
Abstract
Prescription To Get Active (RxTGA) is a community-based organization that partners with healthcare providers and the fitness industry to promote physical activity (PA) through tailored prescriptions. Because enrollment declined during the pandemic, an evidence-based supplement that could be delivered remotely as a support was sought. This randomized pilot trial involved examining the impact of adding Motivational Interviewing via Co-Active Coaching to a traditional 12-week RxTGA offering on health indices and PA adherence among adults. As the first study integrating a validated coaching model into an established prescription program, methodological details will be beneficial for health- and fitness-focused professionals and researchers.
Keywords
Introduction
Each year, chronic conditions such as cancer, diabetes, and cardiovascular disease account for 41 million deaths worldwide—nearly 74% of all global mortality (World Health Organization, 2022). In Canada, 44% of adults over age 20 and 73% of those aged 65 and older live with at least one noncommunicable disease (Public Health Agency of Canada, 2019, 2020). These illnesses significantly diminish both quality and quantity of life (Patra et al., 2007) while imposing a substantial societal and economic burden (Advisory Committee on Population Health et al., 2005; Megari, 2013). The estimated costs of chronic disease to the Canadian economy are more than $190 billion annually (Chronic Disease Prevention Alliance of Canada, 2017). Yet despite widespread recognition of this issue, prevalence rates have continued to rise over recent decades (Public Health Agency of Canada, 2017), a trend accelerated further by the COVID-19 pandemic. As the population ages and diagnoses increase, growing concern surrounds the long-term sustainability of Canada's healthcare system and the subsequent need for structural reform (Canadian Medical Association, 2021, 2022; Frank, 2022; Public Health Agency of Canada, 2013).
Despite these grim statistics, there are modifiable health behaviors known to reduce one's risk for developing chronic disease (World Health Organization, 2022). Regular physical activity, in particular, has been deemed an effective tool to prevent, delay, and manage a wide range of physical and mental health conditions (Booth et al., 2012; Goodwin, 2003; Irwin et al., 2019; ParticipACTION, 2022; Rebar et al., 2015; Warburton et al., 2006), with extensive evidence demonstrating both short- and long-term benefits (e.g., Bize et al., 2007; Rebar et al., 2015). Beyond disease prevention and management, its’ positive effects include enhanced brain health, heightened energy, decreased stress, improved mood, reduced risk of falls, improved ability to carry out daily activities, and lowered risk for premature death (e.g., Centers for Disease Control and Prevention, 2022; Public Health Agency of Canada, 2023). However, few people achieve the amount of physical activity necessary to realize these health benefits (Kohl et al., 2012; Tison et al., 2022). In Canada, the 24-Hour Movement Guidelines outline recommendations across the lifespan to enhance quality of life and reduce chronic disease risk, including at least 150 min of moderate-to-vigorous physical activity per week and two or more days of muscle-strengthening activities for adults (Ross et al., 2020; Tremblay et al., 2016, 2017). Unfortunately, global data indicate that physical activity levels have declined substantially since the COVID-19 pandemic (Caputo & Reichert, 2020; Park et al., 2022; Stockwell et al., 2021; Wunsch et al., 2022), a trend echoed in Canada (Di Sebastiano et al., 2020; Woodruff et al., 2021). Concomitantly, it is likely that many adults formed new habits involving less activity during this time, which may be difficult to change as the pandemic recovery era continues (Maltagliati et al., 2021). Considering the proven advantages of regular movement, identifying effective strategies to increase physical activity has the potential to yield widespread benefits, enhancing individual and population health while reducing strain on the healthcare system (Manuel et al., 2021).
Prescription-Based Physical Activity
One approach that has shown utility as a therapeutic modality is prescription-based physical activity (PPA), a strategy whereby healthcare providers give patients specific movement recommendations to facilitate the prevention and management of chronic disease and combat sedentary behavior (Lundqvist et al., 2022; Pedersen & Saltin, 2015; Thornton et al., 2016, 2022). Healthcare providers are particularly well-positioned to provide such recommendations as they are viewed by patients as credible and valued sources of health-related information (Fowles et al., 2018; Petrella et al., 2007). A large body of evidence highlighting the health and engagement benefits of PPA exists (Loellgen et al., 2020; Onerup et al., 2019; Orrow et al., 2012). Cost effectiveness of PPA has also been demonstrated (Anokye et al., 2014; Ryen et al., 2023), thereby emphasizing its potential as a wide reaching health promotion strategy.
