
Abstract
Introduction
The metabolic syndrome (MS) is a term applied to identify an ever increasing number of individuals presenting with an array of diverse adverse cardiovascular system-related characteristics with insulin resistance being the common denominator. 1 It is overexpressed in hypertensive patients, in whom it imposes an extra burden on target organs and augments cardiovascular risk. 1
An exaggerated blood pressure response to exercise (EBPR), though variably defined as well as influenced by factors such as age, sex and habitual physical activity, provides important information on the cardiovascular risk profile of patients undergoing cardiac stress testing.2,3 Healthy asymptomatic individuals with an EBPR are at increased risk for MI and total cardiovascular events.2,3 EBPR confers a higher risk for development of hypertension in both normotensive subjects and those with high-normal blood pressure (BP).2,4,5 In the setting of essential hypertension, EBPR has been associated with a larger left ventricular mass and impaired diastolic function 6 as well as increased arterial stiffness and albuminuria.7,8
Possible constituents of the pathophysiologic background of the EBPR include a raised sympathetic activity, endothelial dysfunction and an exercise-associated rise in angiotensin II. 9 – 11 EBPR has been reported in patients with type 1 and type 2 diabetes mellitus while impaired glucose metabolism has been observed in normotensive non-diabetic individuals with EBPR. 12 Based on the above, the aim of the present study was to assess the impact of the metabolic syndrome on the BP response to exercise in recently diagnosed hypertensive patients.
Methods
Study population and design
Our study population consisted of 325 non-diabetic consecutive patients, aged between 29 and 75 years old, with newly diagnosed never treated stage I-II essential hypertension who were referred to the outpatient hypertensive unit and were eligible for treadmill exercise testing. Exclusion criteria included secondary hypertension, familial dyslipidemia, history of atherosclerotic cardiovascular disease, severe valvulopathy, any other clinically significant systematic illness, as well as orthopedic problems that would preclude maximal effort on the treadmill. Subjects with bundle branch block, preexcitation syndromes, pacing rhythm, atrial fibrillation, signs of left ventricular hypertrophy or ischemic heart disease in resting electrocardiogram, as well as an exercise test positive for ischemia, were also excluded. None of the participants had received any non-pharmacologic or pharmacologic treatment including lipid-lowering or allopurinol therapy for one month prior to the entry in the study.
The study protocol included ambulatory blood pressure monitoring, echocardiography, routine blood testing and anthropometric measurements, as well as treadmill exercise stress testing. Diagnosis of hypertension was based on three outpatient measurements of office blood pressure ≥140/90 mmHg and confirmed by daytime ambulatory blood pressure values ≥135/85 mmHg. All subjects underwent the usual clinical and laboratory work-up in order to rule out secondary forms of hypertension. 13 MS was defined based on the Adult Treatment Panel III (ATP III) criteria. 14 The study protocol complies with the Declaration of Helsinki and was approved by our institutional ethics committee while all participants gave written informed consent.
Office and ambulatory blood pressure
Office blood pressure values were acquired in our outpatient clinic by one physician, with the use of a mercury sphygmomanometer, on three separate visits one week apart. Three measurements were performed with the patient in the sitting position after a five-minute rest according to running guidelines. 13 Ambulatory blood pressure monitoring was performed over a working day (Monday to Friday) using the automatic Spacelabs units 90207 (Redmond, WA, USA), as previously described. 8 Twenty-four-hour systolic and diastolic blood pressure values were the mean of the overall 24-hour recordings after the artifact editing.
