
Abstract
Background:
Acute viral hepatitis A remains a significant public health concern.
Objective:
This study investigated the relationship between gallbladder wall pathology, liver stiffness measurements, controlled attenuation parameter, and biochemical markers in adult patients with acute viral hepatitis A.
Methods:
Overall, 42 patients with acute viral hepatitis A were studied over 3 months. Patients underwent ultrasound and transient elastography examinations. Gallbladder wall thickness was categorised into two groups: 3–10 mm (group A) and ⩾10 mm (group B).
Results:
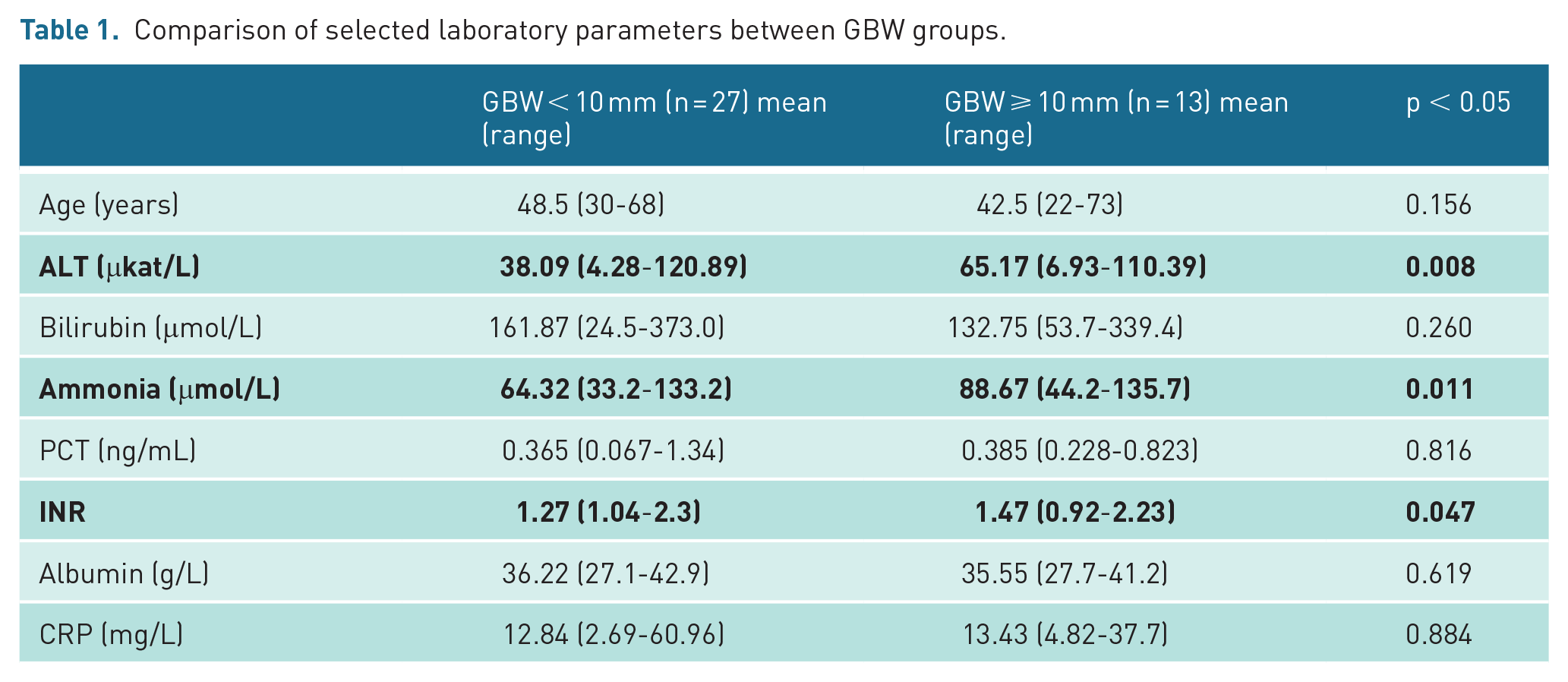
Gallbladder wall thickening was detected in 95% of patients. Stratification and fluid accumulation were present in 71% and 38% of patients, respectively. Gallbladder wall thickness ⩾10mm was significantly associated with stratification and fluid accumulation (p < 0.0001). Higher gallbladder wall thickness correlated with elevated alanine aminotransferase (p = 0.008), ammonia levels (p = 0.011), and international normalised ratio (p = 0.047). A positive correlation was observed between procalcitonin levels ⩾0.25 ng/mL and gallbladder wall thickness ⩾10 mm (p = 0.011). The controlled attenuation parameter values were significantly lower in patients with greater gallbladder wall thickness (p = 0.013), while liver stiffness measurement showed no correlation with gallbladder wall thickness.
Conclusion:
In acute viral hepatitis A, gallbladder wall thickening is almost a pathognomonic finding. Increased gallbladder wall thickness correlates with increased alanine aminotransferase, ammonia, international normalised ratio, and procalcitonin levels, highlighting its potential as a non-invasive marker of disease severity. Controlled attenuation parameter and liver stiffness measurement require cautious interpretation in acute inflammation. These findings support gallbladder wall assessment as a valuable tool in evaluating acute viral hepatitis A.
