
Abstract
Keywords
Introduction
Inflammation plays an essential role in the initiation, progression, and rupture of atherosclerotic lesions. 1 Elevated levels of inflammatory markers, particularly C-reactive protein (CRP), are associated with an increased risk for cardiovascular events both in healthy individuals as well as in individuals with established coronary artery disease (CAD).2,3
Large cross-sectional studies have shown an inverse relationship between physical activity and inflammation, 4 – 6 as illustrated by an inverse correlation between physical activity and standard inflammatory markers such as CRP, fibrinogen, and soluble intercellular adhesion molecule-1. 4 However, while there are several cross-sectional studies on the interaction between training and inflammation in relation to cardiovascular disease, there are fewer data from randomized trials, in particular in patients who have been revascularized with percutaneous coronary intervention (PCI).
We have recently shown that regular high-intensity interval training over 6 months is associated with a significant reduction of instent restenosis and a reduction in CRP. 7 However, CRP is a down-stream marker of inflammation and will not give information of the involved upstream mediators. Also, it is unlikely that this parameter will reflect all inflammatory pathways that are involved in atherogenesis. To further elucidate the effect of training on inflammation, we analysed concentrations of a wide range of inflammatory markers before and after the training period.
Materials and methods
Patients
Forty patients with angina pectoris, referred for planned coronary angiography at the Department of Cardiology, Stavanger University Hospital, were included after successful PCI in one or more native coronary arteries. Successful PCI was defined as a residual diameter stenosis of less than 20% of the reference diameter and no incidence of major cardiac events during hospitalization. Exclusion criteria included a history of myocardial infarction (MI) or coronary artery bypass grafting, age over 80 years, inability to give informed consent, any known chronic inflammatory disease other than atherosclerosis, ongoing clinical infection, inability to participate in regular training due to residency, work situation, or co-morbidity or planned surgery within the next 6 months. All patients were treated with dual platelet inhibition with acetylsalicylic acid and clopidogrel in addition to statins during the study period according to current guidelines. The local ethics committee approved the protocol and all patients gave written informed consent.
Exercise training
The patients were randomized to a high-intensity interval training programme for 6 months or to usual care. The training programme and the effect of the programme on in stent re-stenosis have been previously described. 7 Briefly, the patients trained in groups of 10, starting 11 ± 4 days after PCI, three times a week, 60 minutes per session, for 6 months. The programme consisted of a warm-up period, followed by four 4-minute intervals at 80–90% of maximal heart rate, when patients were riding an ergometric bicycle or were running. Intervals were interrupted by 3 minutes of active recovery at 60–70% of maximal heart rate. Afterwards, there were 5 minutes cool-down, 10 minutes abdominal- and spine-resistance exercises, and 5 minutes of stretching and relaxing. The training sessions were monitored with individual pulse watches allowing the patient to achieve the target heart rate.
Blood sampling protocol
Blood samples were collected by standard venipuncture from the left median cubital vein immediately before cardiac catheterization (baseline) and 6 months after inclusion. Sterile tubes with ethylenediaminetetraacetic acid as anticoagulant were immediately placed on melting ice, and plasma was separated within 30 minutes by centrifugation at 4°C and 1800 g for 15 minutes to obtain platelet-poor plasma. Samples were stored at −80°C until analysis.
Biochemical measurements
Plasma concentrations of interleukin- (IL)-6, Pentraxin 3 (PTX3), tumor necrosis factor (TNF)α, vascular cell adhesion molecule (VCAM)-1, E-selectin, P-selectin, monocyte chemoattractant protein (MCP)-1/CCL2, regulated on activation, normal T-cell expressed and secreted (RANTES/CCL5), CCL19, CCL21, IL-8/CXCL8, and CXCL16 were quantified by enzyme immunoassays (EIA) obtained from R&D Systems (Minneapolis, MN). Plasma concentrations of von Willebrand factor (vWF) were analysed by EIA using antibodies from DakoCytomation (Glostrup, Denmark) as previously described. 8 Plasma concentrations of CD40 ligand (CD40L) were analysed by EIA provided by Bender MedSystems (Vienna, Austria). The intra- and inter-assay coefficients of variation were <10% for all assays. All samples were analysed in duplicates.
