
Abstract
Introduction
Percutaneous thermal ablation of inconspicuous lesions can be challenging. Fusion ultrasound (FUS) allows the use of previously performed diagnostic imaging like computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET–CT) to localise hepatocellular carcinoma (HCC) for treatment. This paper illustrates FUS case studies of pre-, intra- and post-ablation imaging of inconspicuous HCC, supplemented by use of contrast-enhanced ultrasound (CEUS).
Method
Four prospective cases during September 2014 to October 2018, with HCC amenable to ablation, which were poorly identified on ultrasound, underwent FUS. FUS pre-screening was scheduled within three months of the previous CT or MRI, and between one to four weeks prior to the scheduled ablation date. Post-ablation imaging with FUS was performed between four to six weeks to coincide with their routine follow-up CT or MRI.
Findings
There were potential benefits observed in the cases with combined techniques of FUS and CEUS for limiting circumstances such as heat sink effect, multiple lesions targeting, inconspicuous lesion detection and pre-ablation technical feasibility assessment.
Discussion
The combined use of FUS and CEUS improves tumour visibility, increases operator imaging confidence and reduces heat sink effect during percutaneous thermal ablation.
Conclusion
FUS imaging is helpful in targeting poor conspicuity lesions that cannot be detected on grey-scale ultrasound. It facilitates in ensuring optimal treatment of hepatic lesions for improvement of patient prognosis and follow-up imaging.
Introduction
Percutaneous thermal ablation is a widely accepted treatment for small (below 3 cm) hepatocellular carcinoma (HCC) with results comparable to surgical resection. 1 Ultrasound (US) is the preferred modality for needle guidance during percutaneous thermal ablation as it allows real-time lesion tracking despite hepatic respiratory movement, oblique scanning planes to avoid vital structures and is radiation-free. However, many hepatic tumours are inconspicuous on conventional grey-scale US, which can make targeting difficult. Fusion of real-time US images to the previously performed computed tomography (CT), magnetic resonance imaging (MRI) and positron emission tomography (PET–CT) can improve lesion localisation and may be supplemented by use of contrast-enhanced ultrasound (CEUS).2,3
Fusion ultrasound (FUS) technology pairs an electromagnetic field transmitter with a transducer-mounted sensor.4,5 This allows direct overlay of previously performed diagnostic imaging (e.g. contrast-enhanced CT, MRI or PET–CT) with real-time US images to allow detection and documentation of lesions. 3 This is especially beneficial for targeting lesions which are ill-defined on real-time grey-scale US, during US-guided ablation.
US contrast agents utilise microbubble technology which enhances a lesion’s visibility in proportion to its blood supply. These mimic the effect of CT or MRI contrast without the known adverse effects including contrast nephropathy and nephrogenic systemic fibrosis, respectively. Small lesions may also be better delineated compared to CT or MRI given the higher spatial resolution of US. 6 However, US’s small field of view makes it difficult to evaluate the whole liver with each contrast bolus, and the examination must be focussed onto a small area each time. This narrow field of view can be pre-selected with fusion technology, allowing synergy between these modalities.
We hypothesised that FUS-guided ablation combined with CEUS will have higher ablation success rate and improved targeting of lesions, leading to better patient outcomes. Also, we believe that follow-up imaging using this combination would improve the accuracy of detection for residual tumour around the ablation zone.5,7
We present our experience with combined FUS and CEUS in pre-, intra- and post-ablation imaging of inconspicuous HCC nodules in a prospective cohort of patients from a single tertiary centre.
Materials and methods
Our institutional review board approved this prospective study, and written informed consent was obtained from all patients prior to enrolment. Patients presented to the institution from September 2014 to October 2018 with a diagnosis of HCC amenable to percutaneous ablation and were offered pre-ablation imaging with FUS and SonoVue™ (Bracco, Milan, Italy) CEUS. This imaging was scheduled within three months of the most recent CT or MRI and between one to four weeks prior to the scheduled intervention. The lesions discovered not to be visible on US during the pre-screening examination were considered inconspicuous. Post-ablation imaging with FUS and CEUS was done between four to six weeks to coincide with their routine follow-up CT or MRI. This allowed direct comparison of ablation adequacy between the two modalities.