Keywords
Introduction
Millions of people acquire acute viral hepatitis A (VHA) each year, worldwide. An unfavorable trend persists, with VHA remaining prevalent in hyperendemic regions while emerging as a growing concern in areas with historically low endemicity. Global VHA cases increased by 13.90% from 139.54 million in 1990 to 158.94 million in 2019. 1
Over the past 2 years, Slovakia has experienced a resurgence of the VHA epidemic. This is occurring primarily in the region of eastern Slovakia, with focal points identified in communities of the minority Roma population characterised by low hygienic standards. From these focal points, VHA spreads further, affecting all groups of non-immune residents.
Studies show that a substantial proportion of patients with this infection have a thickened gallbladder wall (GBW) when examined with ultrasound (US). Other diseases associated with GBW thickening include acute cholecystitis, congestive heart failure, ascites, chronic renal failure, and hypoalbuminemia. Several hypotheses have been proposed to explain the mechanism of GBW thickening in patients with acute viral hepatitis.2,3
Transient elastography (TE) is a rapid, non-invasive, and reproducible method of measuring liver stiffness. Current evidence indicates that liver stiffness values, as measured by TE, undergo significant changes in response to hepatic inflammation. 4 TE has been shown to be a reasonable tool to quantify liver fibrosis in chronic liver diseases due to varied aetiology. However, several studies have indicated that liver stiffness measurement (LSM) values can be significantly influenced by major changes in aminotransferases level in patients with chronic viral hepatitis and that LSM is unreliable for diagnosing underlying liver fibrosis in patients with acute liver damage.5,6
Studies show that controlled attenuation parameter (CAP) is generally effective in detecting hepatic steatosis; however, its accuracy is reduced during periods of active inflammation. In this study, we also attempted to correlate CAP with GBW thickening. 7
Our study aims to understand the importance of a GBW pathology in patients with confirmed acute VHA and to correlate the significance of US signs with CAP, LSM values, and selected laboratory parameters.
Patients and methods
From November 2023 to February 2024, we have prospectively enrolled and evaluated patients with serologically confirmed acute VHA admitted to the Department of Infectology and Travel Medicine at the University Hospital in Kosice, Slovakia. Most patients were admitted due to jaundice, nausea, myalgias, and fever. Acute VHA was confirmed by enzyme-linked immunosorbent assay (ELISA) test, showing positivity in the immunoglobulin M assay. All patients also had positivity in the immunoglobulin G assay. Other concomitant aetiologies were excluded by examining all sera for viral hepatitis B, C, E, cytomegalovirus (CMV), Epstein-Barr virus (EBV), herpes simplex virus (HSV), and leptospirosis. None of the patients had a documented history of hepatotoxic substance exposure, including medications, alcohol, recreational drugs, or toxic mushrooms.
Patients under 18 years of age, those lost to follow-up (at least two examinations necessary during the study), individuals with chronic liver disease, ascites, and heart failure, and those with a history of cholecystectomy were excluded from the study. The ethics committee of our hospital approved the study protocol, and all patients provided written informed consent before entering the study (no. 235/EK/2023).
GBW thickness measurements were consistently performed by the same sonographer throughout the study to eliminate examiner bias. Based on previous studies, we considered the GBW to be thickened in fasting subjects whenever its width exceeded 3mm. 8 Each patient had their first US examination and TE conducted the next morning after admission to the hospital. Follow-up US and TE assessments were conducted weekly until the patients were discharged from the hospital. Following discharge, follow-up examinations and laboratory tests were scheduled for 2-week intervals.
US examinations were conducted using a USS–HS5NL3M US scanner (Samsung, North Korea) equipped with a 5-MHz convex probe. Examinations were conducted after a fasting period of at least 4 hours. We consistently aimed to measure the thickness in the middle of the gallbladder’s longitudinal diameter with the patient in the right lateral decubitus position. During each examination, three measurements were performed, and the median value was calculated. We evaluated the thickness, presence of fluid accumulation, and separation of wall layers (stratification). Following the US examination, we measured the CAP and liver stiffness using the FibroScan 502 touch (Echosens, Paris, France). We performed 10 TE measurements during each patient’s examination, and all final values had to correlate with a maximum discrepancy of up to 25%. All probes (M and XL size) were properly calibrated and up-to-date at the time of the examination. Normal value of liver stiffness and CAP was considered to be below 7 kPa and 238 dB/m, respectively.
Patients were categorised into two groups: those with GBW thickening of 3–10 mm (group A) and those with GBW thickening ⩾10 mm (group B), according to previous studies. 9
The laboratory test results included aspartate aminotransferase (AST), alanine transaminase (ALT), total bilirubin, direct bilirubin, total protein, albumin, ammonia, alkaline phosphatase (ALP), gamma-glutamyl transpeptidase (GMT), C-reactive protein (CRP), interleukin-6 (IL-6), and International Normalised Ratio (INR). Procalcitonin (PCT) levels were measured in all patients included in the study. Based on their PCT levels, patients were divided into two groups: those with PCT levels below 0.25 ng/mL and those with PCT levels equal to or above 0.25 ng/mL. The laboratory parameters were collected on the same day as the US and TE examinations.