Quantitative coronary angiography
Standard image acquisition was performed using at least two angiographic projections of the stenosis. Intracoronary nitroglycerin was administered to provide maximum coronary vasodilation. At follow-up, repetition of identical angiographic projections of the lesion was performed. With the contrast-filled injection catheter as the calibration source, quantitative angiographic analysis was performed by use of a validated computer-assisted edge-detection algorithm (Camtronics Medical Systems, Hartland, WI). Lesion length was defined as the axial extent of the lesion that contained a shoulder-to-shoulder lumen reduction by 20%. Selected images for analysis were identified by use of angiographic projections that demonstrated the stenosis in an unforeshortened view, minimized the degree of vessel overlap, and displayed the stenosis in its ‘sharpest and tightest’ view. A 5-mm segment of reference diameter proximal and distal to the stenosis was used to calculate the average reference vessel diameter at baseline, after stent implantation, and at follow-up. The target lesion was defined as the stented segment plus a 5-mm segment proximal and distal to the stent. Angiographic follow-up was performed at 6 months after the index procedure unless earlier angiography was required due to clinical reasons. Binary angiographic restenosis was defined as the incidence of diameter stenosis of 50% at the qualifying angiographic follow-up. Late luminal loss was defined as the minimal lumen diameter immediately after the procedure minus the minimal lumen diameter at 6-month follow-up. Two experienced cardiologists independently interpreted the images