Cardiac echocardiography
Standard transthoracic echocardiographic examination was carried out by the same expert, who was blind to the clinical status of the examined subject, in a dimly light room using a Vivid 3 PRO ultrasound imager (General Electric, Milwaukee, Wisconsin, USA) equipped with a 2.5 to 5 MHz (harmonics) phased-array transducer, according to current guidelines. 15 Left ventricular mass was calculated with the method of Devereux et al. and normalized for body surface area (BSA) and height2–7 to obtain LV mass index. 15
Exercise treadmill stress test
Study participants underwent symptom-limited exercise testing according to the multistage Bruce protocol on a Quinton 5000 treadmill system (Quinton Instruments, Seattle, WA, USA). Peak exercise time was recorded in minutes. Maximal exercise tolerance was estimated as metabolic equivalents (METs). Exercise capacity (in METs) was estimated based on exercise time via a commonly used equation for the Bruce protocol and based on the American College of Sports Medicine equations for the ramp protocol. 16 Twelve-lead electrocardiogarm was obtained throughout the test. Resting systolic BP and diastolic BP were the average of three measurements taken in a seated position by a well-trained physician, after the subjects had been resting for at least five minutes. Exercise BP values were measured using a mercury column sphygmomanometer during the last minute of each three-minute stage and at the moment of maximum effort, with the arm relaxed at the side without holding on to the side bar of the treadmill according to guidelines. As needed, the subjects rested their hand on the examiner’s shoulder to minimize movement artifact. The highest systolic BP value achieved during the exercise test was the peak exercise systolic BP and accordingly an exaggerated blood pressure response was defined as a peak exercise systolic BP ≥210 mmHg in men and ≥190 mmHg in women, in line with the Framingham criteria. 6 – 8
In the absence of any symptoms, the exercise test was terminated if the subject achieved more than 90% of the predicted maximal heart rate, had an increase in systolic BP greater than 250 mmHg, or had a decrease in systolic BP ≥10 mmHg, an inability to exercise further because of fatigue or at the occurrence of ischemic ST-segment response. Subjects were encouraged to exercise until volitional fatigue in the absence of symptoms or indicators of ischemia. The use of handrails during the exercise test was discouraged.
Statistical analysis
SPSS statistical package, version 12.0 (SPSS Inc., Chicago, Illinois, USA) was used for all statistical analysis. Continuous variables were expressed as arithmetic means ± SD. Significant differences between the groups of hypertensive subjects with and without MS were assessed with the independent-sample Student’s t-test for continuous variables and the Chi-square test for categorical variables. Analysis of covariance was performed to detect differences in EBPR and METs between the groups after