Prescription to Get Active
While the integration of PPA in Canada and the United States has grown steadily in contexts such as primary care (Laberge et al., 2024), and medical school training (Asif et al., 2022; Capozzi et al., 2022), competing priorities and barriers to use such as lack of time, knowledge, and resources can make implementation a challenge in the clinical setting (Hébert et al., 2012; Tchirkov et al., 2021). One organization that seeks to address such barriers while promoting movement as a health promotion strategy is Prescription to Get Active (RxTGA; RxTGA, 2020). With the goal of enhancing the health and wellbeing of communities across Alberta, RxTGA partners with healthcare providers who identify adults that could benefit from being more active based on Canada's movement guidelines. The RxTGA program is intended for patients who are deconditioned, sedentary, or at risk of developing a chronic condition and can safely begin an unsupervised physical activity routine (RxTGA, 2020). While medical doctors and nurse practitioners have predominantly been involved as prescribers for RxTGA, there has been a rise in engagement from other allied health professionals such as registered nurses, psychologists, occupational therapists, physiotherapists, kinesiologists, and dietitians (RxTGA, 2020).
When a healthcare provider identifies that a patient may benefit from more physical activity, a written exercise prescription is provided. The patient can then redeem this prescription by registering it on the RxTGA (2020) website. The provider is not required to give advice or develop an exercise program but instead, serves as a catalyst for prescription redemption. Once the patient has registered their prescription online, they receive entry to a participant dashboard that provides details on many complementary and low-cost resources to support their physical activity journey including free trial access to local fitness and recreation facilities ranging from 3 to 30 days, outdoor trail routes, online movement and exercise videos, smartphone and web-based behavioral support applications, and written materials to foster a more active lifestyle. To date, RxTGA has established partnerships with more than 150 facilities throughout Alberta including community recreation centers, YMCAs, privately operated gyms/fitness centers, as well as yoga and martial arts studios. This wide range of options allows patients to choose what suits them best: a stated value of RxTGA. Upon arrival at their chosen facility, trained staff members provide prescription recipients with an orientation to the establishment's amenities and services. They also discuss the individual's goals for the duration of the free-trial period, and many provide a mutually agreeable workout program to get started.
Once registered, the prescription recipient may also choose to access free trials from any device with an internet connection for independent exercise programming from qualified online service providers. There is a variety of activities such as yoga, strength training, cardio workouts, and stretching routines that cater to different fitness levels and desired durations. Additionally, participants receive exclusive access to smartphone applications that provide guidance and support for enhancing their activity level through a personalized workout plan. The online platform also includes a resource library with evidence-based literature and videos on various topics including getting started resource guides, balance improvement techniques, walking resources, and strength training methods. If a participant does not have an email address or access to the internet, there is a telephone number that they can call for program support. Using this model, the RxTGA program is uniquely positioned as a conduit between the healthcare system and fitness and recreation industry, actively promoting the connection between regular physical activity and chronic disease reduction.
Since the onset of the COVID-19 pandemic, RxTGA has experienced notable challenges. Public health measures such as isolation requirements and the shift in healthcare priorities toward acute care contributed to a significant decline in program uptake—from approximately 10 new enrollments per day prepandemic to just 1.5 by late 2020. This decline occurred alongside well-documented and longstanding adherence challenges; approximately half of individuals who initiate an exercise program discontinue within 6 months. Although anecdotal feedback has highlighted RxTGA's potential to improve various health indices, no formal evaluation has been conducted to date. Given the well-established benefits of physical activity and the program's broad reach potential, innovative strategies to enhance engagement and retention were warranted.
