
Abstract
Introduction
Urinary tract obstruction (UTO) is a common clinical problem of which there are many potential causes. The aim of this feature article is to explore the role of ultrasound in diagnosing UTO, during guided interventional procedures and the potential procedural complications.
Conclusion
Ultrasound plays a unique role in the planning and active stages of intervention with the provision of dynamic imaging which is crucial for providing safe and effective patient management.
Introduction
Urinary tract obstruction (UTO) is a common pathology that can be detected using different imaging modalities such as computed tomography (CT), magnetic resonance imaging (MRI) and ultrasound (US). US is cheap, free of ionising radiation and widely available in low to high economy countries. The US examination is often the first imaging test performed to detect evidence of UTO. It may be done at the point of care (POC) or in the imaging department by medical and non-medical healthcare practitioners. After diagnosis of UTO, US is used to provide image-guidance during interventional procedures aimed at relieving the obstruction. The aim of this feature article is to explore the role of US in diagnosing UTO, in guided interventional procedures and the potential procedural complications.
Diagnosis of urinary tract obstruction
Obstructive uropathy is a term used to describe either complete or partial obstruction of the urinary tract. Potential causes of native kidney obstruction are numerous and may be congenital or acquired, benign or malignant and can occur in children or adults. Obstruction can be either unilateral or bilateral depending on the type and site of pathology with abnormalities either proximal to, or at the level of, the vesico-ureteric junction (VUJ) tending to cause unilateral obstruction and distal abnormalities causing bilateral obstruction. 1 US, intravenous urography (IVU), CT, MR urography and nuclear medicine renography can all be used to good effect in determining the level of obstruction. With regard to US, colour Doppler can be used to assess ureteric jets within the bladder and help to increase confidence in whether obstruction is present or not.2,3 An absent ureteric jet suggests complete obstruction proximally on the ipsilateral side. In cases of incomplete obstruction, the obstructed side will show reduced relative jet frequency (RJF), the number of ureteric jets observed over a given time period, compared to the contralateral side. If normal ureteric jets are observed bilaterally in a known hydronephrotic patient then it implies obstruction distal to the ureters. One study showed that RJF <0.25 had a sensitivity of 87% and a specificity of 96% for detection of unilateral UTO. 2 Dependent on the severity and acuity of obstruction, permanent damage can be induced in both the affected collecting system and renal parenchyma and may necessitate urgent intervention. 1 Parenchymal damage occurs due to the dilated collecting system causing back-pressure into the renal microvasculature and thereby reducing renal perfusion. Doppler US imaging can be used to aid diagnosis with a raised resistive index in renal interlobar arteries (>0.7) suggesting UTO. 4
Grading of hydronephrosis is often controversial due to issues with intra- and interobserver reliability. 5 The Society of Fetal Urology grading system was originally designed for use in neonates and infants but is now also used in adults.
According to this system, severity of hydronephrosis is graded as follows:
6
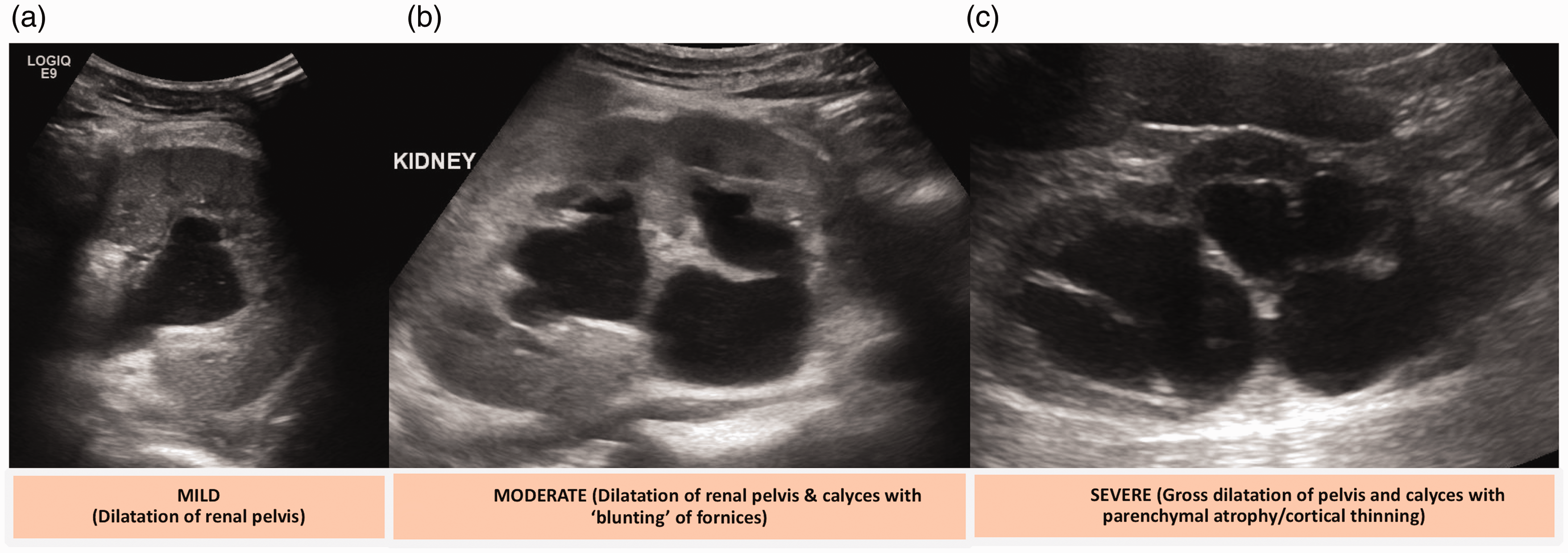
0 – no dilatation. 1 (mild) – dilatation of the renal pelvis without calyceal dilatation (Figure 1(a)).