We used a Canon Aplio 500 (Canon Medical Systems Corporation, Tochigi, Japan) US system for all cases. Baseline CT/MRI investigations were downloaded in Digital Imaging and Communications in Medicine (DICOM)-3 format into the US-system hard disk, and the most appropriate sequences were pre-selected for image fusion. Three standard anatomical reference points were used for all patients: proximal superior mesenteric artery, bifurcation of right or left portal vein (depending on tumour location) and confluence of right or middle hepatic vein and inferior vena cava.8–10 In some cases, after this initial fusion, a lesion representing the tumour could be identified on grey-scale imaging. In these cases, a fourth reference point was taken at this lesion. Fusion was done on suspended inspiration, similar to the CT/MRI acquisition (supplementary video).
CEUS was used during pre- and post-ablation scans to localise and identify inconspicuous lesions on grey-scale US. All operators had more than five years of experience in clinical US.
Results
Case 1
A 67-year-old male with hepatitis-B related cirrhosis, prior transhepatic portosystemic shunt (TIPS) for acute variceal bleeding and two previous ablations for HCC, now presented with a suspicious 0.4 cm arterially-enhancing lesion at a segment-8 ablation margin on CT imaging. This margin recurrence was inconspicuous on grey-scale US. FUS using arterial phase of the axial CT slices allowed selection of the region of interest. CEUS demonstrated rapid wash-in and washout of contrast into the nodule. A Covidien Cool-tip™ Single Electrode Kit E Series 15 cm ablation probe (Medtronic Ltd, Watford, UK) was