Statistical analyses were conducted using t-tests and Pearson’s correlation coefficients to determine relationships between variables such as GBW thickness, laboratory parameters, CAP, and LSM values. Regression analyses were also performed to evaluate the association of GBW pathology with clinical and biochemical markers, ensuring robust evaluation of significance and trends. To enhance data visualisation and interpretation, boxplots and graphs were employed, illustrating the distribution and relationships of the analysed variables.
Results
During the 3-month period, we have hospitalised a total of 64 patients (34 women, 30 men) with serologically confirmed acute VHA. We excluded four patients who had a history of cholecystectomy, ten patients for whom there was no consistent follow-up of US, TE examination, or liver function testing, and eight patients who had chronic liver disease or gallbladder pathology (stones, polyps). In total, 42 consecutive patients (22 women, 20 men) with a median age of 47.1 years (range = 22–73 years) were enrolled in the study (Figure 1). The median age of men was 45 years (range = 30–68 years), and the median age of women was 49.1 years (range = 22–73 years). All patients had at least two examinations (US and TE) performed. Thirty patients (71.4%) underwent three examinations, while 17 patients (40.4%) had four or more examinations performed. The median duration of symptoms prior to the initial examination was 6.7 days (range = 2–14 days). Out of 42 patients, 40 patients exhibited GBW thickening (95%), 30 patients showed GBW stratification (71%), and 16 patients exhibited GBW fluid accumulation (38%).
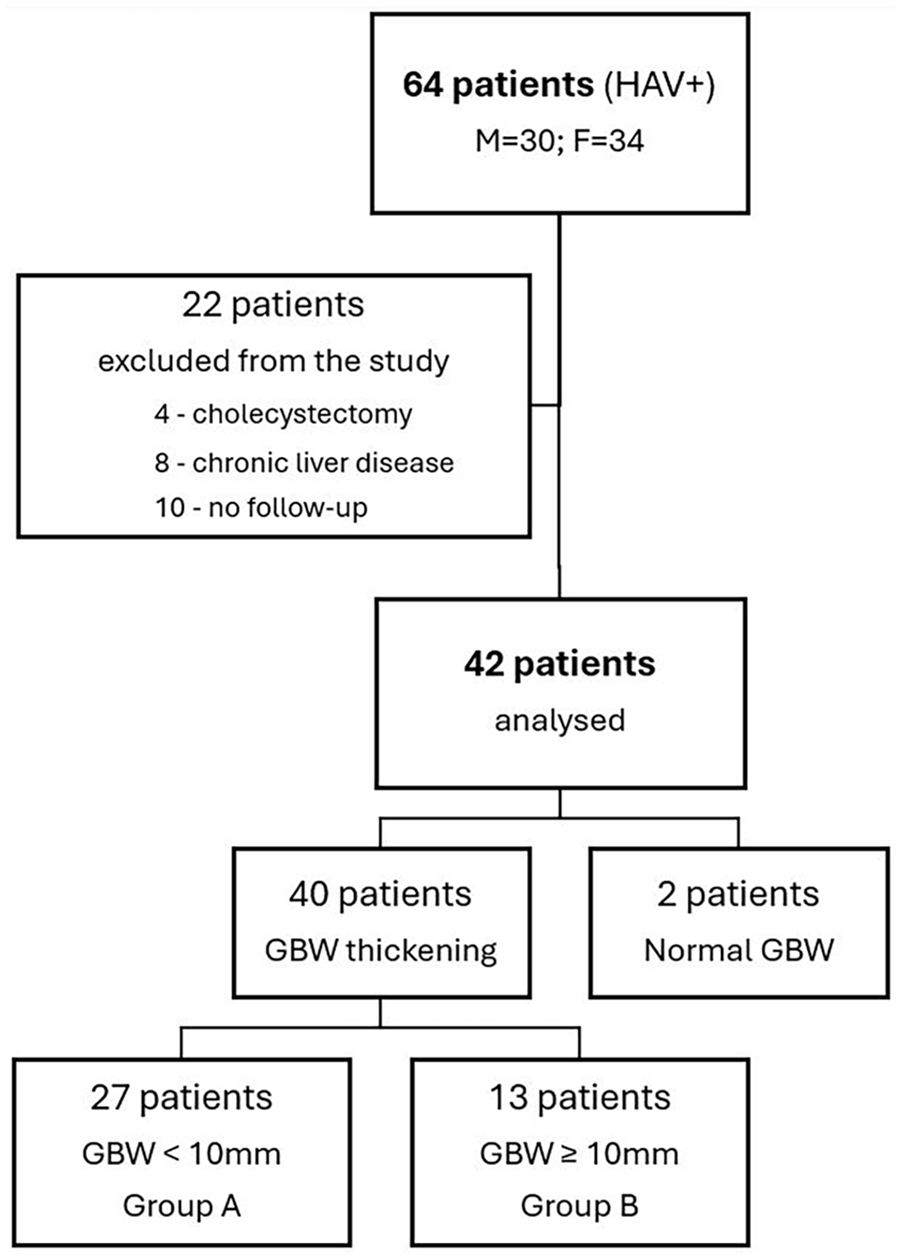
Flowchart of patient selection and classification based on gallbladder wall characteristics.
In group A (n = 27), the median GBW thickening was 6.6 mm (range = 3.6–9.6). In group B (n = 13), the median GBW thickening was 12.6 mm (range = 10–16). Comparison between GBW groups and measured variables is shown in Table 1.
