
Abstract
Introduction
The collateral circulation may prevent ischaemia and protect against tissue damage and infarction. 1 The collateral circulation may therefore constitute an effective rescue system against the detrimental effects of atherosclerotic stenosis and, ultimately, deficits in blood perfusion. The heterogeneity in the degree of collateralization among patients with coronary artery disease (CAD) is poorly understood. Several contributing factors have been reported in relation to collateral development. These include the severity of coronary artery stenosis,2,3 as well as the levels of inflammatory cells 4 and certain growth factors such as vascular endothelial growth factor 5 and angiopoietin. 6
B-type natriuretic peptide (BNP) is synthesized in the ventricular myocardium in response to ventricular stretching and wall stress. The role of BNP in the diagnosis and prognosis of heart failure has been studied in quite considerable depth. Recently, natriuretic peptide was demonstrated to act as a regulator of endothelial regeneration and formation of new blood vessels in animal studies, and an in-vitro study also indicated that natriuretic peptide is a strong stimulator for angiogenesis. 7 – 10 Very little is known about the relationship between the level of BNP in plasma and development of the collateral circulation in patients with CAD, and we sought to clarify this relationship in the present study.
Patients and methods
Ethical approval of the study
This study was carried out according to the regulations set by the Ethical Guidelines Committee of Zhejiang University College of Medicine (Zhejiang, China). All patients provided written informed consent to participate in the study.
Patient recruitment
Between April 2008 and August 2009, 311 consecutive patients with chronic stable angina who underwent coronary angiography were recruited in this study. Exclusion criteria were patients with symptoms of congestive heart failure or a left ventricular ejection fraction of <45% at echocardiographic evaluation; any inflammatory or infectious disease; peripheral vascular disease (transient ischaemic attack, stroke, intermittent claudication, peripheral revascularization, amputation); idiopathic dilated or hypertrophic cardiomyopathy; renal failure (serum creatinine >2.0 mg/dl); severe hepatic diseases; or known malignancies.
Coronary angiographic analysis
Coronary angiography was carried out using a conventional technique. Images were obtained in routine standardized projections and assessed using an automated quantitative coronary artery stenosis assessment programme. Standard selective coronary angiography with at least four views of the left coronary artery and two views of the right coronary artery was performed. For analyses of the effect of multivessel disease on coronary collateral development, the number of diseased vessels was identified according to the number of major coronary arteries having ≥75% stenosis. 5
Collateral grading was carried out by two experienced cardiologists who were not informed of the clinical characteristics and biochemical results of the study group. Coronary collateral development was graded according to the Cohen–Rentrop method 11 : grade 0 (no filling of any collateral vessel); grade 1 (filling of side branches of the artery to be the epicardial segment); grade 2 (partial filling of the epicardial artery by collateral vessels); and grade 3 (complete filling of the epicardial artery by a collateral vessel).
Patients were then divided into three groups according to their collateral grades. The ‘normal group’ consisted of patients with normal coronary angiography findings and grade-0 collaterals. The ‘poor collateral group’ comprised patients with at least one vessel having ≥75% stenosis and grade-0 or grade-1 collaterals. The ‘good collateral group’ consisted of patients with at least one vessel having ≥75% stenosis and grade-2 or grade-3 collaterals. 4
Blood sampling
Blood samples were drawn by venipuncture into tubes containing EDTA, citrate, or serum separator gel. Lipid and apolipoprotein parameters were determined in EDTA plasma, C-reactive protein (CRP) in sera and fibrinogen in citrate plasma. Samples were processed immediately by centrifugation at 1000 g and 4 °C for 20 min, then creatine kinase-MB (CK-MB) levels were evaluated by immunosuppression, troponin I (TNI) levels were by chemiluminescence, CRP levels were by immunoturbidimetric assay, glucose levels were by hexokinase, creatinine levels were by picric acid method and the serum lipid profiles comprising total cholesterol, triglyceride, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol were estimated using routine enzymatic methods.