confidently advanced into the lesion, and ablation was performed successfully. CT imaging immediately following lesion ablation showed a satisfactory ablation zone. Follow-up triphasic CT performed three months post-ablation showed stable complete response (Figure 1).
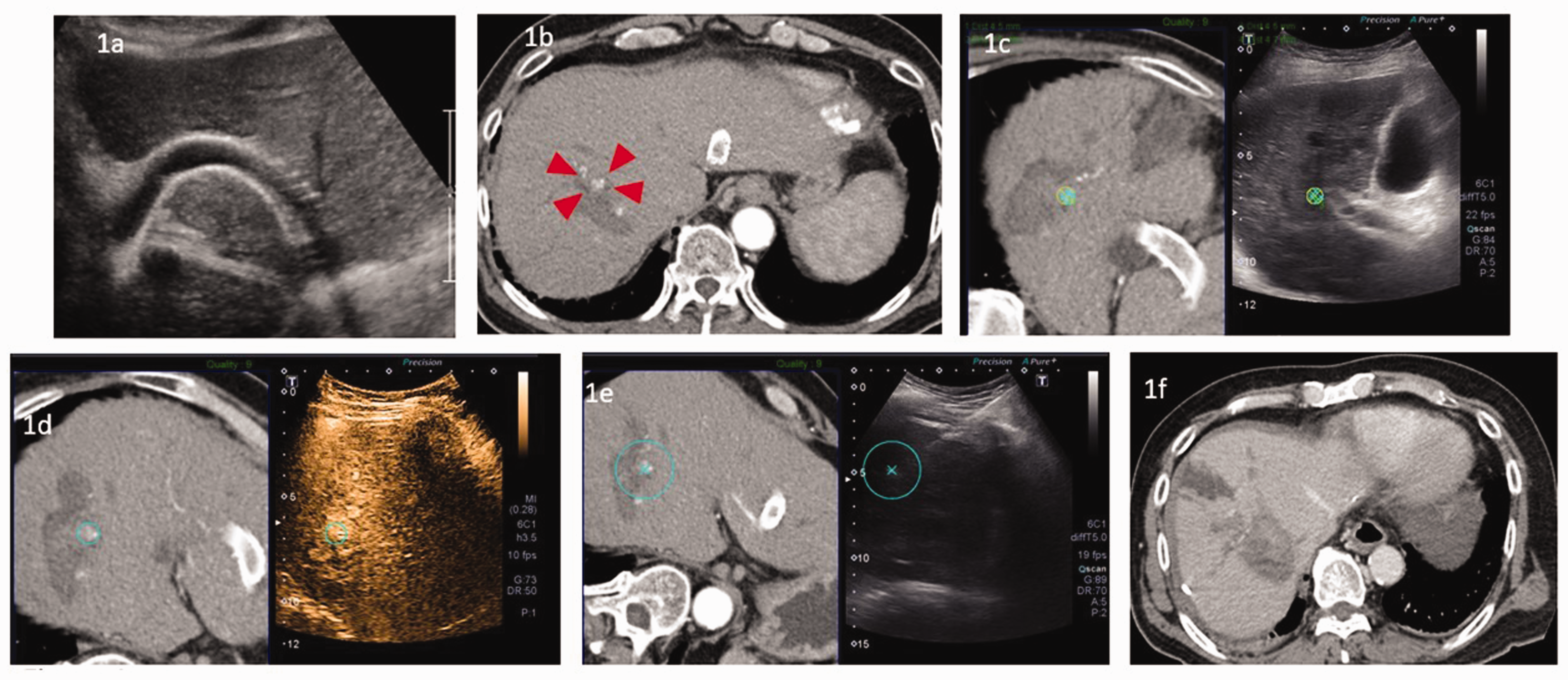
A 67-year-old male had history of hepatitis-B and transhepatic portosystemic shunt (TIPS) insertion in December 2012. (a) Echogenic TIPS seen in the left lobe, (b) 4-mm focus of arterial enhancement (red arrows) at inferomedial aspect of the liver which was indeterminate in nature, (c) fusion ultrasound (FUS) showed targeted lesion appearing vague on grey-scale US, (d) FUS during contrast-enhanced US displayed arterial enhancement, (e) radiofrequency ablation was performed with fusion US guidance and (f) post-ablation axial CT confirmed successful ablation.
Case 2
A 56-year-old male hepatitis-B carrier with prior ablation of a segment 8 HCC presented with two new lesions in segments 5 and 8. On Primovist-enhanced MRI, both lesions displayed avid arterial enhancement and interval growth compared to a prior MRI scan. Both lesions were inconspicuous on grey-scale US and were ablated using Cool-tip™ radiofrequency ablation (RFA) guided by a combination of FUS and CEUS. On immediate post-ablation CEUS, residual enhancement at the segment 5 lesion margin was suspicious for residual tumour (due to heat sink effect from an adjacent vessel). Additional ablation using FUS guidance at the margin was thus performed with satisfactory results (Figure 2). Follow-up MRI one month after ablation confirmed complete ablation of both lesions.