Comparison of selected laboratory parameters between GBW groups.
Correlation of GBW groups, fluid accumulation, and biochemical parameters
The boxplot below shows the distribution of ALT levels across the two GBW groups (Figure 2). The t-test results reveal a t-statistic of −2.782 and a p-value of 0.008 indicating a statistically significant difference in ALT levels between the two GBW groups. Specifically, this suggests that significantly higher ALT levels were observed in patients with GBW thickness above 10 mm.
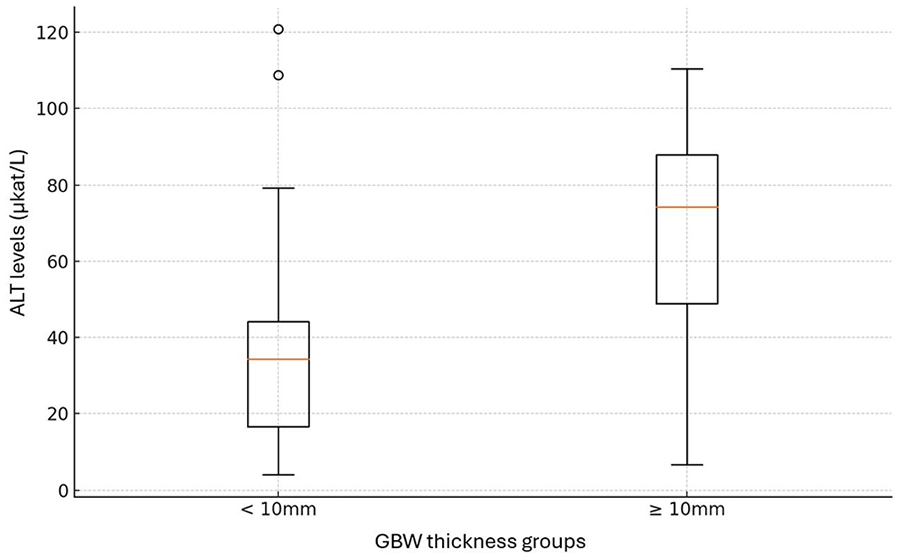
Comparison of ALT levels between GBW thickness groups.
The analysis of the relationship between initial ALT levels and GBW thickness values revealed a positive correlation, with a correlation coefficient r = 0.392, and p-value of 0.012.
The same results were obtained when assessing ALT levels and GBW fluid accumulation, revealing a positive correlation, with a correlation coefficient of 0.38 and p-value of 0.015. These results show that the severity of liver inflammation, measured by ALT levels, correlates significantly with GBW thickness and fluid accumulation.
To further explore the dynamics of ALT levels in relation to GBW thickness over time, we analysed the correlation between GBW measurements and ALT levels at various stages of patient monitoring. The study demonstrates significant correlations between GBW measurements and corresponding ALT levels at various stages of patient monitoring. Initially, a moderate positive correlation (r = 0.392; p = 0.012) was observed between the first GBW exam and first ALT measurement, indicating that higher GBW measurements are associated with elevated ALT levels. This positive relationship strengthens significantly during the second visit (r = 0.529; p = 0.0005), suggesting a strong link between increasing GBW and ALT levels during early follow-up. By the third visit, the correlation diminishes to a weak-to-moderate positive relationship (r = 0.292; p = 0.148) and loses statistical significance, potentially reflecting variability in patient responses or partial resolution of the underlying condition. Notably, a strong negative correlation was observed during the fourth visit (r = −0.677; p = 0.045), indicating that GBW thickness and ALT levels decrease at different rates, with ALT levels resolving more rapidly than GBW thickness (Figure 3). The observed trends in LSM values over multiple visits indicate a gradual decline, reflecting a slower resolution of liver stiffness compared to the rapid decrease seen in ALT levels and GBW thickness (Figure 4).
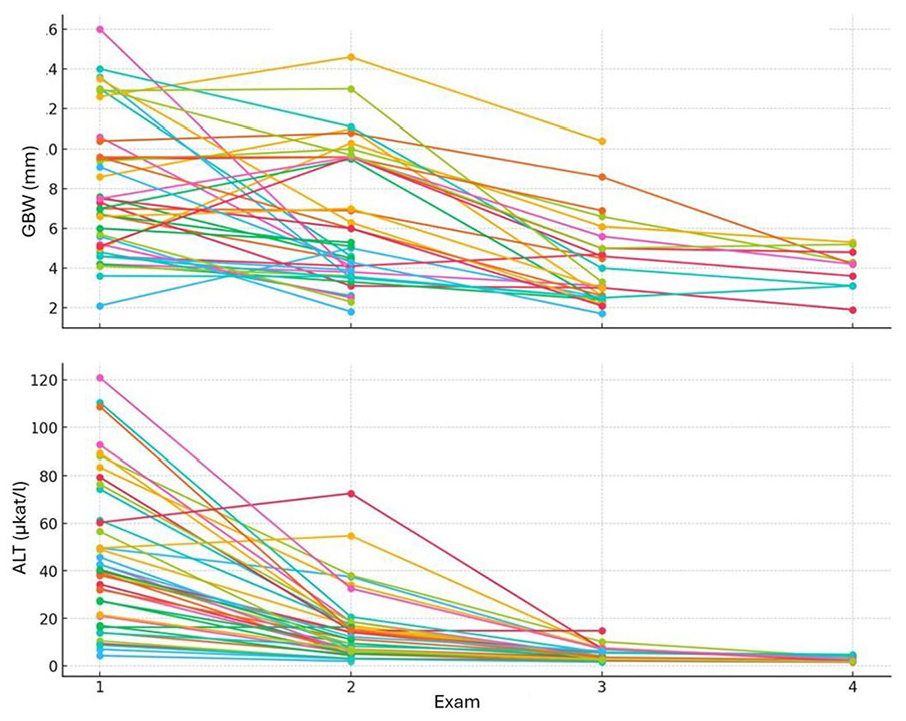
Changes in GBW thickness and ALT levels during successive exams.