Motivational Interviewing via Co-Active Life Coaching
Motivational Interviewing via Co-Active Life Coaching (MI-via-CALC; Kimsey-House et al., 2018; Miller & Rollnick, 2013) has emerged in recent decades as a promising approach for behavior change and was therefore identified as a suitable complement to RxTGA. Motivational Interviewing is a client-centered counselling style that focuses on helping individuals to explore and resolve their ambivalence about change (Miller & Rollnick, 2013; Rollnick & Miller, 1995). However, there have been criticisms regarding its inconsistent training requirements, as well as challenges associated with the practical application of its theoretical principles (Mesters, 2009). To address these concerns, researchers have proposed integrating the CALC model, which encompasses principles similar to MI and also includes specific tools that can be implemented in practice (Newnham-Kanas et al., 2010). The MI and Co-Active models emphasize collaboration between the coach and client based on the belief that clients themselves know what is best for them (Kimsey-House et al., 2018; Miller & Rollnick, 2013; Rollnick & Miller, 1995).
The MI-via-CALC approach is aligned with various health behavior change theories (Ajzen, 1991; Bandura, 1986; Ryan & Deci, 2017), and aims to establish a dynamic relationship between a trained coach and client, with the coach serving as a guide during the client-directed conversations. Within this model, coaches refrain from giving advice or solutions (Kimsey-House et al., 2018). Rather, the role of the coach is to support clients, elicit answers from within them, and facilitate exploration and movement toward achieving goals (Kimsey-House et al., 2018). Each session is unique as it is driven by the client, while coaches are equipped to listen actively, ask meaningful questions, and promote empowerment (Kimsey-House et al., 2018).
Researchers using MI-via-CALC have found positive health-related outcomes in several contexts (e.g., obesity, smoking cessation; Mantler et al., 2010; Pearson et al., 2013) and populations (e.g., new mothers, university students; Harvey et al., 2020; Pearson et al., 2012). However, including this model as part of an established physical activity prescription program in service of maintaining engagement has yet to be examined in the literature and could prove valuable from a public health perspective. The Motivation to Move Study (M2M) study was developed to evaluate the effectiveness of the RxTGA program by comparing outcomes from standard program delivery with those from a version enhanced by a supportive coaching component among adults at risk for chronic disease in Alberta, Canada.
The purpose of this article is to describe the M2M study method and associated rationale in service of assisting future researchers and program planners who are interested in identifying avenues to enhance physical activity engagement and health indices through PPA.
Methodology
M2M Study Purpose and Design
To inform the ongoing development of the RxTGA model, the M2M study was designed around three main objectives: (1) to examine the effectiveness of RxTGA compared to RxTGA enhanced with virtual activity coaching using MI-via-CALC on physical activity adherence, health indices (e.g., quality of life and mental health), and psychological variables related to movement (e.g., self-efficacy and motivation) over a 12-week intervention and 6-month follow-up period; (2) to qualitatively explore participants’ experiences of involvement in the program”; and (3) to conduct a secondary investigation examining the training and program delivery experiences of the volunteer activity coaches who supported M2M participants.
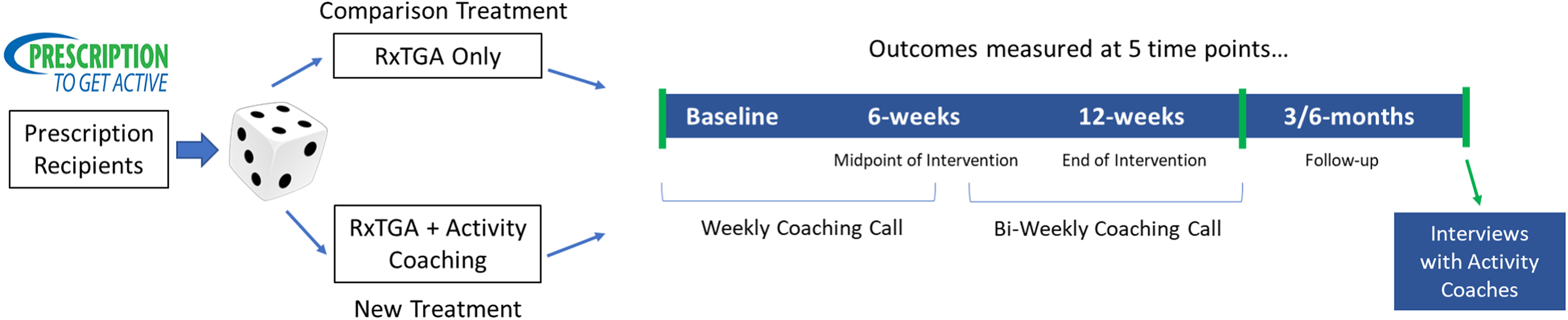
A parallel group, pilot randomized trial design with an equal allocation ratio was employed to enable comparisons between the two conditions at baseline, mid-intervention (6-weeks), immediately post-intervention (12-weeks), and at two follow-up timepoints (i.e., 3- and 6-months post-intervention; see Figure 1). A qualitative component was also integrated to capture a more comprehensive understanding of participant involvement and to provide deeper insights into changes in physical activity and health over time. Given the RxTGA model had not yet been evaluated using a coaching-enhanced format, a pilot design was deemed appropriate to assess feasibility, refine implementation procedures, and generate preliminary effect estimates to inform future large-scale research. Ethical approval for the study was obtained through the host institution's Research Ethics Board (#1469087).