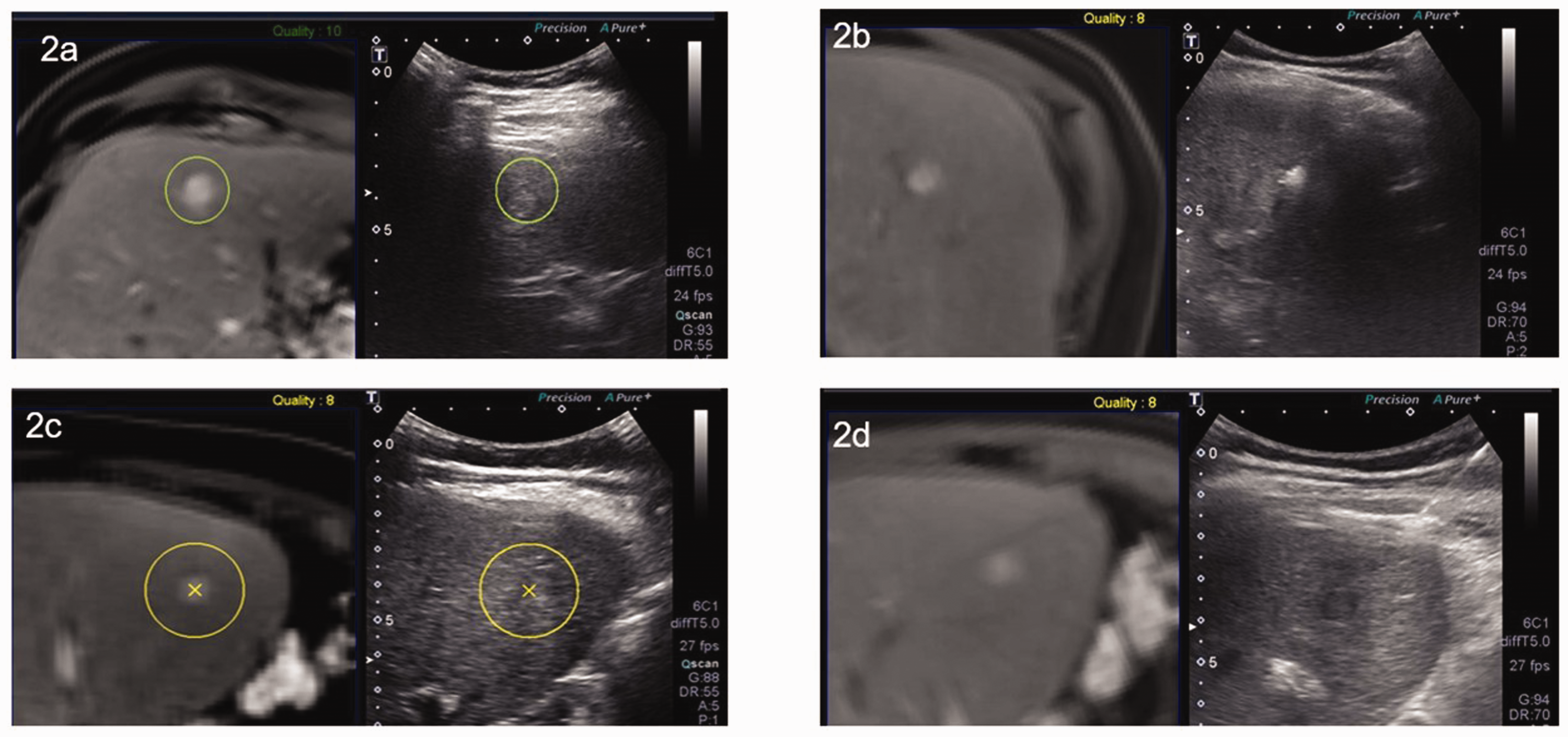
A 56-year-old male hepatitis-B carrier presented with segments 5 and 8 lesion detected on magnetic resonance imaging, fat-suppressed T1-weighted images performed fusion ultrasound (FUS). (a) Segment 8/5 lesion localised on FUS, (b) segment 8/5 lesion FUS during radiofrequency ablation treatment, (c) segment 5 lesion localised on FUS and (d) segment 5 lesion fusion during radiofrequency ablation treatment.
Case 3
An 80-year-old male had history of segment 8/5 wedge-resection for hepatitis-B related HCC, 10 years prior to his current presentation. Primovist-enhanced MRI showed a new 2.2 cm HCC adjacent to the surgical resection margin, and percutaneous ablation was recommended by our multi-disciplinary tumour board (MDTB). The tumour, which was initially inconspicuous on grey-scale US, manifested as an ill-defined lesion at the resection margin after image fusion. Hypervascularity within the lesion was confirmed on CEUS.