(a) Mild hydronephrosis. (b) Moderate hydronephrosis. (c) Severe hydronephrosis. 2 (mild) – dilatation of the renal pelvis and calyces with preservation of the pelvicalyceal pattern and no parenchymal atrophy. 3 (moderate) – dilatation of the renal pelvis and calyces with blunting of the fornices and flattening of the papillae (Figure 1(b)). Mild cortical thinning may be seen. 4 (severe) – gross dilatation of the renal pelvis and calyces, which appear ballooned with loss of borders between the renal pelvis and calyces. Parenchymal atrophy in the form of cortical thinning is seen (Figure 1(c)).
It is important to recognise hydronephrosis does not always relate to an obstructed system and can be mimicked by other entities. Detecting these cases can avoid unnecessary intervention. It is common for hydronephrosis to be picked up on antenatal scans and persist into childhood. Often, however, this is idiopathic and occurs without true mechanical obstruction. Tc-99m-MAG3 renography is often employed to confirm or exclude obstruction in children and can also quantify relative renal function. 7 Mimics of hydronephrosis include congenital megacaliectasis, extrarenal pelvis, and renal cystic disease.
Ultrasound-guided interventional procedures
Safety in intervention
During any interventional procedure, patient safety is paramount and must be considered pre-procedure, intra-procedure and post-procedure.
Pre-procedure
Patient consent. Obtaining both written and verbal consent is essential prior to any interventional procedure. Not only does this allow the patient to understand the intended procedure and any complications that may arise, it presents an opportunity to correct any misunderstandings about the intended procedure/site.
Fasting
Patients do not need to be fasted unless intravenous (IV) sedation is planned.
Checklist
The completion of a pre-procedure checklist is required before any type of invasive procedure. The Royal College of Radiologists (RCR) offers guidance on this stating checklist should be developed locally to ensure they are relevant and proportionate to the procedures carried out at a particular site. 8 In many cases, the checklists are adapted from the World Health Organisation (WHO) Surgical Safety Checklist. 9
Contraindications
The contraindications for procedures will vary depending on the indication and the procedure itself. In the case of intervention related to obstructive uropathy, there are no ‘absolute’ contraindications but the following would usually be considered as a relative contraindication:
10
Coagulation disorder – International normalised ratio (INR) >1.4, platelets <50 × 10
9
/L. Severe hyperkalaemia or metabolic acidosis – potassium >6.5 mmol/L. When patients are turned prone there is inevitably a degree of respiratory compromise, which can precipitate worsening acidaemia and thereby increase the risk of cardiac arrhythmia or arrest. Terminal illness with imminent death.
Antibiotics
Routine pre-procedural antibiotic prophylaxis is recommended for all urinary interventions; given they represent, at best, clean-contaminated procedures.
11
The following factors increase the risk of post-procedural infection and such patients are more likely to benefit from pre-procedure prophylaxis:
Clinical signs/symptoms of infection Indwelling catheters/stents Urinary tract calculi Uro-enteric anastomosis Prior uro-intervention.
12
Usually, prophylaxis takes the form of a single dose of a broad-spectrum antibiotic which should be guided by local antimicrobial guidelines. The efficacy of prophylaxis is greatest when given within 1 hour of the procedure commencing. 12 If the patient is already receiving a course of appropriate antibiotics, there may be no need for further prophylaxis.
Review previous imaging
Relevant prior imaging should be reviewed, usually in the form of US, CT or fluoroscopic images. This allows confirmation of the side of procedure and any anatomical features that warrant consideration, e.g. retrorenal bowel.
Intra-procedure
Sterility
To reduce the risk of procedural infection, sterile conditions should be maintained. This includes the use of sterile personal protective equipment (PPE) by the practitioner, skin cleaning, sterile drape and sterile covers for the US transdcuer and console. All other equipment is single use and sterile.
Patient monitoring
The patient should have their vital signs monitored throughout the procedure including: blood pressure, heart rate and oxygen saturation. 13
Analgesia
Local anaesthetic is used (described further below). Conscious IV sedation may be utilised depending on patient’s comfort levels and preference. Systemic analgesia may be employed on a case-by-case basis e.g. IV Fentanyl. 13
Post-procedure
Patients are advised to have flat bed rest for a minimum of 4 to 6 hours post-procedure, during which their vital signs are monitored regularly. This helps to minimise the risk of bleeding (see complications). If nephrostomy tubes are required long term, they are listed for a routine exchange at three-month intervals reducing risk of blockage. 14
Intervention in malignant and benign disease
Percutaneous nephrostomy
Indications
UTO or renal failure due to intrinsic or extrinsic ureteral compression or VUJ/bladder mass/compression Pyonephrosis Urinary leak/fistula Access prior to further intervention
Seldinger technique
PCN is performed with a Seldinger technique under a combination of US and fluoroscopic guidance. 14 Patient positioning varies with anatomy and indication but usually they will either be prone or a tilted supine position (with the affected side raised).