Study design and randomization.
Study Timeline
Recruitment commenced in March 2022, with the first participant enrolled in April 2022. Recruitment continued until the last participant was enrolled in October 2022. For the duration of the study, there were few public health protections related to COVID-19 in place in Alberta (Canadian Institute for Health Information, 2022).
Participant Inclusion and Exclusion Criteria
Prescription Recipients
Eligibility criteria included being an adult aged 18 years or older, residing in Alberta with Internet access, and engaging in less than 150 min per week of moderate-to-vigorous intensity physical activity as defined by the Canadian Physical Activity Guidelines (Ross et al., 2020) and determined by the referring healthcare provider. Pregnant women were not considered eligible. For safety reasons, individuals with prescriptions older than 1 year were asked to obtain an updated referral prior to enrollment. Given the pilot-oriented nature of the study and the uncertainty surrounding COVID-19-related disruptions, no formal power calculation was performed. Instead, sample size estimates were informed by RxTGA enrollment rates at the time and comparable behavior change studies (Cotten & Prapavessis, 2016; Duvivier et al., 2017; Edwards & Loprinzi, 2017; Sui & Prapavessis, 2021). Accordingly, the recruitment target was set at 60 participants (n = 30 per condition) on a rolling basis between February and December 2022.
RxTGA Activity Coaches
Volunteer “Activity Coaches” with backgrounds in health and/or fitness who were willing to be trained in MI-via-CALC principles through a vetted standardized training program, had internet access, and resided in Canada were eligible to participate. Coaches were required to support at least two prescription recipients over a 6-month period. Consistent with the participant sample size rationale, it was anticipated that five to eight coaches would be recruited.
Recruitment and Onboarding
Prescription Recipients
Traditionally, RxTGA participants are referred to the program by a healthcare provider and instructed to register their prescription online. Thus, the RxTGA website served as the primary recruitment method for the M2M study. Additional participants were recruited through posters placed in Alberta-based recreation facilities, coffee shops, and other community venues, as well as through emails sent to individuals on the RxTGA mailing list. Those recruited through these means were directed to request a prescription from their healthcare provider. Upon registering their prescription on the RxTGA website, individuals were asked whether they were interested in joining the M2M study, selecting either “Yes, I would like to participate in the M2M Study” or “No, please take me back to the main registration site” (i.e., traditional RxTGA enrollment without research involvement). For those who opted in, contact information was forwarded to the study research assistant, who followed up to confirm eligibility, review the letter of information, address questions, and obtain informed consent.
RxTGA Activity Coaches
Activity coaches were recruited through Canadian personal trainer and kinesiology networks, the International Coaching Federation, and graduates of the standardized MI-via-CALC training program (Monarch System, n.d.). Advertisements were also distributed to canfitproTM Trainers, Canada's largest provider of fitness training and education (canfitpro, 2023). Interested individuals contacted the RxTGA Executive Director, who, in consultation with the research team, assessed eligibility. Those who met the inclusion criteria and elected to participate were enrolled in the online Activity Coach training and the M2M/RxTGA Study Orientation.