adjusting for covariates. Pearson’s correlation coefficient was used to examine univariate relations of clinical, echocardiographic and exercise test-related variables. Multivariate linear regression analysis was conducted to identify independent associates of peak exercise systolic BP and METs. Logistic regression was performed to check for independent predictors of EBPR. All statistical assumptions were met and all tests were considered to be significant at the level of p < 0.05.
Results
Demographic, clinical, laboratory, echocardiographic and exercise characteristics in hypertensive patients with and without the metabolic syndrome
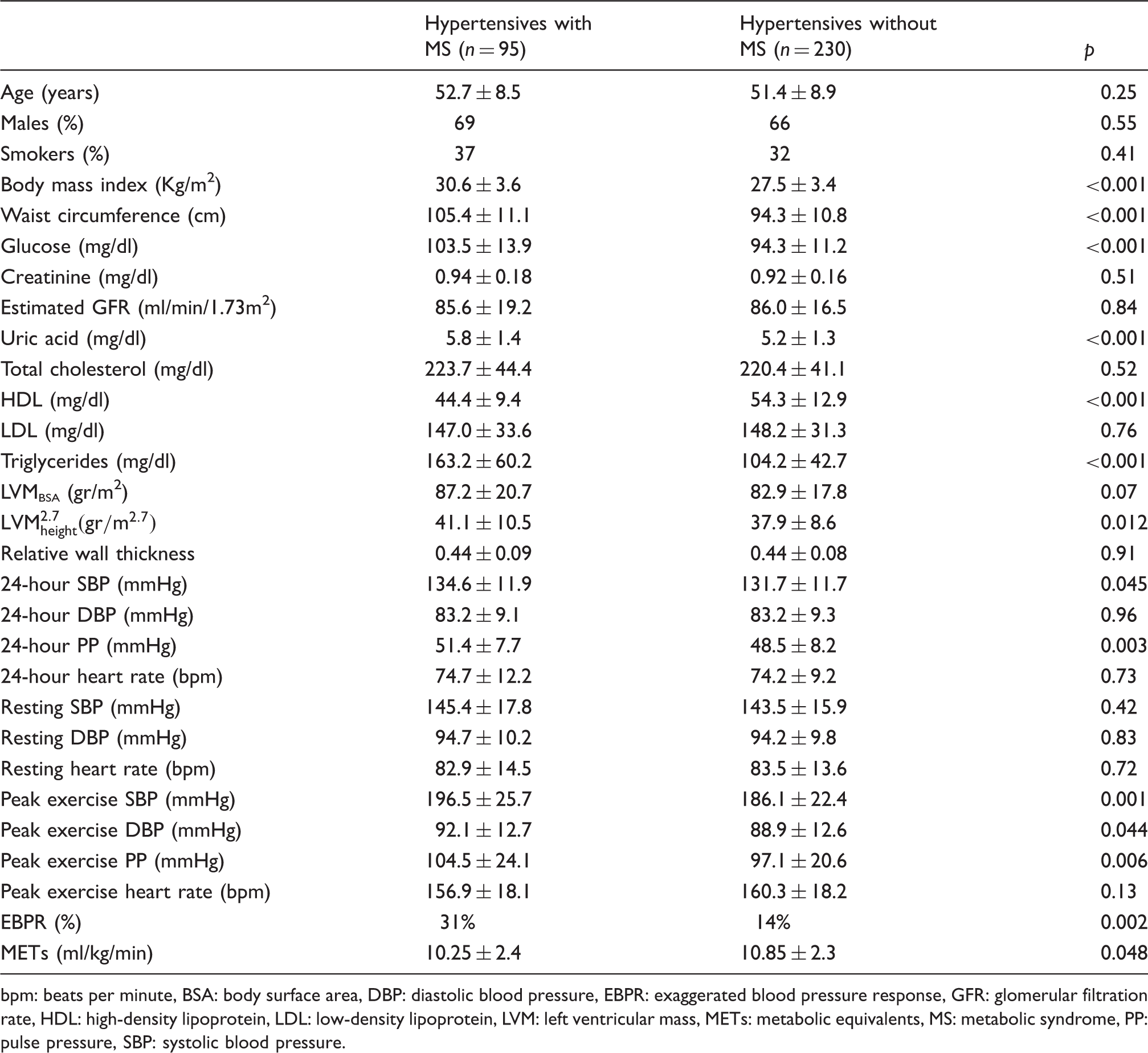
bpm: beats per minute, BSA: body surface area, DBP: diastolic blood pressure, EBPR: exaggerated blood pressure response, GFR: glomerular filtration rate, HDL: high-density lipoprotein, LDL: low-density lipoprotein, LVM: left ventricular mass, METs: metabolic equivalents, MS: metabolic syndrome, PP: pulse pressure, SBP: systolic blood pressure.
Peak exercise systolic BP and the prevalence of EBPR were significantly higher in hypertensive patients with MS (196.5 mmHg vs. 186.1 mmHg, p = 0.001 and 31% vs. 14%, p = 0.002 respectively) compared to those without MS. The significant difference in peak exercise systolic BP was preserved even after adjusting for age, gender, BMI and 24-hour systolic BP. No difference was observed in the prevalence of EBPR between MS patients with impaired fasting glucose and those without impaired fasting glucose (25.7 vs. 33.3, p = 0.49). Additionally, an observed difference in METs in the MS group (by 0.6 ml/kg/min, p = 0.048) lost significance after adjusting for the above covariates.
In the entire population, significant positive correlates of peak exercise systolic BP were age (r = 0.14, p = 0.013), male gender (r = 0.14, p = 0.012), waist (r = 0.16, p = 0.005), 24-hour systolic BP (r = 0.25, p < 0.001), 24-hour diastolic BP (r = 0.12, p = 0.028) and 24-hour pulse pressure (r = 0.22, p < 0.001), plasma triglycerides (r = 0.16, p = 0.003), and uric acid (r = 0.14, p = 0.01). METs were positively correlated with male gender (r = 0.35, p < 0,001) and smoking (r = 0.14, p = 0.025) and inversely correlated with age (r = −0.39, p < 0.001), BMI (r = −0.27, p < 0.001) and waist (r = −0.13, p = 0.01). In a model of multiple regression analysis with age, gender, BMI, waist, 24-hour systolic and diastolic BP and presence of MS as independent variables, peak exercise systolic BP was independently predicted by age (β = 0.13, p = 0.02), male gender (β = 0.13, p = 0.04), 24-hour systolic BP (β = 0.23, p = 0.007) and presence of MS (β = 0.16, p = 0.008). Likewise, in linear regression analysis that included age, gender, BMI, waist, smoking status, 24-hour systolic and diastolic BP and presence of MS as independent variables, independent predictors of METs were BMI (β = −0.19, p = 0.02) along with age (β =−0.31, p < 0.001) and male gender (β = 0.34, p < 0.001) but not MS (β = 0.02, p = 0.77).