US-guidance is used when making the initial puncture into the renal collecting system. Ideally, a longitudinal view of the kidney should be obtained to allow assessment of the degree of dilatation and selection of an appropriate puncture site and target calyx (Figure 2(a)).
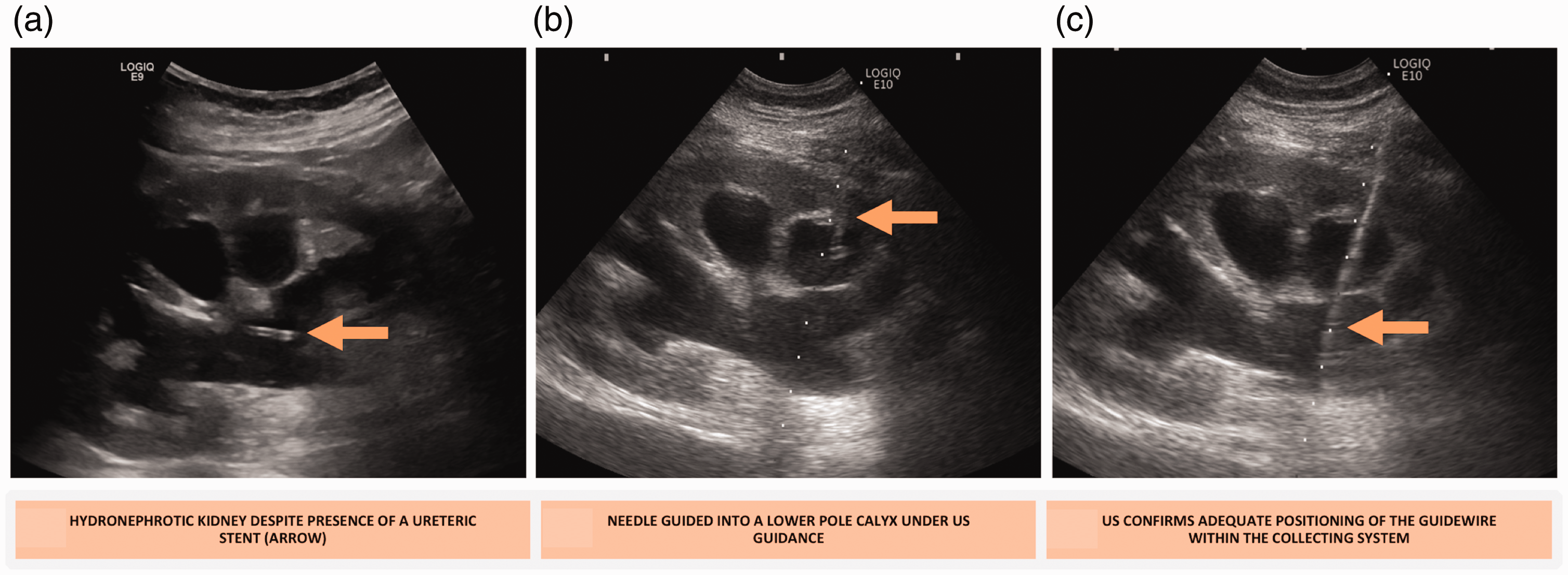
(a) Ultrasound hydronephrotic kidney. (b) Ultrasound needle access. (c) Ultrasound guidewire visualisation.
When simple drainage is required, a lower pole calyx is usually chosen due to ease of access and its location away from other structures including liver, spleen, diaphragms and pleura. Use of an US transducer needle guide may help with entry site visualisation and is routinely used in our centre. This approach is favoured as it can take advantage of Brodel’s avascular plane, which helps minimise vascular injury. 14 The plane is located at the junction of the anterior two-thirds and posterior one-third of the renal parenchyma and is created by the division of the renal artery into major dorsal and ventral branches forming a relatively avascular region.
Once the preferred calyx is identified, the skin is anaesthetised (usually 1% lidocaine) and a small scalpel incision is made. US guidance can then be used to instil local anaesthetic along the tract and principally adjacent to the renal capsule. Now the renal puncture is made. A 22 G or 20-G needle is guided with US to the renal capsule with the patient in gentle respiration. Once the target calyx is aligned with the needle (usually at end inspiration/expiration), the needle is promptly advanced into the collecting system (Figure 2(b)). Successful puncture is confirmed if urine can be aspirated. 14
Contrast solution is injected with the intention of opacifying the collecting system. If successful puncture is confirmed, the US transducer can be put aside (unless required as a troubleshooting tool) and fluoroscopy becomes the main imaging modality.
Once access to the collecting system has been gained, a guidewire can be passed through the needle and into the renal pelvis under fluoroscopy (Figure 3(a)). While holding the guidewire in place, the introducer needle can be removed over the wire. Serial tract dilatation with fascial dilators over the wire is now required before the catheter can be inserted. The angle of dilator insertion must match the angle of the wire to avoid kinking it.