Further confirmation was attained during the ablation procedure by performing a non-contrast CT scan after placing a 22G Chiba needle at the medial margin of lesion. Ablation was performed uneventfully using an Emprint™ 15G microwave ablation probe. Post-procedure CEUS was performed showing no suspicious nodular enhancement at the ablation zone extending beyond the lesion. Two months after ablation, contrast-enhanced MRI and fusion CEUS both confirmed successful ablation with no residual tumour (Figure 3).
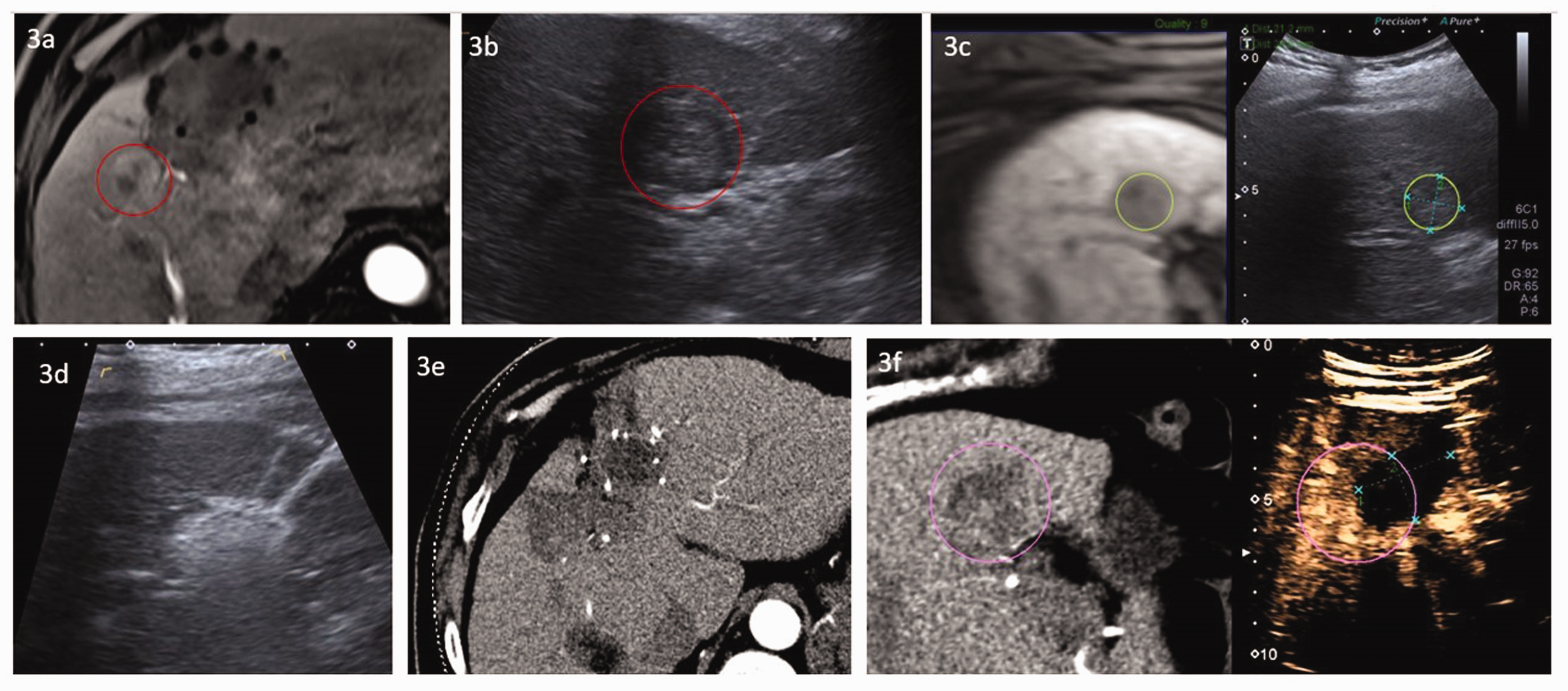
An 80-year-old male had history of fatty liver and prior resection of hepatocellular carcinoma. (a) T1-weighted MRI using 10 ml post-contrast Primovist adjacent to the surgical resection margin showed a predominantly hypervascular lesion in segment 8/5, with delayed washout and capsular enhancement measuring 2.2 cm, (b) lesion appears isoechoic and slightly vague on ultrasound (US), (c) fusion US was performed with MRI, (d) ablation needle directed to lesion with successful ablation, (e) satisfactory post-ablation changes shown on CT axial arterial phase and (f) satisfactory post-ablation changes shown on fusion US with CEUS, with no contrast uptake seen.
