient clinic for the Study of Hypertension, Department of Internal Medicine and Clinical Oncology, University of Bari, School of Medicine. Concerning the inclusion criteria, they were recruited at the first medical examination in the absence of antihypertensive drugs. In addition, they showed a BMI higher than 25.0 kg/m2. All of them were addressed to the outpatient clinic by their general practitioners because of a recent increase of their ambulatory blood pressure levels.
To obtain the selected population for this study, patients with the following disorders were excluded: endocrinological diseases, diabetes mellitus, stroke, transient ischaemic attack, angina pectoris, heart infarction, claudicatio intermittens, congenital heart disease, and electrocardiogram abnormalities. Patients with impaired FT3 and FT4 levels were also excluded. Thus, the study enrolled 180 patients, including 80 women and 100 men, aged 20–63 years.
All subjects gave their informed consent for the study, which was performed in accordance with the guidelines proposed in the Declaration of Helsinki.
Among women, 61 were premenopausal and 19 were postmenopausal. Twenty-five subjects were smokers and included eight among normotensive and 17 among hypertensive subjects. All patients reported to have normal fasting blood glucose (FBG) levels, eight had a FBG ≥126 mg/dl, but lower than 140 mg/dl.
All study subjects were judged in good health on the basis of physical examination, medical history, routine blood work, urinalysis, and electrocardiogram. None of patients were receiving any medication (including oral contraceptives for pre-menopausal women and hormone replacement therapy for post-menopausal women) since at least 3 months before the enrolment into the study. Moreover, none of them had been involved into intensive or competitive physical activity prior to the enrolment. During the testing period, all subjects were asked to keep their normal mixed diet and not to perform any sporting activity. The day before the measurement, they were abstained from both caffeinated and alcoholic drinks but maintained their normal diet.
Anthropometric measurements and general data
Body weight was measured to the nearest kg. Height was determined to the nearest cm. BMI was calculated as the weight (kg) divided by the square of height (m2). Waist circumference was measured at the narrowest part of the abdomen, i.e. at the natural indentation between the tenth rib and the iliac crest (minimum waist).
Blood pressure measurements
Outpatient clinic blood pressure was recorded on at least three different occasions, using a mercury manometer with an appropriate cuff size. Ambulatory blood pressure was measured with 15-min intervals from 0700 to 2300 and with 30-min intervals from 2300 to 0700 for consecutive 24 h, starting from 0830 (Ultralite ABPM Monitor 90217; SpaceLabs Media Inc, Redmond, WA). Heart rate was measured over 24 h by the same instrument. According to the 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension, 19 hypertension was confirmed when 24-h mean systolic blood pressure was ≥125 mmHg and/or 24-h mean diastolic blood pressure was ≥80 mmHg. Thus, 118 subjects were affected by hypertension, whereas 62 individuals were normotensive. Among the hypertensive population, 75 subjects were men and 43 individuals women. Among normotensive subjects, 25 individuals were men and 37 were women.
Hormone and metabolic parameters
Blood samples were drawn between 0800 and 0900 after an overnight fast, within 1 week from the day of the ambulatory blood pressure measurement. Serum insulin concentrations were measured by radioimmunoassay (Behring, Scoppitto, Italy) and intra- and interassay coefficients of variation were 3.7% and 7.5%, respectively. Serum TSH, FT3, and FT4 serum levels were measured as previously described. 20
24-h urine collection was performed within 1 week from the day of the ambulatory blood pressure measurement. 24-h urine catecholamines were determined as previously described. 20 24-h urinary aldosterone was measured by solid-phase RIA by the Coat-A-Count method (Diagnostic Products Corp, Los Angeles, CA). The intrassay coefficient of variation was 4.0% and the interassay coefficient of variation was 6.4%.
Plasma glucose levels were determined by the glucose-oxidase method (Sclavo, Siena, Italy). Plasma lipids (triglycerides, total cholesterol, and high-density lipoprotein (HDL) cholesterol) were determined by an automatic colorimetric method (Hitachi; Boehringer Mannheim, Mannheim, Germany).