Multiple logistic regression analysis with an exaggerated BP response to exercise (EBPR) as the dependent variable in the total population
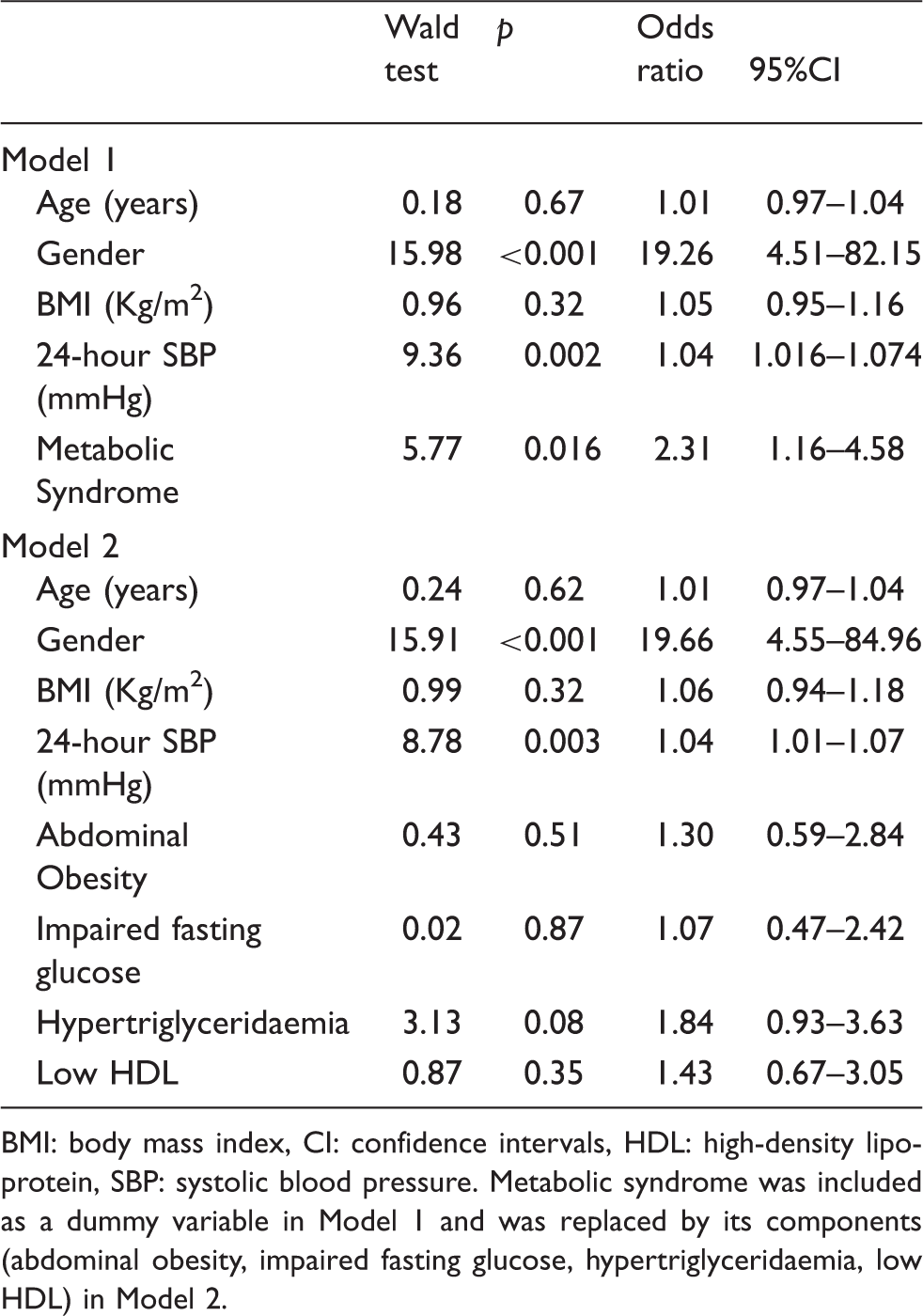
BMI: body mass index, CI: confidence intervals, HDL: high-density lipoprotein, SBP: systolic blood pressure. Metabolic syndrome was included as a dummy variable in Model 1 and was replaced by its components (abdominal obesity, impaired fasting glucose, hypertriglyceridaemia, low HDL) in Model 2.
Discussion
The novel finding in our study is that never-treated hypertensive patients with MS exhibit higher values of peak systolic BP during exercise compared to hypertensive-only controls. Most importantly, in such a population, presence of MS predicts EBPR independently of ambulatory BP levels and anthropometric characteristics. Moreover patients with MS have BMI-related impairment of exercise capacity compared to their hypertensive counterparts. These findings provide evidence of a further magnified adverse cardiovascular status of individuals presenting with the couplet of hypertension and the cardiometabolic disorder.