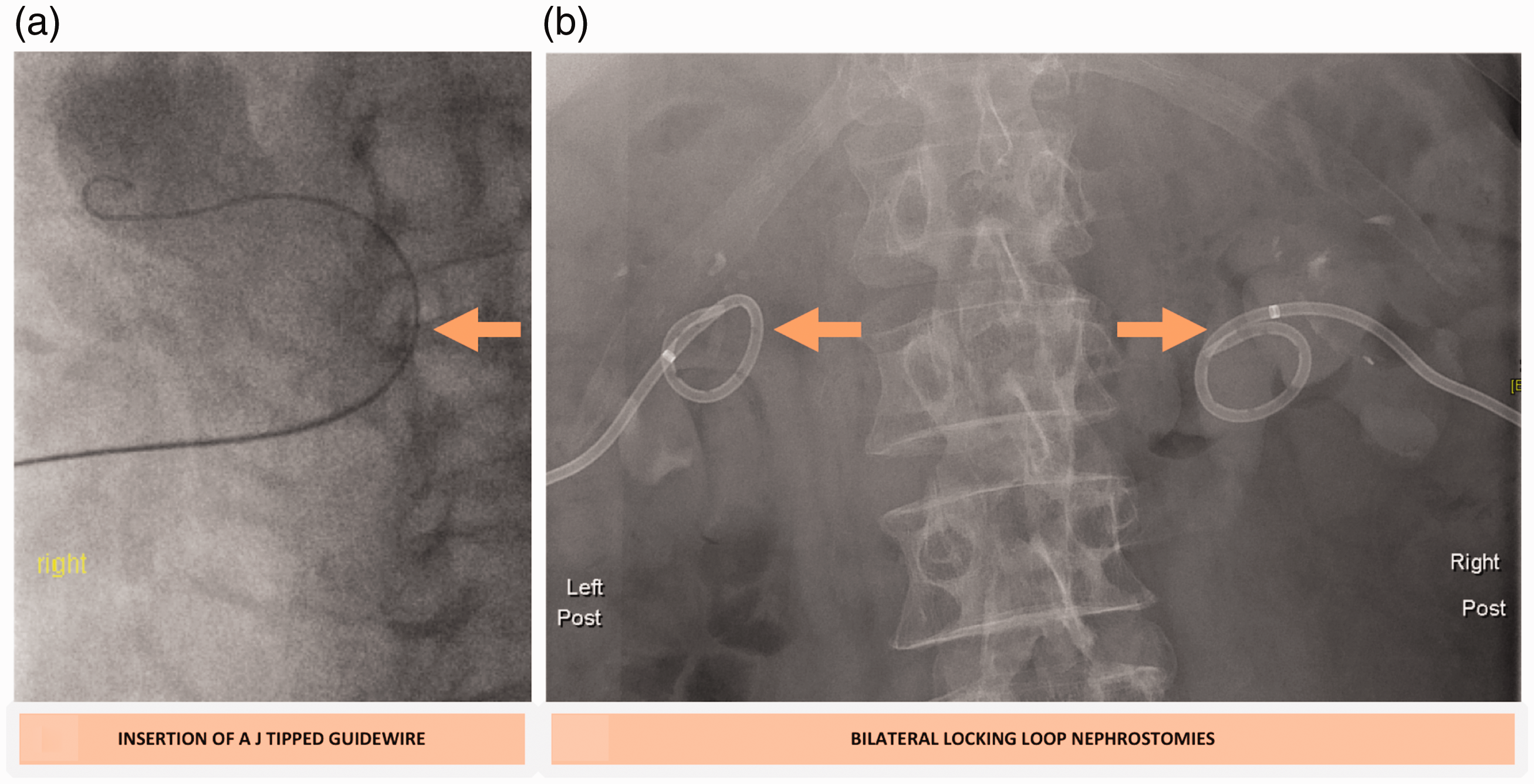
(a) Fluoroscopy guidewire visualisation. (b) Fluoroscopy nephrostomies.
In the case of simple hydronephrosis (rather than pyonephrosis), an 8.5 Fr catheter is typically used in our centre. The catheter contains either a metal or plastic stiffener to support its passage through the soft tissues. Some catheter designs have a locking loop system which can now be deployed and are preferred to non-locking systems (Figure 3(b)). 15 The tube is secured in place either with retention sutures or a special adhesive dressing.
Less commonly, US can be used in its entirety (Figure 2(c)). This has the advantage of being free from ionising radiation and may therefore be useful in pregnant women and children. US also enables nephrostomies to be performed portably in settings such as the intensive care unit (ICU) and operating theatre. Disadvantages of an US-only technique include inability to visualise the catheter and fine wire manipulations and difficulty when working with minimally/non-dilated systems.
Antegrade ureteric stenting
Antegrade ureteric stenting may be successful even when retrograde cystoscopic stenting has failed and is therefore a useful technique for dealing with longer term UTO. Consequently, it is the most common extension of the PCN.
