
Abstract
Introduction
Major cardiovascular events such as myocardial infarction or stroke are important causes of morbidity in the elderly and cardiovascular disease (CVD) is still death cause number one in high- and middle-income countries.1–3 The incidence of CVD rises sharply with age, as well as the prevalence of cardiovascular risk factors including hypertension, obesity, physical inactivity, and diabetes mellitus type II (DM). Research on cardiovascular interventions in subjects over 70 years of age is relatively scarce. However, several recent randomized controlled trials (RCTs) on antihypertensive and cholesterol-lowering treatment showed beneficial effects on major cardiovascular events (especially stroke) in elderly up to 85 years, mainly in secondary prevention populations.4–6 Also, there is some evidence that antihypertensive treatment may lead to postponement or prevention of incident dementia.7,8
Nevertheless, there is still a lack of consensus on optimal target levels for blood pressure and lipids for patients aged 70 and older. 3 In most guidelines, recommendations apply to populations up to 65 or 70 years of age only, especially when considering primary prevention. Fear of adverse effects (e.g. falls caused by hypotension) and/or doubt on the net benefit of medication in later life may explain the reserved attitude towards treatment by clinicians and/or patients. 9
With a growing population of elderly there is an urgent need for evidence-based cardiovascular risk management in people over 70 years of age, aimed at reduction of morbidity and disability. 1 To illustrate the window of opportunity for primary as well as secondary prevention, we here present the prevalence of hypertension among other cardiovascular risk factors in a relatively unselected sample of Dutch community-dwelling men and women aged 70–78. In addition, we calculate the potential benefit of blood pressure-lowering treatment on the prevention of coronary heart disease (CHD) and stroke in this population.
Methods
Subjects
All subjects participating in the preDIVA study (Prevention of Dementia by Intensive Vascular care) were included in this analysis. This cluster-randomized, open-label, controlled trial is designed to assess the effects of nurse-led intensive vascular care on the prevention or postponement of dementia and disability in primary care practices. 10 Secondary outcomes are all-cause mortality, major vascular events (including myocardial infarction, stroke, and peripheral arterial disease), and overall changes in cognitive functioning and mood.
The background, methods, and projected follow-up of the preDIVA trial have been described in detail elsewhere. 10 In short, all subjects in participating primary healthcare centres aged 70–78 years, without dementia, and able to visit their primary care practice were eligible for this study. Patients with a condition likely to hinder successful long-term follow up (e.g. terminal illness, alcoholism) were excluded by their general practitioner (GP).
After inclusion and baseline assessment, practices were randomized to intensive vascular care or to standard care. Intensive vascular care comprises 4-monthly visits to a practice nurse aimed at minimizing cardiovascular risk. Follow-up measurements in the two groups are at 2, 4, and 6 years.
Measurements and assessment of cardiovascular risk
Cross-sectional data of the preDIVA trial were used to study the prevalence of risk factors in community-dwelling elderly subjects with or without a history of CVD. A positive history of CVD is defined as at least one of the following: myocardial infarction, angina pectoris, peripheral arterial disease, stroke or transient ischaemic attack (TIA). At baseline, practice nurses with direct access to medical records assessed the medical history together with participants.
Demographic characteristics, diet, smoking habits, and medication use were recorded, as well as measurements relevant for the cardiovascular risk profile: blood pressure (measured twice with an electronic device), body mass index (BMI), abdominal circumference, laboratory values, and medical history. Cognitive function was assessed using the Mini Mental State Examination 11 and disability was measured by the AMC Linear Disability Scale. 12 A detailed questionnaire on physical activity was used: the LASA Physical Activity Questionnaire. 13 Questionnaires are all validated specifically in elderly subjects.
In the absence of clear guidelines for elderly subjects, modifiable cardiovascular risk factors were conservatively defined as: blood pressure ≥160 mmHg, total cholesterol ≥5 mmol/l (primary prevention), low-density lipoprotein (LDL) cholesterol ≥2.5 mmol/l (secondary prevention), BMI ≥ 30 kg/m2, current smoking, and physical inactivity.
Statistical analysis
Data were analysed using STATA, version 10.0. Bivariate comparisons were performed using Student's t-test, chi-squared test, and Fisher's exact test for continuous, ordinal, and discrete variables respectively.
Potential impact of antihypertensive treatment
The intensive vascular care intervention used in the preDIVA study is aimed at decreasing incident dementia and CVD. As a first step towards a proof of concept, we attempt to predict the approximate number of cases with CHD and stroke that can be prevented by one of preDIVA's most important targets: improved blood pressure control. For blood pressure control, sufficient data are available from the literature to allow for such a projection, whereas for other risk factors data are sparse or absent for this age group.