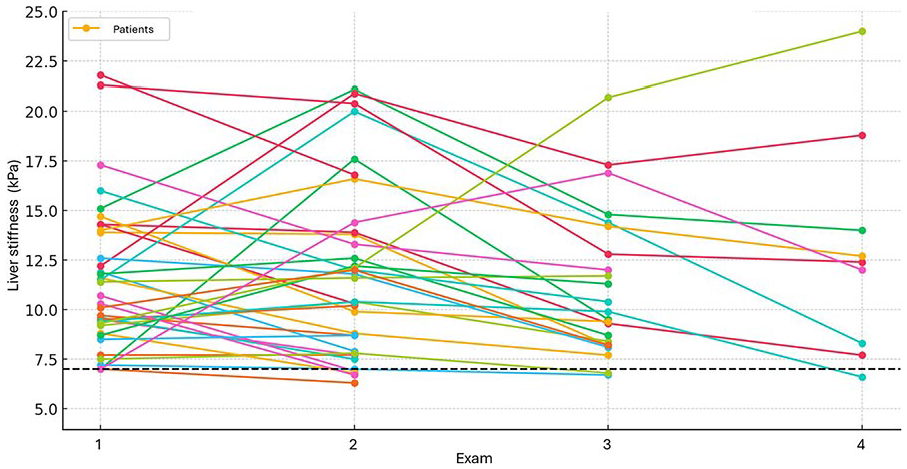
Liver Stiffness Measurements during successive exams.
Our investigation also revealed the association of GBW thickness and ammonia levels. The analysis demonstrated a positive correlation between GBW thickness and ammonia levels, yielding a correlation coefficient r = 0.40. This correlation achieved statistical significance, with a p-value of 0.011, indicating a robust association (Figure 5).
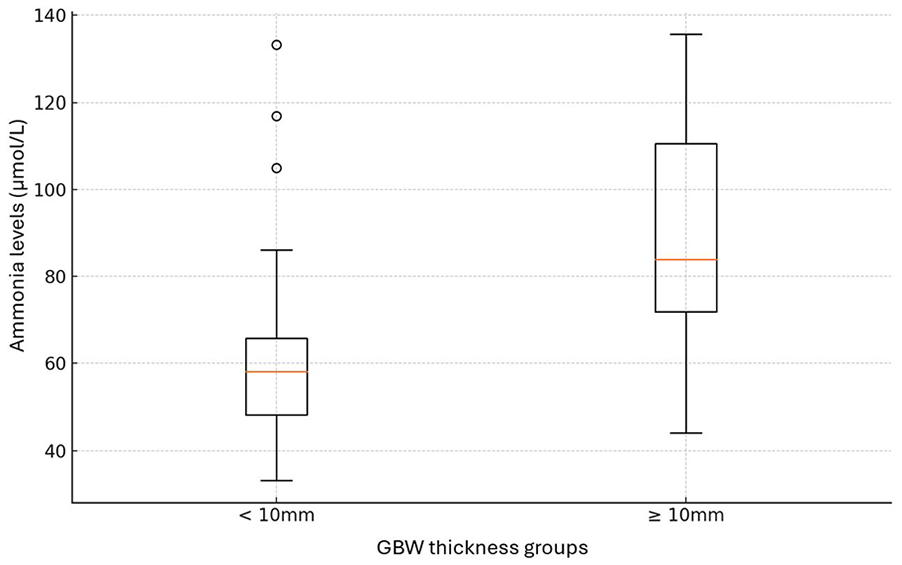
Comparison of ammonia levels between GBW thickness groups.
This was also true when analysing patients with GBW fluid accumulation and ammonia levels. The correlation coefficient was r = 0.368. This relationship is statistically significant with a p-value of approximately 0.0196, suggesting that as the amount of fluid in the GBW increases, ammonia levels also tend to increase.
The analysis revealed a positive correlation between the two GBW groups and initial INR levels (r = 0.316; p = 0.047). Patients with GBW greater than 10 mm exhibit significantly higher INR levels compared to those with GBW less than 10 mm (Figure 6).