in a blinded manner. Disagreement was resolved by reanalysis and consensus. The intraobserver variability of absolute vessel dimensions for 20 randomly selected measurements was 0.09 mm. The interobserver variability of absolute vessel dimensions was 0.11 mm.
Statistical analysis
All data were statistically analysed by SPSS 15.0 (SPSS, Chicago, Illinois) by a medical expert statistician. Data are expressed as mean ± standard deviation (SD) unless otherwise stated. The Kolmogorov-Smirnov test in combination with visual inspection of ‘normal QQ plots’ was used to evaluate normal distribution of data. Comparisons between groups were performed using t-tests, Mann-Whitney U-tests, or chi-squared tests as appropriate. A linear mixed-effect model (R-statistics with package for linear mixed-effects models [R version 2.9.1,2009]) was used to analyse the changes in plasma levels of inflammatory mediators as the dependent variables, with random intercepts and slopes as a function of time and fixed effects for intervention, stent type, access site, sex, and diabetes. Spearman correlation was used to calculate correlation coefficients. All tests were two-tailed and a p-value below the 0.05 level was considered significant.
Results
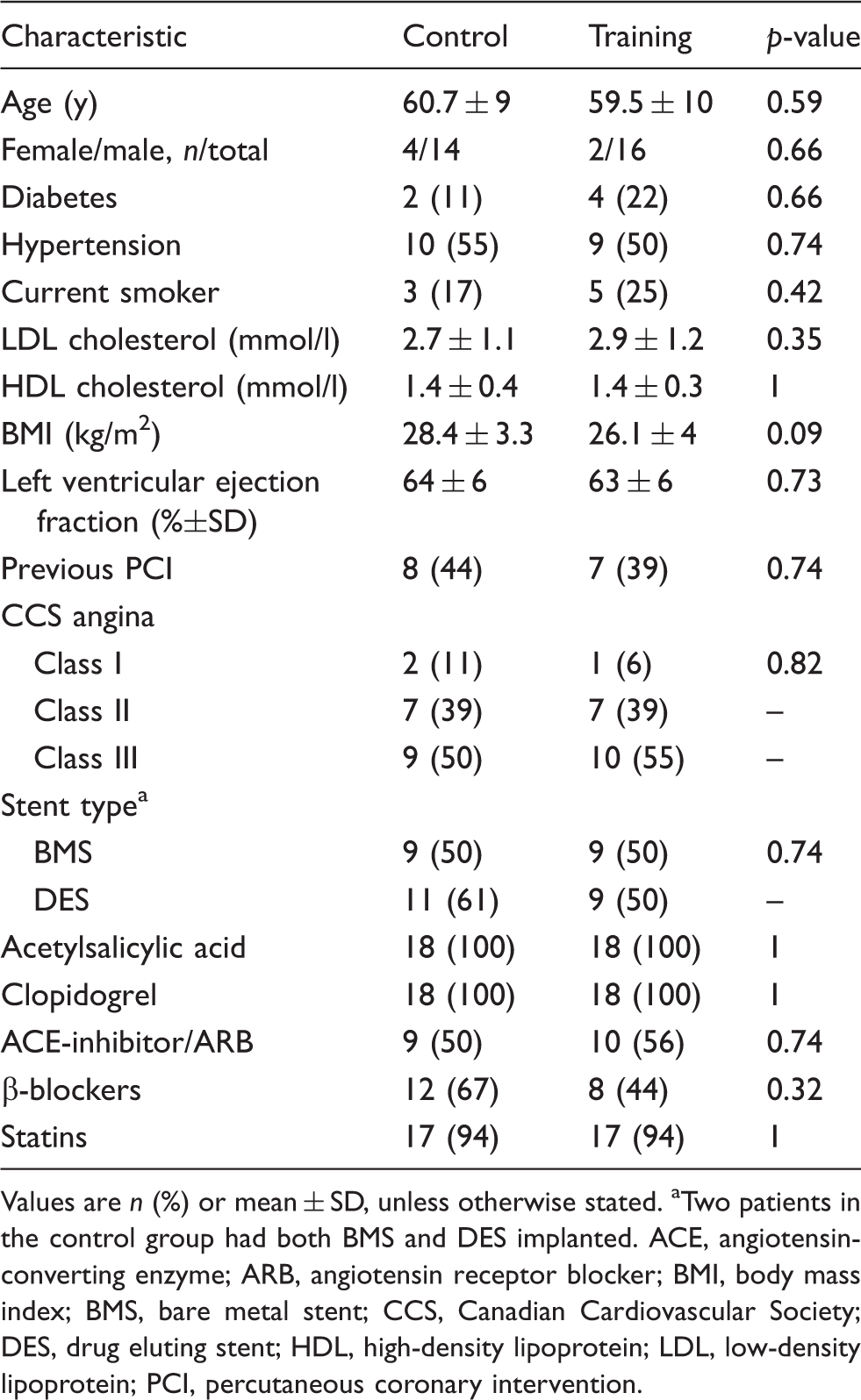
Forty patients with angina pectoris were prospectively enrolled and randomized to training or to a control group. No patients withdrew consent or were lost to follow-up. Four patients with unstable angina were excluded from analysis (Figure 1). Patients in the two groups did not differ significantly in risk profile, clinical presentation, medical treatment, or angiographic or procedural characteristics at