The MI-via-CALC Training Program
Once recruitment was complete, eligible Activity Coaches were enrolled in a 2-day online training program delivered through the Monarch SystemTM Inc. (n.d.). This evidence-based behavior change model for health professionals was created and facilitated by two professors of health sciences who are also Certified Professional Co-Active Coaches. The curriculum integrates a unique blend of processes adapted from MI, coaching, and complementary behavior change theories to enhance communication and client support skills. Training content emphasized strategies such as asking meaningful questions, using reflective listening, connecting values to behavioral goals, and genuinely affirming/acknowledging clients, alongside extensive opportunities for hands-on practice and personalized feedback from the instructor. The goal was to equip coaches with practical, evidence-informed tools to help clients reach their health potential. Training occurred over two weekends and was funded by RxTGA as a token of appreciation for the coaches’ anticipated volunteer contributions.
In addition to this standardized training, volunteers completed a 120min online orientation led by the RxTGA Executive Director and a Board of Directors Member with expertise in coaching, which provided an overview of the RxTGA program and study requirements. The M2M Principal Investigator also presented the study's evaluative components and research involvement criteria. Following these sessions, Activity Coaches received a detailed handout outlining study-related procedures, expectations, and tools designed to foster motivation and support commitment to healthier behaviors among clients.
Procedures: RxTGA Participants
Once eligibility was confirmed and informed consent obtained, the research assistant emailed participants a link to the baseline assessment survey. Upon its completion, participants received an email detailing their group assignment (i.e., the traditional RxTGA program or the traditional RxTGA program plus activity coaching) which was allocated by simple randomization using a computer-generated sequence. Also included in this email was a list of RxTGA activity offerings, link for physical activity tracking, and the coaches’ contact information, if applicable. Procedures specific to each group are outlined below.
The Traditional RxTGA Group
Participants in the traditional RxTGA group received a physical activity prescription from their healthcare provider and redeemed it on the RxTGA website. They were encouraged to create a personalized activity plan using available RxTGA resources and to record the frequency, duration, and type of their weekly physical activity throughout the 12-week study period using the provided tracking link.
The Activity Coaching Group
Participants assigned to the Activity Coaching group were likewise encouraged to create a personalized physical activity plan using RxTGA resources and to record weekly activity (i.e., frequency, duration, and type) via the link provided. Additionally, participants were paired—based on a predetermined randomization sequence—with an Activity Coach trained for the study. Coaching was conducted remotely through a mutually agreed upon platform or by telephone. If a designated coach was unavailable at the time of the pairing, the next coach in sequence was assigned. Participants received their coach's contact information and were asked to arrange an initial meeting within 2 days, while the research assistant notified the coach of the new assignment and provided a tracking sheet to record the date, duration, and mode of each session, along with notes pertaining to the format or general experience.
Participants and coaches met weekly for the first 6 weeks, and then bi-weekly for the remaining 6 weeks, totaling nine sessions over the 12-week intervention. Each encounter lasted approximately 30 to 45 min. Remote delivery is consistent with standard coaching practice and aligned with pandemic-related restrictions in effect at the time. The duo was responsible for scheduling all sessions. In terms of content, coaches were instructed to apply principles from their MI-via-CALC training and the M2M orientation. The first session focused on establishing the coach-participant relationship, identifying barriers to an active lifestyle, setting and agreeing upon goals, and developing an activity schedule. Subsequent sessions centered on applying MI-via-CALC techniques to support progress toward these goals and address emerging participant priorities. The research assistant maintained ongoing contact with the coaches to monitor session completion and coordinate the timely distribution of assessment invitations and survey links for participants.
Assessments
All M2M participants completed five assessments to evaluate health indices and study-related experiences at baseline, 6-weeks, 12-weeks, and 3- and 6-months post-intervention. Surveys were administered via Survey Monkey and could be completed independently or, if preferred, with the help of a research assistant through a phone or video call. One week before each scheduled assessment, participants received an email reminder that included the option of booking a guided session. Those who did not respond or declined assistance were sent the survey link to complete on their own. Each assessment took approximately 20 min.
Measures
Demographic Information
To characterize the sample, participants completed a demographic questionnaire at baseline that included items such as gender, age, height, weight, education, income, relationship status, employment status, and ethnicity.