To estimate the number of cases of CHD and stroke that can be prevented, relative risks for these events are needed for different levels of blood pressure reduction, along with information on the expected incidence rates in the population under study. Data from a meta-analysis on blood pressure-lowering medication by Law et al., 14 based on 147 RCTs including 464,000 subjects, provides age-specific relative risks for CHD and stroke for several degrees of blood pressure reduction (in mmHg). The results of this meta-analysis show that the relative risks are similar for patients with or without a history of CVD. The preventive effect of blood pressure reduction is detectable within a year, in contrast to, for instance, serum cholesterol reduction. 14 The expected incidence of CHD and stroke in our population is estimated using a national registry on community-dwelling subjects from general practices in the Netherlands. The incidences of events are based on five large general practitioner registries, with a total of 22,545 cases of CHD and 9623 cases of stroke (reported for men and women separately) in the age groups 70–74 and 75–79 years in 2007. 15
Within the preDIVA population, the incidence of new cases of CHD and stroke are calculated for the first 2 years after inclusion for men and women separately. To correct for mortality within the first year, which varies between 1–10% for 70–80-year-old subjects, the number of subjects at risk is conservatively multiplied by 1.9 for a 2-year prediction. Numbers of cases are displayed in rounded figures. The slightly higher risk of CHD and stroke due to a shift in age group for a part of the participants after 1 year is considered negligible and is not corrected for.