Case 4
A 75-year-old female presented with tumour recurrence in the remnant liver, within a year of a left lateral segmentectomy for hepatitis-B related HCC (Edmondson Grade 3). Primovist-enhanced MRI demonstrated a new T1-weighted hypointense 0.6 cm lesion at the border of segments 7 and 8 showing faint arterial enhancement becoming more prominent in the venous phase. This was determined by MDTB to represent recurrent HCC and recommended for percutaneous ablation. She was enrolled in the study as the lesion was not visible on initial grey-scale US. On FUS, a 0.9 × 0.7 cm ill-defined focus was noted at the segment 7/8 junction corresponding to the lesion seen on MRI.
CEUS following initial FUS demonstrated arterial enhancement and equivocal delayed washout. Covidien Cool-tip™ RFA was performed using real-time FUS monitoring. Post-ablation CEUS confirmed absence of residual enhancement. On two-month follow-up fusion CEUS, index tumour location was verified by using the pre-ablation MRI scan, and target size was adjusted according to the initial index tumour size. FUS on grey-scale showed the target marker to be within the ablated area. Corresponding two-month contrast-enhanced CT confirmed absence of enhancement, consistent with complete ablation of the lesion (Figure 4).
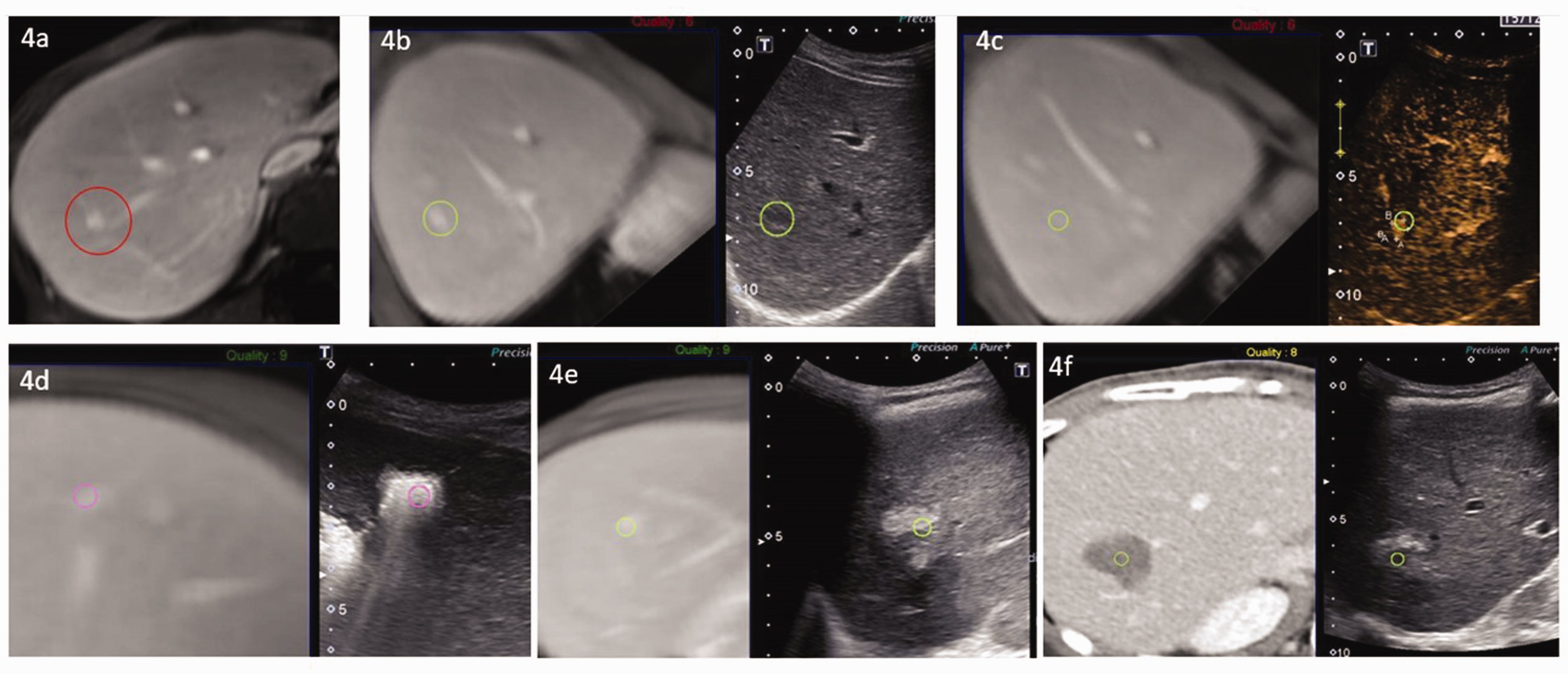
A 74-year-old female had history of hepatitis-B cirrhosis on Entecavir. (a) T1-weighted MRI with 6 ml of Primovist showed a 6-mm focus in segment 7/8 with faint arterial enhancement, (b) fusion ultrasound (FUS) targeted the area, where lesion was ill-defined on grey-scale US, (c) fusion and contrast-enhanced US, showed uptake on arterial phase, (d) lesion was successfully ablated with fusion US and (e) post-ablation follow-up of lesion with pre-ablation MRI was used as fusion US reference. Original lesion size was seen within the ablated area (f) post-contrast CT was used as reference for fusion and lesion was seen within the ablated area.
Discussion