The initial technique is identical to that of a PCN puncture, although an interpolar or upper pole calyx may be preferred as this provides a more direct route for a guidewire via the renal pelvis and into the ureter. Once access to the collecting system is gained, a safety wire is inserted with the tip in the renal pelvis. A ureteric access catheter can be inserted over the safety wire before exchanging to a hydrophilic wire. A hydrophilic wire can be safely navigated down the ureter – closely followed by the catheter. The aim is to pass the point of obstruction and reach the urinary bladder. The plastic catheter will remain in the bladder, while the hydrophilic wire is exchanged for a stiff wire – such as an Amplatz wire. A ureteric stent can be deployed over the stiff wire so that its distal tip lies in the bladder and proximal tip within the renal pelvis (Figure 4(a) to (c)). These are known as double ‘J’ or double ‘pigtail’ stents as they have coiled ends both proximally and distally – thereby reducing the risk of migration (Figure 4(a) and (b)). 16
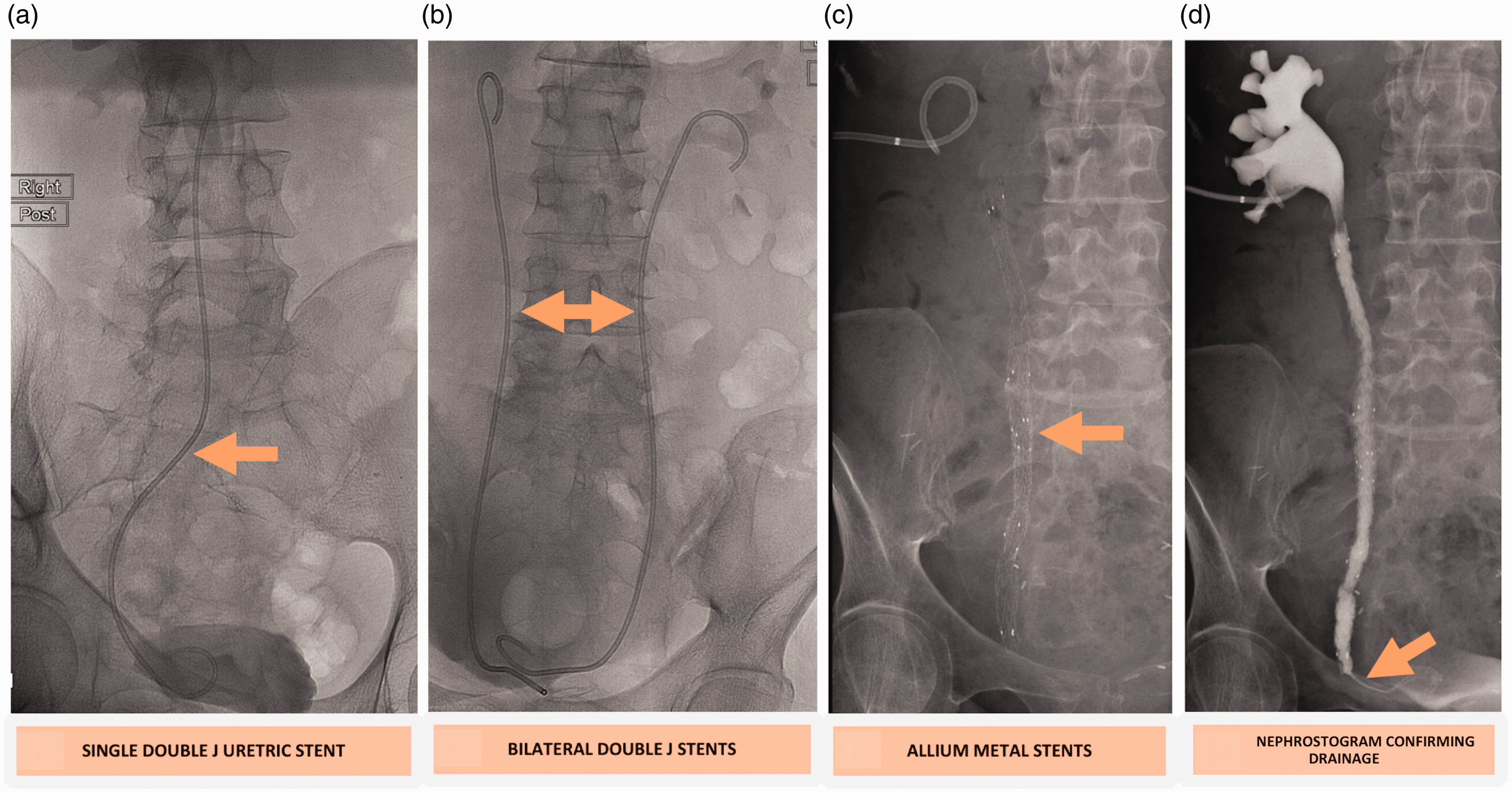
(a) Fluoroscopy single ureteric stent. (b) Fluoroscopy double ureteric stents. (c) Fluoroscopy metallic stents. (d) Fluoroscopy metallic stents drainage.
If ureteric passage is attempted unsuccessfully at the time of PCN, the procedure may be revisited after five to seven days of drainage. This can allow the degree of mucosal oedema to reduce and increases the probability of subsequent, successful ureteric passage.