For the intervention group, the potential risk benefit can be applied for different degrees of systolic blood pressure reduction to estimate the absolute numbers of prevented events.
Safety and ethical aspects
The preDIVA study was approved by the medical ethics committee of the Academic Medical Centre, Amsterdam.
Results
Subjects
Between the May 2006 and March 2009, 125 GP practices within 29 healthcare centres were invited to participate in the preDIVA study. Nine primary care practices (within three healthcare centres) decided not to take part due to internal organizational problems.
Of 7774 subjects in 116 general practices, 13% were considered to be not eligible by their GP (Figure 1). A total of 6764 potential participants were informed about the study by a letter from the preDIVA investigators and their own general practitioner, of whom 3602 subjects (53%) signed for inclusion. During the inclusion period (before or within 2 weeks after the baseline measurement), 68 participants were excluded for various reasons (Figure 1). By March 2009, a total of 3534 subjects from 116 GP practices within 26 healthcare centres were included.
Recruitment and inclusion process of patients. *Specific data was available for >70% of GP (general practitioner) practices. ‡Cannot visit practice, alcoholic, living abroad, etc.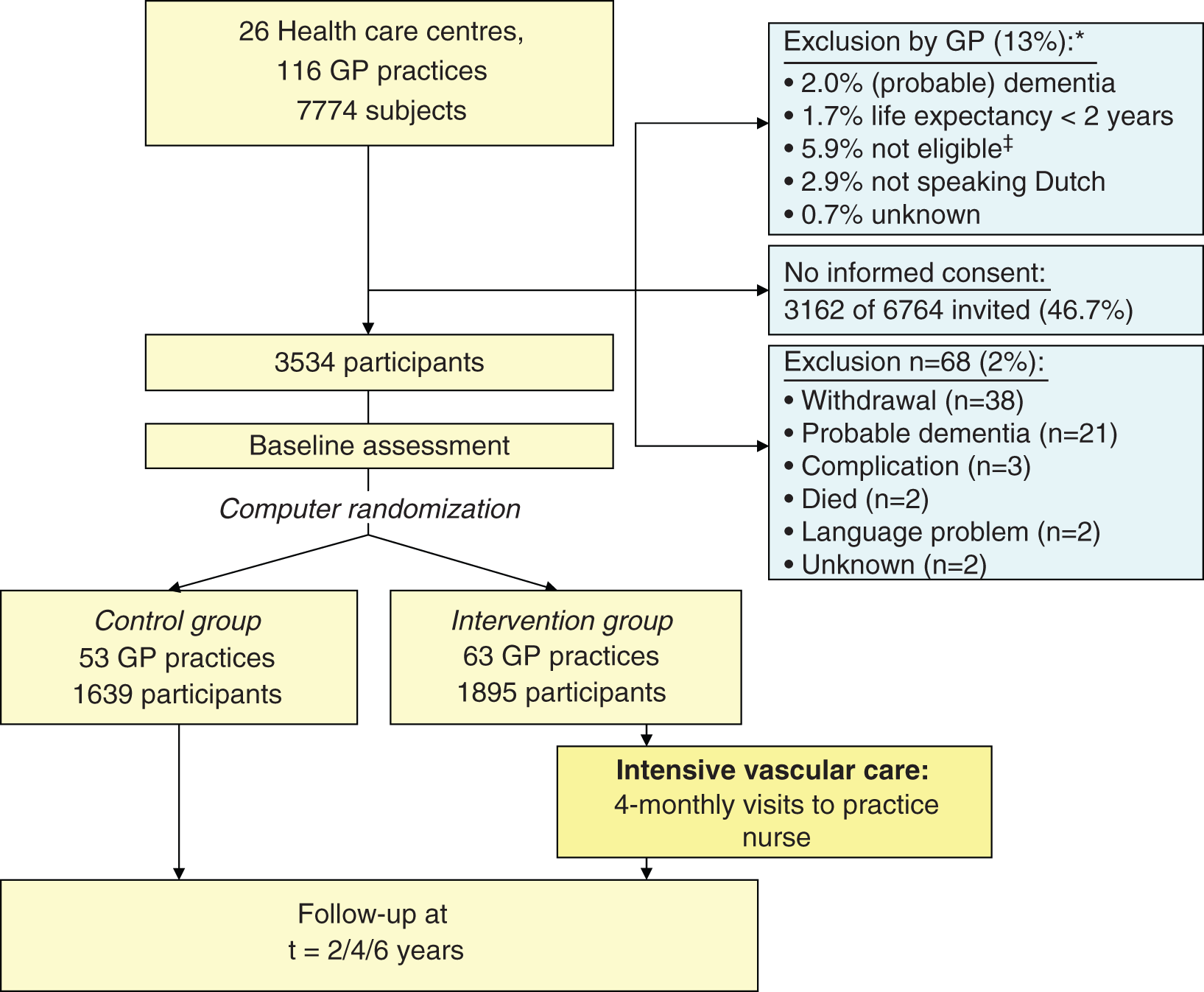
Baseline characteristics of participants
Characteristicsof all participants and with or without a history of cardiovascular disease
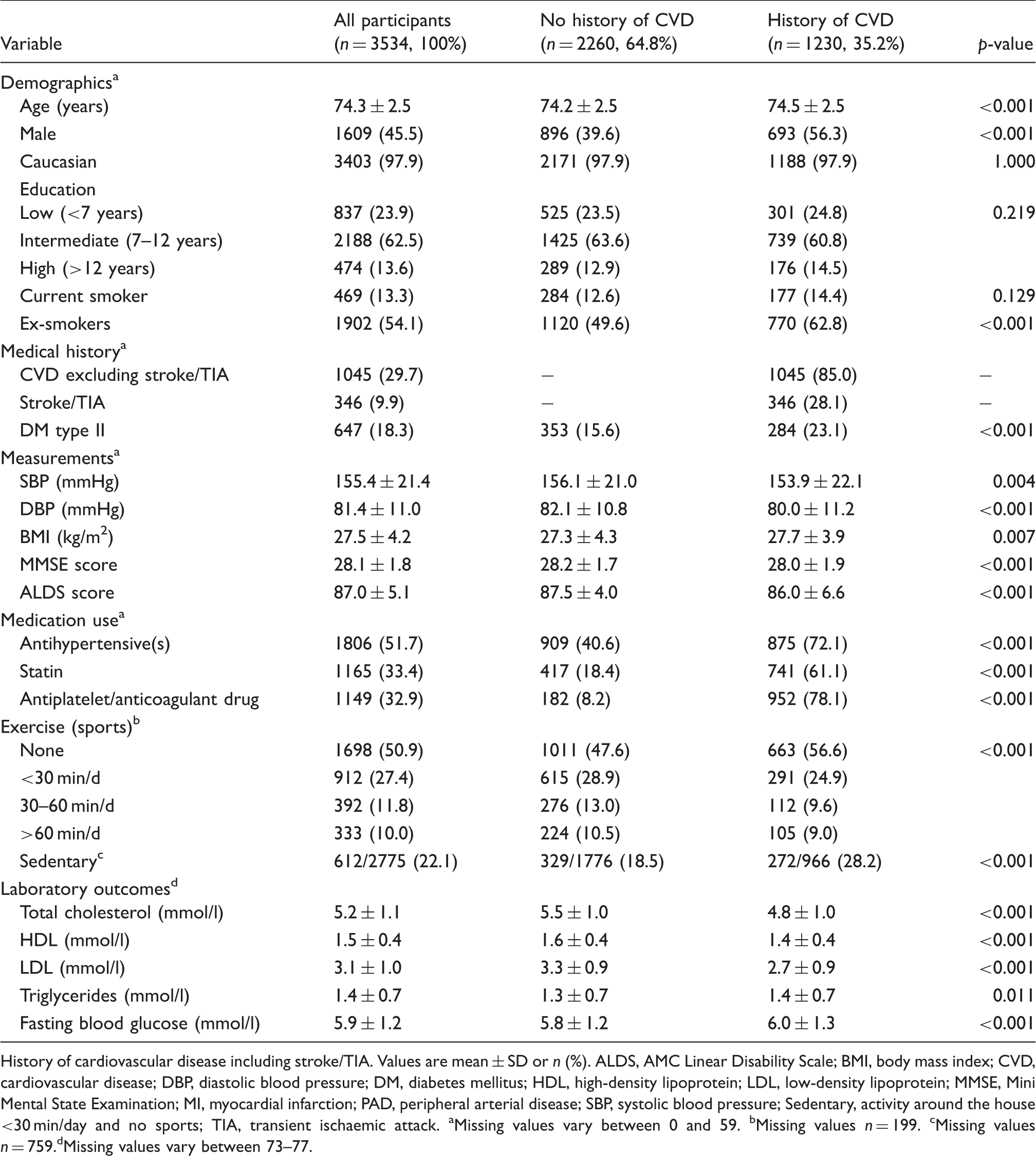