baseline (Table 1). Medication did not change during the study period, except for one patient in the control group, in whom the metoprolol dose was increased from 50 to 100 mg. All patients except for one attended more than 90% of the training sessions. There were no serious events during the training sessions requiring hospitalization.
Enrolment, randomization, and treatment. CABG, coronary artery bypass graft; MI, myocardial infarction. Baseline population characteristics and medication Values are n (%) or mean ± SD, unless otherwise stated. Two patients in the control group had both BMS and DES implanted. ACE, angiotensin-converting enzyme; ARB, angiotensin receptor blocker; BMI, body mass index; BMS, bare metal stent; CCS, Canadian Cardiovascular Society; DES, drug eluting stent; HDL, high-density lipoprotein; LDL, low-density lipoprotein; PCI, percutaneous coronary intervention.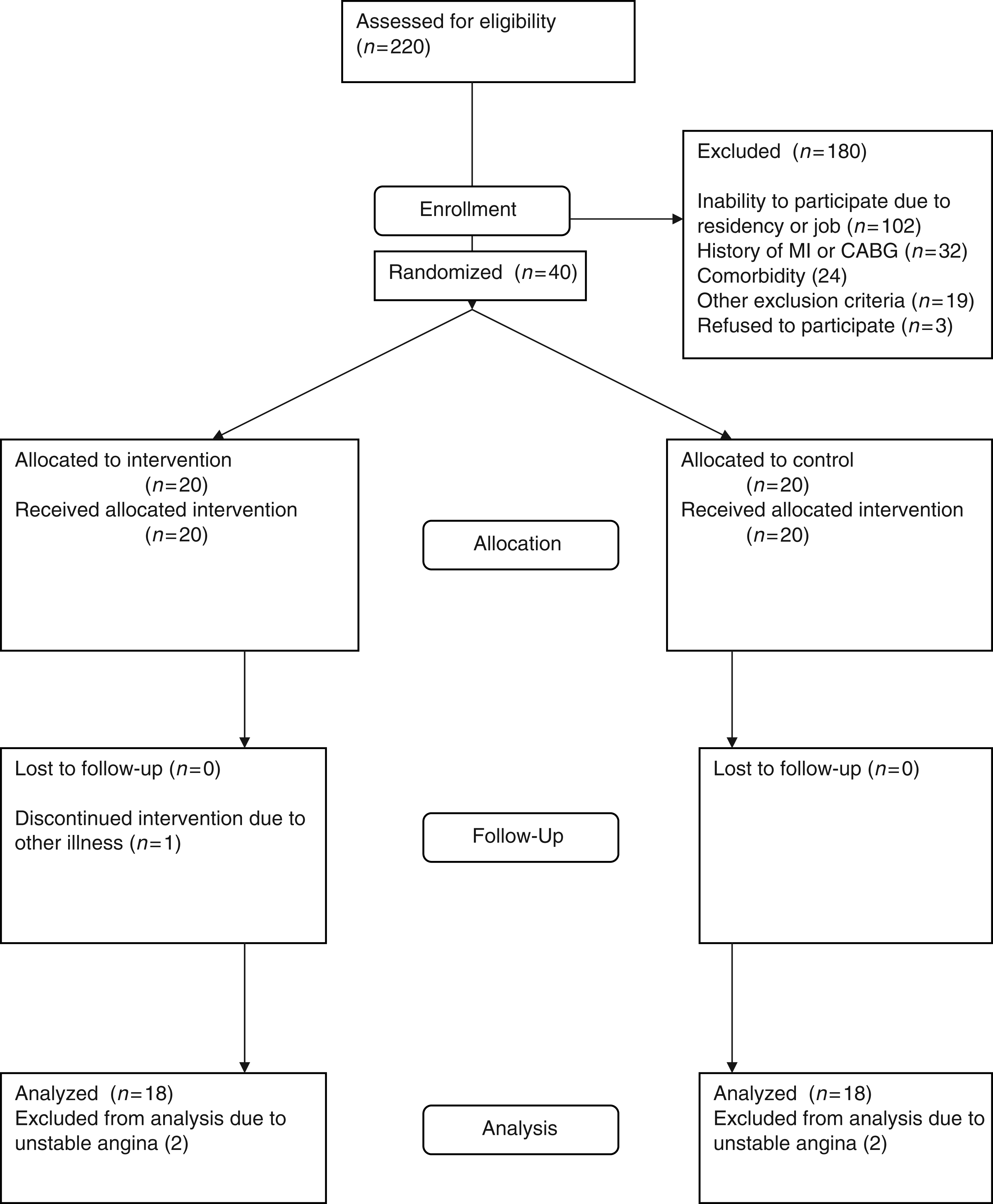
The body weight in the control group increased by 1.2 ± 3.3 kg, while it decreased in the training group by 1.7 ± 1.7 kg (p = 0.002 for group difference).
Plasma levels of inflammatory and anti-inflammatory markers
Plasma levels of inflammatory markers and chemokines
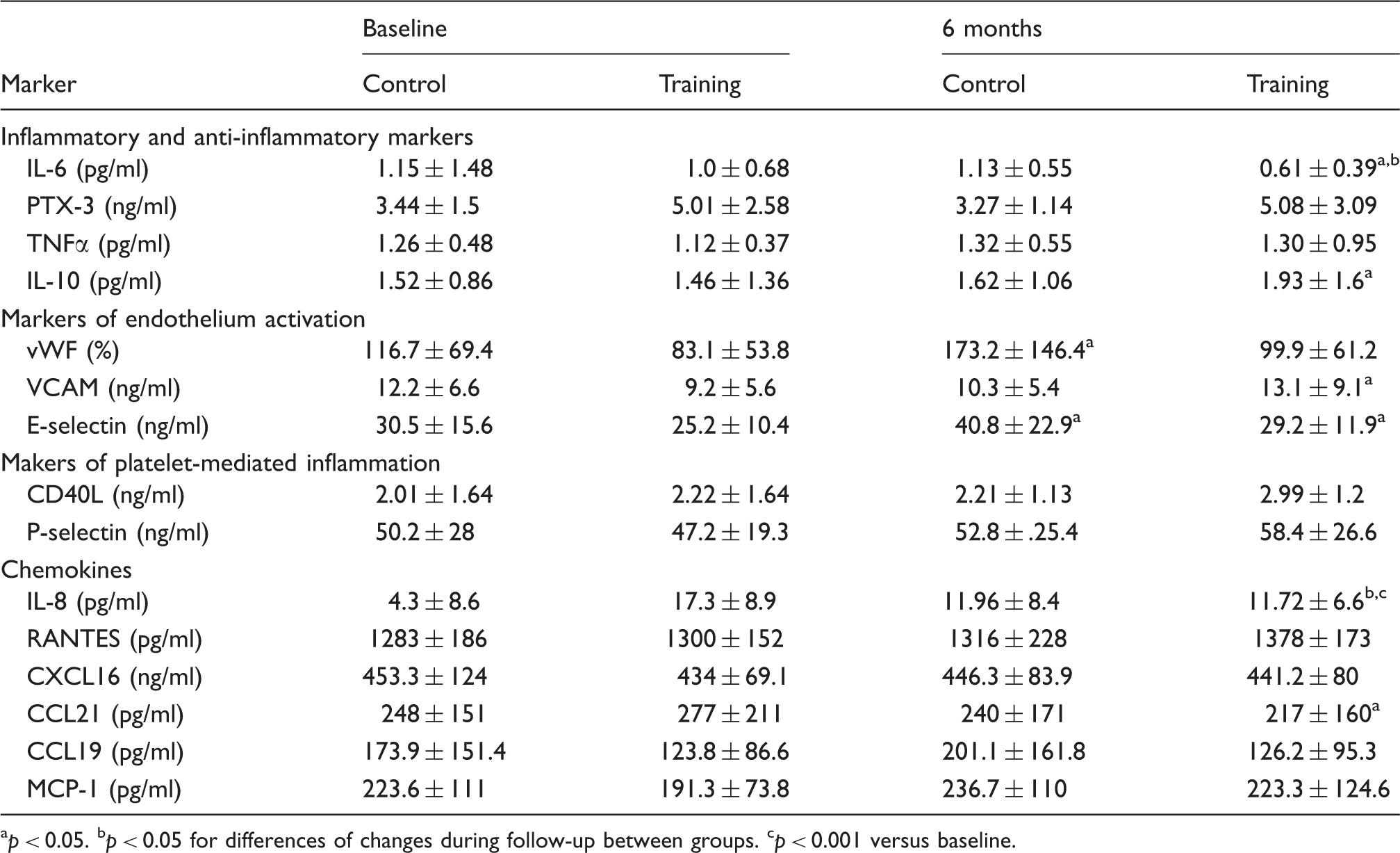
p < 0.05.
p < 0.05 for differences of changes during follow-up between groups.
p < 0.001 versus baseline.
Plasma levels of markers of endothelial cell activation
During the study period, there was a significant increase in plasma levels of vWF in the control group, but not in the training group (Table 2). In contrast, E-selectin levels were significantly increased at 6 months in both the study groups, and VCAM-1 levels showed a modest, but significant increase in the training group, but not in the control group (Table 2).