Our study demonstrates that real-time FUS and CEUS improve tumour visibility and operators’ confidence in detecting inconspicuous hepatic lesions. Targeting of small lesions including those in difficult locations, e.g. adjacent to implanted hardware (TIPS stent) and previous ablation sites, is shown to be possible, with favourable outcomes. 11 FUS allows precision guidance and real-time monitoring of index tumour during ablation to ensure the ablation probe is seated at the correct location for the procedure. CEUS adds confidence for both lesion detection and complete ablation during the procedure. 12 When necessary, additional ablation can be performed for residual disease, without subjecting the patient to excessive radiation or iodinated contrast exposure.
We routinely perform ablation of small (<1 cm) lesions if they are classic HCC on imaging, patient has attributable risk factors for HCC and consensus is for ablation after MDTB discussion. The Asian Pacific Association of the Study of the Liver criteria is used for diagnosis of HCC. Based on local and regional best practice, highly suspicious lesions even smaller than 1 cm are routinely offered treatment, e.g. with percutaneous ablation.
Multiple lesion targeting can be facilitated by the Global Positioning System marker function of FUS. All lesions can be marked prior to commencement of ablation. This allows easy sequential identification of lesions for subsequent ablation despite artefacts generated from the ablation.
Heat sink effect may limit the efficacy of RFA when the index tumour is adjacent to large blood vessels.3,8,13 Additional ablations can be done along the vessel margin to reduce the chance of recurrence.14–16 Increasing total ablation time can also reduce the likelihood of heat sink effect.17,18 Combination of FUS and CEUS provides immediate confirmation of complete lesion ablation in this situation. If necessary, additional ablations can be done at the vessel margins, as shown in case 2.