Insulin resistance was assessed by using the homeostasis model assessment (HOMAIR). 21
Statistics
Results were calculated as mean and standard deviation (SD) for all parameters. Student’s t-test for independent samples was used to evaluate the differences between the groups for continuous variables. Categorical variables are given as frequencies and percentages, and were compared between groups by the chi-squared test. To the aim of determining the predictors of high 24-h systolic and diastolic blood pressure levels (≥125 mmHg and/or ≥80 mmHg, respectively), the odds ratio (OR) was calculated by univariate logistic regressions. Variables having a univariate probability value <0.05 were selected for inclusion in a multivariable logistic regression model. The OR and 95% confidence interval (CI) were computed per unit of standard deviation increase of the continuous analysed variable.
Concerning the statistical power of the study, the sample size provided >80% of the power to detect differences between groups, >50% of the standard deviation of the continuous variable, and a odds ratio >3.0 for the association between 24-h systolic and diastolic mean blood pressure levels and dichotomous variables (gender and smoking). p values of <0.05 were considered statistically significant. Statistical power was analysed using STATISTICA Power Analysis (StatSoft, Tulsa, Oklahoma) and the statistical analyses were made using STATISTICA version 6.1 (StatSoft).
Results
Men had a significant higher prevalence of hypertension than women (p < 0.01) and the percentage of smokers was significantly (p < 0.05) higher in the group of hypertensive patients (18%) than in that of normotensive subjects (6%).
General and anthropometric parameters, ABPM data, and metabolic and hormone variables in normotensive and hypertensive subjects
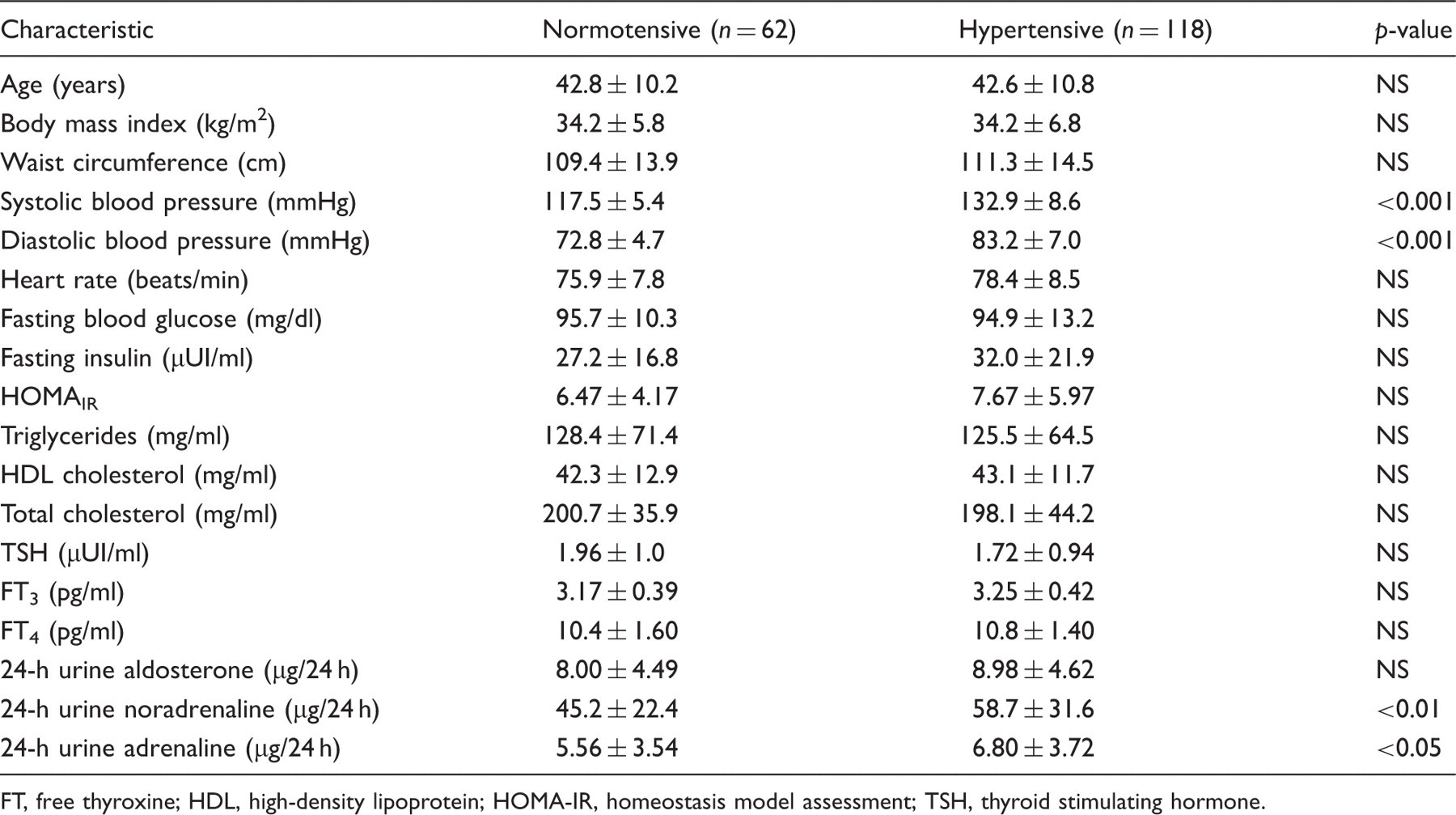
FT, free thyroxine; HDL, high-density lipoprotein; HOMA-IR, homeostasis model assessment; TSH, thyroid stimulating hormone.
Several univariate and multivariate logistic regression analyses, with the determination of odds ratio (OR), was performed to evaluate the predictive factors of high 24-h blood pressure mean values. It is noteworthy that 77 patients had high systolic and high diastolic blood pressure levels, 31 had only high systolic blood pressure levels, and 10 had only high diastolic blood pressure levels.