History of cardiovascular disease including stroke/TIA. Values are mean ± SD or n (%). ALDS, AMC Linear Disability Scale; BMI, body mass index; CVD, cardiovascular disease; DBP, diastolic blood pressure; DM, diabetes mellitus; HDL, high-density lipoprotein; LDL, low-density lipoprotein; MMSE, Mini Mental State Examination; MI, myocardial infarction; PAD, peripheral arterial disease; SBP, systolic blood pressure; Sedentary, activity around the house <30 min/day and no sports; TIA, transient ischaemic attack. aMissing values vary between 0 and 59. bMissing values n = 199. cMissing values n = 759.dMissing values vary between 73–77.
Risk factors and treatment
Cardiovascular risk factors are shown in Table 1 and Figure 2 for all participants with and without CVD (CVD+ and CVD−) in their history. For 44 patients (1.2%), medical history is unknown. Of all participants, 35.2% have a history of CVD. These participants are slightly older and more often male than the subjects in the group without a history of CVD.
Percentages of cardiovascular risk factors in subjects with or without a history of cardiovascular disease. BMI, body mass index; CVD, cardiovascular disease; Hyperlipidaemia, total cholesterol ≥5.0 mmol/l in primary prevention group, low-density lipoprotein >2.5 mmol/l in secondary prevention group; No sports, including no recreational walking/bicycling tours; SBP, systolic blood pressure (mmHg); Smokers, current smokers.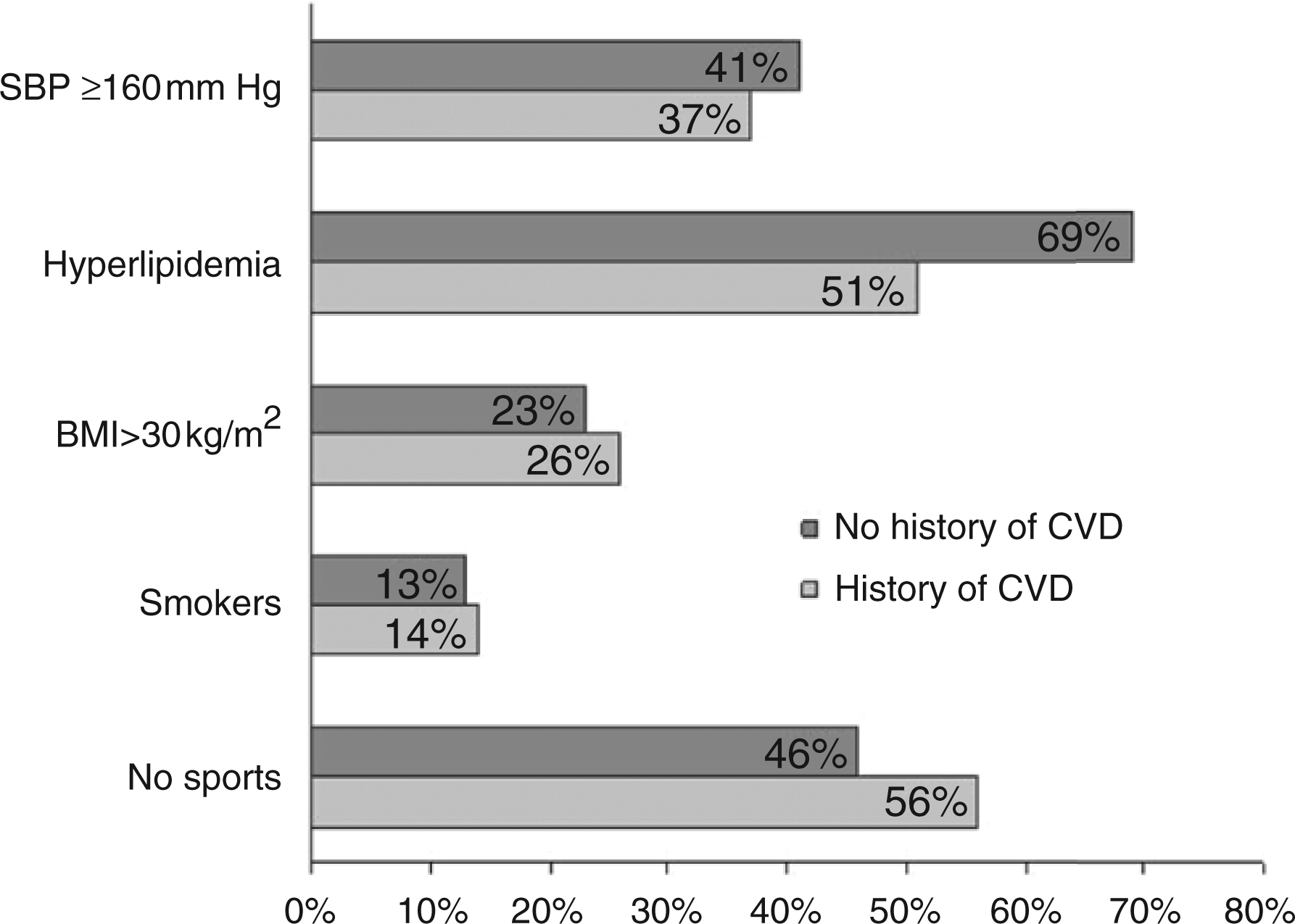