Physical Activity Behavior: The International Physical Activity Questionnaire (IPAQ)
The IPAQ is a validated and widely used instrument for assessing physical activity. Participants recalled their activity over the previous 7 days at vigorous, moderate, and walking intensities, as well as their average daily sedentary time. Physical activity was expressed in Metabolic Equivalent Task (MET) minutes, a composite measure reflecting duration, frequency, and intensity of activity. Higher MET values indicate greater overall physical activity levels. The IPAQ has demonstrated acceptable measurement properties for monitoring adult physical activity across diverse settings (Craig et al., 2003). Data truncation and scoring followed standardized protocols outlined by Craig et al. (2003).
Physical Activity Tracking
Participants provided a detailed account of their weekly physical activity throughout their M2M involvement using a SurveyMonkey link or paper form. They were asked to record the date, type, duration (in minutes), and perceived intensity of each physical activity session over the previous 7 days. Every Friday, the research assistant emailed all active participants a link to the tracking template, and on the following Tuesday, reminder emails were sent to those who had not yet submitted their entries.
Health-Related Quality of Life: 12-Item Short-Form Health Survey (SF-12)
The SF-12 Health Survey is a widely used multidimensional measure of health-related quality of life (QOL), reflecting individuals’ self-perceived physical and mental health over time. Adapted from the longer SF-36 Health Survey (Ware & Sherbourne, 1992), the SF-12 includes eight health concepts that contribute to two summary measures: the Physical Component Summary and the Mental Component Summary. The eight domains include: physical functioning, role-physical, bodily pain, general health, vitality, social functioning, role-emotional, and mental health—each capturing different aspects of physical, emotional, and social wellbeing. The SF-12 contains 12 items comprised of Likert scale and yes/no responses. Sample items include: “In general, would you say your health is:____,” rated from poor (1) to excellent (5), and “During the past 4 weeks, how much did pain interfere with your normal work (including work outside the home and housework)?” rated from not at all (1) to extremely (5). Scoring followed the standardized procedures outlined by Ware et al. (1996). The SF-12 has demonstrated strong reliability and validity for use in adult populations.
Exercise Motivation: Behavioral Regulations in Exercise Questionnaire (BREQ-3)
The BREQ-3 assesses behavioral regulation in exercise along the motivational continuum, consistent with Self-Determination Theory (Deci & Ryan, 1985, 1991). The questionnaire includes 24 items across six subscales: amotivation and external, introjected, identified, integrated, and intrinsic regulation. Researchers have found that autonomous types of motivation are favorable when it comes to starting and continuing to engage in physical activity (Ryan & Deci, 2017; Teixeira et al., 2012). Participants rate how true each statement is for them (e.g., “It's important for me to exercise regularly,” “I exercise because other people say I should,” “I feel like a failure when I haven’t exercised in a while”). Mean scores are calculated for each subscale, with higher scores reflecting a greater degree of the corresponding motivational regulation. The BREQ-3 has demonstrated sound psychometric properties and is widely used in exercise motivation research (Markland & Tobin, 2004; Wilson et al., 2006).
The 18-Item Psychological Well-Being Scale
This 18-item instrument assesses six dimensions of wellness: autonomy, personal growth, environmental mastery, positive relations with others, purpose in life, and self-acceptance. Each domain is measured using three items rated on a seven-point Likert scale. Sample items include: “I like most parts of my personality,” “In many ways I feel disappointed about my achievements in life,” and “I tend to be influenced by people with strong opinions.” Scores for each domain are summed, with higher totals reflecting greater psychological wellbeing. The scale has demonstrated satisfactory reliability and validity among adult populations (Ryff & Keyes, 1995).
Overcoming Barriers to Physical Activity: Self-Efficacy for Exercise Scale (SEE)
The SEE is a validated measure assessing confidence in one's ability to maintain regular exercise despite common barriers such as poor weather, lack of time, or exercising alone. The nine-item questionnaire asks participants to rate their confidence in exercising three times per week for 20 min on a 10-point scale ranging from (0) not confident to (10) very confident. Responses are summed to yield a total score between 0 and 90, with higher scores indicating greater exercise self-efficacy. The SEE has shown strong reliability for use with adult populations (Resnick & Jenkins, 2000).
Study-Related Goals and Experiences
In addition to the validated tools described above, a series of questions about study-related experiences was also included (e.g., rationale for joining the program, primary goals, challenges, and motivations related to being active). Question type included a combination of multiselect responses with an option for participants to add a written response as well as several open-ended questions. As well, participants were asked to describe their use of the various activity offerings provided by RxTGA at all time points. This qualitative portion of the study was included at the baseline, 12-week, 3- and 6-month assessments.