The serum lipid profiles comprising total cholesterol, triglyceride, and LDL cholesterol were estimated using routine enzymatic methods. HDL cholesterol was quantitated using the same enzymatic method after precipitation of the plasma with phosphotungstic acid in the presence of magnesium ions.
Blood samples were obtained immediately before angiography. BNP levels were evaluated using Bayer ADVIA Centaur analyzer (Bayer Diagnostics, Tarrytown, New York). The intra-assay and inter-assay coefficients of variation were 5% and 6%, respectively. The lower limit of detection of the assay was 0.05 pg/ml. Laboratory personnel were blinded to the results of diagnosis and coronary angiography.
Echocardiography
Two-dimensional and M-mode resting echocardiographic recordings were obtained using commercially available instruments (GE, vivid 7) in accordance with the recommendations of the American Society of Echocardiography. Two-dimensional apical two- and four-chamber views were used for volume measurements, from which ejection fraction was derived. 12 Left ventricular dimensions at end diastole [LVEDd (cm)] and end systole (LVESd) were measured at the papillary muscle level from the parasternal short-axis view, and LVEDd and LVESd were used to calculate left ventricular ejection fraction [LVEF (%)]. Left atrium dimension (LA) was measured at the end systole on the basis of an M-mode recording at the level of the aortic root.
Statistical analysis