A systolic blood pressure ≥160 mmHg is present in 41% (CVD−) and 37% (CVD+), and ≥140 mmHg in 79% (CVD−) and 74% (CVD+) of participants. Dyslipidemia defined as total cholesterol ≥5.0 mmol/l is present in 69% of CVD− participants. In CVD+ participants, 39% have a total cholesterol ≥5 mmol/l, but 51% do not meet current treatment targets (LDL cholesterol <2.5 mmol/l). The overall score on the AMC Linear Disability Scale is high in both groups, indicating no or little physical impairment. Overall, in 63% of subjects two or more cardiovascular risk factors amenable to treatment can be identified, 64% and 60% for CVD− and CVD+ respectively.
It could be argued that patients with DM should be regarded as a secondary prevention group, because most of them are already regularly under control for glucose levels and cardiovascular risk factors. Exclusion of these participants from the CVD− group did not substantially change the results, with exception of presence of obesity which decreased from 23% to 20%, and dyslipidaemia which increased from 17% to 19%.
Cardiovascular medication use is shown in Table 1 and an overview of antihypertensive medication is presented in Figure 3. Use of blood pressure-lowering medication is reported by 41% (CVD−) and 72% (CVD+) of participants, resulting in a slightly better controlled blood pressure in the CVD+ group. CVD− participants mainly use thiazide diuretics which are the drug of first choice in primary prevention populations according to Dutch national guidelines. Of all participants with a systolic blood pressure ≥160 mmHg, 52% (CVD−) and 28% (CVD+) do not use antihypertensive medication. Those who do receive antihypertensive treatment still have a blood pressure ≥160 mmHg in 49% (CVD−) and 37% (CVD+), indicating suboptimal treatment. Statins are prescribed in 18% (CVD−) and 61% (CVD+), which results in better controlled lipids in CVD+ participants.