Procedures: The Activity Coaches
After providing informed consent to participate, the Monarch SystemTM Inc. training, and M2M study orientation, all coaches completed a demographic questionnaire which included a series of open and closed-ended questions to explore employment history and study-related goals. Within 1 week of completing the final session with their last participant, coaches were invited to participate in a one-on-one semistructured interview with a member of the research team to explore study-related experiences and recommendations for future programming. The interviews were conducted remotely by the study research assistant and/or Principal Investigator over video call or telephone, and lasted between 30 and 60 min.
Data Analysis
Primary analysis of the quantitative data involved calculating descriptive statistics (e.g., means and frequencies) and conducting multiple two-way mixed analysis of variances (ANOVAs) to examine changes over time between groups, where the within-subjects factor was time, and the between-subjects factor was group allocation. The dependent variables included physical activity behavior, quality of life, exercise motivation, psychological wellbeing, and self-efficacy to overcome barriers. SPSS was used to conduct these analyses. Data analysis was conducted using the principle of intention to treat with series mean or last outcome carried forward applied to account for missing data. Participants were included in the analysis up to the end of intervention if they completed the baseline and one or more of the 6- or 12-week assessments. Participants were included in the follow-up analysis if they completed the baseline, one or more of the 6- or 12-week assessments, and one or more of the follow-up assessments.
To synthesize and generate the qualitative data (i.e., open ended questions from study participants; coach interviews), a combination of inductive (Elo & Kyngäs, 2008) and deductive (Thomas et al., 2015) thematic approaches were used and data were analyzed manually. Strategies (e.g., member checking and audit trail) were applied throughout the study development, implementation, and evaluation processes to enhance data trustworthiness (Lincoln & Guba, 1985).
Discussion
This article presents a comprehensive methodological overview of the M2M randomized pilot trial, with a view to inform the development of future population-based PPA programs. To our knowledge, this is the first study to evaluate an established real-world physical activity prescription model augmented with a supportive coaching adjunct grounded in a MI-via-CALC framework.
The integration of structured activity coaching represents a unique feature of the M2M design. Traditionally, MI-via-CALC is delivered weekly within behavioral interventions (e.g., Goddard & Morrow, 2015; Mantler et al., 2010; Pearson et al., 2013). While such consistency has been shown to promote meaningful behavior change, participants often report an abrupt sense of loss when intervention support ends (Newnham-Kanas et al., 2008). To mitigate this and enhance feelings of autonomy and competence, key determinants of sustained behavior change (Sheeran et al., 2021), the M2M study applied a stepwise coaching schedule. Participants received 6 weekly sessions followed by three biweekly sessions, a structure intended to promote gradual independence and foster internalized motivation over time.
It is noteworthy that this research was conducted entirely during the COVID-19 pandemic using remote platforms, an approach recognized as accessible, flexible, and cost-effective for promoting behavior change (Jiang et al., 2019; Salwen-Deremer et al., 2020). Moreover, because online interventions can reach larger audiences, the scalability potential of this model is high (Jiang et al., 2019; Salwen-Deremer et al., 2020). Similarly, delivering motivational interviewing and Co-Active coaching in this format, methods often inaccessible to those who might benefit most, offers a promising and democratizing strategy to expand the reach of such evidence-based behavior change supports. Findings from this pilot will help refine data collection methods, recruitment logistics, and fidelity procedures essential for future successful and cost-effective implementation. Given the ongoing decline in physical activity and concurrent rise in chronic disease among Canadians, the M2M study represents a timely and necessary step toward developing scalable, theory-driven approaches to improve population health through coaching.
Footnotes
Acknowledgments
We gratefully acknowledge Jeff Tareta (RxTGA Executive Director), Lisa Dare (RxTGA Board Member), The Monarch SystemTM Inc., Kayla Waddington (RxTGA Research Assistant), as well as our study participants.
Ethical Considerations
The ethical approval was received from the Lakehead University Research Ethics Board (#1469087).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Provincial funding via Prescription to Get Active.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.