Plasma levels of markers of platelet-mediated inflammation
At 6 months, CD40L levels were not different from baseline in neither group (Table 2). As for P-selectin, there was a non-significant increase after 6 months, with no difference between the two study groups (Table 2).
Plasma levels of chemokines
During follow-up, there was a significant decrease in plasma levels of IL-8 in the training group, but not in the control group, resulting in a significant difference in changes between the two study groups (p = 0.026; Table 2). Also, during the study period there was a significant reduction of CCL21 levels in the training group only (Table 2). In contrast, plasma levels of RANTES, CXCL16, CCL19, and MCP-1 did not change significantly during follow-up in neither group (Table 2).
Inflammation and restenosis
As previously reported, the exercise training programme was associated with a significant reduction of late luminal loss at 6 months in a population of 40 patients with stable and unstable angina.
7
The effect of the training programme on the late luminal loss was still significant in the 36 patients with stable angina who were included in the present analysis (0.49 ± 0.34 mm versus 0.24 ± 0.4 mm; p = 0.04), and notably, this decrease in luminal loss was significantly correlated with the decrease in IL-6 (Figure 2) and CRP (R = 0.42, p = 0.018). Finally, a multivariable analysis showed no differences in levels of biomarkers between bare metal stent and drug eluting stent with the exception of RANTES that was significantly decreased in the latter group during follow-up (p < 0.001).