Intervention in septic patients
In cases of pyonephrosis, larger catheter sizes in the order of 12–14 Fr may be required to adequately drain the increased-viscosity urine and reduce the risk of catheter occlusion. Care should be taken not to over-pressurise the collecting system when injecting contrast, as it increases the risk of bacteraemia and septic shock. Pure, rather than diluted contrast can therefore be used to reduce the volume required and as a rule of thumb, the volume of contrast injected should not exceed the volume of urine aspirated. 15
Interventions along with urologists
Percutaneous nephrolithotomy
This is a surgical procedure designed to remove large renal calculi and is often performed as a joint procedure under radiology and urology. It is indicated for calculi too large for treatment by extracorporeal shockwave lithotripsy, namely staghorn calculi or calculi >2 cm diameter (Figure 5). Initial access is usually performed by an ultrasound practitioner (radiologist or interventional sonographer) or urologist trained in image-guided access. Ideally, access to the collecting system is via the calyx containing the stone. Exceptions include an upper pole stone (risk of pneumothorax if targeting upper pole) or pelvic stone where a mid/lower pole calyx may be preferred. In the case of low-lying or pelvic kidneys, it may be relatively safe to target the upper pole. 17
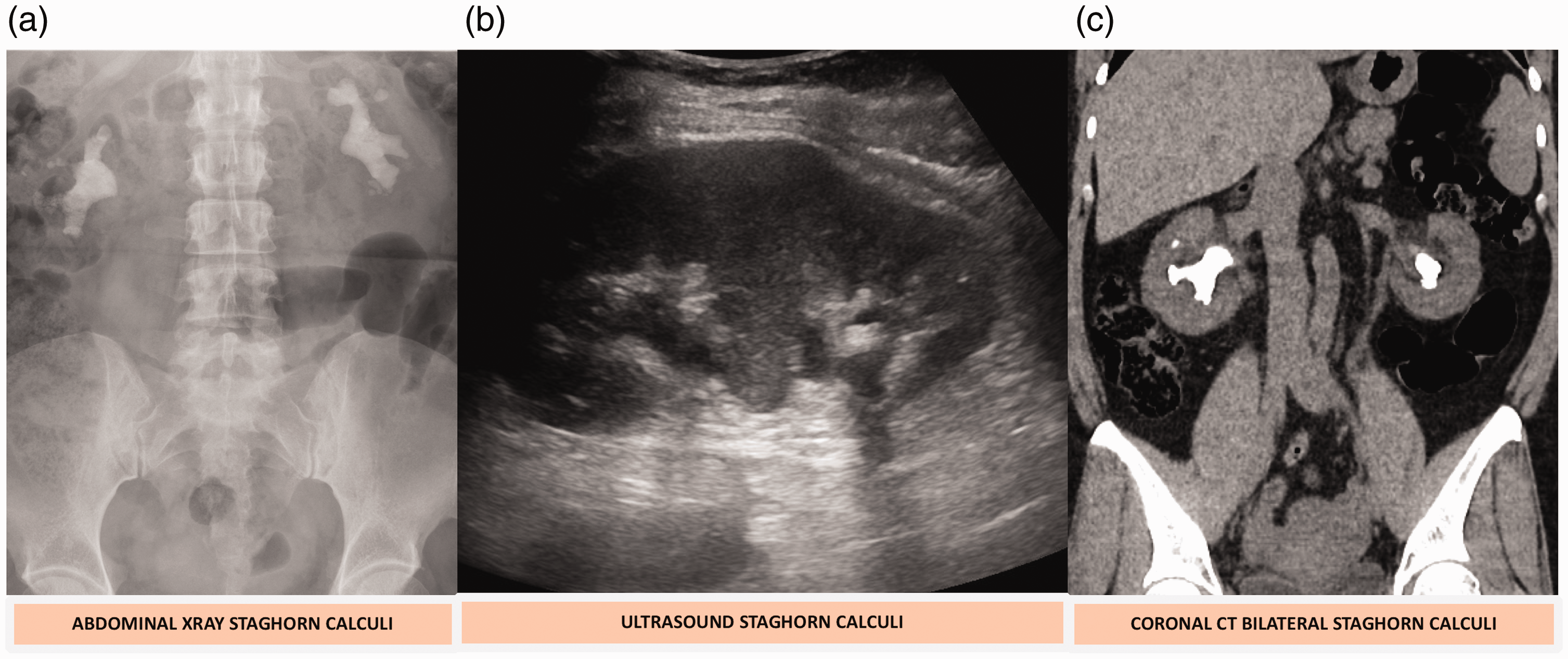
(a) Abdominal X-ray calculi. (b) US calculi. (c) CT calculi.
Often, these patients do not have a dilated collecting system, limiting the use of US. A urologist will place a ureteric catheter cystoscopically (into the bladder) which can be used to induce iatrogenic dilatation of the calyces to assist US-guided access. This step can also be performed fluoroscopically by opacifying the calyces with contrast medium via the ureteric catheter. The ultrasound practitioner then gains percutaneous renal access using fluoroscopic guidance. 17
Due to the increased intra-renal manipulation in PCNL, two wires are normally used. One as a ‘safety wire’ inserted into the ureter and one as a ‘working wire’ in the collecting system. In the case of positional disruption of the working wire due to manipulation, renal access is maintained by the safety wire. Larger tracts (up to 30 Fr) are needed for PCNL and therefore dilatation is performed using either co-axial dilators or balloon dilation systems. Following the procedure, a large calibre catheter (24–30 Fr) is placed in the tract to both drain the kidney and tamponade the tract. These catheters are usually removed one to seven days’ post-procedure dependent on the indication. Advances in technology have meant smaller tracts can now be made to accommodate the smaller nephroscopes reducing morbidity associated with large tracts. 18
Standard and detour extra-anatomical stents
EAS are an option in both malignant and benign causes of obstruction and can be a viable long-term management solution. They may be considered in patients too frail to undergo reconstructive surgery or who have failed PCN drainage or ureteric stenting. 19 Renal access is gained via PCN – the calibre of these stents can be up to 29 Fr and therefore large bore access is required. The proximal end of the stent is secured in the collecting system. The urologist or radiologist then tunnels the stent subcutaneously down the anterior abdominal wall and inserts and sutures it into the bladder via cystostomy (usually suprapubically).