The ORs and their 95% CIs estimating the association between the analysed parameters and high blood pressure levels are illustrated in Figures 1–3. It is noteworthy that categorical variables (sex, smoking, and physical activity) have been evaluated in the statistical analyses, but they are not represented in the figures. Physical activity was not predictive of higher blood pressure in all analyses (data not shown).
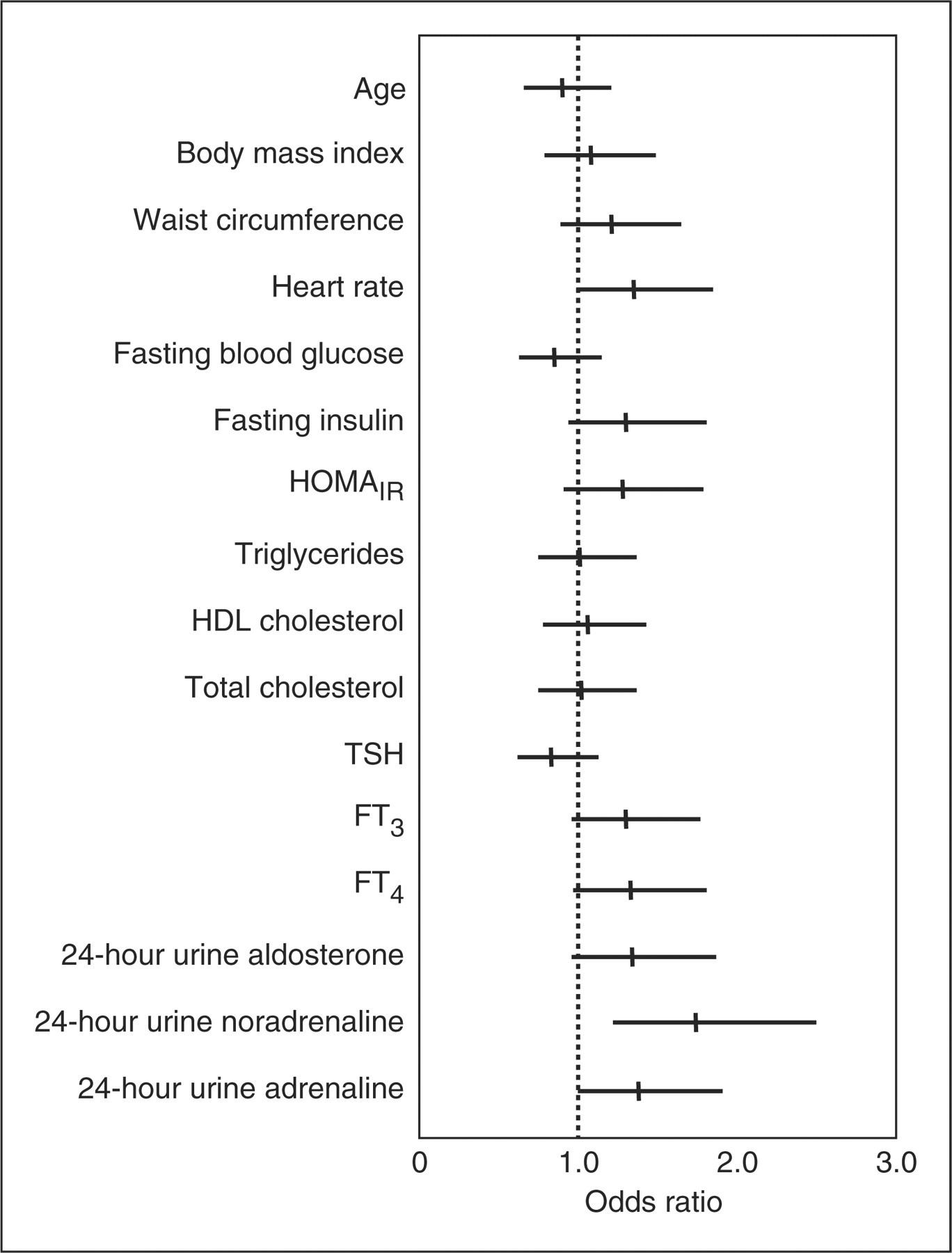
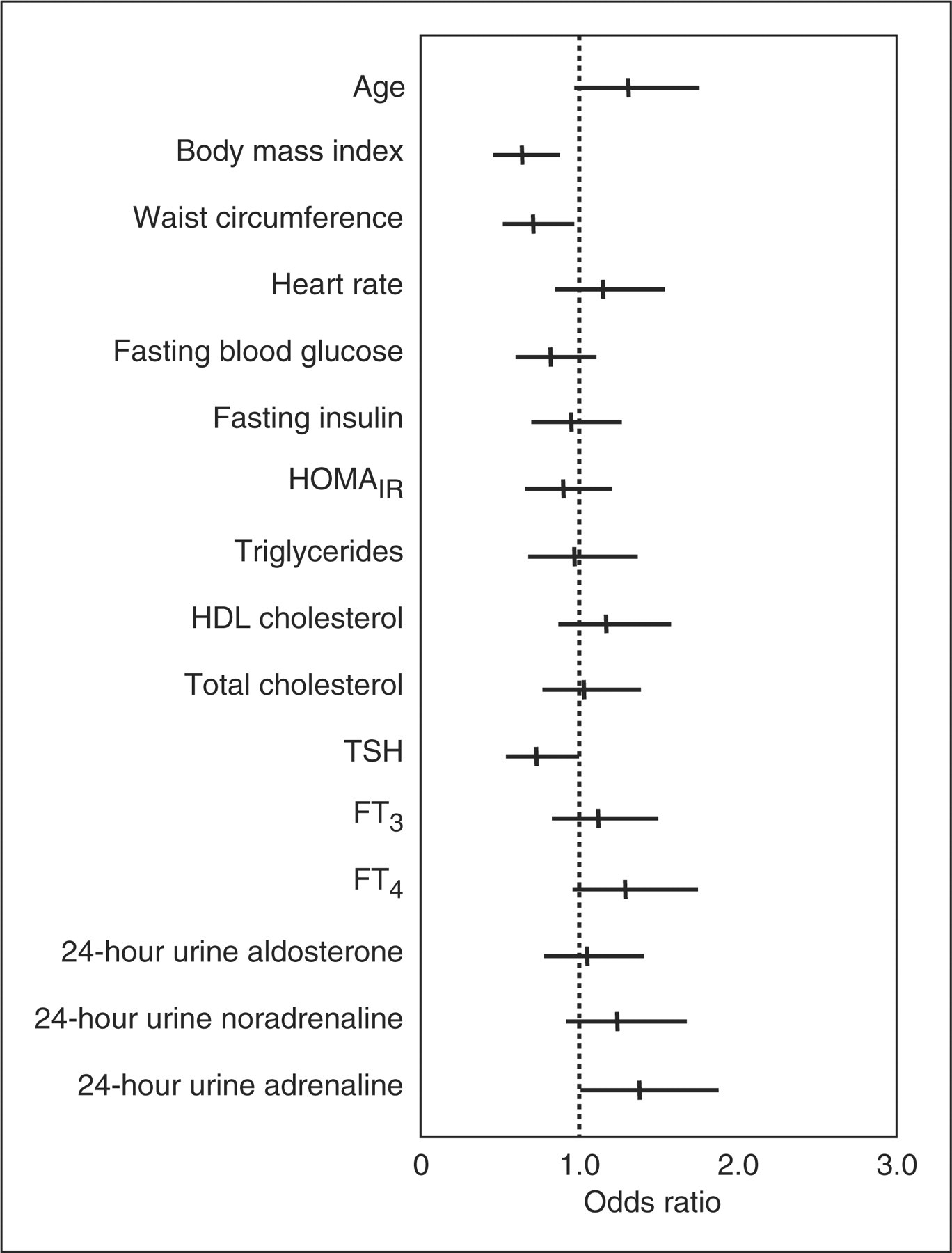
Odds ratios and 95% confidence intervals for 24-h systolic blood pressure mean values >125 mmHg or diastolic blood pressure mean values >80 mmHg. Odds ratios and 95% confidence intervals for 24-h systolic blood pressure mean values >125 mmHg. Odds ratios and 95% confidence intervals for 24-h diastolic blood pressure mean values >80 mmHg.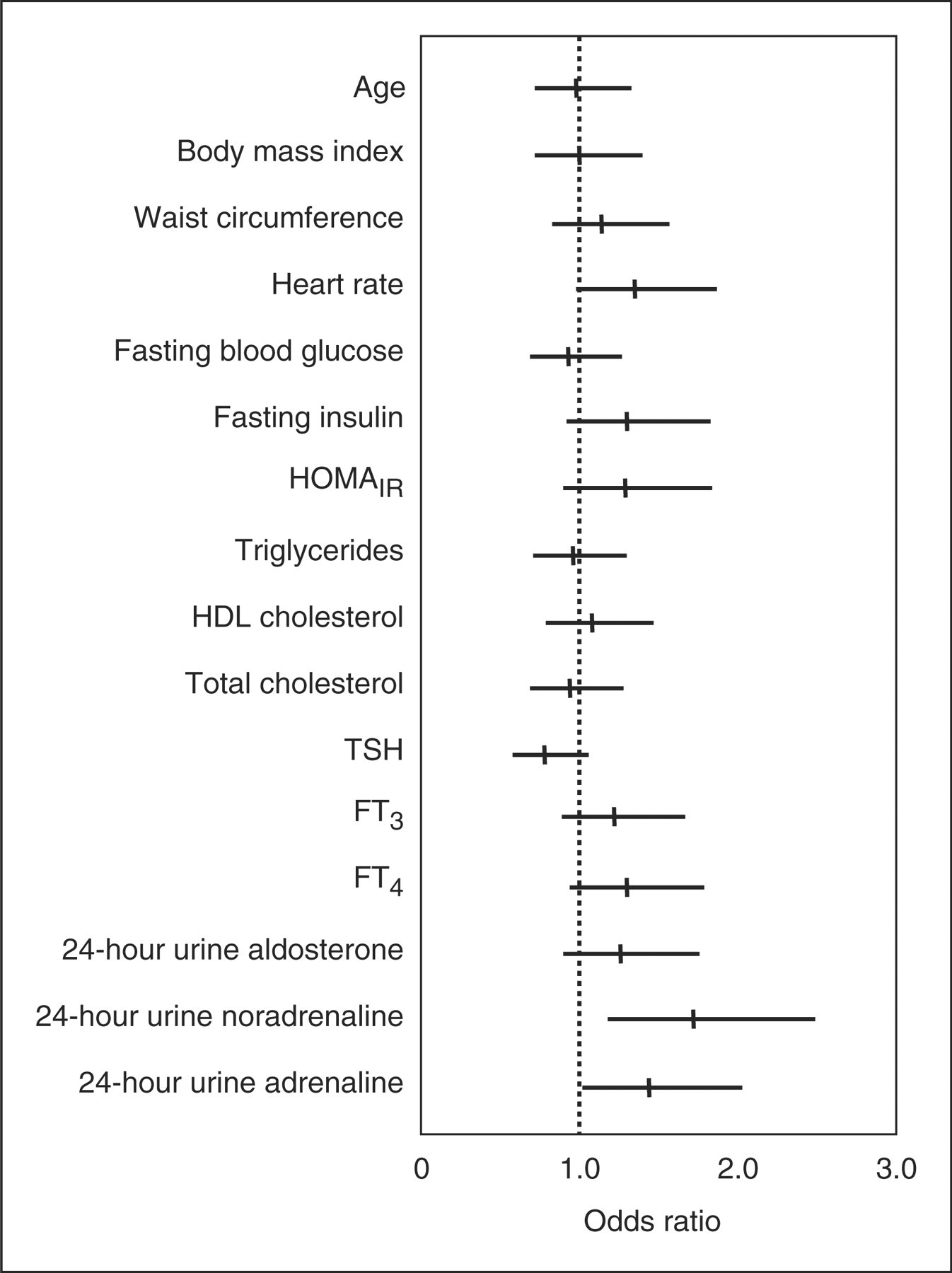
The ORs and their 95% CIs estimating the association between the analysed parameters and high systolic and/or high diastolic blood pressure levels are illustrated in Figure 