Continuous variables were given as mean ± standard error. Categorical variables were defined as percentages. Data were tested for normal distribution using the Kolmogorov–Smirnov test. The Student’s t-test and one-way ANOVA followed by Bonferroni posthoc analysis were used for continuous variables and the chi-square test for categorical variables. Multiple ordinal logistic regression analysis was applied to identify factors that correlated with the Cohen–Rentrop score. All tests of significance were two-tailed. Statistical significance was defined as p < 0.05.
Results
Patient enrolment and characterization of study groups
Baseline characteristics of the study population
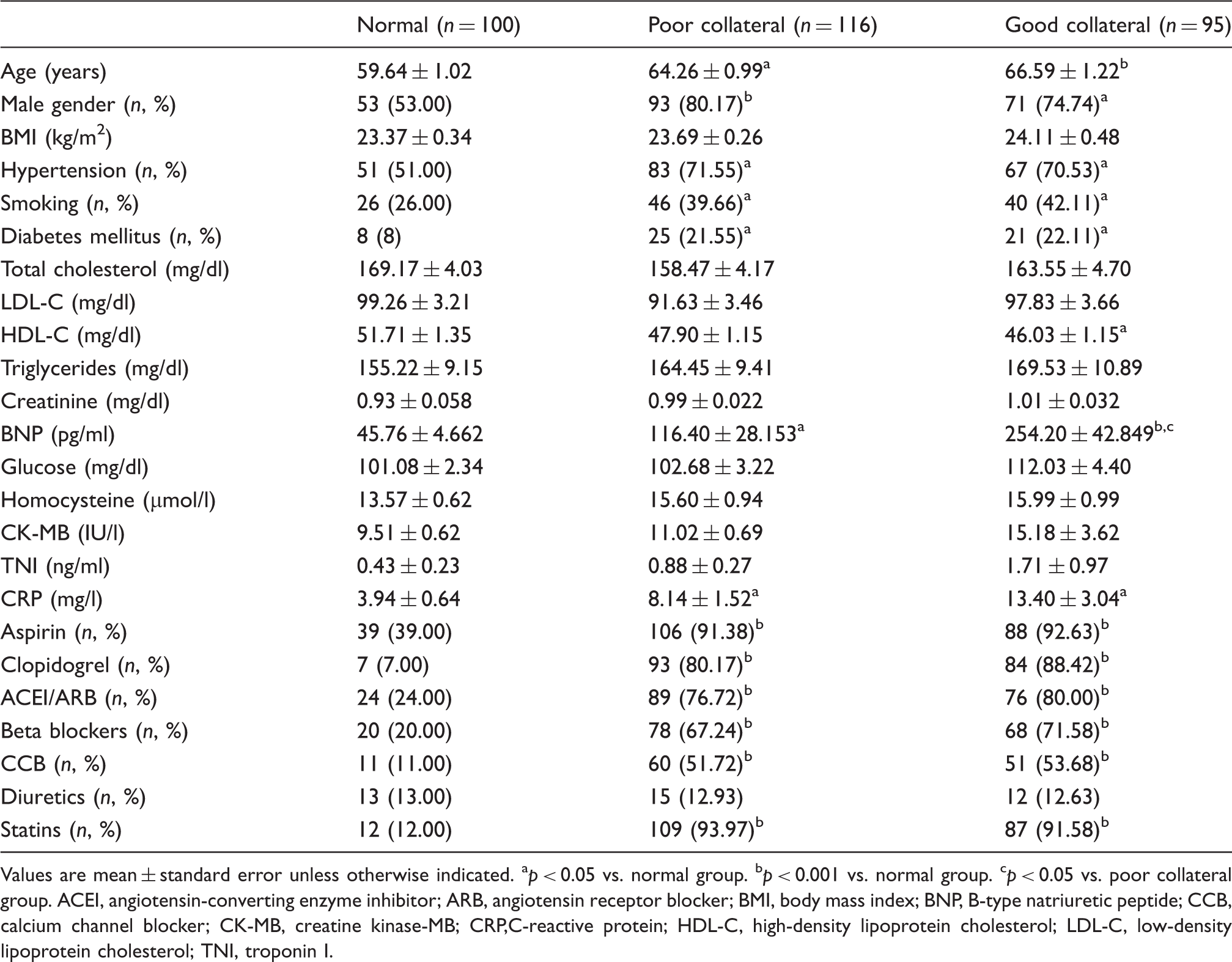
Values are mean ± standard error unless otherwise indicated.
p < 0.05 vs. normal group.
p < 0.001 vs. normal group.
p < 0.05 vs. poor collateral group.
ACEI, angiotensin-converting enzyme inhibitor; ARB, angiotensin receptor blocker; BMI, body mass index; BNP, B-type natriuretic peptide; CCB, calcium channel blocker; CK-MB, creatine kinase-MB; CRP,C-reactive protein; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TNI, troponin I.
Compared with the normal group, the good collateral group, and poor collateral group were older and had more male patients, higher C-reactive protein (CRP) levels, and a higher number of subjects who smoked. The prevalence of hypertension, diabetes, and use of cardiovascular medication were also higher in the good collateral group and poor collateral group than in the normal group. Significant differences in baseline characteristics between the good collateral group and poor collateral group were not observed.
Echocardiographic parameters
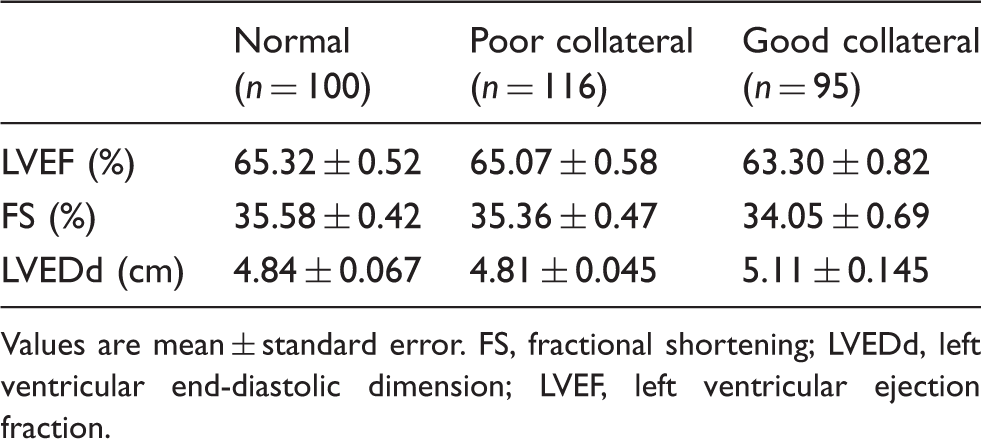
Values are mean ± standard error.