Placement of these stents is not recommended in close proximity to a tumour as seeding along the stent can occur. They are therefore contraindicated in patients with active bladder malignancy or tumours invading the bladder. 20 A benefit of these stents is that they generally only require exchange every 12 months.
Intervention in paediatrics
Cases of UTO in young children will usually be identified with a combination of US and micturating cystography. This combination can usually define the cause of obstruction. Following this, renal scintigraphy, e.g. Tc-99m-MAG3 renogram can illustrate the degree of obstruction and guide surgical management.
The most common causes of paediatric UTO are pelviureteric junction (PUJ)-type obstruction (whether congenital or post-surgical), stone disease, clot or extrinsic compression from an abdominal/pelvic mass. 21 An emergency indication for PCN, as in adults, is pyonephrosis. Severe vesicoureteric reflux and posterior urethral valves are less commonly seen but are paediatric-specific.
Percutaneous nephrostomy
PCN insertion in children is mostly used as a bridge to more definitive surgical management. Patient preparation is similar to in adults with optimisation of coagulation profile and routine antibiotic prophylaxis in many institutions. Although in very young children, general anaesthesia may be required, the majority of cases can be undertaken with conscious sedation and local anaesthetic. The patient is positioned prone or semi-prone and Seldinger technique would be the preferred access method. 22
Paediatric nephrostomy catheter sizes range from 5 to 10 Fr and the size used will depend on patient size and indication. As in adults, patients with pyonephrosis or urinary sediment may require larger catheter sizes.
The complications encountered in children are the same as those in adults. However, any planned procedure should be performed expediently to prevent issues with tube maintenance. 22
Percutaneous nephrolithotomy
PCNL is performed under general anaesthesia in an operating theatre usually by the Urology and Radiology team. Access as described is required prior to PCNL and is similar in both paediatric and adult age groups. A larger tract is however required – up to 18–28 Fr to facilitate nephroscopic access. As in adults, either a PCN or ureteric stent may be left in situ following the procedure to tamponade the tract and allow free drainage of the collecting system.
Antegrade ureteric stenting
The majority of paediatric ureteric stents are done in a retrograde fashion cystoscopically by urologists. Where this fails or is deemed inappropriate, antegrade stenting can be performed by an ultrasound practitioner. 23 Indications include failed pyeloplasty, postoperative ureteric stenosis, ureteric injury, ureteric fistula and extrinsic compression by tumour. The technical factors involved in ureteric stenting in the paediatric population are similar to in adults. However, in younger children, variable length silicone stents may be used due to variability in ureteric length. In teenagers this is less of an issue and fixed length stents will usually be sufficient. 16
Imaging for trouble shooting to aid intervention
The typical way to check for nephrostomy position and patency is with a fluoroscopic nephrostogram (Figures 4(d) and 6(a) and (b)). This involves injection of a contrast agent down the nephrostomy catheter. If the catheter is patent and correctly sited, the renal collecting system will opacify with contrast. If the tube has been dislodged, a contrast spill into the retroperitoneum may be demonstrated. If the tube is blocked, then neither aspiration of urine nor injection of contrast will be possible. If the nephrostomy catheter has only recently come out of the kidney, it is usually possible to navigate a guidewire back into the collecting system with fluoroscopic guidance (Figure 6(c)). This provides access for the deployment of a new PCN (Figure 6(d)).
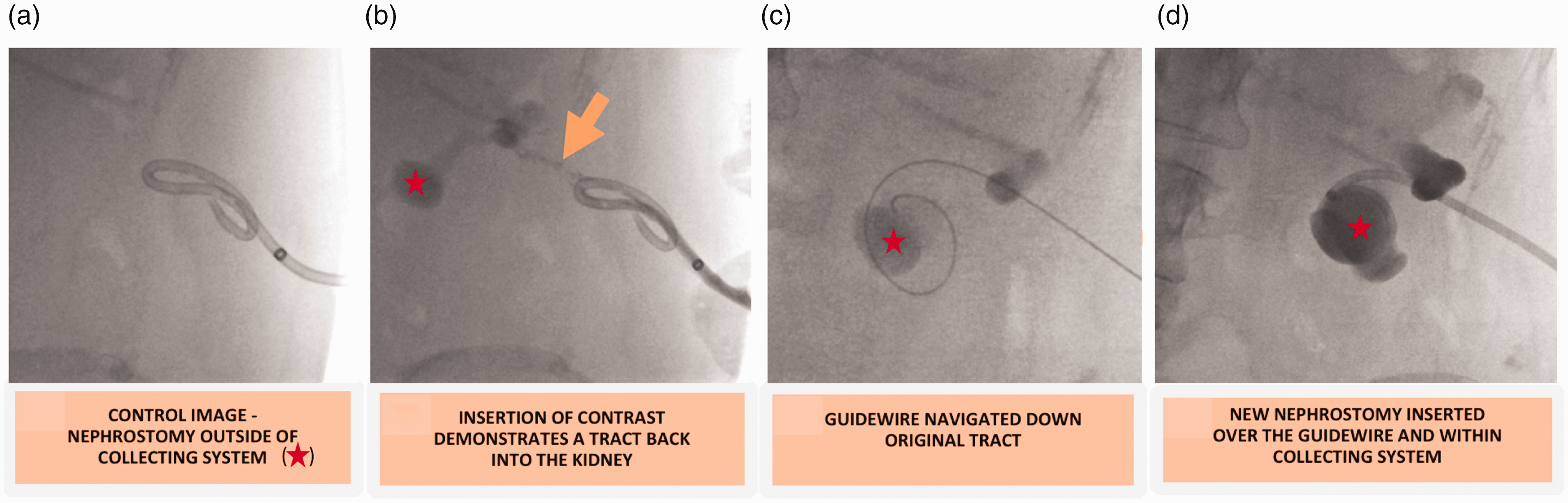
(a) Fluoroscopy 1. (b) Fluoroscopy 2. (c) Fluoroscopy 3. (d) Fluoroscopy 4.