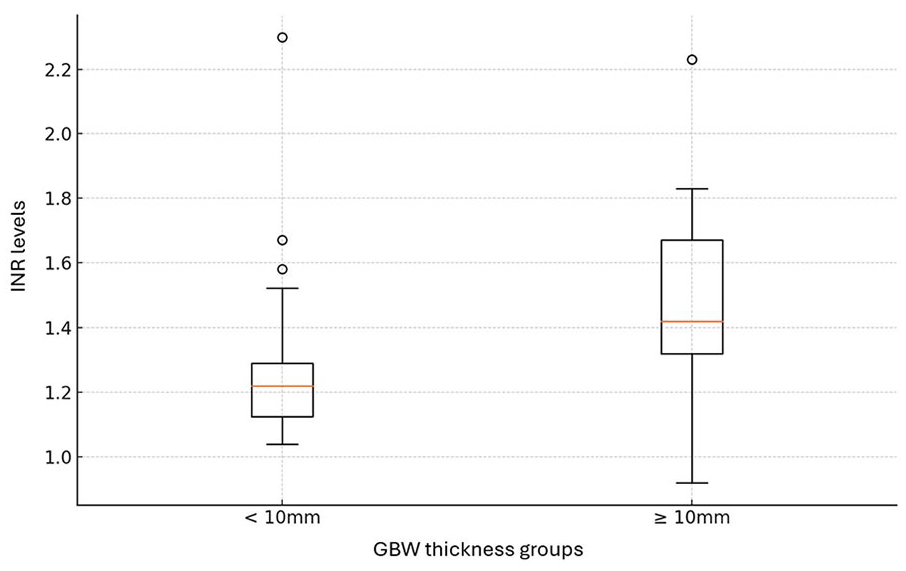
Comparison of INR levels between GBW thickness groups.
In the analysis of GBW groups using a predefined PCT threshold of 0.25 ng/mL, significant correlations were observed, highlighting a potential relationship between PCT levels and GBW thickness in patients with liver inflammation during acute VHA. Specifically, a positive correlation (r = 0.397; p = 0.011) was identified in GBW group B, indicating that PCT levels exceeding 0.25 ng/mL were more frequently associated with GBW thickness greater than 10 mm.
However, higher thresholds, such as PCT levels above 0.5 ng/mL, did not exhibit significant correlations. This suggests that in patients with acute VHA, the elevation and relevance of PCT as an indicator of hepatocyte damage may be most pronounced at moderate values. The mean PCT level was 0.371 ng/mL (range = 0.067–1.340; SD = 0.251). Moreover, only one patient had PCT lower than 0.1 ng/mL.
There was a strong positive correlation (r = 0.654; p < 0.0001) between GBW thickness in group B and the combined presence of GBW stratification and fluid accumulation, suggesting that patients with thicker GBW are significantly more likely to have these conditions.
Correlation of LSM and CAP with GBW thickening
The CAP values in the data set have a mean of 202.83 dB/m (SD = 35.04; range = 100–248). The LSM shows a mean of 10.92 kPa (SD = 3.86 kPa; range = 5.1–21.8 kPa).
We explored the potential relationships of LSM in patients with acute VHA with respect to GBW thickness groups and GBW thickness in millimeters. The statistical analysis of LSM in relation to GBW categories produced a p-value of 0.742, showing no significant difference. Similarly, the Pearson correlation test between LSM and GBW thickness revealed a coefficient r = 0.151 and a p-value of 0.353, confirming the presence of a weak and statistically non-significant relationship.
Statistical analysis using a t-test revealed significant variations in CAP values between different GBW groups. The mean CAP level for the GBW group A was 212.15 dB/m, whereas for the GBW group B, it was 183.46 dB/m. The higher mean CAP values observed in group A were statistically significant, indicating a notable difference between the two groups (t = 2.597; p = 0.013). This indicates that higher GBW thickness is associated with lower CAP levels. This finding suggests an inverse relationship between CAP levels and GBW thickness.
Furthermore, the relationship between CAP levels and continuous measurement of GBW thickness was assessed during the initial examination. Regression analysis revealed a statistically significant relationship between GBW thickness and CAP levels, with an intercept of 238.40 (p < 0.001) and a negative coefficient of −4.47 (p = 0.004), indicating that CAP levels decrease as GBW thickness increases.
Discussion
According to previous studies, VHA can present with several US abnormalities including ascites, GBW pathology or abdominal lymphadenopathy. 10 However, the GBW thickening may be observed in cases of acute and chronic cholecystitis, neoplasm, obstructive jaundice, ascites, hypoalbuminemia, heart failure, and cirrhosis as well. 8
In our cohort of VHA patients who underwent US examinations, we analyzed GBW pathology in relation to liver inflammation severity, correlating it with biochemical parameters, liver stiffness, and CAP measurements.