1. Univariate analysis showed a positive association of hypertension with male gender (OR 2.58, 95% CI 1.37–4.87, p = 0.003), smoking (OR 3.14, 95% CI 1.02–9.67, p = 0.045), noradrenaline (OR 1.72, 95% CI 1.18–2.49, p = 0.004), and adrenaline (OR 1.44, 95% CI 1.02–2.03, p = 0.035). However, multivariate analysis showed an independent association of hypertension only with male gender (OR 2.00, 95% CI 1.03–3.90, p = 0.039) and noradrenaline levels (OR 1.52, 95% CI 1.03–2.25, p = 0.032).
The ORs and their 95% CIs estimating the association between the analysed parameters and high systolic blood pressure levels are illustrated in Figure 2. Univariate analysis showed a positive association of high systolic blood pressure with male gender (OR 2.13, 95% CI 1.15–3.92, p = 0.015), smoking (OR 4.10, 95% CI 1.33–12.61, p = 0.013), noradrenaline (OR 1.74, 95% CI 1.22–2.5, p = 0.002), and adrenaline (OR 1.38, 95% CI 1–1.91, p = 0.048). However, multivariate analysis showed an independent association of high systolic blood pressure only with noradrenaline levels (OR 1.58, 95% CI 1.08–2.31, p = 0.016).
The ORs and their 95% CIs estimating the association between the analysed parameters and high diastolic blood pressure levels are illustrated in Figure 3. Univariate analysis showed a relationship of high diastolic blood pressure with BMI (negative correlation) (OR 0.64, 95% CI 0.46–0.88, p = 0.007), waist circumference (negative correlation) (OR 0.71, 95% CI 0.52–0.97, p = 0.029), TSH (negative correlation) (OR 0.73, 95% CI 0.54–1, p = 0.045), and adrenaline (OR, positive correlation) (OR 1.38, 95% CI 1.01–1.88, p = 0.040). However, multivariate analysis showed an independent association of high diastolic blood pressure only with BMI (negative correlation) (OR 0.64, 95% CI 0.46–0.9, p = 0.009). It is noteworthy that the multivariate analysis was performed excluding waist circumference from the model because of its collinearity with body mass index (Pearson correlation coefficient 0.87; p < 0.001).
Discussion
At the best of our knowledge, this is the first study examining the relationship between BMI and 24-h mean blood pressure levels in euthyroid overweight and obese subjects, normotensive or with recently developed hypertension, who had never received antihypertensive medication.