Percentages of antihypertensive use. ACE, angiotensin-converting enzyme; CVD, cardiovascular disease.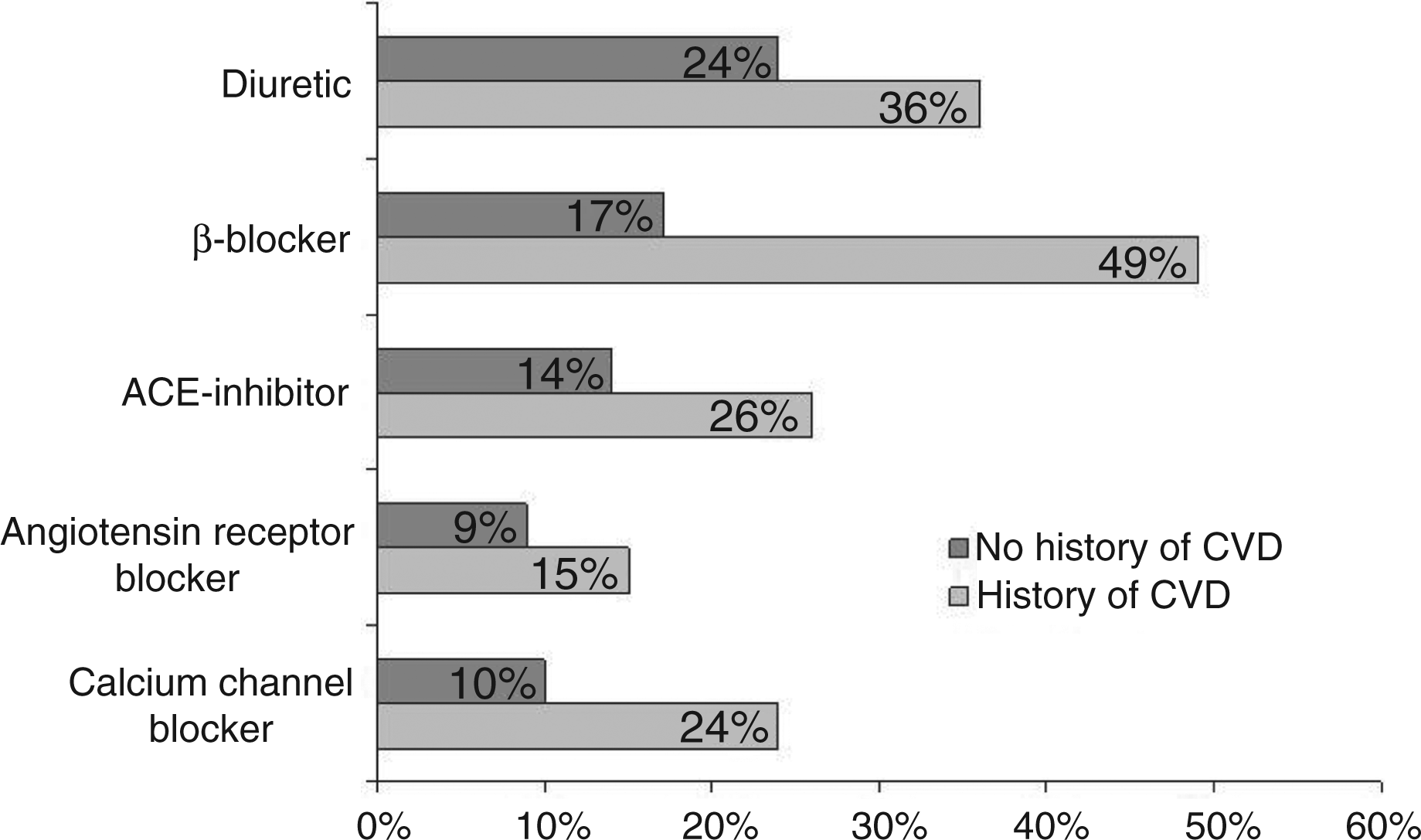
Potential impact of treatment of blood pressure
The number of cases of CHD and stroke that may be prevented per 1000 patient-years for different levels of blood pressure reduction are shown in Figure 4. The yearly incidences of CHD for the age groups 70–74 and 75–79 in the 2007 national registry were 25.4 and 28.5 (men) and 15.0 and 18.4 (women) per 1000 persons, respectively. For stroke, incidences were 8.4 and 12.5 (men) and 6.6 and 9.9 (women) in the same database.
15
Without the intervention under study, 75 cases of CHD and 32 cases of stroke are expected to occur among our total population of 3534 subjects in the first year of preDIVA. Of these, 40 CHD cases and 17 strokes (76 and 32 within 2 years) would occur in the intervention group, respectively (n = 1895). If the systolic blood pressure in the intervention group can be lowered by 5 mmHg, this corresponds with a relative risk (RR) of 0.88 for CHD and 0.84 for stroke in this specific age group.
16
This would result in absolute prevented numbers of nine CHD cases and five strokes in the preDIVA intervention group within 2 years (5/1000 and 3/1000 respectively, see Figure 4). For a reduction of 10 mmHg, relative risks are 0.77 for CHD and 0.70 for stroke, resulting in an absolute reduction of 17 cases of CHD and 10 cases of stroke in the intervention group within the first 2 years. For a 15 mmHg reduction, absolute numbers are 25 (CHD, RR 0.68) and 13 (stroke, RR 0.59). With increasing age, the relative risk of CHD and stroke events will rise but the number of participants ‘at risk’ will decrease.