FS, fractional shortening; LVEDd, left ventricular end-diastolic dimension; LVEF, left ventricular ejection fraction.
Angiographic characteristics
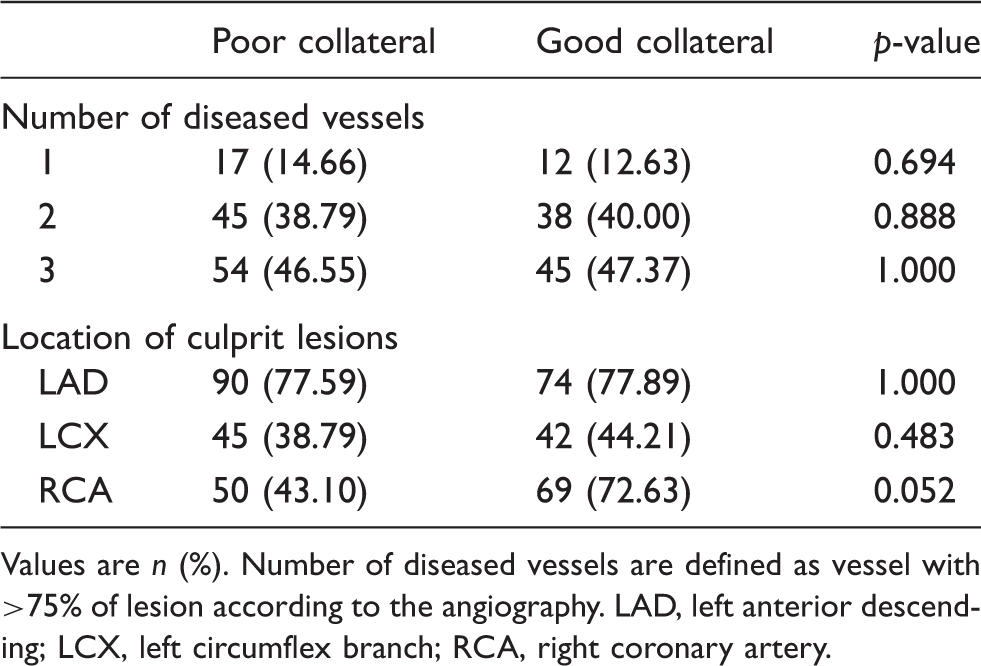
Values are n (%).
Number of diseased vessels are defined as vessel with >75% of lesion according to the angiography.
LAD, left anterior descending; LCX, left circumflex branch; RCA, right coronary artery.
BNP and analysis of the Cohen–Rentrop score
Relationship between Cohen–Rentrop score and clinical and laboratory parameters
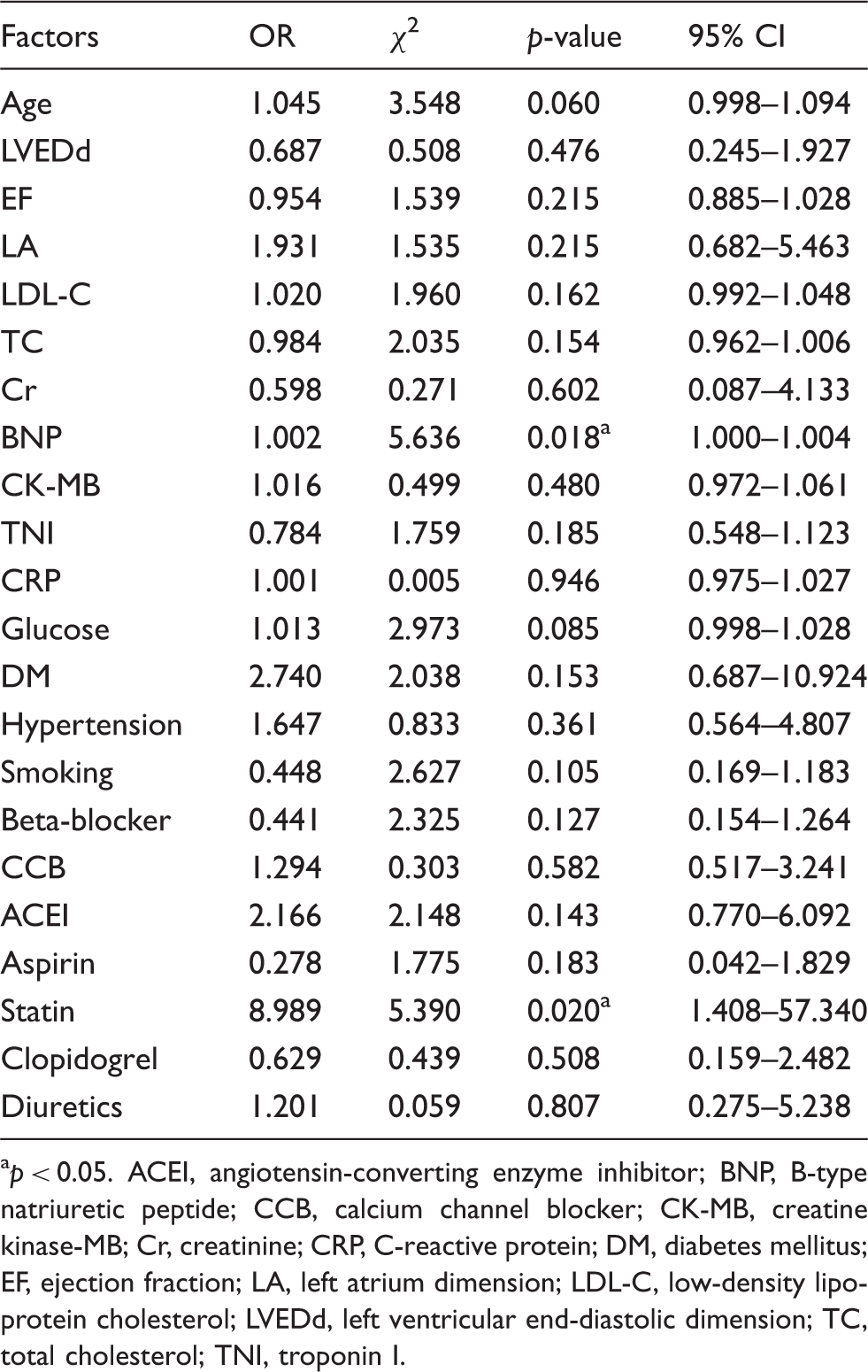
p < 0.05.
ACEI, angiotensin-converting enzyme inhibitor; BNP, B-type natriuretic peptide; CCB, calcium channel blocker; CK-MB, creatine kinase-MB; Cr, creatinine; CRP, C-reactive protein; DM, diabetes mellitus; EF, ejection fraction; LA, left atrium dimension; LDL-C, low-density lipoprotein cholesterol; LVEDd, left ventricular end-diastolic dimension; TC, total cholesterol; TNI, troponin I.
Multiple ordinal logistic regression analysis was done to identify factors that correlated with the collateral Cohen–Rentrop score. The model showed that the BNP level (χ2 = 5.636, OR = 1.002, 95% CI 1.000 to 1.004, p = 0.018) and statin (χ2 = 5.390, OR = 8.989, 95% CI 1.408 to 57.340, p = 0.020) correlated well with the Cohen–Rentrop score. The correlation between the Cohen–Rentrop score and BNP was independent of diabetes mellitus, hypertension, smoking, levels of total cholesterol, LDL cholesterol, glucose level, creatinine, CK-MB, TNI, CRP, LVEF, LA, and LVEDd as well as other medications are shown in Table 4.