GBW thickening was observed in the majority of patients (95%), suggesting that increased GBW thickness is highly characteristic, if not pathognomonic, in patients with acute VHA. GBW stratification and GBW fluid accumulation were observed in 71% and 38%, respectively. Patients with GBW thickness <10 mm were significantly more common than those with thickness ⩾10 mm. In the study by Sharma, GBW thickening was observed in 98.2% of VHA patients. 11 Other literature sources report a frequency of approximately 70% of cases. Furthermore, the presence of GBW thickening predicts a more severe course of VHA. 9 Our observations are supported by previous findings, although the frequency of GBW thickening varies across studies. 11 The higher detection rate of GBW thickening in our study may be related to our methodology, which included three US measurements of GBW thickness at different stages of disease progression. This approach may have enhanced the detection of positive cases compared to a single assessment approach in studies by other authors.9,12
Several hypotheses have been proposed to explain the mechanism behind GBW thickening in patients with acute hepatitis. One theory suggests that injury to hepatocytes leads to reduced bile production and excretion, which may cause changes in gallbladder function and structure. Another hypothesis states that the hepatitis virus directly injures the mucosal and muscular layers of the gallbladder itself, as the virus is present in the bile. In addition, hepatocyte necrosis could trigger an inflammatory response in adjacent tissues, including the GBW.9,13– 15
In addition, a statistically significant difference in initial ALT levels was noted between the two GBW groups, indicating that patients with GBW thickness above 10mm exhibited notably higher ALT levels. Furthermore, the positive correlation between ALT levels and GBW fluid accumulation underscores that the severity of liver inflammation, as measured by ALT levels, is significantly associated with both GBW thickness and fluid accumulation. This is supported by the study of Kim et al., which found that patients with highly elevated serum liver enzyme levels are more likely to have GBW thickening and disruption of planes between the muscular and serosal layers than are patients with normal liver enzyme levels. 16
When comparing our findings with those from the study by Ahn et al., several similarities emerge. Ahn et al. also found a correlation between ALT levels and different GBW groups. This consistency in results highlights the significance of GBW thickness as an indicator of liver function and overall disease severity. In addition, Ahn et al. observed a correlation between GBW groups and INR, which was also demonstrated in our study.
On the contrary, our investigation revealed a significant association between GBW thickness and ammonia levels, a finding not reported by Ahn et al. or other studies. 9 This novel observation suggests that GBW thickness and fluid accumulation may serve as indicators of more severe hepatic dysfunction, as mentioned above. Elevated ammonia levels are commonly associated with hepatic encephalopathy, a severe complication of liver disease, implying that GBW thickening and fluid accumulation could be markers of advanced liver damage. The correlation between increased GBW thickness and higher ammonia levels, along with the relationship between GBW fluid accumulation and ammonia levels, underscores the potential significance of these US parameters in assessing the severity of liver pathology.
These results collectively demonstrate the potential of GBW thickness and fluid accumulation to serve as significant non-invasive markers for predicting severe liver inflammation in patients presenting with acute VHA, showing that the severity of hepatic dysfunction, as measured by ALT, ammonia, and INR levels, is significantly correlated with these GBW findings.
PCT levels are elevated in patients with various liver injuries for several reasons. Bacterial infections are a common cause of elevated PCT. 16 Ischemia-reperfusion injury (IRI), a common occurrence in liver transplantation, also leads to significant increases in PCT due to tissue damage and inflammatory responses. 17 18
Moreover, acute liver failures (ALFs) such as those from acute hepatitis or drug-induced liver injury can elevate PCT as part of the systemic inflammatory response. Chronic liver diseases, including hepatocellular carcinoma or chronic hepatitis, can cause intermittent increases in PCT, especially during acute exacerbations. 19
These references and findings underscore the multifactorial reasons behind elevated PCT in liver injuries, providing a valuable marker for clinicians in diagnosing and monitoring liver conditions.
Our study demonstrated that PCT levels were moderately elevated in patients with VHA. Notably, in cases where GBW thickness exceeded 10 mm, PCT levels over 0.25 ng/mL were positively correlated, suggesting that more severe liver inflammation might contribute to increased PCT values. This observation aligns with findings from the study on ALF by Rule et al., which reported that elevated PCT levels in ALF patients reflect hepatocyte necrosis and systemic inflammation rather than bacterial infection. 20
In our cohort, the relevance of PCT as a marker of liver inflammation was most evident when PCT values were between 0.25 and 0.5 ng/mL, as higher thresholds did not show significant correlations with GBW abnormalities. Rule et al. similarly noted that elevated PCT levels in ALF were influenced by the severity of hepatic injury rather than infection status. In their study, the median PCT values for non-infected ALF groups ranged from 1.57 to 2.29 ng/mL, highlighting the pivotal role of hepatic necrosis and systemic inflammation in elevating PCT levels. 20
These findings underscore the potential of PCT as a biomarker for liver injury severity in acute VHA. However, given the overlap between infection-induced and sterile inflammation-induced PCT elevation, caution should be exercised in interpreting PCT levels as a diagnostic tool for bacterial infections in this patient population.
The observed strong positive correlation between GBW thickness and the presence of both stratification and fluid accumulation in group B patients, during the initial examination (first visit), is noteworthy. This finding suggests a significant association between increased GBW thickness and severe GBW abnormalities such as stratification and fluid accumulation. We were not able to find any study correlating the GBW pathology (stratification/fluid accumulation) with GBW thickness in patients with acute viral hepatitis.
Furthermore, we observed a significant correlation between GBW thickening and CAP values in patients with VHA. CAP, a non-invasive tool for detecting hepatic steatosis, showed variability depending on the severity of inflammation and GBW pathology.