Projected potential prevention of cases (n) of coronary heart disease (CHD) and/or stroke per 1000 subjects in the first 2 years, depending on the degree of systolic blood pressure decrease (mmHg) that will be achieved.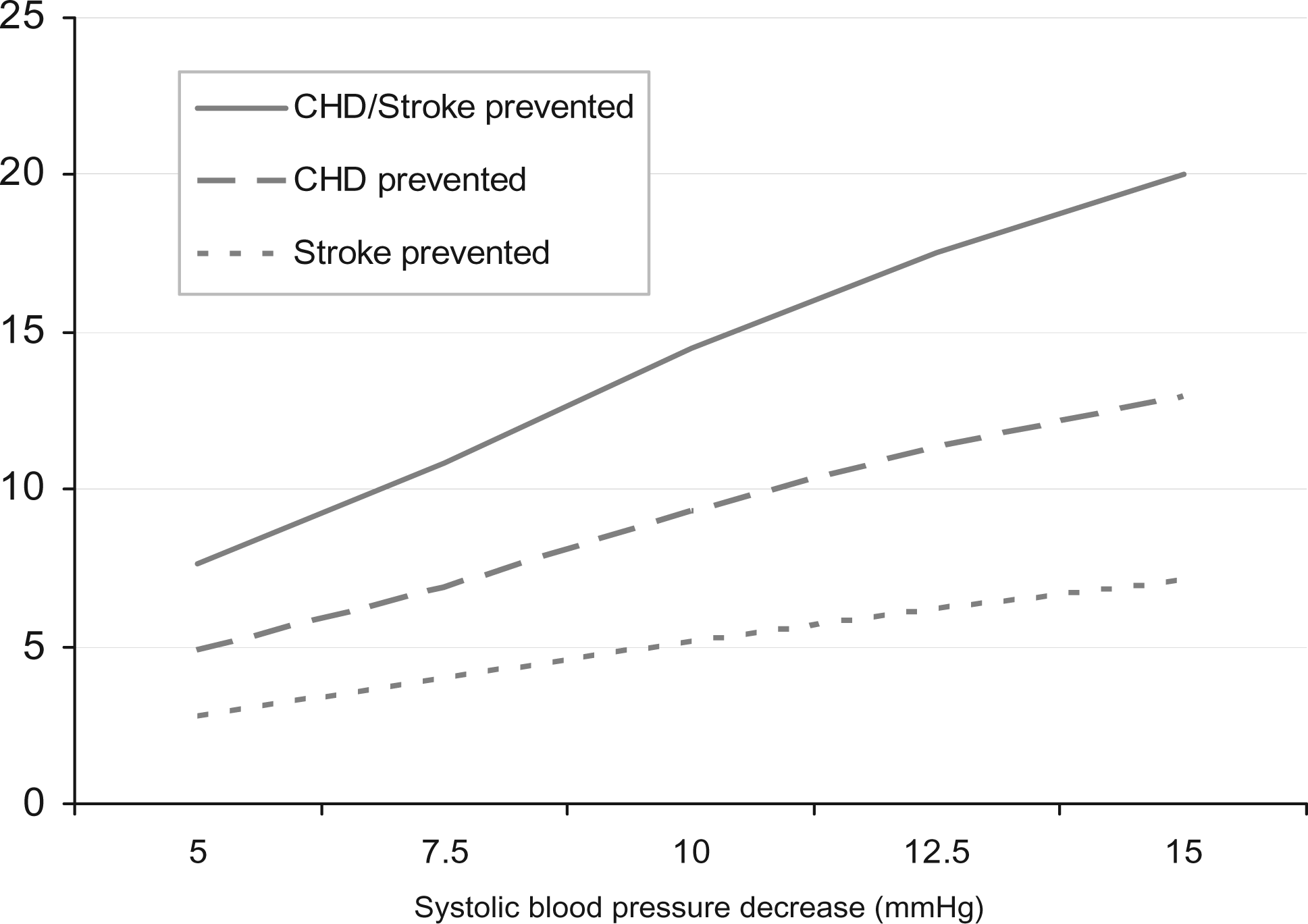
Discussion
Despite well-established, accessible primary healthcare and prevention programmes in the Netherlands, the majority of elderly in our population have a SBP ≥ 140 mmHg and more than one-third have a SBP ≥ 160 mmHg in both primary and secondary prevention populations. More than a quarter are obese and more than half do not meet treatment targets for LDL cholesterol. This indicates a substantial window of opportunity for better cardiovascular care and reduction of cardiovascular events. We illustrate this by presenting the projected benefit of blood pressure reduction. The actual benefit could be even higher when better treatment of other risk factors is taken into account and leads to an additive effect.
PreDIVA is the first study to assess the effects of an intervention aimed at improving the cardiovascular risk profile as a whole in a general practice population of participants above 70 years of age with a special focus on dementia prevention. The possible relation between cardiovascular risk factors and cognitive decline or dementia was previously studied in several RCTs, but these were mainly based on secondary outcome measures and on assessment of one risk factor at the time. 17 When systematically reviewed, data on antihypertensive treatment and cognition are not yet conclusive while for statins no benefit was found on cognition.18,19
The preDIVA participants, who were recruited through GPs, represent a relatively unselected population. This offers an excellent opportunity to explore patterns of morbidity and mortality among community-dwelling elderly. The results could therefore be of great value when considering better cardiovascular healthcare on a population level and could facilitate decision making in public health policies.