Discussion
Recently, experiments revealed that BNP is a potent activator of angiogenesis and arteriogenesis. Enhanced angiogenesis was observed in the development of terminal heart failure, and BNP level was positively associated with the potent in-vivo inducer of neovascularization, angiogenin. 13 BNP systemically overproduced in mice accelerated angiogenesis in tissue ischaemia with activation of the cGMP/cGK pathway (an important signal pathway in angiogenesis). 9 Kuhn et al. 14 demonstrated that in ischaemic skeletal muscle or cardiomyocytes, BNP stimulated the proliferation, migration, and angiogenic sprouting of microvascular endothelial cells, and that this regulation of regeneration of neighbouring endothelia was through activation of the receptor guanylyl cyclase-A in a paracrine manner. The guanylyl cyclase-A receptor is expressed in many tissues and ablation of the endothelial receptor impaired ischaemic limb arteriogenesis and angiogenesis. Another study showed that BNP treatment also promotes vessel growth by increasing the number of endothelial progenitors and enhancing the proliferation capacity of human endothelial progenitor cells as well as their adhesive, migratory, and tube-formation properties. 10 Taken together, these studies suggested that BNP function is a strong regulator of angiogenesis and arteriogenesis in vivo and in vitro. In the present study, it was found that the BNP level in plasma was related to the development of coronary collateral vessels in CAD patients. Patients with good collateral development had a higher level of plasma BNP than normal patients. BNP levels have been shown to be primarily affected by the severity of left ventricular dysfunction, age, 15 exercise-based cardiac rehabilitation,16,17 and severity of coronary lesions. 2 In the present study, BNP differences between the normal group and the poor collateral group should therefore be mainly due to coronary lesions and older age in the poor collateral group. When compared with the good collateral group and poor collateral group, there were no significant differences in LVEF, LVEDd, age, and severity of coronary lesions, whereas the BNP level was twofold higher in patients with good collaterals than in those with poor collaterals. A higher level of BNP in the good collateral group should be mainly due to the extent of collateral formation, which was the only difference between the two groups. The association between plasma levels of BNP and collateral development existed even after adjusting the multivariable model for ejection fraction and other cardiovascular risk factors. The BNP level was therefore an independent predictor of collateral formation. This was the first study illustrating the relationship between plasma BNP level and collateral formation in CAD patients.
A large body of evidence has demonstrated that an increased level of BNP is also strongly correlated with severity of myocardial ischaemia.2,3 An elevated level of BNP therefore reflects a greater degree of myocardial ischaemia and left ventricular dysfunction and, unsurprisingly, was reported to be associated with a higher risk of death. 18 It seems that the present study, which demonstrated that an elevated level of BNP is positively associated with good collateral circulation, is not in accord with the previous hypothesis. One explanation for this discrepancy is that collateral formation has a complex role on prognosis in CAD patients. Good collateral circulation does not always mean better prognosis when comparing CAD patients with different extents of ischaemia burden. Myocardial ischaemia is a potent trigger for collateral formation, and the severity of myocardial ischaemia is positively correlated with collateral formation 19 but, simultaneously, myocardial ischaemia has a deleterious effect on cardiovascular mortality and morbidity. The benefit derived by the collateral circulation may therefore be masked by the harm from extensive myocardial ischaemia burden. Patients with collateral formation may have a poorer prognosis than patients without collateral formation but have less severe myocardial ischaemia. The controversial results yielded by studies assessing the effect of the collateral circulation on cardiac events and survival may be accounted for (at least in part) by differences in the extent of vessel stenosis and myocardial ischaemic burden. The severity of myocardial ischaemia should therefore be considered in a more comprehensive study to demonstrate the role of collateral formation on the prognosis in CAD patients. In the present study, the severity of myocardial ischaemia would not have been a factor because the good collateral group and poor collateral group had almost the same extent of vessel stenosis.
In conclusion, this study showed that, in a series of consecutive CAD patients, the good collateral group had a higher level of BNP in plasma, and that collateral formation was strongly correlated with plasma BNP level. Nevertheless, there was one limitation in the study protocol: we did not measure other angiogenic or inflammatory molecules that could have affected the results.
Footnotes
*
These authors contributed equally to this work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.