The MS has been associated with increased prevalence of target organ damage such as left ventricular hypertrophy, microalbuminuria and carotid atherosclerosis as well as higher cardiovascular mortality and morbidity in hypertensive subjects.1,17 To the best of our knowledge this is the first study to identify a relation of the presence of MS in a hypertensive population to EBPR status. Fasting blood glucose has been reported to have a strong positive association with maximal exercise BP in apparently healthy men independently from physical activity. 18 In healthy normotensive, non-diabetic individuals, the systolic BP response to exercise is significantly correlated with HbA1c levels. 19 In a recent study on subjects with normal BP, diverse indexes of impaired glucose metabolism were shown to be independent determinants of an EBPR. 12 Further down the dysmetabolic continuum, in patients with type 2 diabetes mellitus, systolic BP response to exercise is correlated to insulin resistance measures. 20
From a pathophysiologic point of view, essential alterations accompanying MS (i.e. reciprocal activation of the sympathetic and the renin-angiotensin-aldosterone system) may predispose to EBPR. Indeed, increases in plasma norepinephrine during exercise have been associated with EBPR, although in one study sympathetic stimulation of patients with MS and hypertension was not followed by a significantly higher response of BP.9,21 Furthermore, higher levels of resting angiotensin II as well as an augmented rise during exercise in patients with EBPR have been reported. 11 Functional abnormality of the endothelium is interwined with the insulin resistant state. 22 In turn, impaired endothelium-dependent vasodilation and raised levels of ADMA have been identified in patients with EBPR implicating a poor vascular relaxation during exercise hyperemia.10,23 Moreover, MS is associated with impaired aortic elastic properties, 1 a finding that has also been attributed to patients with an EBPR.7,8
In contrast to exercise haemodynamic parameters, impaired exercise capacity in our hypertensive patients with MS compared to those without is attributed to a higher BMI. A dose-dependent association of MS components with exercise capacity measured by peak maximum oxygen uptake has been observed in a high risk population and not solely hypertensive, yet adjustment for BMI was not performed. 24 Nevertheless, our results underline an at least indirect deleterious effect of the MS on exercise capacity, a strong predictor of all-cause mortality.
In the clinical setting, there has been a raging debate regarding the MS and its true predictive significance for cardiovascular disease as a sole entity. Our study identifies MS as a determinant of EBPR in hypertensive subjects while its individual components failed to predict EBPR. This is in line with the concept that MS exerts its deleterious action over and above that of its single ingredients. 1 Taken into consideration that EBPR reflects pronounced hypertensive sequelae and adverse cardiovascular prognosis one may suggest that identification of hypertensives (even grade 1) with MS and EBPR confines a patient group at higher risk for developing target organ damage and at higher cardiovascular risk requiring prompter initiation of antihypertensive treatment. Additionally, our results extend the importance of a graded regular physical activity in the frame of lifestyle modifications for patients with MS and hypertension to incorporate potential beneficial effects on the abnormal increase in exercise BP as well; Although, no data are available regarding the impact of different ways of physical exercise in patients according to EBPR status, there is evidence that aerobic exercise may attenuate the BP response to exertion possibly by restricting the accompanying sympathetic neural response.25,26
Specific limitations of the present study should be considered. The study is a cross-sectional one conducted in newly diagnosed patients with essential hypertension, therefore neither can it imply direct causation of the presence of the MS for an abnormal BP response to exercise nor its findings are applicable to other patients groups from a primary, as well as secondary, cardiovascular point of view. In addition, we did not measure markers of possible pathophysiologic intermediates such as sympathetic and renin-angiotensin-aldosterone system activity, as well as neither oral glucose tolerance test nor measurements of plasma insulin levels were performed in order to identify and investigate patients with impaired glucose tolerance. Furthermore, habitual physical activity of the subjects was not assessed as it has been shown to affect exercise test measures. However, the study population was specifically selected to include never treated hypertensives without left ventricular hypertrophy, thus avoiding a confounding of EBPR and its associations. Finally, MS was defined according to NCEP-ATP III criteria allowing easier comparisons with the majority of studies, while its prevalence appears to be relatively low since patients with arterial hypertension often possess other cardiovascular risk factors. 26
In conclusion, middle-aged newly-diagnosed hypertensive patients with MS exhibit increased peak systolic BP during exercise as well as a higher risk for EBPR compared to hypertensive only individuals. The adverse prognosis of the couplet of hypertension and MS may be further augmented through the abnormal exercise BP response beyond the effects of resting BP and the separate MS components.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of interest
None.