A growing number of GP practices in the Netherlands have (nurse-led) secondary prevention programmes (e.g. for DM) or hypertension programmes, which may favourably influence cardiovascular risk profiles over time (and may have done so in previous years). A positive change of cardiovascular risk profile over time has been reported before 20 and in our population this is illustrated by significantly better controlled blood pressures and lipids in participants with a history of CVD. Nevertheless, we see a large window of opportunity to improve care, similar to other reports from Western European countries. 21 We expect that regular care, close monitoring of blood pressure, and continued counselling of medication adherence and life-style changes can add significantly to participants’ health, as has been previously shown.22–25
Cardiovascular history was assessed by practice nurses together with patients. The nurses are trained in cardiovascular risk management and have access to medical records from which cardiovascular events can be easily extracted. Participants were also asked if they were taking antihypertensive medication, cholesterol-lowering medication, or anticoagulants (yes/no/don't know). In addition, medication lists were collected to verify these data.
There are some limitations to our analysis that merit consideration. The potential impact of blood pressure reduction on major cardiovascular events was predicted using published data on relative risks and incidence numbers.14,15 Although these data are based on large population studies, we cannot be absolutely sure that they are representative for our study population. The incidence of events might be overestimated due to the selection of motivated and possibly relatively healthy elderly in our prevention study. However, the prevalence of hypertension (SBP ≥ 140/90 mmHg) in US populations of subjects aged 70 and older varied between 63–83%, which is comparable to our population (SBP ≥ 140/90 in 74–79% of participants). 26
Comparison of the characteristics of the preDIVA population with national (cohort) data suggests that our population is to a large degree representative for the Dutch general population. In the Dutch Doetinchem cohort study (n = 4520, 2003–2007), 27 73–76% of subjects aged 65–75 had hypertension according to the WHO criteria. In the same cohort, 18–28% was reported to have obesity (BMI > 30 kg/m2) versus 24% in our population The number of smokers in 2008 in the overall Dutch population was 12–15% in women and men aged 65 and up, which is also comparable to our study population (13.3% smokers). 15
We only assessed the effect of reduction of blood pressure, while in fact the intervention aims to improve the cardiovascular risk profile as a whole. Influence of other factors could not be taken into account in this prediction, due to a lack of data in elderly patients. In several years, we will be able to validate the projected preventive effect in the preDIVA population.
Many older people already use a considerable number of drugs. Due to physical changes, comorbidity, and drug interactions, elderly are more likely to experience adverse effects from prescribed medication. 28 On the other hand, there is convincing evidence that blood pressure- and cholesterol-lowering treatment prevent major cardiovascular events in elderly aged up to 80 years.4,5,29 Vigilance regarding polypharmacy and close monitoring of medically induced adverse events that relate to prescribed (added) medication is of great importance in this elderly population. Hence, completeness of follow up will be pivotal to assess a realistic harm–benefit ratio of the intervention studied.
At advanced age, there is an increasing presence of competing risk of mortality: for instance, the RR reduction from cardiovascular death is offset by a growing cancer mortality risk with increasing age. Nevertheless, the benefits of cardiovascular interventions such as treatment of blood pressure or dyslipidaemia have proven to remain substantial at high age because of high incidence rates of myocardial infarction, stroke, and other major cardiovascular events.6,14,30 Also, recent evidence suggests that lowering blood pressure in elderly people may prevent or postpone dementia, which is a major cause of disability and a social and economic burden.7,8 Therefore, competing risks should not be considered a decisive argument against preventive strategies for CVD in the elderly.
Conclusion
Our data show that cardiovascular risk profiles in elderly people with and without overt CVD can be improved substantially. By lowering systolic blood pressure by 5–15 mmHg in an elderly population, the incidence of CHD may be reduced by 12–32% and for stroke by 16–41%. Continued follow up of the preDIVA study will answer the question whether these potential benefits can be realized in practice and whether the advantages ultimately outweigh potential drawbacks such as side-effects of the treatments that are initiated.
Footnotes
Acknowledgments
The authors thank CE Miedema for project management, MM Langemeijer for help with database management, BJ van den Born for advice on the manuscript and all practice nurses and participants for taking part in this study.
Funding
This work was supported by the Dutch Ministry of Health, Welfare and Sports (grant number 50-50110-98-020), the ‘Innovatiefonds Zorgverzekeraars’ (Innovation fund of collaborative health insurances, grant number 05-234) and ZonMw (Dutch nonprofit research organization, grant number 62000015).
Conflict of interests
The authors declare that there is no conflict of interest.