Correlation between changes in plasma levels of interleukin (IL)-6 and late luminal loss at 6 months. Linear regression with 95% individual prediction interval.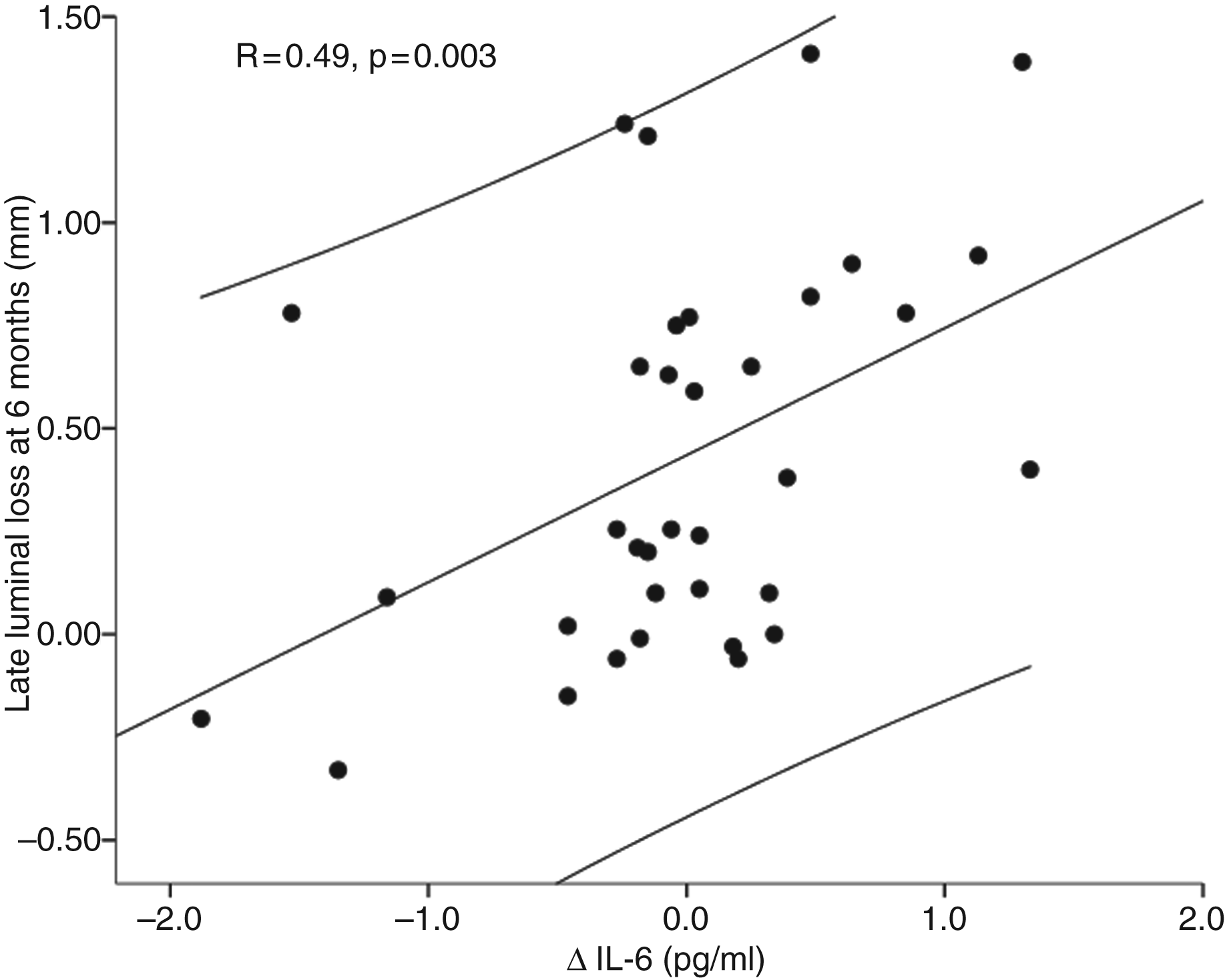
Discussion
In the present study, in patients with stable angina, randomized to aerobic interval training or a control group for 6 months following PCI, we found that the training group, but not the control group, showed a significant decrease in plasma levels of the inflammatory mediators IL-6, IL-8, and CCL21 as well as an increase in plasma levels of the anti-inflammatory cytokine IL-10, and as for IL-6 and IL-8, the difference in changes between the two study groups reached statistical significance. Also, the decrease in IL-6 and CRP levels was significantly correlated with a significant reduction of late luminal loss following PCI, which may suggest a possible link between the effect of aerobic interval training on restenosis following PCI and the anti-inflammatory net effects of such physical activity.