More recently, there has been interest in contrast-enhanced US (CEUS) nephrostograms as an alternative method. Several papers have shown that CEUS nephrostograms are comparable to fluoroscopic nephrostograms in detecting catheter placement and ureteric patency. They also have the benefit of being free from ionising radiation and the ability to be performed portably if required.24–26
In the case of suspected ureteric stent occlusion, there are various options. In the first instance, a B-mode US may demonstrate hydronephrosis and thereby imply stent occlusion. If a covering nephrostomy has been left in situ, then a nephrostogram can be performed – this can identify if the stent has migrated and whether contrast is able to drain into the bladder.
A plain radiograph KUB (kidneys, ureters and bladder) series is able to show stent migration; however, a CT, even unenhanced as a KUB is able to show both hydronephrosis and stent positioning/migration as well as other possible complications but comes with an increased radiation burden.
Procedural complications
As with any interventional procedure, complications can and do occur. The frequency and type of complication will depend on the procedure undertaken.
Percutaneous nephrostomy complications 27
Transient haematuria
Occurs in most patients following renal puncture in the first 48–72 hours and on its own is of limited concern.
Severe bleeding
Approximately 1–3% of cases may require transfusion or further intervention. If bleeding is noticed during the procedure, it can usually be controlled by tamponading the tract with a nephrostomy catheter or, if required, a balloon dilatation catheter. If severe bleeding develops post procedure, it may require angiographic evaluation and sometimes selective embolisation.
Infection/sepsis
The major concern being systemic sepsis and shock. Risk factors are discussed in pre-procedural section. Preceding pyonephrosis/high pressure system is the main risk with the prevalence of septic complications reported as high as 25%. 28 Care should be taken to minimise the volume of contrast administered.
Perirenal collection/urinoma
With puncture of the urinary system being a requirement of PCN, there runs a risk that urine may leak around the nephrostomy tube. If the collection becomes large enough then further intervention may be required in the form of percutaneous ultrasound-guided drainage.
Damage to local structures
Viscera most likely to be damaged are the liver, spleen, colon (especially if retrorenal) and pleura. Damage to the pleura may result in a pneumothorax and is more likely when using an intercostal or upper calyceal approach.
Stent complications 15
Most of the complications associated with PCN insertion apply here but stent specific complications are as follows:
Urinary tract infection
This can either present as a short- or long-term complication. In patients with known UTI, stenting should be delayed to first allow treatment with targeted antimicrobials. As with any foreign body, stents are susceptible to microbial colonisation, which will ultimately require exchange or removal of the stent.
Malposition
Incorrect deployment/position despite use of fluoroscopy. Stents of insufficient length may deploy outside of the renal pelvis or the bladder. Stents, particularly stiffer ones, can penetrate the renal parenchyma, renal pelvis or ureter resulting in urinomas or haematomas.
Migration
Stents can migrate either proximally or distally – the latter being more common due to peristalsis. The main issue is loss of its decompressive effect and subsequent reaccumulation of hydroureteronephrosis. In order to reduce this risk, all fully internalised stents have double ‘J’ or ‘pigtail’ configuration.
Occlusion
Blockage of the stent and/or nephrostomy tube may occur. In the short term, this may be secondary to clots or increased urine viscosity (pus) in an infected system. Late causes include stones, encrustation of urinary deposits or extrinsic compression (often tumour). To reduce the risk of encrustation, good hydration, aggressive treatment of urine infection and regular exchanges are required.
Forgotten stent
Adequate documentation and regular follow-up are required to ensure stents are not forgotten. Risk of complications increase the longer the stent remains in situ.
Conclusion
US is an integral imaging modality throughout the management pathway of a patient with UTO. It is often utilised as a first-line test in detection. It plays a unique role in the planning and active stages of intervention with the provision of dynamic imaging – crucial for providing safe and effective management. It is a widely available resource which is both cost effective and safe, helping to avoid the use of ionising radiation in the patient population.
Supplemental Material
sj-pdf-1-ult-10.1177_1742271X211049495 - Supplemental material for Urinary tract obstruction: Ultrasound-guided intervention
Supplemental material, sj-pdf-1-ult-10.1177_1742271X211049495 for Urinary tract obstruction: Ultrasound-guided intervention by Alexander Lory, Christopher Stubbs, Stephen Wolstenhulme and Atif Khan in Ultrasound
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethics Approval
Not applicable.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
AK.
Contributorship
AL – Performed literature search, drafted the manuscript and implemented suggested revisions.
CS – Reviewed and assisted with drafting of the manuscript. Implemented revisions, sourced and formatted images for the included figures.
SW – Advised on revisions to the manuscript both in terms of text and formatting.
AK – Conceptualised and provided a framework for the manuscript. Advised on suggested revisions. Aided in sourcing images for the included figures.
Acknowledgements
Not applicable.