Patients with greater GBW thickness (⩾10 mm) tended to have significantly lower CAP values, suggesting an inverse relationship between GBW thickness and hepatic steatosis detection by CAP. This inverse correlation may be attributable to the acute inflammatory changes in the liver and GBW during VHA episodes. Increased GBW thickness likely reflects more severe inflammatory oedema, which can alter liver tissue echogenicity and thus modify CAP measurements. The reduced CAP accuracy during inflammatory phases is consistent with findings in autoimmune liver diseases (AILDs), where hepatic inflammation significantly impairs CAP’s diagnostic performance. Studies on autoimmune hepatitis (AIH) and primary biliary cholangitis (PBC) have shown that CAP values increase only after inflammation subsides. Moreover, while previous studies have described the effect of inflammation on CAP in chronic liver diseases, to the best of our knowledge, this is the first study to demonstrate a direct relationship between GBW thickening and altered CAP values in acute VHA. The unique nature of our results emphasises the potential role of GBW pathology as a factor influencing CAP interpretation during acute liver inflammation. Given these insights, it is crucial to consider both liver and gallbladder pathology when interpreting CAP in acute hepatitis. Our findings indicate that hepatic injury, as evidenced by increased GBW thickness, may obscure accurate assessment of hepatic fat content. This underscores the importance of follow-up CAP evaluations after recovery to reliably evaluate hepatic steatosis. 7
Our study also evaluated LSM in patients with acute VHA using TE. LSM is widely recognised as a non-invasive tool for assessing liver fibrosis in chronic liver diseases. However, as observed in our cohort, liver stiffness can be significantly elevated during acute liver inflammation, even in the absence of fibrosis.
Our study found no significant correlation between LSM and GBW thickness or fluid accumulation. The statistical analysis revealed a weak correlation between LSM and GBW thickness, confirming that TE measurements in acute VHA are primarily influenced by transient inflammatory changes rather than structural liver alterations.
These findings are consistent with those reported by Arena et al., who demonstrated that liver stiffness values during acute viral hepatitis exceed the cutoff values typically used to predict significant fibrosis or cirrhosis. In their study, a statistically significant positive correlation was observed between aminotransferase levels (ALT and AST) and LSM during the peak phase of inflammation (r = 0.53, p = 0.02 for ALT; r = 0.51, p = 0.03 for AST). A similar pattern was observed in our cohort, where elevated LSM values corresponded to peak aminotransferase levels, suggesting that hepatic necroinflammatory activity significantly influences LSM during acute hepatitis episodes. 21
The graphs depicting the trends in GBW thickness, ALT levels, and LSM values across multiple visits further illustrate the progression and resolution of acute hepatitis in our patients. ALT levels and GBW thickness measurements declined rapidly after peaking; however, LSM values declined at a slower pace (Figures 3 and 4).
This pattern suggests that while ALT levels provide an early indicator of liver inflammation, LSM values reflect more prolonged changes associated with tissue edema. LSM may serve as markers for ongoing tissue recovery rather than immediate inflammation. Our data suggest that elevated LSM values in acute VHA primarily reflect necroinflammatory activity, hepatocyte swelling, and tissue edema rather than permanent fibrotic changes. In contrast to CAP and GBW thickening correlation, the absence of a significant correlation between LSM and GBW thickness may indicate that liver stiffness, as measured by TE, is less affected by the degree of inflammatory changes reflected in GBW thickening. Thus, LSM should not be relied upon as a sole diagnostic tool for fibrosis in patients presenting with acute liver inflammation. Instead, clinicians should correlate LSM results with biochemical markers, particularly aminotransferase levels, and consider repeated LSM after the resolution of inflammation.
Conclusion
This study demonstrates the clinical utility of GBW thickening as a non-invasive marker of disease severity in acute VHA. The correlation of GBW thickness with ALT, ammonia, and INR levels aids in early outpatient risk stratification. GBW thickening ⩾10 mm, along with stratification and fluid accumulation, signals more severe liver inflammation, making US a useful tool for identifying high-risk patients.
A key strength of this study is its integration of imaging findings with biochemical markers and TE. The inverse relationship between GBW thickness and CAP values highlights the need for cautious CAP interpretation during acute inflammation. Likewise, TE overestimated liver stiffness, reflecting transient inflammation rather than fibrosis.
Clinicians should interpret PCT levels in VHA with caution, as mild elevations indicate inflammation rather than bacterial infection. Antibiotics should be prescribed only with clear evidence of bacterial infection or when PCT shows significant dynamics. This strategy minimises unnecessary antibiotic use.
Despite the small sample size and single-center study design, which limits generalisability, US and TE offer valuable insights. In clinical practice, combining US with ALT, ammonia, INR, and PCT can enhance patient management. Regular follow-up with US and biochemical assessment is recommended to monitor disease progression and recovery in acute VHA.
Footnotes
Acknowledgements
None.
Contributors
Stefan Porubcin—writing.
Alena Rovnakova—data curation and editing.
Ondrej Zahornacky—article supervision and graph generation.
Pavol Jarcuska—review and corrections.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
The Ethics Committee or Institutional Review Board of our hospital approved the study protocol, and all patients provided written informed consent before entering the study (Hospital: The Department of Infectious Diseases and Travel Medicine, Louis Pasteur University Hospital, Rastislavova 43, Kosice 04011, Slovakia, EU. The approval number is 235/EK/2023).
Permission from patient(s) or subject(s) obtained in writing for publishing their case report
Yes.
Permission obtained in writing from patient or any person whose photo is included for publishing their photographs and images
Yes.
Confirm that you are aware that permission from a previous publisher for reproducing any previously published material will be required should your article be accepted for publication and that you will be responsible for obtaining that permission
Yes.
Guarantor
A.R., MD, PhD.