Previous studies examining the effect of exercise training on markers of inflammation in different populations with cardiovascular risk factors have been diverging, and several of these studies were not randomized. 9 – 18 In a study comparing PCI with exercise training, regular physical exercise training was associated with a significant reduction of both inflammatory markers and ischemic events. 19 In addition, Peschel et al. 20 found that high-frequency exercise training reduced the expression of adhesion molecules on monocytes in stable CAD patients, while a less intensive home-based programme did not, indicating that the intensity of the training programme matters with regard to the anti-inflammatory effect. However, although training and PCI have been compared, no previous randomized studies have prospectively examined the effect of exercise training on inflammation in CAD patients following PCI. Here, we show a significant difference in changes in plasma levels of the prototypical inflammatory cytokines IL-6 and IL-8 between the training and the control group, with a significant decrease in these cytokines during exercise training, accompanied by an increase in the anti-inflammatory cytokine IL-10. Our findings further support an anti-inflammatory potential of exercise training in CAD patients, including the follow-up period after PCI.
The decrease in IL-8 levels, being a pro-atherogenic chemokine, may be of interest, and notably, the regulation of IL-8 seems to be closely related to oxidative stress and hypoxia, that could have been attenuated by training. We have previously shown a decrease in CRP in this study population and the decrease in IL-6 levels in the training group, further support that aerobic interval training could attenuate the inflammatory IL-6-CRP pathway. Plasma levels of IL-6 are strongly associated with future cardiac events and mortality in patients with stable CAD, 21 and peri-procedural plasma CRP and IL-6-levels have been associated with the risk of restenosis.22,23 IL-6 has been shown to promote vascular smooth muscle cell proliferation, and our findings in the present study, showing a strong correlation between the decrease in plasma levels of IL-6 and the reduction of late luminal loss in the training group following PCI, may further relate IL-6 to the restenosis process, a process that seems to be attenuated by exercise training.
While most studies on the effects of exercise training on inflammation in CAD patients have been focused on a few central mediators, the present randomized trial examined a wide range of inflammatory mediators. Thus, while training had attenuating effects on some central inflammatory markers (i.e., IL-6 and IL-8), aerobic interval training had no effect of markers of platelet-mediated inflammation. Moreover, whereas training decreased IL-8 and CCL21 levels, plasma concentration of most of the chemokines that were examined (i.e., RANTES, MCP-1, CXCL16, CCL19) did not change during the training period. Finally, whereas exercise training has been shown to improve endothelial function in CAD patients, our findings in the current study may suggest a more complex effect of training on endothelial cells, inducing both attenuating (i.e. decreased vWF levels) and enhancing (i.e., increased VCAM-1 and E-selectin levels) effects on markers of endothelial cell activation.
There was a small, but significant reduction of body weight in the training group only. Large weight loss has been shown to be associated with a reduction of inflammatory markers in obese individuals. 24 As visceral fat is a key regulator site for inflammation, the weight loss might have contributed to the reduction of inflammatory markers.
Strengths of the present study include its randomized, prospective design and the carefully selected patients trying to minimize the influence of confounders such as accompanying inflammatory disease and heart failure. Nearly all patients were on optimal standard cardiovascular medications such as statins. However, the study also has some limitations such as a relative small sample size. A further limitation is the heterogeneity of stents implanted, which might have influenced the inflammatory response after PCI. The effect of inflammation on restenosis was not the primary end-point of this sub-study, and these data must be interpreted with some caution. Moreover, correlation does not necessarily mean any causal relationship. The present study was performed in stable CAD patients following PCI, and this situation may not necessarily be extrapolated to the general CAD population.
The current randomized study in stable CAD patients, nearly all on statin therapy, showed that 6 months high-intensity exercise programme after successful PCI in CAD patients, had beneficial effects on the inflammatory profile, and that this modulation may be operative for the training-induced reduction of in-stent restenosis. However, several inflammatory pathways seemed not to be modified, underscoring the need for additional anti-inflammatory intervention in these patients.
ClinicalTrials.gov Identifier
NCT00469950
Footnotes
Funding
The study was supported by the Norwegian Health Association (grant number 6562) and Stavanger University Hospital (grant number 500516).
Conflict of interest
None.