FUS can also be used to mark out critical structures to be avoided during ablation.19,20 During real-time monitoring, this is valuable when snowstorm artefacts from the ablation zone reduce the visibility in the immediate vicinity. Other operators have similarly demonstrated high technical success rates for targeting inconspicuous lesions with real-time FUS guidance: ranging from 90% to 100%.2,10
There are several reasons why FUS is preferable to CT guidance in ablation. First, lesions are often not well seen on unenhanced CT. With contrast enhancement, the lesion is also visible only transiently; hence, it is not very easy to localise the moving target on CT fluoroscopy, especially for small lesions.
Second, critical structures, e.g. portal vein and hepatic arteries are also not well seen on unenhanced CT. Additionally, some lesion locations in the liver for ablation may be only millimetres away from the lung or heart.
Third, continuous CT fluoroscopy is avoided during needle advancement because of the significant radiation dose to the operator. Intermittent CT fluoroscopy is used only when there were risks involved to critical structures during needle advancement.
Last, we find US to be the most user-friendly imaging tool in providing real-time needle guidance. Having the prior CT, MRI or PET–CT image fusion with US gives added confidence to the operator.
The local control rate for tumours with transarterial chemoembolisation alone has been reported to be approximately 70%. 21 This also depends on technical factors including selectivity of injection and 3-D safety margin. Ablation, on the other hand, provides close to 100% local response if the lesion is targeted correctly. Fusion CEUS provides full-circle imaging confidence to the operator, from pre-ablation technical feasibility assessment and planning, real-time procedure-guidance and post-procedure confidence of ablation margins, and adds an extra layer of safety in all directions. 12
Limitations
This was a single-arm, single-centre study with a small number of patients. While the findings are illustrative of potential benefits, they cannot prove that the combination is superior to alternative targeting methods. US is an operator-dependent modality, and adoption by other centres would depend on availability of experienced staff, appropriate equipment and contrast agents. Further, all cases in this report involve HCCs which tend to show avid contrast enhancement. The application to relatively hypovascular lesions such as intrahepatic cholangiocarcinoma or colorectal metastases requires further study.
FUS technique has its limitations. First, rotational malalignment is common as the scan is usually done in held expiration or held inspiration, while US is typically done in shallow free breathing. There are rotational liver movements which can cause significant geographical errors. Small lesions can be missed, as other small pseudolesions in a cirrhotic liver can sometimes be confused for the target lesion, due to misalignment. Hence, repeat CEUS is an added safety measure to avoid missed lesions.
Second, the visibility of the liver can be severely impaired by prior surgery, small high-riding liver and presence of adjacent or internal air-containing structures. This can greatly limit fusion success.
Third, if reference imaging is not very recent, there can be significant changes in hepatic size and shape in the interim, especially in post-surgical cases. This can cause significant errors in FUS due to changes in geographical landmarks.
We routinely use FUS in almost all liver ablation cases within our institution, as CT guidance is challenging due to liver movement from respiration. FUS has been described for kidney and bone ablations; nonetheless, the results with CT guidance for these procedures are easier and more reliable.
Conclusion
Fusion CEUS imaging guidance potentially provides synergy and operator confidence in planning, executing and follow-up of hepatic ablation for small and inconspicuous HCC lesions even in challenging locations. Further work is needed to assess the cost-effectiveness of the combination compared to alternative targeting methods and its reliability in hypovascular lesions.
Footnotes
Acknowledgements
We would like to acknowledge Dr Richard Lo who assisted in reviewing recruited patients during the project, and Jedhrie Bautista Crudo for the supplementary file video edits. We would also like to acknowledge the support the ultrasound team in Singapore General Hospital.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by Department of Diagnostic Radiology, Singapore General Hospital.
Ethical Approval
The ethics committee of SingHealth Singapore approved this study (CIRB Ref No. 2014/032/C, revised CIRB Ref No. 2018/3111).
Guarantor
AMA
Contributorship
AMA and AG conceived the study concepts and design. AMA, SMDL and ODL researched literature. AMA was involved in study development and gaining ethical approval. AMA, SMDL, SMT, ODL, ASAR, CWT and AG were involved in patient recruitment. AMA wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.