The strongest novel finding of this study was the negative association between BMI and diastolic blood pressure, independently from other variables showing a significant correlation with diastolic blood pressure. This result is apparently surprising since a direct relationship between central obesity and hypertension is postulated, and this association is commonly attributed to increased sympathetic nerve activity, as assessed by microneurography and catecholamine assays. 9–11 However, first, Agapitov et al. 22 have recently shown that sympathetic vascular tone in the forearm circulation is not increased in obese normotensive subjects, despite increased sympathetic outflow. This suggestion is in line with our findings, since 24-h urine noradrenaline and adrenaline levels were higher in hypertensive as compared to normotensive subjects, but the daily urinary noradrenaline was not independently associated with systolic or diastolic blood pressure. Agapitov et al. have suggested that vasodilator factors or mechanisms occurring in obese normotensive subjects could oppose the vasoconstrictor actions of increased sympathoactivation, thus explaining why some obese subjects are protected from the development of hypertension. Interestingly, progressive weight gain is associated to an increase, and not to a decrease, of the blood flow in adipose tissue and in other tissues (heart, kidneys, gastrointestinal tract, and skeletal muscle). 23 Second, total peripheral resistance in obese hypertensive patients is less elevated than it would be expected in the lean hypertensive subjects. 23 Vasodilation in tissues appears to be due, at least in part, to increased metabolic rate and local accumulation of vascular metabolites, as well as to organ and tissue growth in response to increased metabolic demands. 23 Third, perivascular fat produces several substances that exert inhibitory action on the contraction of arterial wall and are in balance with other substances having contractile action. 24 Fourth, elevated blood pressure has been shown in transgenic lipoatrophic mice. 25
Therefore, it may well be that both vasodilation and blood flow increase prevail in normotensive subjects and/or in individuals who recently developed hypertension, thus possibly explaining the inverse relationship between BMI and diastolic blood pressure in the present study. In addition, it may well be that more muscle mass in overweight and obese subjects who have not yet developed stable hypertension has a healthful and protective effect. By contrast, it is possible that vasoconstriction and decrease in blood flow would prevail when atherosclerosis or mechanisms related to hypertension have become stable or when the kidney dysfunction starts.
There is an ongoing debate on whether insulin resistance is a cause or a consequence of hypertension or whether both conditions arise from a common substrate though the clinical investigations have not yielded consistent results.
Insulin and HOMAIR were not significantly different between hypertensive and normotensive subjects and were not associated to hypertension or to systolic or diastolic blood pressure levels in this study. These findings are in line with cross-sectional or prospective reports showing an attenuation of the association between insulin resistance and the risk of hypertension on adjustment for BMI or baseline blood pressure. 17,26–35 In a recent 4-year longitudinal study, performed in a large community-based sample, reduced insulin sensitivity predicted blood pressure tracking in young people with normal BMI. By contrast, insulin sensitivity was not related to incidence of hypertension in obese participants. 36 Further studies should probably examine the relationship between insulin and blood pressure by using ABPM.
As expected, men had a significant higher prevalence of hypertension than women, and hypertension was associated independently with male gender.
According to previous studies performed in overweight and obese subjects, 17 thyroid hormones were not significantly associated with blood pressure levels.
Concerning the study limitations, this study has not compared normal weight and overweight and obese subjects. Unfortunately, we were not able to involve a sufficient number of normal weight normotensive subjects, but we have little reason to believe that inclusion of normal weight subjects should have changed the conclusions of the study. It is to note that the same subjects enrolled in the present study are going to be examined in a follow-up study.
In conclusion, the present study, performed in overweight and obese subjects, either normotensive or with recently discovered hypertension, shows that BMI is negatively and independently associated with diastolic blood pressure, supporting the hypothesis that adipose tissue accumulation is responsible for a decrease (and not an increase) in diastolic blood pressure, before the hypertensive state becomes stable. Moreover, it confirms that male gender and daily noradrenaline production contribute to higher systolic blood pressure in these subjects. Lastly, it seems to exclude a significant role of hyperinsulinaemia and/or insulin resistance and/or thyroid hormones in the early increase of blood pressure.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.